
Efficacy and Safety of a Long-Term Multidisciplinary Weight Loss Intervention under Hospitalization in Aging Patients with Obesity: An Open Label Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design and Setting
2.2. Participants
2.3. Intervention
2.4. Study Outcomes
2.4.1. Anthropometric Measurements
2.4.2. Body Composition
2.4.3. Physical Activity
2.4.4. Behavioural and Psychodynamic Treatment
2.4.5. Assessment of REE
2.4.6. Biochemical Analysis
2.5. Statistical Analysis
3. Results
3.1. The Effect of the Hypo-Caloric Diet on the Outcomes
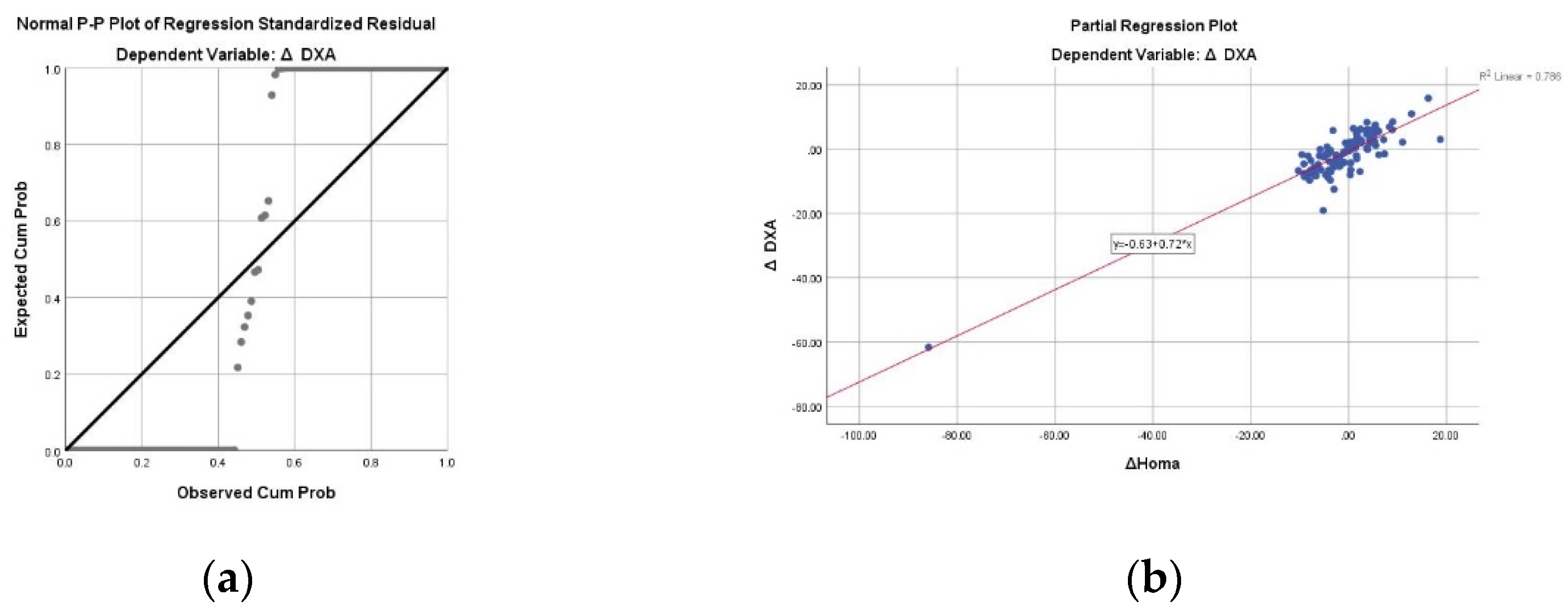
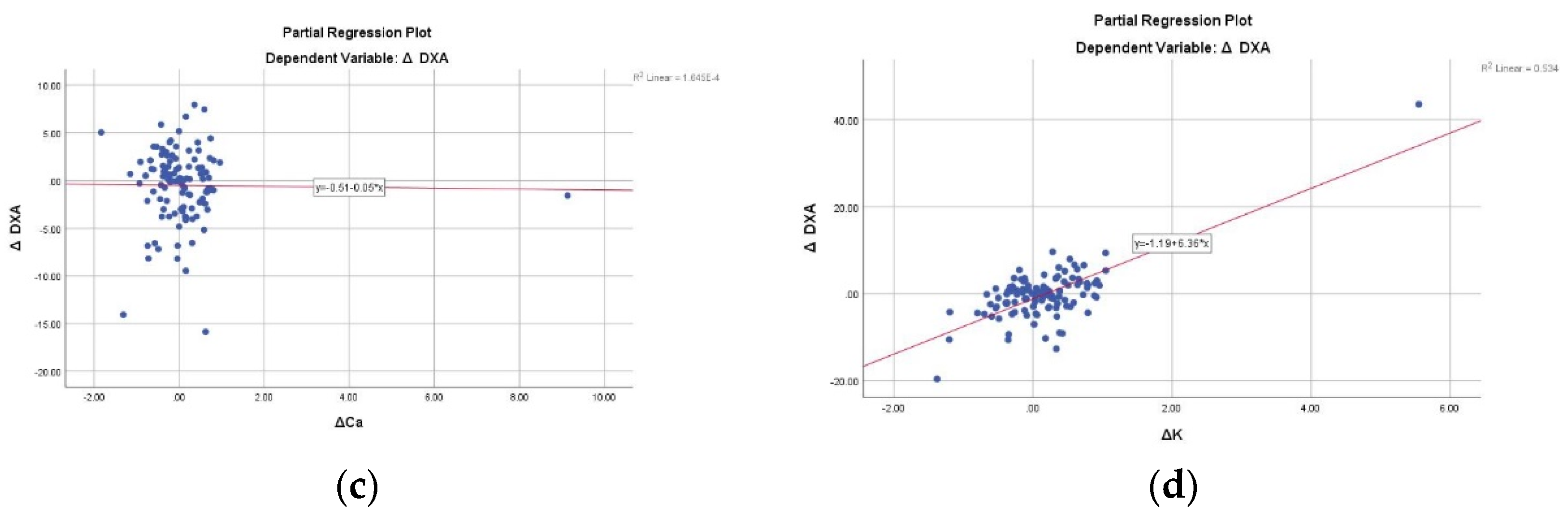
3.2. The Association between the Outcomes and the Weight Loss
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Garvey, W.T. Clinical definition of overweight and obesity. In Bariatric Endocrinology: Evaluation and Management of Adiposity, Adiposopathy and Related Diseases; Springer International Publishing: Cham, Switzerland, 2018; pp. 121–143. ISBN 9783319956558. [Google Scholar]
- De Lorenzo, A.; Romano, L.; Di Renzo, L.; Di Lorenzo, N.; Cenname, G.; Gualtieri, P. Obesity: A preventable, treatable, but relapsing disease. Nutrition 2020, 71, 110615. [Google Scholar] [CrossRef] [PubMed]
- Keaver, L.; Webber, L.; Dee, A.; Shiely, F.; Marsh, T.; Balanda, K.; Perry, I. Application of the UK foresight obesity model in Ireland: The health and economic consequences of projected obesity trends in Ireland. PLoS ONE 2013, 8, e79827. [Google Scholar] [CrossRef]
- World Health Organization. WHO|Target 7: Halt the Rise in Obesity; World Health Organization: Geneva, Switzerland, 2017.
- Bray, G.A. Medical consequences of obesity. J. Clin. Endocrinol. Metab. 2004, 89, 2583–2589. [Google Scholar] [CrossRef] [PubMed]
- Yu, K.; Li, L.; Zhang, L.; Guo, L.; Wang, C. Association between MC4R rs17782313 genotype and obesity: A meta-analysis. Gene 2020, 733, 144372. [Google Scholar] [CrossRef]
- El Hajj Chehadeh, S.; Osman, W.; Nazar, S.; Jerman, L.; Alghafri, A.; Sajwani, A.; Alawlaqi, M.; AlObeidli, M.; Jelinek, H.F.; AlAnouti, F.; et al. Implication of genetic variants in overweight and obesity susceptibility among the young Arab population of the United Arab Emirates. Gene 2020, 739, 144509. [Google Scholar] [CrossRef]
- Li, S.; Zhao, J.H.; Luan, J.; Luben, R.N.; Rodwell, S.A.; Khaw, K.T.; Ong, K.K.; Wareham, N.J.; Loos, R.J.F. Cumulative effects and predictive value of common obesity-susceptibility variants identified by genome-wide association studies. Am. J. Clin. Nutr. 2010, 91, 184–190. [Google Scholar] [CrossRef]
- Shama, N.; Kumari, R.; Bais, S.; Shrivastava, A. Some important peptides and their role in obesity-current insights. Obes. Med. 2019, 16, 100144. [Google Scholar] [CrossRef]
