
Associations between Dietary Antioxidant Vitamin Intake and the Changes in Bone Mass in Chinese Adolescents: A 2.5-Year Longitudinal Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Calcaneal Quantitative Ultrasound Measurements
2.3. Assessment of Dietary Vitamin A, C, and E Intakes
2.4. Assessment of Covariates
2.5. Statistical Analysis
3. Results
3.1. Descriptive Characteristics
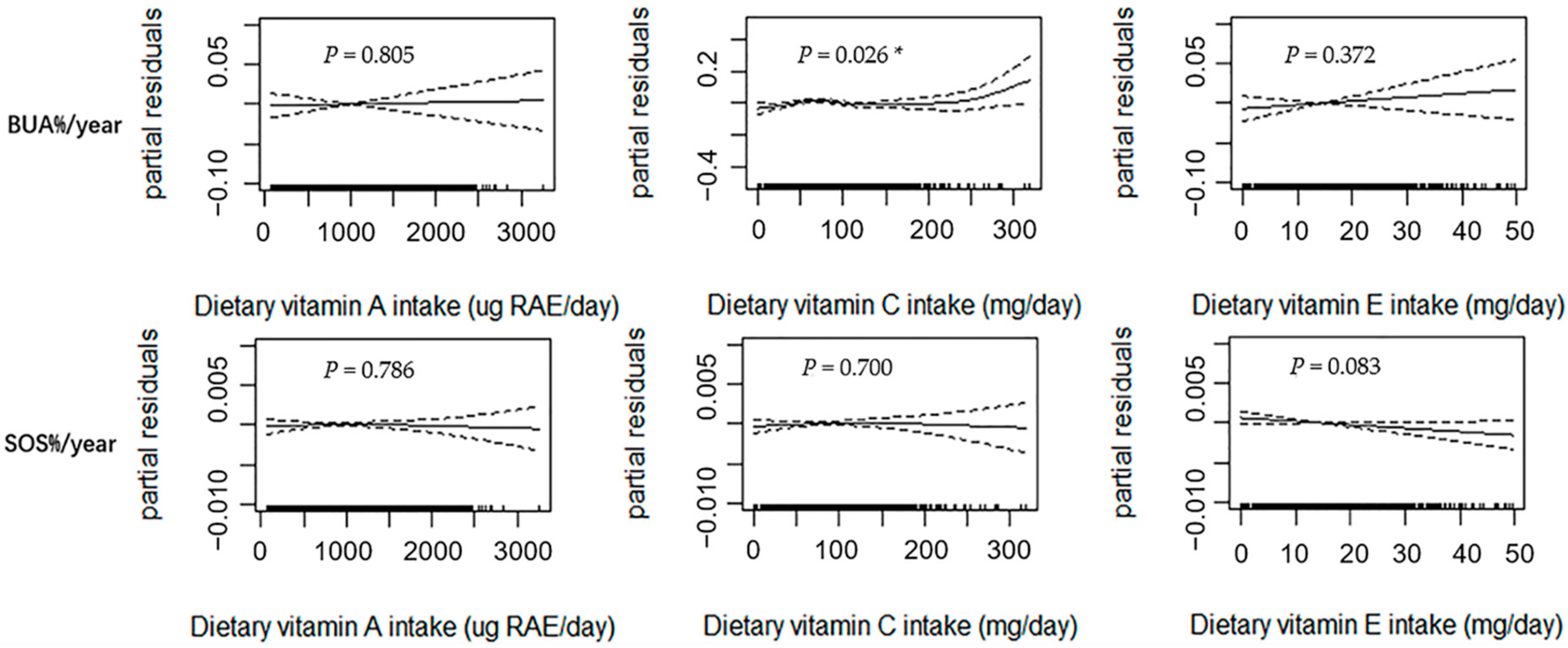
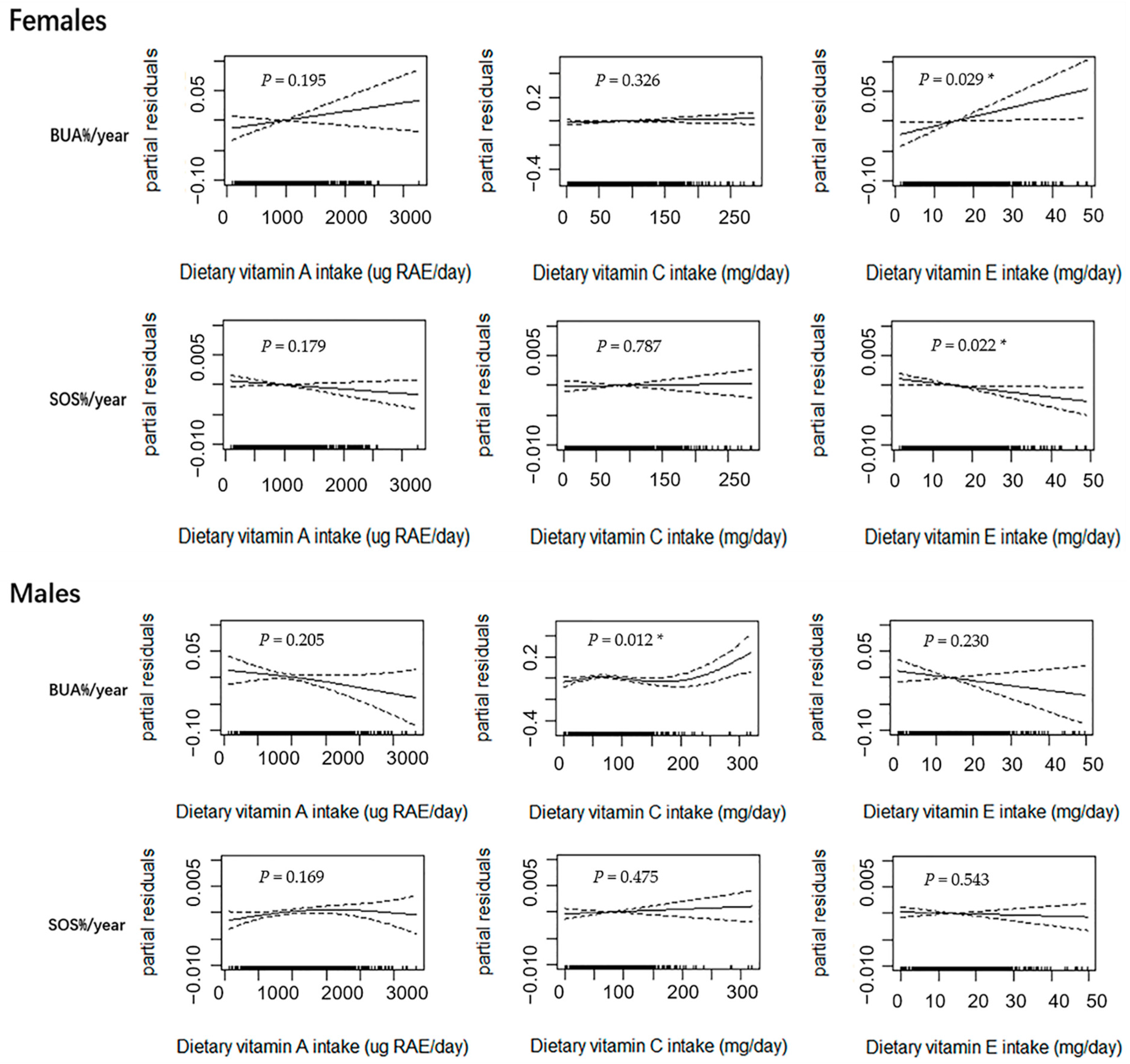
3.2. GAM Analysis of Dietary Vitamin A, C, and E Intakes and Changes in Bone Parameters
3.3. Linear Regression Analysis for the Association between Dietary Vitamin E Intake and Changes in Bone Parameters
3.4. Threshold Analysis for the Dietary Vitamin C Intake and Changes in BUA in Male Subjects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Matkovic, V.; Jelic, T.; Wardlaw, G.M.; Ilich, J.Z.; Goel, P.K.; Wright, J.K.; Andon, M.B.; Smith, K.T.; Heaney, R.P. Timing of peak bone mass in Caucasian females and its implication for the prevention of osteoporosis. Inference from a cross-sectional model. J. Clin. Investig. 1994, 93, 799–808. [Google Scholar] [CrossRef] [Green Version]
- Hernandez, C.J.; Beaupré, G.S.; Carter, D.R. A theoretical analysis of the relative influences of peak BMD, age-related bone loss and menopause on the development of osteoporosis. Osteoporos. Int. 2003, 14, 843–847. [Google Scholar] [CrossRef]
- Baxter-Jones, A.D.; Faulkner, R.A.; Forwood, M.R.; Mirwald, R.L.; Bailey, D.A. Bone mineral accrual from 8 to 30 years of age: An estimation of peak bone mass. J. Bone Miner. Res. 2011, 26, 1729–1739. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Rodríguez, M.A.; Ruiz-Ramos, M.; Correa-Muñoz, E.; Mendoza-Núñez, V.M. Oxidative stress as a risk factor for osteoporosis in elderly Mexicans as characterized by antioxidant enzymes. BMC Musculoskelet. Disord. 2007, 8, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bai, X.C.; Lu, D.; Liu, A.L.; Zhang, Z.M.; Li, X.M.; Zou, Z.P.; Zeng, W.S.; Cheng, B.L.; Luo, S.Q. Reactive oxygen species stimulates receptor activator of NF-kappaB ligand expression in osteoblast. J. Biol. Chem. 2005, 280, 17497–17506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baek, K.H.; Oh, K.W.; Lee, W.Y.; Lee, S.S.; Kim, M.K.; Kwon, H.S.; Rhee, E.J.; Han, J.H.; Song, K.H.; Cha, B.Y.; et al. Association of oxidative stress with postmenopausal osteoporosis