
Ideal Life’s Simple 7 Score Relates to Macrovascular Structure and Function in the Healthy Population
 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Methods
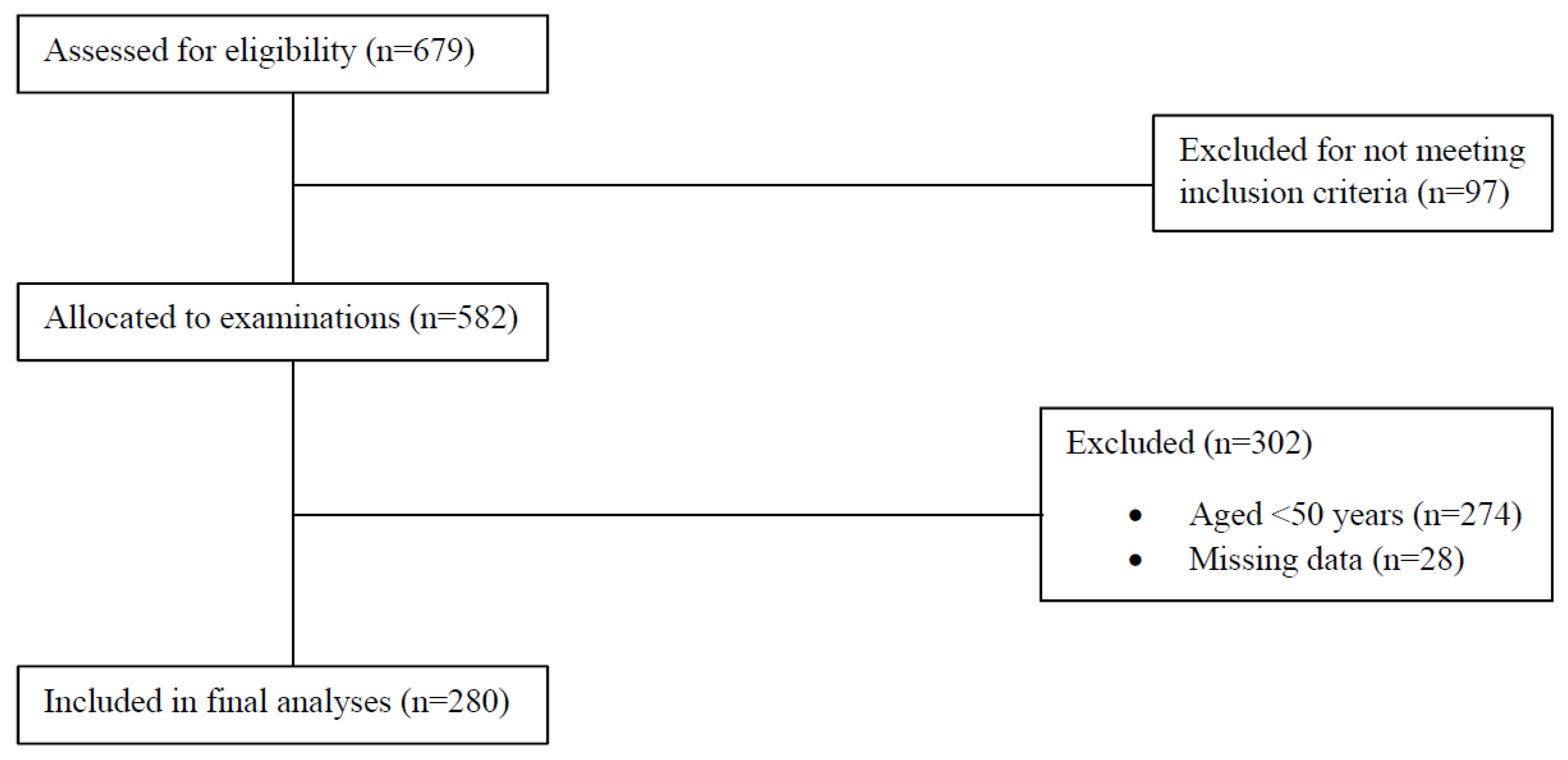
2.1. Population and Recruitment
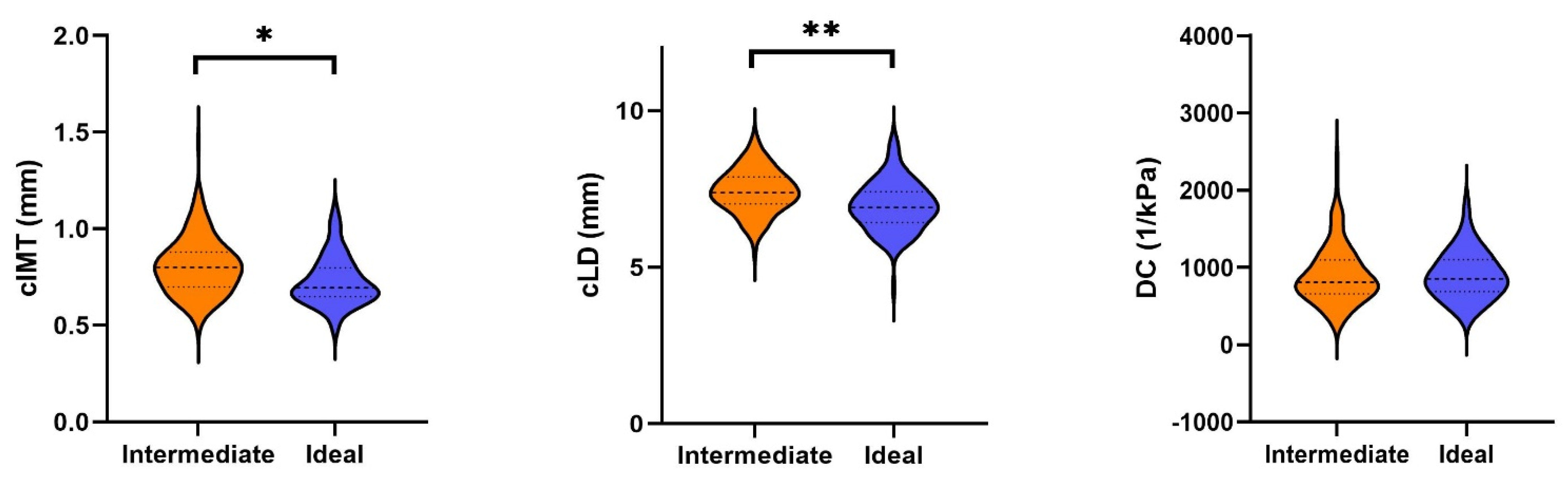
2.2. Carotid Properties
2.3. Pulse Wave Velocity
2.4. Endothelial Function
2.5. Physical Activity
2.6. Nutrition
2.7. Other Measurements
Cardiovascular Health Score
2.8. Statistical Analyses
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mahmood, S.S.; Levy, D.; Vasan, R.S.; Wang, T.J. The Framingham Heart Study and the epidemiology of cardiovascular disease: A historical perspective. Lancet 2014, 383, 999–1008. [Google Scholar] [CrossRef]
- Seals, D.R.; Justice, J.N.; LaRocca, T.J. Physiological geroscience: Targeting function to increase healthspan and achieve optimal longevity. J. Physiol. 2016, 594, 2001–2024. [Google Scholar] [CrossRef]
- Lloyd-Jones, D.M.; Hong, Y.; Labarthe, D.; Mozaffarian, D.; Appel, L.J.; Van Horn, L.; Rosamond, W.D. Defining and Setting National Goals for Cardiovascular Health Promotion and Disease Reduction. Circulation 2010, 121, 586–613. [Google Scholar] [CrossRef] [PubMed]
- Enserro, D.M.; Vasan, R.S.; Xanthakis, V. Twenty-Year Trends in the American Heart Association Cardiovascular Health Score and Impact on Subclinical and Clinical Cardiovascular Disease: The Framingham Offspring Study. J. Am. Heart Assoc. 2018, 7, e008741. [Google Scholar] [CrossRef]
- (BFS), B.f.S. Körperliche Aktivität. 2018. Available online: https://www.bfs.admin.ch/bfs/de/home/statistiken/gesundheit/determinanten/koerperliche-aktivitaet.html (accessed on 28 June 2022).