- Wilding, J.P.H. Endocrine testing in obesity. Eur. J. Endocrinol. 2020, 182, C13–C15. [Google Scholar] [CrossRef]
- Apovian, C.M. Obesity: Definition, Comorbidities, Causes, and Burden. Am. J. Manag. Care 2016, 22, S176–S185. [Google Scholar]
- Wright, S.M.; Aronne, L.J. Causes of obesity. Abdom. Imaging 2012, 37, 730–732. [Google Scholar] [CrossRef]
- Ma, X.; Chen, Q.; Pu, Y.; Guo, M.; Jiang, Z.; Huang, W.; Long, Y.; Xu, Y. Skipping breakfast is associated with overweight and obesity: A systematic review and meta-analysis. Obes. Res. Clin. Pract. 2020, 14, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, K.; Tasali, E.; Leproult, R.; Van Cauter, E. Effects of poor and short sleep on glucose metabolism and obesity risk. Nat. Rev. Endocrinol. 2009, 5, 253–261. [Google Scholar] [CrossRef] [PubMed]
- McCafferty, B.J.; Hill, J.O.; Gunn, A.J. Obesity: Scope, Lifestyle Interventions, and Medical Management. Tech. Vasc. Interv. Radiol. 2020, 23, 100653. [Google Scholar] [CrossRef] [PubMed]
- Sibuyi, N.R.S.; Moabelo, K.L.; Meyer, M.; Onani, M.O.; Dube, A.; Madiehe, A.M. Nanotechnology advances towards development of targeted-treatment for obesity. J. Nanobiotechnol. 2019, 17, 1–21. [Google Scholar] [CrossRef]
- Taylor, J. Looking Beyond Lifestyle: A Comprehensive Approach to the Treatment of Obesity in the Primary Care Setting. J. Nurse Predict. 2020, 16, 74–78. [Google Scholar] [CrossRef]
- Giordani, I.; Malandrucco, I.; Donno, S.; Picconi, F.; Di Giacinto, P.; Di Flaviani, A.; Chioma, L.; Frontoni, S. Acute caloric restriction improves glomerular filtration rate in patients with morbid obesity and type 2 diabetes. Diabetes Metab. 2014, 40, 158–160. [Google Scholar] [CrossRef]
- Morel, O.; Luca, F.; Grunebaum, L.; Jesel, L.; Meyer, N.; Desprez, D.; Robert, S.; Dignat-George, F.; Toti, F.; Simon, C.; et al. Short-term very low-calorie diet in obese females improves the haemostatic balance through the reduction of leptin levels, PAI-1 concentrations and a diminished release of platelet and leukocyte-derived microparticles. Int. J. Obes. 2011, 35, 1479–1486. [Google Scholar] [CrossRef]
- Hammer, S.; Snel, M.; Lamb, H.J.; Jazet, I.M.; van der Meer, R.W.; Pijl, H.; Meinders, E.A.; Romijn, J.A.; de Roos, A.; Smit, J.W.A. Prolonged Caloric Restriction in Obese Patients With Type 2 Diabetes Mellitus Decreases Myocardial Triglyceride Content and Improves Myocardial Function. J. Am. Coll. Cardiol. 2008, 52, 1006–1012. [Google Scholar] [CrossRef]
- Von Bibra, H.; Wulf, G.; Sutton, M.; Pfützner, A.; Schuster, T.; Heilmeyer, P. Low-carbohydrate/high-protein diet improves diastolic cardiac function and the metabolic syndrome in overweight-obese patients with type 2 diabetes. IJC Metab. Endocr. 2014, 2, 11–18. [Google Scholar] [CrossRef]