and the effects of hydrogen peroxide on osteoclast formation in human bone marrow cell cultures. Calcif. Tissue Int. 2010, 87, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Zwart, S.R.; Morgan, J.L.; Smith, S.M. Iron status and its relations with oxidative damage and bone loss during long-duration space flight on the International Space Station. Am. J. Clin. Nutr. 2013, 98, 217–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maggio, D.; Barabani, M.; Pierandrei, M.; Polidori, M.C.; Catani, M.; Mecocci, P.; Senin, U.; Pacifici, R.; Cherubini, A. Marked decrease in plasma antioxidants in aged osteoporotic women: Results of a cross-sectional study. J. Clin. Endocrinol. Metab. 2003, 88, 1523–1527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arjmandi, B.; Juma, S.; Beharka, A.; Bapna, M.; Akhter, M.; Meydani, S. Vitamin E improves bone quality in the aged but not in young adult male mice. J. Nutr. Biochem. 2002, 13, 543. [Google Scholar] [CrossRef]
- Chavan, S.N.; More, U.; Mulgund, S.; Saxena, V.; Sontakke, A.N. Effect of supplementation of vitamin C and E on oxidative stress in osteoporosis. Indian J. Clin. Biochem. IJCB 2007, 22, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Pasco, J.A.; Henry, M.J.; Wilkinson, L.K.; Nicholson, G.C.; Schneider, H.G.; Kotowicz, M.A. Antioxidant vitamin supplements and markers of bone turnover in a community sample of nonsmoking women. J. Womens Health 2006, 15, 295–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunnes, M.; Lehmann, E.H. Dietary calcium, saturated fat, fiber and vitamin C as predictors of forearm cortical and trabecular bone mineral density in healthy children and adolescents. Acta Paediatr. 1995, 84, 388–392. [Google Scholar] [CrossRef]
- Yu, C.H.; Lee, J.S.; Lee, L.; Kim, S.H.; Lee, S.S.; Kang, S.A. Nutritional Factors Related to Bone Mineral Density in the Different Age Groups of Korean Men. Korean J. Nutr. 2004, 37, 132–142. [Google Scholar]
- Prynne, C.J.; Mishra, G.D.; O’Connell, M.A.; Muniz, G.; Laskey, M.A.; Yan, L.; Prentice, A.; Ginty, F. Fruit and vegetable intakes and bone mineral status: A cross sectional study in 5 age and sex cohorts. Am. J. Clin. Nutr. 2006, 83, 1420–1428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.C.; Moore, E.C.; Crawford, P.B.; Hudes, M.; Sabry, Z.I.; Marcus, R.; Bachrach, L.K. Influence of pre-adolescent diet on quantitative ultrasound measurements of the calcaneus in young adult women. Osteoporos. Int. 1999, 9, 532–535. [Google Scholar] [CrossRef] [PubMed]
