
Lean Mass Improvement from Nutrition Education and Protein Supplementation among Rural Indian Women Living with HIV/AIDS: Results from Cluster Randomized Factorial Trial at 18-Month Follow-Up

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
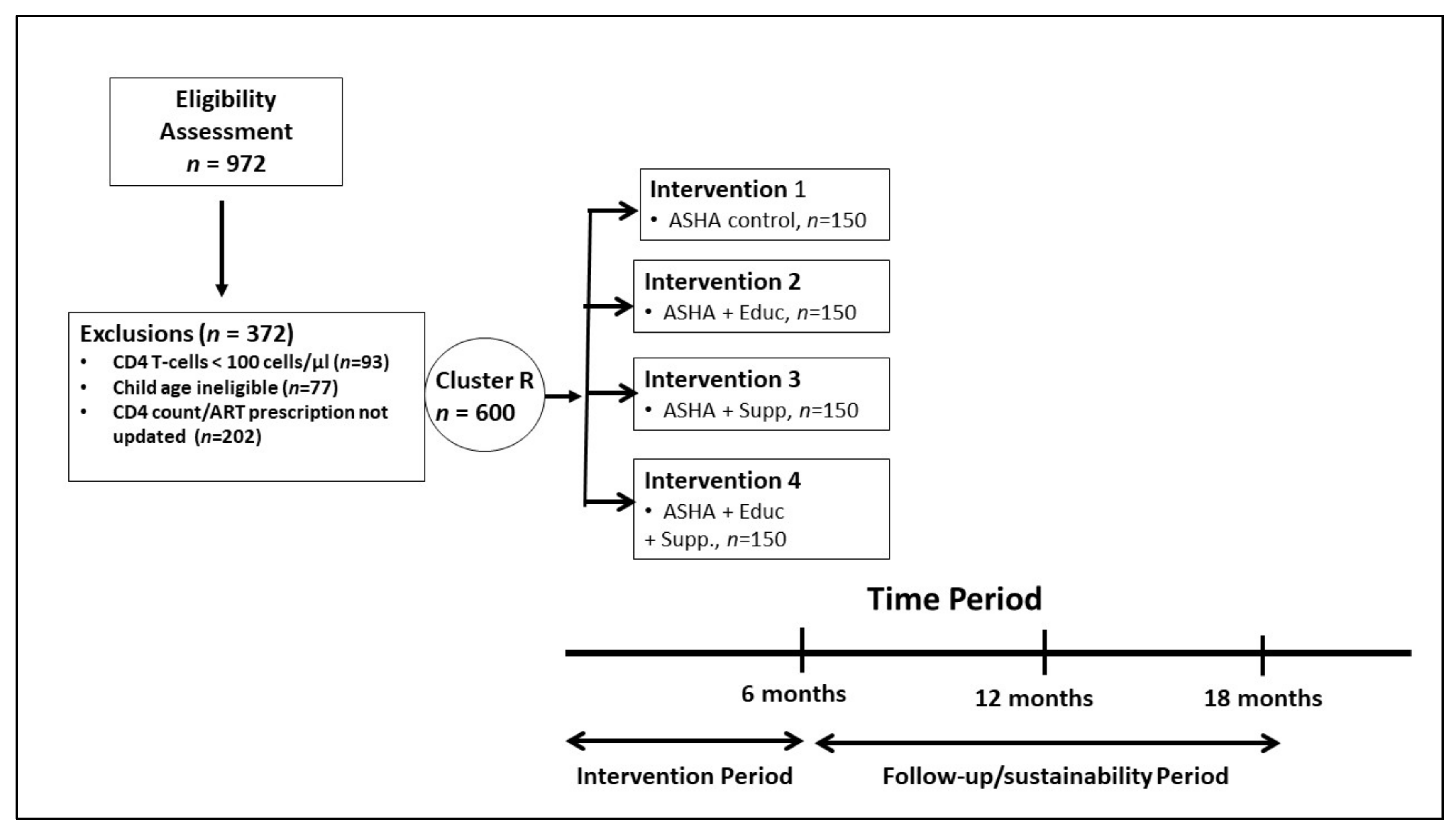
2.1. Design
2.2. Sample and Setting
2.3. Asha Selection and Training
2.4. Description of Sampling and Asha Nutrition Intervention Programs
2.5. Assessment Measures
2.6. Statistical Methods
2.6.1. Sample Size Estimation
2.6.2. Data Collection
2.6.3. Data Analysis
3. Results
3.1. Overall Study Sample
3.2. Study Sample by Group
3.3. Anthropometric Outcomes
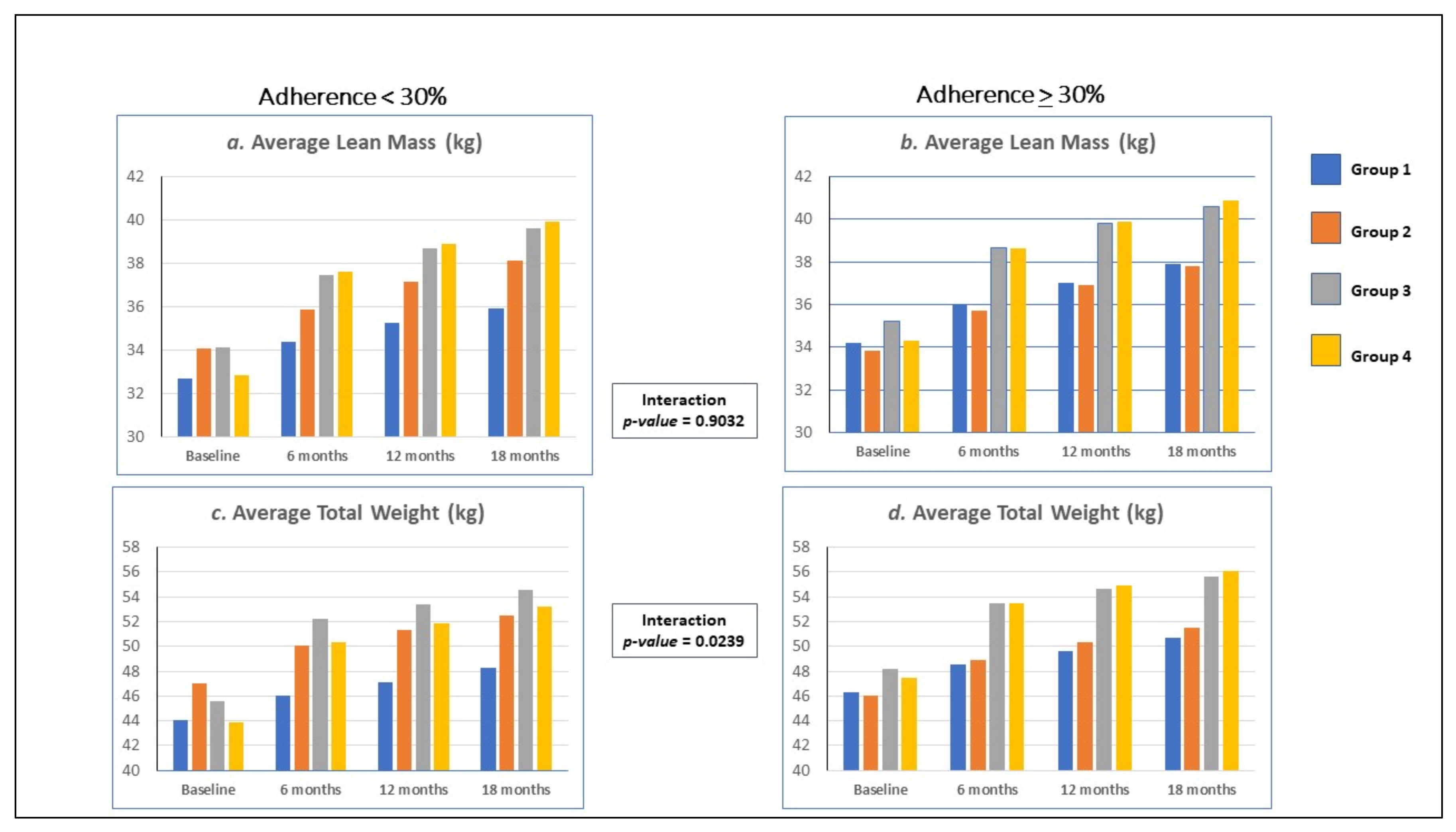
3.4. Anthropometric Outcomes: Stratified by Adherence to ART
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cunningham-Rundles, S.; McNeeley, D.F.; Moon, A. Mechanisms of nutrient modulation of the immune response. J. Allergy Clin. Immunol. 2005, 115, 1119–1128. [Google Scholar] [CrossRef] [PubMed]
- Grobler, L.; Siegfried, N.; Visser, M.E.; Mahlungulu, S.S.; Volmink, J. Nutritional Interventions for Reducing Morbidity and Mortality in People with HIV. Cochrane Database Syst. Rev. 2013. Available online: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD004536.pub3/full (accessed on 29 December 2021). [CrossRef] [PubMed] [Green Version]
- Schaible, U.E.; Kaufmann, S.H. Malnutrition and infection: Complex mechanisms and global impacts. PLoS Med. 2007, 4, e115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beisel, W.R. Nutrition in pediatric HIV infection: Setting the research agenda. Nutrition and immune function: Overview. J. Nutr. 1996, 126 (Suppl. S10), 2611S–2615S. [Google Scholar] [CrossRef] [Green Version]
- Gupta, A.; Nadkarni, G.; Yang, W.T.; Chandrasekhar, A.; Gupte, N.; Bisson, G.P.; Hosseinipour, M.; Gummadi, N. Early mortality in adults initiating antiretroviral therapy (ART) in low- and middle-income countries (LMIC): A systematic review and meta-analysis. PLoS ONE 2011, 6, e28691. [Google Scholar] [CrossRef] [Green Version]
- Chandrasekhar, A.; Gupta, A. Nutrition and disease progression pre-highly active antiretroviral therapy (HAART) and post-HAART: Can good nutrition delay time to HAART and affect response to HAART? Am. J. Clin. Nutr. 2011, 94, 1703S–1715S. [Google Scholar] [CrossRef] [Green Version]
- De Pee, S.; Semba, R.D. Role of nutrition in HIV infection: Review of evidence for more effective programming in resource-limited settings. Food Nutr. Bull. 2010, 31, S313–S344. [Google Scholar] [CrossRef] [Green Version]