- Jazet, I.M.; de Craen, A.J.; van Schie, E.M.; Meinders, A.E. Sustained beneficial metabolic effects 18 months after a 30-day very low calorie diet in severely obese, insulin-treated patients with type 2 diabetes. Diabetes Res. Clin. Pract. 2007, 77, 70–76. [Google Scholar] [CrossRef]
- Snel, M.; Sleddering, M.A.; Vd Peijl, I.D.; Romijn, J.A.; Pijl, H.; Edo Meinders, A.; Jazet, I.M. Quality of life in type 2 diabetes mellitus after a very low calorie diet and exercise. Eur. J. Intern. Med. 2012, 23, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Dalle Grave, R.; Melchionda, N.; Calugi, S.; Centis, E.; Tufano, A.; Fatati, G.; Fusco, M.; Marchesini, G. Continuous care in the treatment of obesity: An observational multicentre study. J. Intern. Med. 2005, 258, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Bennett, J.A. The Consolidated Standards of Reporting Trials (CONSORT): Guidelines for Reporting Randomized Trials. Nurs. Res. 2005, 54, 128–132. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association; Bantle, J.; Wylie-Rosett, J.; Albright, A.; Apovian, C.; Clark, N.; Franz, M.; Hoogwerf, B.; Lichtenstein, A.; Mayer-Davis, E.; et al. Nutrition recommendations and interventions for diabetes: A position statement of the American Diabetes Association. Diabetes Care 2008, 31, S61–S78. [Google Scholar] [CrossRef]
- Davis, N.J.; Emerenini, A.; Wylie-Rosett, J. Obesity management: Physician practice patterns and patient preference. Diabetes Educ. 2006, 32, 557–561. [Google Scholar] [CrossRef]
- Wylie-Rosett, J.; Albright, A.A.; Apovian, C.; Clark, N.G.; Delahanty, L.; Franz, M.J.; Hoogwerf, B.; Kulkarni, K.; Lichtenstein, A.H.; Mayer-Davis, E.; et al. 2006–2007 American Diabetes Association Nutrition Recommendations: Issues for practice translation. J. Am. Diet. Assoc. 2007, 107, 1296–1304. [Google Scholar] [CrossRef]
- Frisancho, A.R. New standards of weight and body composition by frame size and height for assessment of nutritional status of adults and the elderly. Am. J. Clin. Nutr. 1984, 40, 808–819. [Google Scholar] [CrossRef]
- Janssen, I.; Baumgartner, R.N.; Ross, R.; Rosenberg, I.H.; Roubenoff, R. Skeletal muscle cutpoints associated with elevated physical disability risk in older men and women. Am. J. Epidemiol. 2004, 159, 413–421. [Google Scholar] [CrossRef]
- Mohammad, A.; De Lucia Rolfe, E.; Sleigh, A.; Kivisild, T.; Behbehani, K.; Wareham, N.J.; Brage, S.; Mohammad, T. Validity of visceral adiposity estimates from DXA against MRI in Kuwaiti men and women. Nutr. Diabetes 2017, 7, e238. [Google Scholar] [CrossRef]
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.B.; Ross, R.R.; Garry, P.J.; Lindeman, R.D. Epidemiology of sarcopenia among the elderly in New Mexico. Am. J. Epidemiol. 1998, 147, 755–763. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2011.