- Kohri, T.; Kaba, N.; Murakami, T.; Narukawa, T.; Yamamoto, S.; Sakai, T.; Sasaki, S. Search for promotion factors of ultrasound bone measurement in Japanese males and pre/post-menarcheal females aged 8–14 years. J. Nutr. Sci. Vitaminol. 2012, 58, 263–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heydenreich, J.; Schweter, A.; Lührmann, P. Association between Body Composition, Physical Activity, Food Intake and Bone Status in German Children and Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 7294. [Google Scholar] [CrossRef] [PubMed]
- Falcini, F.; Bindi, G.; Ermini, M.; Galluzzi, F.; Poggi, G.; Rossi, S.; Masi, L.; Cimaz, R.; Brandi, M.L. Comparison of quantitative calcaneal ultrasound and dual energy X-ray absorptiometry in the evaluation of osteoporotic risk in children with chronic rheumatic diseases. Calcif. Tissue Int. 2000, 67, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Waud, C.E.; Lew, R.; Baran, D.T. The relationship between ultrasound and densitometric measurements of bone mass at the calcaneus in women. Calcif. Tissue Int. 1992, 51, 415–418. [Google Scholar] [CrossRef]
- Yang, Y.Y. China Food Composition Table, 6th ed.; Peking University Medical Press: Beijing, China, 2019. [Google Scholar]
- Yang, Y.X. China Food Composition Table, 5th ed.; Peking University Medical Press: Beijing, China, 2004. [Google Scholar]
- Huang, Y.J.; Wong, S.H.; Salmon, J. Reliability and validity of the modified Chinese version of the Children’s Leisure Activities Study Survey (CLASS) questionnaire in assessing physical activity among Hong Kong children. Pediatr. Exerc. Sci. 2009, 21, 339–353. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, T.; Kawai, R. Advances in food composition tables in Japan-Standard Tables Of Food Composition in Japan—2015—(Seventh Revised Edition). Food Chem. 2018, 238, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Chan, N.P.; Sung, R.Y.; Nelson, E.A.; So, H.K.; Tse, Y.K.; Kong, A.P. Measurement of pubertal status with a Chinese self-report Pubertal Development Scale. Matern. Child Health J. 2010, 14, 466–473. [Google Scholar] [CrossRef] [PubMed]
- Breitling, L.P. Calcium intake and bone mineral density as an example of non-linearity and threshold analysis. Osteoporos. Int. 2015, 26, 1271–1281. [Google Scholar] [CrossRef] [PubMed]