- Olsen, M.F.; Abdissa, A.; Kæstel, P.; Tesfaye, M.; Yilma, D.; Girma, T.; Wells, J.C.; Ritz, C.; Mølgaard, C.; Michaelsen, K.F.; et al. Effects of nutritional supplementation for HIV patients starting antiretroviral treatment: Randomised controlled trial in Ethiopia. BMJ (Clin. Res. Ed.) 2014, 348, g3187. [Google Scholar] [CrossRef] [Green Version]
- Nyamathi, A.; Sinha, S.; Ganguly, K.K.; Ramakrishna, P.; Suresh, P.; Carpenter, C.L. Impact of protein supplementation and care and support on body composition and CD4 count among HIV-infected women living in rural India: Results from a randomized pilot clinical trial. AIDS Behav. 2013, 17, 2011–2021. [Google Scholar] [CrossRef]
- Humphrey, J.H.; Quinn, T.; Fine, D.; Lederman, H.; Yamini-Roodsari, S.; Wu, L.S.; Moeller, S.; Ruff, A.J. Short-term effects of large-dose vitamin A supplementation on viral load and immune response in HIV-infected women. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 1999, 20, 44–51. [Google Scholar] [CrossRef] [Green Version]
- Kelly, P.; Katubulushi, M.; Todd, J.; Banda, R.; Yambayamba, V.; Fwoloshi, M.; Zulu, I.; Kafwembe, E.; Yavwa, F.; Sanderson, I.R.; et al. Micronutrient supplementation has limited effects on intestinal infectious disease and mortality in a Zambian population of mixed HIV status: A cluster randomized trial. Am. J. Clin. Nutr. 2008, 88, 1010–1017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baum, M.K.; Lai, S.; Sales, S.; Page, J.B.; Campa, A. Randomized, controlled clinical trial of zinc supplementation to prevent immunological failure in HIV-infected adults. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2010, 50, 1653–1660. [Google Scholar] [CrossRef]
- Hurwitz, B.E.; Klaus, J.R.; Llabre, M.M.; Gonzalez, A.; Lawrence, P.J.; Maher, K.J.; Greeson, J.M.; Baum, M.K.; Shor-Posner, G.; Skyler, J.S.; et al. Suppression of human immunodeficiency virus type 1 viral load with selenium supplementation: A randomized controlled trial. Arch. Intern. Med. 2007, 167, 148–154. [Google Scholar] [CrossRef] [PubMed]
- McDermott, A.Y.; Terrin, N.; Wanke, C.; Skinner, S.; Tchetgen, E.; Shevitz, A.H. CD4+ cell count, viral load, and highly active antiretroviral therapy use are independent predictors of body composition alterations in HIV-infected adults: A longitudinal study. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2005, 41, 1662–1670. [Google Scholar] [CrossRef]