- American College of Sports Medicine. American College of Sports Medicine Position Stand. Progression models in resistance training for healthy adults. Med. Sci. Sport. Exerc. 2014, 41, 687–708. [Google Scholar]
- Chlif, M.; Chaouachi, A.; Ahmaidi, S. Effect of aerobic exercise training on ventilatory efficiency and respiratory drive in obese subjects. Respir. Care 2017, 62, 936–946. [Google Scholar] [CrossRef] [PubMed]
- Beutel, M.; Thiede, R.; Wiltink, J.; Sobez, I. Effectiveness of behavioral and psychodynamic in-patient treatment of severe obesity—First results from a randomized study. Int. J. Obes. 2001, 25, S96–S98. [Google Scholar] [CrossRef]
- Compher, C.; Frankenfield, D.; Keim, N.; Roth-Yousey, L. Best Practice Methods to Apply to Measurement of Resting Metabolic Rate in Adults: A Systematic Review. J. Am. Diet. Assoc. 2006, 106, 881–903. [Google Scholar] [CrossRef]
- Weir, J.B. New methods for calculating metabolic rate with special reference to protein metabolism. J. Physiol. 1949, 109, 1–9. [Google Scholar] [CrossRef]
- Frayn, K.N. Calculation of substrate oxidation rates in vivo from gaseous exchange. J. Appl. Physiol. 2016, 121, 628–634. [Google Scholar] [CrossRef]
- Kwaifa, I.K.; Bahari, H.; Yong, Y.K.; Md Noor, S. Endothelial dysfunction in obesity-induced inflammation: Molecular mechanisms and clinical implications. Biomolecules 2020, 10, 291. [Google Scholar] [CrossRef] [PubMed]
- Lau, D.C.W.; Dhillon, B.; Yan, H.; Szmitko, P.E.; Verma, S. Adipokines: Molecular links between obesity and atheroslcerosis. Am. J. Physiol.-Hear. Circ. Physiol. 2005, 288, H2031–H2041. [Google Scholar] [CrossRef]
- Feinman, R.D.; Pogozelski, W.K.; Astrup, A.; Bernstein, R.K.; Fine, E.J.; Westman, E.C.; Accurso, A.; Frassetto, L.; Gower, B.A.; McFarlane, S.I.; et al. Dietary carbohydrate restriction as the first approach in diabetes management: Critical review and evidence base. Nutrition 2015, 31, 1–13, Erratum in Nutrition 2019, 62, 213. [Google Scholar] [CrossRef]
- Dashti, H.M.; Mathew, T.C.; Khadada, M.; Al-Mousawi, M.; Talib, H.; Asfar, S.K.; Behbahani, A.I.; Al-Zaid, N.S. Beneficial effects of ketogenic diet in obese diabetic subjects. Mol. Cell. Biochem. 2007, 302, 249–256. [Google Scholar] [CrossRef]
- Makki, K.; Froguel, P.; Wolowczuk, I. Adipose Tissue in Obesity-Related Inflammation and Insulin Resistance: Cells, Cytokines, and Chemokines. ISRN Inflamm. 2013, 2013, 139239. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro Volp, A.C.; Santos Silva, F.C.; Bressan, J. Hepatic Inflammatory Biomarkers and Its Link with Obesity and Chronic Diseases. Nutr. Hosp. 2015, 31, 1947–1956. [Google Scholar] [PubMed]
- Son, P.; Lewis, L. Hyperhomocysteinemia; StatPearls: Treasure Island, FL, USA, 2020. [Google Scholar]
- Stanger, O.; Herrmann, W.; Pietrzik, K.; Fowler, B.; Geisel, J.; Dierkes, J.; Weger, M. Clinical use and rational management of homocysteine, folic acid, and B vitamins in cardiovascular and thrombotic diseases. Z. Kardiol. 2004, 93, 439–453. [Google Scholar] [CrossRef] [PubMed]
- Zemel, M.B.; Shi, H.; Greer, B.; Dirienzo, D.; Zemel, P.C. Regulation of Adiposity by Dietary Calcium. FASEB J. 2000, 14, 1132–1138. [Google Scholar] [CrossRef]
- Shi, H.; Halvorsen, Y.-D.; Ellis, P.N.; Wilkison, W.O.; Zemel, M.B. Role of intracellular calcium in human adipocyte differentiation. Physiol. Genom. 2000, 2000, 75–82. [Google Scholar] [CrossRef]