- (BFS), B.f.S. Ernährung. 2018. Available online: https://www.bfs.admin.ch/bfs/de/home/statistiken/gesundheit/determinanten/ernaehrung.html (accessed on 28 June 2022).
- (BFS), B.f.S. Tabak. 2020. Available online: https://www.bfs.admin.ch/bfs/de/home/statistiken/gesundheit/determinanten/tabak.html (accessed on 28 June 2022).
- (BFS), B.f.S. Alkohol. 2018. Available online: https://www.bfs.admin.ch/bfs/de/home/statistiken/gesundheit/determinanten/alkohol.html (accessed on 28 June 2022).
- Folsom, A.R.; Yatsuya, H.; Nettleton, J.A.; Lutsey, P.L.; Cushman, M.; Rosamond, W.D.; ARIC Study Investigators. Community prevalence of ideal cardiovascular health, by the American Heart Association definition, and relationship with cardiovascular disease incidence. J. Am. Coll. Cardiol. 2011, 57, 1690–1696. [Google Scholar] [CrossRef] [PubMed]
- Folsom, A.R.; Olson, N.C.; Lutsey, P.L.; Roetker, N.S.; Cushman, M. American Heart Association’s Life’s Simple 7 and incidence of venous thromboembolism. Am. J. Hematol. 2015, 90, E92. [Google Scholar] [CrossRef]
- Oyenuga, A.O.; Folsom, A.R.; Cheng, S.; Tanaka, H.; Meyer, M.L. Greater Adherence to Life’s Simple 7 Is Associated with Less Arterial Stiffness: The Atherosclerosis Risk in Communities (ARIC) Study. Am. J. Hypertens. 2019, 32, 769–776. [Google Scholar] [CrossRef]
- Nonterah, E.A.; Crowther, N.J.; Oduro, A.; Agongo, G.; Micklesfield, L.K.; Boua, P.R.; Klipstein-Grobusch, K. Poor cardiovascular health is associated with subclinical atherosclerosis in apparently healthy sub-Saharan African populations: An H3Africa AWI-Gen. study. BMC Med. 2021, 19, 30. [Google Scholar] [CrossRef]
- Talegawkar, S.A.; Jin, Y.; Kandula, N.R.; Kanaya, A.M. Cardiovascular health metrics among South Asian adults in the United States: Prevalence and associations with subclinical atherosclerosis. Prev. Med. 2017, 96, 79–84. [Google Scholar] [CrossRef]
- Santos, I.S.; Goulart, A.C.; Pereira, A.C.; Lotufo, P.A.; Bensenor, I.M. Association between Cardiovascular Health Score and Carotid Intima-Media Thickness: Cross-Sectional Analysis of the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil) Baseline Assessment. J. Am. Soc. Echocardiogr. 2016, 29, 1207–1216.e4. [Google Scholar] [CrossRef]
- Bauer, M.; Caviezel, S.; Teynor, A.; Erbel, R.; Mahabadi, A.A.; Schmidt, A. Carotid intima-media thickness as a biomarker of subclinical atherosclerosis. Swiss Med. Wkly. 2012, 142, w13705. [Google Scholar] [CrossRef] [PubMed]
- Sedaghat, S.; Van Sloten, T.T.; Laurent, S.; London, G.M.; Pannier, B.; Kavousi, M.; Stehouwer, C.D. Common Carotid Artery Diameter and Risk of Cardiovascular Events and Mortality. Hypertension 2018, 72, 85–92. [Google Scholar] [CrossRef] [PubMed]
- van den Munckhof, I.; Scholten, R.; Cable, N.T.; Hopman, M.T.; Green, D.J.; Thijssen, D.H.J. Impact of age and sex on carotid and peripheral arterial wall thickness in humans. Acta Physiol. 2012, 206, 220–228. [Google Scholar] [CrossRef]