- Mangili, A.; Murman, D.H.; Zampini, A.M.; Wanke, C.A. Nutrition and HIV infection: Review of weight loss and wasting in the era of highly active antiretroviral therapy from the nutrition for healthy living cohort. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2006, 42, 836–842. [Google Scholar] [CrossRef] [Green Version]
- Stampfer, M.J.; Buring, J.E.; Willett, W.; Rosner, B.; Eberlein, K.; Hennekens, C.H. The 2 × 2 factorial design: Its application to a randomized trial of aspirin and carotene in U.S. physicians. Stat. Med. 1985, 4, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Nyamathi, A.; Hanson, A.Y.; Salem, B.E.; Sinha, S.; Ganguly, K.K.; Leake, B.; Yadav, K.; Marfisee, M. Impact of a rural village women (Asha) intervention on adherence to antiretroviral therapy in southern India. Nurs. Res. 2012, 61, 353–362. [Google Scholar] [CrossRef] [Green Version]
- Nyamathi, A.; Salem, B.; Ernst, E.J.; Keenan, C.; Suresh, P.; Sinha, S.; Ganguly, K.; Ramakrishnan, P.; Liu, Y. Correlates of Adherence among Rural Indian Women Living with HIV/AIDS. J. HIV/AIDS Soc. Serv. 2012, 11, 327–345. [Google Scholar] [CrossRef] [Green Version]
- Hurley, J.C. How the Cluster-randomized Trial “Works”. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, 70, 341–346. [Google Scholar] [CrossRef]
- Nyamathi, A.M.; Carpenter, C.L.; Ekstrand, M.L.; Yadav, K.; Garfin, D.R.; Muniz, L.C.; Kelley, M.; Sinha, S. Randomized controlled trial of a community-based intervention on HIV and nutritional outcomes at 6 months among women living with HIV/AIDS in rural India. AIDS 2018, 32, 2727–2737. [Google Scholar] [CrossRef]
- Nyamathi, A.N.; Shin, S.S.; Sinha, S.; Carpenter, C.L.; Garfin, D.R.; RK, P.; Yadav, K.; Ekstrand, M.L. Sustained Effect of a Community-based Behavioral and Nutrition Intervention on HIV-related Outcomes Among Women Living with HIV in Rural India: A Quasi-experimental Trial. J. Acquir. Immune Defic. Syndr. (1999) 2019, 81, 429–438. [Google Scholar] [CrossRef]
- Ekstrand, M.L.; Chandy, S.; Heylen, E.; Steward, W.; Singh, G. Developing useful highly active antiretroviral therapy adherence measures for India: The Prerana study. J. Acquir. Immune Defic. Syndr. (1999) 2010, 53, 415–416. [Google Scholar] [CrossRef] [Green Version]