- Tal, B.; Sack, J.; Yaron, M.; Shefer, G.; Buch, A.; Ben Haim, L.; Marcus, Y.; Shenkerman, G.; Sofer, Y.; Shefer, L.; et al. Increment in dietary potassium predicts weight loss in the treatment of the metabolic syndrome. Nutrients 2019, 11, 1256. [Google Scholar] [CrossRef]
- Cai, X.; Li, X.; Fan, W.; Yu, W.; Wang, S.; Li, Z.; Scott, E.M.; Li, X. Potassium and obesity/metabolic syndrome: A systematic review and meta-analysis of the epidemiological evidence. Nutrients 2016, 8, 183. [Google Scholar] [CrossRef]
- Damms-Machado, A.; Weser, G.; Bischoff, S.C. Micronutrient deficiency in obese subjects undergoing low calorie diet. Nutr. J. 2012, 11, 34. [Google Scholar] [CrossRef]
- Aigner, E.; Feldman, A.; Datz, C. Obesity as an emerging risk factor for iron deficiency. Nutrients 2014, 6, 3587–3600. [Google Scholar] [CrossRef]
- Feingold, K.; Grunfeld, C. Obesity and dyslipidemia. In Endotext; Feingold, K., Anawalt, B., Boyce, B., Eds.; MDText.com Inc.: South Dartmouth, MA, USA, 2018. [Google Scholar]
- Dattilo, A.M.; Kris-Etherton, P.M. Effects of Weight Reduction on Blood Lipids and Lipoproteins: A Meta-Analysis. Am. J. Clin. Nutr. 1992, 56, 320–328. [Google Scholar] [CrossRef]
- Bosello, O.; Cominacini, L.; Zocca, I.; Garbin, U.; Compri, R.; Davoli, A.; Brunetti, L. Short- and long-term effects of hypocaloric diets containing proteins of different sources on plasma lipids and apoproteins of obese subjects. Ann. Nutr. Metab. 1988, 32, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Ko, H.; Kim, J.; Kim, M. The Impact of Very Low-Calorie Diet-Induced Weight Loss on Changes in the Serum Vitamin D Levels, Insulin Resistance, and Inflammatory Biomarkers in Overweight Korean Women. J. East Asian Soc. Diet. Life 2019, 29, 238–252. [Google Scholar] [CrossRef]
- Rolland, C.; Broom, I. The Effects of Very-Low-Calorie Diets on HDL: A Review. Cholesterol 2011, 2011, 30278. [Google Scholar] [CrossRef] [PubMed]
- Keller, U. Nutritional Laboratory Markers in Malnutrition. J. Clin. Med. 2019, 8, 775. [Google Scholar] [CrossRef]
- Nguyen, D.T.; Nguyen, T.T.H.; Van Nguyen, P.; Huynh, K.K.; Tung Bui, H.T. Evaluation of malnutrition among elderly people above 75 years of age. J. Crit. Rev. 2019, 7, 74–77. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| (A) | ||
| Characteristic | Minimum–Maximum | |
| Age (years) (n = 151) | 18–81 | 69.38 (14.1) |
| Gender (n = 151) | ||
| Male | 49 (32.5%) | |
| Female | 102 (67.5%) | |
| Duration of hospitalisation (days) (n = 148) | 17–91 | 47.47 (15.6) |
| * BMR (mean Kcal/day/kgBW) (n = 51) | 30.7–70.9 | 1490.76 (427.3) |
| RQ (n = 48) | 0.64–0.92 | 0.794 (0.09) |
| (B) | ||
| Characteristic | Minimum–Maximum | |
| Anthropometric Measurements | ||
| BMI (kg/m2) (n = 151) | 30.7–70.9 | 41.87 (7.1) |
| Class I | 23 (15.3%) | |
| Class II | 41 (27.3%) | |
| Class III | 86 (57.3%) | |
| Arm Circumference (cm) (n = 99) | 28–58 | 37.3 (4.3) |
| Calf Circumference (cm) (n = 99) | 32–62 | 42.6 (5) |
| Waist Circumference (cm) (n = 151) | 94–164 | 122.99 (14.1) |
| Hips Circumference (cm) (n = 143) | 105.5–162 | 127.6 (12.4) |
| DXA Measurements | ||
| FFM (g) (n = 144) | 23,218.0–82,728.0 | 51,407.4 (10,847.9) |
| FM (g) (n = 144) | 13,184.0–84,666.0 | 49,220.3 (11,468.6) |