- Fritze, F.; Ittermann, T.; Volzke, H.; Felix, S.B.; Schminke, U.; Bahls, M. Carotid Lumen Diameter Is Associated with All-Cause Mortality in the General Population. J. Am. Heart Assoc. 2020, 9, e015630. [Google Scholar] [CrossRef]
- Yeboah, J.; Folsom, A.R.; Burke, G.L.; Johnson, C.; Polak, J.F.; Post, W.; Lima, J.A.; Crouse, J.R.; Herrington, D.M. Predictive value of brachial flow-mediated dilation for incident cardiovascular events in a population-based study: The multi-ethnic study of atherosclerosis. Circulation 2009, 120, 502–509. [Google Scholar] [CrossRef]
- Königstein, K.; Wagner, J.; Frei, M.; Knaier, R.; Klenk, C.; Carrard, J.; Schmidt, A. Endothelial function of healthy adults from 20 to 91 years of age: Prediction of cardiovascular risk by vasoactive range. J. Hypertens. 2021, 39, 1361–1369. [Google Scholar] [CrossRef]
- Konigstein, K.; Wagner, J.; Infanger, D.; Knaier, R.; Neve, G.; Klenk, C.; Schmidt, A. Cardiorespiratory Fitness and Endothelial Function in Aging Healthy Subjects and Patients with Cardiovascular Disease. Front. Cardiovasc. Med. 2022, 9, 870847. [Google Scholar] [CrossRef]
- Sutton-Tyrrell, K.; Najjar, S.S.; Boudreau, R.M.; Venkitachalam, L.; Kupelian, V.; Simonsick, E.M.; Havlik, R.; Lakatta, E.G.; Spurgeon, H.; Kritchevsky, S.; et al. Elevated aortic pulse wave velocity, a marker of arterial stiffness, predicts cardiovascular events in well-functioning older adults. Circulation 2005, 111, 3384–3390. [Google Scholar] [CrossRef]
- Hodes, R.J.; Lakatta, E.G.; McNeil, C.T. Another modifiable risk factor for cardiovascular disease? Some evidence points to arterial stiffness. J. Am. Geriatr. Soc. 1995, 43, 581–582. [Google Scholar] [CrossRef]
- Wagner, J.; Knaier, R.; Infanger, D.; Arbeev, K.; Briel, M.; Dieterle, T.; Schmidt, A. Functional aging in health and heart failure: The COmPLETE Study. BMC Cardiovasc. Disord. 2019, 19, 180. [Google Scholar] [CrossRef]
- Stein, J.H.; Korcarz, C.E.; Hurst, R.T.; Lonn, E.; Kendall, C.B.; Mohler, E.R.; Najjar, S.S.; Rembold, C.M.; Post, W.S. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: A consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascular Medicine. J. Am. Soc. Echocardiogr. 2008, 21, 93–111. [Google Scholar]
- Königstein, K.; von Schenck, U.; Buschges, J.C.; Schweizer, D.; Vogelgesang, F.; Damerow, S.; Neuhauser, H. Carotid IMT and Stiffness in the KiGGS 2 National Survey: Third-Generation Measurement, Quality Algorithms and Determinants of Completeness. Ultrasound Med. Biol. 2021, 47, 296–308. [Google Scholar] [CrossRef]
- Li, Y.; Recio-Rodriguez, J.I.; Garcia-Ortiz, L.; Hanssen, H.; Schmidt, A. Diurnal variation of arterial stiffness in healthy individuals of different ages and patients with heart disease. Scand. J. Clin. Lab. Invest. 2014, 74, 155–162. [Google Scholar] [CrossRef]
- Thijssen, D.H.J.; Bruno, R.M.; van Mil, A.C.; Holder, S.M.; Faita, F.; Greyling, A.; Ghiadoni, L. Expert consensus and evidence-based recommendations for the assessment of flow-mediated dilation in humans. Eur. Heart J. 2019, 40, 2534–2547. [Google Scholar] [CrossRef]
- Esliger, D.W.; Rowlands, A.V.; Hurst, T.L.; Catt, M.; Murray, P.; Eston, R.G. Validation of the GENEA Accelerometer. Med. Sci. Sports Exerc. 2011, 43, 1085–1093. [Google Scholar] [CrossRef]