- Sahni, S.; Hannan, M.T.; Gagnon, D.; Blumberg, J.; Cupples, L.A.; Kiel, D.P.; Tucker, K.L. High vitamin C intake is associated with lower 4-year bone loss in elderly men. J. Nutr. 2008, 138, 1931–1938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon, J.A.; Hudes, E.S. Relation of ascorbic acid to bone mineral density and self-reported fractures among US adults. Am. J. Epidemiol. 2001, 154, 427–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finck, H.; Hart, A.R.; Jennings, A.; Welch, A.A. Is there a role for vitamin C in preventing osteoporosis and fractures? A review of the potential underlying mechanisms and current epidemiological evidence. Nutr. Res. Rev. 2014, 27, 268–283. [Google Scholar] [CrossRef] [Green Version]
- Katsimbri, P. The biology of normal bone remodelling. Eur. J. Cancer Care 2017, 26, e12740. [Google Scholar] [CrossRef] [PubMed]
- Park, J.K.; Lee, E.M.; Kim, A.Y.; Lee, E.J.; Min, C.W.; Kang, K.K.; Lee, M.M.; Jeong, K.S. Vitamin C deficiency accelerates bone loss inducing an increase in PPAR-γ expression in SMP30 knockout mice. Int. J. Exp. Pathol. 2012, 93, 332–340. [Google Scholar] [CrossRef]
- Ali, A.A.; Weinstein, R.S.; Stewart, S.A.; Parfitt, A.M.; Manolagas, S.C.; Jilka, R.L. Rosiglitazone causes bone loss in mice by suppressing osteoblast differentiation and bone formation. Endocrinology 2005, 146, 1226–1235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odai, T.; Terauchi, M.; Hirose, A.; Kato, K.; Miyasaka, N. Bone Mineral Density in Premenopausal Women Is Associated with the Dietary Intake of α-Tocopherol: A Cross-Sectional Study. Nutrients 2019, 11, 2474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, R.; Woo, J.; Lau, W.; Leung, J.; Xu, L.; Zhao, X.; Yu, W.; Lau, E.; Pocock, N. Effects of lifestyle and diet on bone health in young adult Chinese women living in Hong Kong and Beijing. Food Nutr. Bull. 2009, 30, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Shi, W.Q.; Liu, J.; Cao, Y.; Zhu, Y.Y.; Guan, K.; Chen, Y.M. Association of dietary and serum vitamin E with bone mineral density in middle-aged and elderly Chinese adults: A cross-sectional study. Br. J. Nutr. 2016, 115, 113–120. [Google Scholar] [CrossRef] [Green Version]