- Ekstrand, M.L.; Shet, A.; Chandy, S.; Singh, G.; Shamsundar, R.; Madhavan, V.; Saravanan, S.; Heylen, E.; Kumarasamy, N. Suboptimal adherence associated with virological failure and resistance mutations to first-line highly active antiretroviral therapy (HAART) in Bangalore, India. Int. Health 2011, 3, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Steward, W.T.; Chandy, S.; Singh, G.; Panicker, S.T.; Osmand, T.A.; Heylen, E.; Ekstrand, M.L. Depression is not an inevitable outcome of disclosure avoidance: HIV stigma and mental health in a cohort of HIV-infected individuals from Southern India. Psychol. Health Med. 2011, 16, 74–85. [Google Scholar] [CrossRef]
- Ekstrand, M.; Solomon, D.; Gopalkrishnan, S.; Krishman, A.K.; Kumarasamy, N. (Eds.) Alcohol use, partner violence and sexual risk among South India female sex workers: Implications for interventions. In Proceedings of the 2nd International Conference on Alcohol and HIV: Insights from Interventions, New Delhi, India, 28–30 September 2010. [Google Scholar]
- Endicott, J.; Nee, J.; Harrison, W.; Blumenthal, R. Quality of Life Enjoyment and Satisfaction Questionnaire: A new measure. Psychopharmacol. Bull. 1993, 29, 321–326. [Google Scholar]
- Coates, J.; Swindale, A.; Bilinsky, P. Household Food Insecurity Access Scale (HFIAS) for Measurement of Household Food Access: Indicator Guide; USAID, Food and Nutrition Technical Assistance Project: Washington, DC, USA, 2007. [Google Scholar]
- Weiser, S.D.; Young, S.L.; Cohen, C.R.; Kushel, M.B.; Tsai, A.C.; Tien, P.C.; Hatcher, A.M.; Frongillo, E.A.; Bangsberg, D.R. Conceptual framework for understanding the bidirectional links between food insecurity and HIV/AIDS. Am. J. Clin. Nutr. 2011, 94, 1729S–1739S. [Google Scholar] [CrossRef]
- Vargas Puello, V.; Alvarado Orellana, S.; Atalah Samur, E. Food insecurity among elderly people in 15 districts of the Great Santiago area; an unresolved issue. Nutr. Hosp. 2013, 28, 1430–1437. [Google Scholar]
- Pasricha, S.R.; Black, J.; Muthayya, S.; Shet, A.; Bhat, V.; Nagaraj, S.; Prashanth, N.S.; Sudarshan, H.; Biggs, B.A.; Shet, A.S. Determinants of anemia among young children in rural India. Pediatrics 2010, 126, e140–e149. [Google Scholar] [CrossRef] [Green Version]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Nyamathi, A.; Heravian, A.; Zolt-Gilburne, J.; Sinha, S.; Ganguly, K.; Liu, E.; Ramakrishnan, P.; Marfisee, M.; Leake, B. Correlates of depression among rural women living with AIDS in Southern India. Issues Ment. Health Nurs. 2011, 32, 385–391. [Google Scholar] [CrossRef] [Green Version]