- Dillon, C.B.; Fitzgerald, A.P.; Kearney, P.M.; Perry, I.J.; Rennie, K.L.; Kozarski, R.; Phillips, C.M. Number of Days Required to Estimate Habitual Activity Using Wrist-Worn GENEActiv Accelerometer: A Cross-Sectional Study. PLoS ONE 2016, 11, e0109913. [Google Scholar] [CrossRef]
- Nève, G.; Bur, L.; Lampert, L.; Höchsmann, C.; Brombach, C.; Steinemann, N.; Schmidt-Trucksäss, A. Validation of a Visually Aided Dietary Assessment Tool to Estimate Dietary Intake in an Adult Swiss Population. Front. Nutr. 2022, 9, 844156. [Google Scholar] [CrossRef]
- Ford, E.S.; Greenlund, K.J.; Hong, Y. Ideal Cardiovascular Health and Mortality from All Causes and Diseases of the Circulatory System Among Adults in the United States. Circulation 2012, 125, 987–995. [Google Scholar] [CrossRef]
- Krejza, J.; Arkuszewski, M.; Kasner, S.E.; Weigele, J.; Ustymowicz, A.; Hurst, R.W.; Cucchiara, B.L.; Messe, S.R. Carotid Artery Diameter in Men and Women and the Relation to Body and Neck Size. Stroke 2006, 37, 1103–1105. [Google Scholar] [CrossRef]
- Harrell, F. Regression Modeling Strategies, 2nd ed.; Springer International Publishing: Cham, Switzerland, 2015. [Google Scholar]
- Jakobsen, J.C.; Gluud, C.; Wetterslev, J.; Winkel, P. When and how should multiple imputation be used for handling missing data in randomised clinical trials—A practical guide with flowcharts. BMC Med. Res. Methodol. 2017, 17, 162. [Google Scholar] [CrossRef]
- van Buuren, S. Flexible Imputation of Missing Data, 2nd ed.; Chapman and Hall/CRC: Boca Raton, FL, USA, 2018. [Google Scholar]
- Lorenz, M.W.; Markus, H.S.; Bots, M.L.; Rosvall, M.; Sitzer, M. Prediction of clinical cardiovascular events with carotid intima-media thickness: A systematic review and meta-analysis. Circulation 2007, 115, 459–467. [Google Scholar] [CrossRef] [Green Version]
- Ramírez-Vélez, R.; Saavedra, J.M.; Lobelo, F.; Celis-Morales, C.A.; del Pozo-Cruz, B.; García-Hermoso, A. Ideal Cardiovascular Health and Incident Cardiovascular Disease Among Adults: A Systematic Review and Meta-analysis. Mayo Clin. Proc. 2018, 93, 1589–1599. [Google Scholar] [CrossRef]
- Wilson, P.W.; D’Agostino, R.B.; Levy, D.; Belanger, A.M.; Silbershatz, H.; Kannel, W.B. Prediction of Coronary Heart Disease Using Risk Factor Categories. Circulation 1998, 97, 1837–1847. [Google Scholar] [CrossRef]
- Hemann, B.A.; Bimson, W.F.; Taylor, A.J. The Framingham Risk Score: An appraisal of its benefits and limitations. Am. Heart Hosp. J. 2007, 5, 91–96. [Google Scholar] [CrossRef]
- Zyriax, B.-C.; Dransfeld, K.; Windler, E. Carotid intima-media thickness and cardiovascular risk factors in healthy volunteers. Ultrasound J. 2021, 13, 17. [Google Scholar] [CrossRef]
- Allison, P. Missing Data—Quantitative Applications in the Social Sciences; Sage Publishing: Newburry Park, CA, USA, 2001; Volume 136. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | All | N | Ideal HS | N | Intermediate HS | p-Value | |
|---|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | |||||