- Norazlina, M.; Maizatul-Neza, J.; Azarina, A.; Nazrun, A.S.; Norliza, M.; Ima-Nirwana, S. Effects of vitamin E on receptor activator of nuclear factor kappa B ligand (RANKL) and osteoprotegerin (OPG) in rats treated with nicotine. Med. J. Malays. 2010, 65, 14–17. [Google Scholar]
- Wong, S.K.; Mohamad, N.V.; Ibrahim, N.; Chin, K.Y.; Shuid, A.N.; Ima-Nirwana, S. The Molecular Mechanism of Vitamin E as a Bone-Protecting Agent: A Review on Current Evidence. Int. J. Mol. Sci. 2019, 20, 1453. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, N.; Mohamed, N.; Soelaiman, I.N.; Shuid, A.N. The Effects of Targeted Deliveries of Lovastatin and Tocotrienol on Ossification-Related Gene Expressions in Fracture Healing in an Osteoporosis Rat Model. Int. J. Environ. Res. Public Health 2015, 12, 12958–12976. [Google Scholar] [CrossRef] [Green Version]
- Wong, S.K.; Chin, K.Y.; Suhaimi, F.H.; Ahmad, F.; Ima-Nirwana, S. The Effects of Vitamin E from Elaeis guineensis (Oil Palm) in a Rat Model of Bone Loss Due to Metabolic Syndrome. Int. J. Environ. Res. Public Health 2018, 15, 1828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rejnmark, L.; Vestergaard, P.; Charles, P.; Hermann, A.P.; Brot, C.; Eiken, P.; Mosekilde, L. No effect of vitamin A intake on bone mineral density and fracture risk in perimenopausal women. Osteoporos. Int. 2004, 15, 872–880. [Google Scholar] [CrossRef] [PubMed]
- Lim, L.S.; Harnack, L.J.; Lazovich, D.; Folsom, A.R. Vitamin A intake and the risk of hip fracture in postmenopausal women: The Iowa Women’s Health Study. Osteoporos. Int. 2004, 15, 552–559. [Google Scholar] [CrossRef] [Green Version]
- Promislow, J.H.; Goodman-Gruen, D.; Slymen, D.J.; Barrett-Connor, E. Retinol intake and bone mineral density in the elderly: The Rancho Bernardo Study. J. Bone Miner. Res. 2002, 17, 1349–1358. [Google Scholar] [CrossRef]
- Melhus, H.; Michaëlsson, K.; Kindmark, A.; Bergström, R.; Holmberg, L.; Mallmin, H.; Wolk, A.; Ljunghall, S. Excessive dietary intake of vitamin A is associated with reduced bone mineral density and increased risk for hip fracture. Ann. Intern. Med. 1998, 129, 770–778. [Google Scholar] [CrossRef]
- Bauernfeind, J.C. Vitamin A—Application technology. Food Nutr. 1980, 6, 10–20. [Google Scholar]
- Frankel, T.L.; Seshadri, M.S.; McDowall, D.B.; Cornish, C.J. Hypervitaminosis A and calcium-regulating hormones in the rat. J. Nutr. 1986, 116, 578–587. [Google Scholar] [CrossRef] [PubMed]