- Steward, W.T.; Herek, G.M.; Ramakrishna, J.; Bharat, S.; Chandy, S.; Wrubel, J.; Ekstrand, M.L. HIV-related stigma: Adapting a theoretical framework for use in India. Soc. Sci. Med. 2008, 67, 1225–1235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekstrand, M.L.; Bharat, S.; Ramakrishna, J.; Heylen, E. Blame, symbolic stigma and HIV misconceptions are associated with support for coercive measures in urban India. AIDS Behav. 2012, 16, 700–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherbourne, C.D.; Stewart, A.L. The MOS social support survey. Soc. Sci. Med. 1991, 32, 705–714. [Google Scholar] [CrossRef]
- Giordano, T.P.; Guzman, D.; Clark, R.; Charlebois, E.D.; Bangsberg, D.R. Measuring adherence to antiretroviral therapy in a diverse population using a visual analogue scale. HIV Clin. Trials 2004, 5, 74–79. [Google Scholar] [CrossRef] [PubMed]
- WHO. Physical Status: The Use and Interpretation of Anthropometry; WHO Technical Report Series 854; WHO: Geneva, Switzerland, 1995; pp. 1–416. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.F.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Kapur, A.; Kapur, K. Computer aided interactive nutrition assistant—A unique tool for improving diabetes nutrition management. Diabetologia 1977, 40, 1519. [Google Scholar]
- Daniel, C.R.; Prabhakaran, D.; Kapur, K.; Graubard, B.I.; Devasenapathy, N.; Ramakrishnan, L.; George, P.S.; Shetty, H.; Ferrucci, L.M.; Yurgalevitch, S.; et al. A cross-sectional investigation of regional patterns of diet and cardio-metabolic risk in India. Nutr. J. 2011, 10, 12. [Google Scholar] [CrossRef] [Green Version]
- Daniel, C.R.; Kapur, K.; McAdams, M.J.; Dixit-Joshi, S.; Devasenapathy, N.; Shetty, H.; Hariharan, S.; George, P.S.; Mathew, A.; Sinha, R. Development of a field-friendly automated dietary assessment tool and nutrient database for India. Br. J. Nutr. 2014, 111, 160–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hebert, J.R.; Gupta, P.C.; Mehta, H.; Ebbeling, C.B.; Bhonsle, R.R.; Varghese, R. Sources of variability in dietary intake in two distinct regions of rural India: Implications for nutrition study design and interpretation. Eur. J. Clin. Nutr. 2000, 54, 479–486. [Google Scholar] [CrossRef] [Green Version]
- Chang, E.; Sekhar, R.; Patel, S.; Balasubramanyam, A. Dysregulated energy expenditure in HIV-infected patients: A mechanistic review. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2007, 44, 1509–1517. [Google Scholar] [CrossRef] [Green Version]