| FM (%) (n = 144) | 34.2–61.5 | 48.9 (5.7) |
| FFMI (n = 113) | 14,749.2–28454.2 | 20,046.5 (2460) |
| FMI (n = 114) | 4632.5–31,098.6 | 19,225.1 (4621.1) |
| Weight (DXA) (n = 144) | 68.3–157.1 | 103.7 (18.9) |
| VAT (g) (n = 111) | 960–5550 | 2398.7 (943.2) |
| SMI (kg/m2) (n = 142) | 6.89–15.7 | 9.7 (1.5) |
| T-Score Femur (n = 96) | −2.5–2.5 | −0.312 (1.3) |
| (C) | ||
| Parameter | Reference Minimum–Maximum | |
| Folic acid (ng/mL) (n = 105) | 1.3–40 | 8.1 (8.3) |
| Normal (2.7–17) | 90 (85.7%) | |
| Low | 7 (6.7%) | |
| High | 8 (7.6%) | |
| Low | 16 (14.3%) | |
| Vitamin B12 (ng/mL) (n = 108) | 100–833 | 350.1 (143.2)) |
| Normal (200–900) | 93 (86.1%) | |
| Low | 15 (13.9%) | |
| Transferrin (mg/dL) (n = 95) | 68–441 | 258.8 (57.5) |
| Normal (170–370) | 90 (94.7%) | |
| Low | 1 (1.1%) | |
| High | 4 (4.2%) | |
| Vitamin D (ng/mL) (n = 102) | 3–62.7 | 19.2 (12.8) |
| Normal (30–100) | 20 (19.6%) | |
| Insufficient (10–30) | 55 (53.9%) | |
| Deficient (<10) | 27 (26.5%) | |
| ESR (mm/h) (n = 102) | 1–77 | 22.96 (18) |
| Normal Males (0–20) Females (0–30) | 68 (66.7%) | |
| High | 35 (34.3%) | |
| CRP (mg/L) (n = 121) | 0.01–5.45 | 0.8 (1.04) |
| Normal (0–3) | 115 (95%) | |
| High | 6 (4%) | |
| Homocysteine (µmol/L) (m = 97) | 6.8–101.2 | 19.5 (12.4) |
| Normal (<15) | 30 (30.6%) | |
| Moderate (15–30) | 64 (65.3%) | |
| Intermediate (30–100) | 3 (3.1%) | |
| High (>100) | 1 (1%) | |
| Glucose (mg/dL) (n = 142) | 66–253 | 101.13 (28.7) |
| Low (<79) | 13 (9.2%) | |
| Normal (80–100) | 82 (57.7%) | |
| Pre-diabetic (101–126) | 31 (21.8%) | |
| Diabetic (>126) | 16 (11.3%) | |
| Insulin (mcIU/mL) (n = 114) | 1.76–49.50 | 16.2 (8.9) |
| Normal (2.6–24.9) | 95 (83.5%) | |
| Low | 1 (0.9%) | |
| High | 18 (15.7%) | |
| HOMA-IR (mass units) (n = 112) | 0.89–15.03 | 4.1 (2.7) |
| Normal (0.5–1.8) | 17 (15.5%) | |
| Early insulin resistance (1.9–2.9) | 30 (25.5%) | |
| Significant insulin resistance (>2.9) | 65 (59.1%) | |
| Pre-albumin (mg/dL) (n = 127) | 7–38 | 23.9 (5.1) |
| Normal (15–36) | 121 (95.3%) | |
| Low | 3 (2.3%) | |
| High | 3 (2.3%) | |
| Albumin (g) (n = 137) | 2.25–4.97 | 3.9 (0.38) |
| Normal (≥3.5) | 122 (88.7%) | |
| Low | 17 (11.3%) | |
| (D) | ||
| Parameter | Minimum–Maximum | |
| Uric acid (mg/dL) (n = 139) | 3.7–10.5 | 6.5 (1.5) |
| Normal (3–6) | 87 (62.6%) | |
| High | 52 (37.4%) | |
| Creatinine (mg/dL) (n = 139) | 0.58–2.07 | 0.89 (0.27) |
| Normal Males (0.7–1.3) Females (0.6–1.1) | 119 (85.6%) | |
| Low | 4 (2.9%) | |
| High | 16 (11.5%) | |
| Total bilirubin (mg/dL) (n = 134) | 0.18–2.56 | 0.75 (0.37) |
| Normal | 123 (91.8%) | |
| High | 11 (8.2%) | |
| Na (mEq/L) (n = 140) | 135–144 | 139.6 (2) |
| Normal (135–145) | 140 (100%) | |
| K (mmol/L) (n = 140) | 2.9–5.6 | 4.4 (0.43) |
| Normal (3.5–5.0) | 125 (89.3%) | |
| Low | 2 (1.4%) | |
| High | 13 (9.3%) | |
| Cl (mmol/L) (n = 139) | 92–116 | 103.7 (3.5) |
| Normal (96–106) | 110 (79.1%) | |
| Low | 2 (1.4%) | |
| High | 27 (19.4%) | |
| Ca (mg/dL) (n = 138) | 8–10.6 | 9.3 (0.5) |
| Normal (8.5–10.5) | 132 (95.7%) | |
| Low | 5 (3.6%) | |
| High | 1 (0.7%) | |
| Total Cholesterol (mg/dL) (n = 140) | 63–372 | 185.9 (43.2) |
| Normal (<200) | 99 (70.7%) | |
| High (200–240) | 29 (20.7%) | |
| Very high (>240) | 12 (8.6%) | |
| HDL (mg/dL) (n = 140) | 24–80 | 45.4 (12.1) |