| Male, n (%) | 280 | 142 (50.7) | 125 | 63 (50.4) | 155 | 79 (51.0) | |
| Age | 280 | 68.1 (10.7) | 125 | 64.7 (10.1) | 155 | 70.9 (10.4) | <0.001 |
| cIMT (mm) | 277 | 0.772 (0.144) | 124 | 0.730 (0.127) | 153 | 0.807 (0.148) | <0.001 |
| cLD (mm) | 216 | 7.21 (0.77) | 103 | 6.96 (0.78) | 113 | 7.43 (0.68) | <0.001 |
| DC (l/kPa) | 216 | 905.5 (344.9) | 103 | 903.3 (308.0) | 113 | 907.6 (376.7) | 0.872 |
| baPWV (m/s) | 280 | 13.65 (2.49) | 125 | 12.77 (2.22) | 155 | 14.36 (2.48) | <0.001 |
| FMD (%) | 212 | 5.86 (3.66) | 98 | 6.27 (3.69) | 114 | 5.51 (3.62) | 0.122 |
| Systolic BP (mmHg) | 280 | 131 (13) | 125 | 125 (12) | 155 | 136 (12) | <0.001 |
| Diastolic BP (mmHg) | 280 | 81 (8) | 125 | 78 (8) | 155 | 83 (8) | <0.001 |
| Body mass index (kg/m2) | 280 | 24.0 (2.7) | 125 | 23.3 (2.4) | 155 | 24.5 (2.8) | <0.001 |
| Waist to hip ratio | 280 | 0.90 (0.08) | 125 | 0.88 (0.07) | 155 | 0.91 (0.08) | <0.001 |
| Low PA (min) | 272 | 107 (34) | 125 | 109 (36) | 147 | 104 (32) | 0.213 |
| Moderate PA (min) | 272 | 154 (65) | 125 | 177 (62) | 147 | 134 (60) | <0.001 |
| Vigorous PA (min) | 272 | 6 (9) | 125 | 9 (11) | 147 | 4 (7) | <0.001 |
| Triglycerides (mg/dl) | 278 | 121 (59) | 124 | 126 (55) | 154 | 125 (54) | 0.119 |
| Total cholesterol (mg/dl) | 278 | 238 (38) | 124 | 226 (34) | 154 | 248 (39) | <0.001 |
| Fruits and vegetables (portions/d) | 277 | 3.5 (1.7) | 124 | 4.2 (1.8) | 153 | 3.0 (1.4) | 0.024 |
| Antihypertensives n (%) | 280 | 49 (17.5) | 125 | 11 (8.8) | 155 | 38 (24.5) | <0.001 |
| Beta-blocker n (%) | 280 | 9 (3.2) | 125 | 2 (1.6) | 155 | 7 (4.5) | 0.150 |
| Outcome Variable | Health Score | Estimate | 95% Confidence Intervals | p-Value | |
|---|---|---|---|---|---|
| cIMT (mm) | Ideal-Intermediate | −0.038 | −0.069 | −0.007 | 0.017 |
| cLD (mm) | Ideal–Intermediate | −0.28 | −0.46 | −0.11 | 0.002 |
| DC (1/kPa) 1 | Ideal–Intermediate | 0.94 | 0.85 | 1.05 | 0.207 |
| FMD (%) | Ideal–Intermediate | 0.31 | −0.58 | 1.20 | 0.495 |
| baPWV (%) 1 | Ideal-Intermediate | 0.95 | 0.92 | 0.98 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nève, G.; Wagner, J.; Knaier, R.; Infanger, D.; Klenk, C.; Carrard, J.; Hinrichs, T.; Hanssen, H.; Schmidt-Trucksäss, A.; Königstein, K. Ideal Life’s Simple 7 Score Relates to Macrovascular Structure and Function in the Healthy Population. Nutrients 2022, 14, 3616. https://doi.org/10.3390/nu14173616
Nève G, Wagner J, Knaier R, Infanger D, Klenk C, Carrard J, Hinrichs T, Hanssen H, Schmidt-Trucksäss A, Königstein K. Ideal Life’s Simple 7 Score Relates to Macrovascular Structure and Function in the Healthy Population. Nutrients. 2022; 14(17):3616. https://doi.org/10.3390/nu14173616
Chicago/Turabian StyleNève, Gilles, Jonathan Wagner, Raphael Knaier, Denis Infanger, Christopher Klenk, Justin Carrard, Timo Hinrichs, Henner Hanssen, Arno Schmidt-Trucksäss, and Karsten Königstein. 2022. "Ideal Life’s Simple 7 Score Relates to Macrovascular Structure and Function in the Healthy Population" Nutrients 14, no. 17: 3616. https://doi.org/10.3390/nu14173616