- White, E.; Kristal, A.R.; Shikany, J.M.; Wilson, A.C.; Chen, C.; Mares-Perlman, J.A.; Masaki, K.H.; Caan, B.J. Correlates of serum alpha- and gamma-tocopherol in the Women’s Health Initiative. Ann. Epidemiol. 2001, 11, 136–144. [Google Scholar] [CrossRef]
- Landrier, J.F.; Marcotorchino, J.; Tourniaire, F. Lipophilic micronutrients and adipose tissue biology. Nutrients 2012, 4, 1622–1649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bredella, M.A. Sex Differences in Body Composition. Adv. Exp. Med. Biol. 2017, 1043, 9–27. [Google Scholar] [CrossRef]
- Meczekalski, B.; Podfigurna-Stopa, A.; Genazzani, A.R. Hypoestrogenism in young women and its influence on bone mass density. Gynecol. Endocrinol. 2010, 26, 652–657. [Google Scholar] [CrossRef]
- Li, R.; Wen, Z.; Yu, Q.; Xiao, S.M. Associations between sex hormone levels and calcaneal ultrasound bone parameters in female adolescents. Life Sci. Res. 2020, 24, 208–213. [Google Scholar] [CrossRef]
- Neville, C.E.; Robson, P.J.; Murray, L.J.; Strain, J.J.; Twisk, J.; Gallagher, A.M.; McGuinness, M.; Cran, G.W.; Ralston, S.H.; Boreham, C.A. The effect of nutrient intake on bone mineral status in young adults: The Northern Ireland young hearts project. Calcif. Tissue Int. 2002, 70, 89–98. [Google Scholar] [CrossRef]
- Gou, G.H.; Tseng, F.J.; Wang, S.H.; Chen, P.J.; Shyu, J.F.; Pan, R.Y. Nutritional factors associated with femoral neck bone mineral density in children and adolescents. BMC Musculoskelet. Disord. 2019, 20, 520. [Google Scholar] [CrossRef] [Green Version]
- Bonjour, J.P.; Carrie, A.L.; Ferrari, S.; Clavien, H.; Slosman, D.; Theintz, G.; Rizzoli, R. Calcium-enriched foods and bone mass growth in prepubertal girls: A randomized, double-blind, placebo-controlled trial. J. Clin. Investig. 1997, 99, 1287–1294. [Google Scholar] [CrossRef] [Green Version]
- El-Hajj Fuleihan, G.; Nabulsi, M.; Tamim, H.; Maalouf, J.; Salamoun, M.; Khalife, H.; Choucair, M.; Arabi, A.; Vieth, R. Effect of vitamin D replacement on musculoskeletal parameters in school children: A randomized controlled trial. J. Clin. Endocrinol. Metab. 2006, 91, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Golden, N.H.; Abrams, S.A. Optimizing bone health in children and adolescents. Pediatrics 2014, 134, e1229–e1243. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Values | Total (n = 1418) | Girl (n = 721) | Boy (n = 697) | p |
|---|---|---|---|---|
| Age (years) | 14.97 ± 1.46 | 14.99 ± 1.47 | 14.95 ± 1.45 | 0.974 |