| Normal (>60) | 18 (12.9%) | |
| Low (40–60) | 60 (42.9%) | |
| Very low (<40) | 62 (44.3%) | |
| Triglycerides (mg/dL) (n = 140) | 40–378 | 142.5 (67.7) |
| Normal (<150) | 94 (67.1%) | |
| Borderline high (150–200) | 25 (17.9%) | |
| High (201–500) | 21 (15%) | |
| LDL (mg/dL) (n = 138) | 25–304.8 | 112 (42.1) |
| Normal | 104 (75.4%) | |
| High | 27 (19.6%) | |
| Very high | 7 (5.1%) | |
| ApoA (mg/dL) (n = 132) | 84–250 | 134.8 (27.3) |
| Normal Males (≥120) Females (≥140) | 59 (44.7%) | |
| Low | 73 (55.3%) | |
| ApoB (mg/dL) (n = 132) | 26–209 | 102.7 (29) |
| Normal (<99) | 67 (50.8%) | |
| High (100–139) | 52 (39.4%) | |
| Very high (≥140) | 13 (9.8%) | |
| (E) | ||
| Parameter | Minimum–Maximum | |
| AST (IU/L) (n = 139) | 10–109 | 21.5 (11.5) |
| Normal Males (10–40) Females (9–32) | 130 (93.5%) | |
| High | 9 (6.5%) | |
| ALT (U/L) (n = 139) | 7–204 | 28.3 (22.8) |
| Normal (<56) | 131 (94.2%) | |
| High | 8 (5.8%) | |
| GGT (U/L) (n = 139) | 6–170 | 35 (30.3) |
| Normal (<48) | 114 (82.0%) | |
| High | 25 (18%) | |
| ALP (U/L) (n = 120) | 3.5–189 | 66.2 (26.7) |
| Normal (20–140) | 116 (76.8%) | |
| Low | 2 (1.3%) | |
| High | 2 (1.3%) | |
| Lipase (U/L) (n = 110) | 4–128 | 25.6 (17.8) |
| Normal (<70) | 107 (97.3%) | |
| High | 3 (2.7%) | |
| Amylase (U/L) (n = 118) | 18–115 | 51.7 (19.7) |
| Normal (23–140) | 115 (97.5%) | |
| High | 3 (2.5%) | |
| TSH (µU/mL) (n = 109) | 0–9.32 | 2.2 (1.5) |
| Normal (0.4–4.0) | 96 (88.1%) | |
| Low | 6 (5.5%) | |
| High | 7 (6.4%) | |
| FT3 (pmol/L) (n = 49) | 1.94–3.84 | 2.9 (0.5) |
| Normal (3.5–7.8) | 44 (89.8%) | |
| Low | 5(10.2%) | |
| FT4 (pmol/L) (n = 57) | 7.7–18 | 12.4 (1.8) |
| Normal (9–25) | 55 (96.5%) | |
| Low | 2 (3.5%) | |
| (F) | ||
| Parameter | Minimum–Maximum | |
| WBC (K/µL) (n = 138) | 3.6–14.2 | 7 (1.8) |
| Normal (4–11) | 133 (96.4%) | |
| Low | 2 (1.4%) | |
| High | 3 (2.2%) | |
| Lymphocytes (%) (n = 135) | 33.2 (7.3) | |
| RBC (M/µL) (n = 138) | 3.2–7.04 | 4.7 (0. 6) |
| Normal Males (4.7–6.1) Females (4.2–5.4) | 100 (72.5%) | |
| Low | 31 (22.5%) | |
| High | 7 (5.1%) | |
| Hb (g/dL) (n = 138) | 10.1–17.9 | 13.4 (1.4) |
| Normal Males (13.5–17.5) Females (12–15.5) | 106 (76.8%) | |
| Low | 30 (21.7%) | |
| High | 2 (1.5%) | |
| HCT (%) (n = 138) | 30.8–54.8 | 41.1 (4.1) |
| Normal Males (38.3–48.6)) Females (35.5–44.9)) | 106 (76.8%) | |
| Low | 14 (10.2%) | |
| High | 18(13%) | |
| MCV (fL) (n = 138) | 60.8–104.7 | 87.2 (6.3) |
| Normal (80–96) | 119 (86.2%) | |
| Low | 11 (8%) | |
| High | 8 (5.8%) | |
| PLT (n = 138) | 66–440 | 253.6 (65.3) |
| Normal (150–400) | 129 (93.5%) | |
| Low | 6 (4.3%) | |
| High | 3 (2.2%) | |
| Outcome | Mean Difference (95%CI) |
|---|---|
| BMR (cal/day) (n = 51) | −121.4 (−188.5; −54.3) |
| RQ (n = 48) | 0.3 (0.0; 0.0) |
| Anthropometric Measurements | |
| BMI (points) (n = 151) | −2.7 (−2.9; −2.5) |
| Arm Circumference (cm) (n = 99) | −1.9 (−2.3; −1.4) |
| Calf Circumference (cm) (n = 99) | −1.2 (−1.4; −1.0) |
| Waist Circumference (cm) (n = 151) | −6.4 (−7.0; −5.9) |
| Hips Circumference (cm) (n = 143) | −4.9 (−5.5; −4.2) |
| DXA Measurements | |
| FFM (g) (n = 144) | −1772.4 (−2780.5; −764.3) |
| FM (g) (n = 144) | −4446.9 (−4875.0; −4018.8) |
| FM (%) (n = 144) | −2.0 (−2.4; −1.7) |
| FFMI (n = 113) | −592.4 (−1010.7; −174.2) |