| Height (cm) | 161.34 ± 9.33 | 157.54 ± 5.85 | 165.27 ± 10.56 | <0.001 * |
| Weight (kg) | 49.99 ± 10.59 | 47.72 ± 8.13 | 52.33 ± 12.20 | <0.001 * |
| Total physical activity (MET·h/day) | 19.59 ± 9.60 | 19.44 ± 10.45 | 19.75 ± 8.64 | 0.007 * |
| Dietary energy intake (kcal/day) | 2185 ± 845 | 1909 ± 827 | 2471 ± 764 | <0.001 * |
| Dietary calcium intake (mg/day) | 396.90 ± 171.18 | 356.41 ± 149.60 | 438.78 ± 181.81 | <0.001 * |
| Dietary vitamin D intake (µg/day) | 1.85 ± 1.29 | 1.81 ± 1.14 | 1.90 ± 1.43 | 0.467 |
| Dietary vitamin A intake (µg RAE/day) | 994.10 ± 528.45 | 973.10 ± 535.78 | 1015.82 ± 520.26 | 0.052 |
| Dietary vitamin C intake (mg/day) | 82.57 ± 47.37 | 84.81 ± 48.93 | 80.25 ± 45.62 | 0.118 |
| Dietary vitamin E intake (mg/day) | 14.59 ± 8.64 | 15.33 ± 8.48 | 13.82 ± 8.74 | <0.001 * |
| Annual relative rate of BUA change (%/year) | 20.50 ± 16.93 | 18.92 ± 16.19 | 22.13 ± 17.53 | 0.002 * |
| Annual relative rate of SOS change (%/year) | 1.17 ± 0.81 | 1.39 ± 0.81 | 0.95 ± 0.75 | <0.001 * |
| BUA%/year | SOS%/year | |||
|---|---|---|---|---|
| sβ | p | sβ | p | |
| Total (n = 1418) | 0.027 | 0.331 | −0.036 | 0.184 |
| Females (n = 721) | 0.082 | 0.033 * | −0.065 | 0.092 |
| Males (n = 697) | −0.042 | 0.283 | −0.014 | 0.736 |
| Dietary Vitamin C Intake | BUA%/year | |
|---|---|---|
| sβ | p | |
| <159.01 (mg/day) | −0.016 | 0.666 |
| ≥159.01 (mg/day) | 0.395 | 0.036 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, H.; Hou, J.-L.; Yang, W.-Y.; Zhang, Q.; Feng, H.; Wang, X.-B.; Deng, K.-L.; Mao, X.-L.; Xiao, S.-M. Associations between Dietary Antioxidant Vitamin Intake and the Changes in Bone Mass in Chinese Adolescents: A 2.5-Year Longitudinal Study. Nutrients 2022, 14, 4187. https://doi.org/10.3390/nu14194187
Li H, Hou J-L, Yang W-Y, Zhang Q, Feng H, Wang X-B, Deng K-L, Mao X-L, Xiao S-M. Associations between Dietary Antioxidant Vitamin Intake and the Changes in Bone Mass in Chinese Adolescents: A 2.5-Year Longitudinal Study. Nutrients. 2022; 14(19):4187. https://doi.org/10.3390/nu14194187
Chicago/Turabian StyleLi, Hui, Jin-Li Hou, Wan-Yu Yang, Qiong Zhang, Hao Feng, Xiao-Bao Wang, Kai-Li Deng, Xin-Liang Mao, and Su-Mei Xiao. 2022. "Associations between Dietary Antioxidant Vitamin Intake and the Changes in Bone Mass in Chinese Adolescents: A 2.5-Year Longitudinal Study" Nutrients 14, no. 19: 4187. https://doi.org/10.3390/nu14194187