| FMI (n = 114) | −1824.5( −2146.0; −1503.0) |
| Weight (DXA) (n = 144) | −5.9 (−6.4; −5.3) |
| VAT (g) (n = 111) | −339.7 (−427.3; −252.2) |
| SMI (kg/m2) (n = 142) | −0.17 (−0.3; 0.0) |
| Biochemical parameters | |
| Folate (ng/mL) (n = 105) | 4.7 (2.9; 6.5) |
| Iron (µg/dL) (n = 112) | −14.9 (−18.1; −11.7) |
| Vitamin B12 (ng/mL) (n = 108) | 35.4 (11.6; 59.2) |
| Transferrin (mg/dL) (n = 95) | −26.0 (−30.8; −21.1) |
| Vitamin D (ng/mL) (n = 102) | 13.0 (10.5; 15.6) |
| ESR (mm/hr) (n = 102) | 1.4 (−0.8; 3.6) |
| CRP (mg/L) (n = 121) | −0.2 (−0.4; −0.1) |
| Glucose (mg/dL) (n = 142) | −11.3 (−13.4; −9.1) |
| Insulin (mcIU/mL) (n = 114) | −2.5 (−4.2; −0.9) |
| HOMA-IR (mass units) (n = 112) | −1.1 (−1.5; −0.7) |
| Uric acid (mg/dL) (n = 139) | −0.1 (−0.3; 0.1) |
| Creatinine (mg/dL) (n = 139) | 0.1 (0.0; 0.1) |
| Na (mEq/L) (n = 140) | 0.3 (−0.0; 0.6) |
| K (mmol/L) (n = 140) | −0.0 (−0.1; 0.0) |
| Cl (mmol/L) (n = 139) | 0.5 (0.0; 0.9) |
| Ca (mg/dL) (n = 138) | 0.1 (0.0; 0.2) |
| Total Cholesterol (mg/dL) (n = 140) | −25.0 (−29.2; −20.7) |
| HDL (mg/dL) (n = 140) | −4.7 (−5.7; −3.8) |
| Triglycerides (mg/dL) (n = 140) | −22.8 (−29.3; −16.3) |
| LDL (mg/dL) (n = 138) | −12.5 (−17.0; −8.0) |
| ApoA (mg/dL) (n = 132) | −15.7 (−18.1; −13.4) |
| ApoB (mg/dL) (n = 132) | −14.2 (−17.1; −11.3) |
| AST (IU/L) (n = 139) | −1.2 (−2.2; −0.2) |
| ALT (U/L) (n = 140) | −1.2 (−3.2; 0.8) |
| GGT (U/L) (n = 139) | −9.1 (−12.7; −5.5) |
| Pre-albumin (mg/dL) (n = 127) | −1.8 (−2.3; −1.3) |
| ALP (U/L) (n = 120) | −5.7 (−8.4; −3.1) |
| Total bilirubin (mg/dL) (n = 134) | −0.1 (−0.2; −0.1) |
| Lipase (U/L) (n = 109) | 2.5 (−0.5; 5.5) |
| Amylase (U/L) (n = 118) | 4.7 (2.4; 6.9) |
| Homocystein (µmol/L) (n = 97) | −2.9 (−4.0; −1.9) |
| TSH (µU/mL) (n = 109) | 0.5 (−0.4; 1.5) |
| FT3 (pmol/L) (n = 48) | −0.0 (−0.1; 0.1) |
| FT4 (pmol/L) (n = 57) | 0.4 (−0.0; 0.9) |
| Albumin (g) (n = 137) | −0.1 (−0.1; −0.0) |
| WBC (K/µL) (n = 138) | −0.7 (−0.9; −0.5) |
| Lymphocytes (%) (n = 135) | 2.8 (1.7; 3.8) |
| RBC (M/µL) (n = 138) | −0.1 (−0.2; −0.1) |
| Hb (g/dL) (n = 138) | −0.2 (−0.3; −0.1) |
| HCT (%) (n = 138) | −0.9 (−1.5; −0.3) |
| MCV (fL) (n = 138) | 0.4 (0.1; 0.8) |
| PLT (n = 138) | −24.3 (−29.1; −19.4) |
| Outcome | B | p-Value | CI95% |
|---|---|---|---|
| ∆ HOMA-IR | 1.322 | <0.001 | 1.218; 1.426 |
| ∆ Ca | −5.858 | 0.001 | −7.093; −4.623 |
| ∆ K | −1.499 | 0.017 | −2.479; −0.519 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abbas, H.; Perna, S.; Shah, A.; Gasparri, C.; Rondanelli, M. Efficacy and Safety of a Long-Term Multidisciplinary Weight Loss Intervention under Hospitalization in Aging Patients with Obesity: An Open Label Study. Nutrients 2022, 14, 3416. https://doi.org/10.3390/nu14163416
Abbas H, Perna S, Shah A, Gasparri C, Rondanelli M. Efficacy and Safety of a Long-Term Multidisciplinary Weight Loss Intervention under Hospitalization in Aging Patients with Obesity: An Open Label Study. Nutrients. 2022; 14(16):3416. https://doi.org/10.3390/nu14163416
Chicago/Turabian StyleAbbas, Hanan, Simone Perna, Afzal Shah, Clara Gasparri, and Mariangela Rondanelli. 2022. "Efficacy and Safety of a Long-Term Multidisciplinary Weight Loss Intervention under Hospitalization in Aging Patients with Obesity: An Open Label Study" Nutrients 14, no. 16: 3416. https://doi.org/10.3390/nu14163416