- Ambrus, J.L., Sr.; Ambrus, J.L., Jr. Nutrition and infectious diseases in developing countries and problems of acquired immunodeficiency syndrome. Exp. Biol. Med. 2004, 229, 464–472. [Google Scholar] [CrossRef]
- McDermott, A.Y.; Shevitz, A.; Knox, T.; Roubenoff, R.; Kehayias, J.; Gorbach, S. Effect of highly active antiretroviral therapy on fat, lean, and bone mass in HIV-seropositive men and women. Am. J. Clin. Nutr. 2001, 74, 679–686. [Google Scholar] [CrossRef] [Green Version]
- Agrawal, S.; Millett, C.J.; Dhillon, P.K.; Subramanian, S.V.; Ebrahim, S. Type of vegetarian diet, obesity and diabetes in adult Indian population. Nutr. J. 2014, 13, 89. [Google Scholar] [CrossRef] [Green Version]
- Misra, A.; Rastogi, K.; Joshi, S.R. Whole grains and health: Perspective for Asian Indians. J. Assoc. Physicians India 2009, 57, 155–162. [Google Scholar]
- Evans, W.J.; Hellerstein, M.; Orwoll, E.; Cummings, S.; Cawthon, P.M. D3-Creatine dilution and the importance of accuracy in the assessment of skeletal muscle mass. J. Cachexia Sarcopenia Muscle 2019, 10, 14–21. [Google Scholar] [CrossRef] [Green Version]
- Treyzon, L.; Chen, S.; Hong, K.; Yan, E.; Carpenter, C.L.; Thames, G.; Bowerman, S.; Wang, H.J.; Elashoff, R.; Li, Z. A controlled trial of protein enrichment of meal replacements for weight reduction with retention of lean body mass. Nutr. J. 2008, 7, 23. [Google Scholar] [CrossRef] [Green Version]
- Carpenter, C.L.; Yan, E.; Chen, S.; Hong, K.; Arechiga, A.; Kim, W.S.; Deng, M.; Li, Z.; Heber, D. Body fat and body-mass index among a multiethnic sample of college-age men and women. J. Obes. 2013, 2013, 790654. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Continuous Variables | Total Study Population | ASHA (AS) Control | Nutr. Education + AS | Nutrition + AS | Nutr. Educ + AS | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| (n = 600) | (n = 150) | (n = 150) | (n = 150) | (n = 150) | F-Test | ||||||
| Variable | Mean | Std Dev | Mean | Std Dev | Mean | Std Dev | Mean | Std Dev | Mean | Std Dev | p-Value 1 |
| Age | 34.30 | 6.97 | 36.05 | 6.98 | 34.66 | 6.91 | 33.6 | 6.42 | 32.91 | 7.18 | 0.001 |
| Number of Children | 1.86 | 0.80 | 1.83 | 0.73 | 1.78 | 0.78 | 1.91 | 0.93 | 1.92 | 0.76 | 0.37 |
| Monthly Income (INR) | 2113.50 | 678.68 | 2110.00 | 758.9 | 2158.67 | 611.98 | 2137.33 | 626.97 | 2048.00 | 707.93 | 0.52 |
| Quality of Life | 0.30 | 0.29 | 0.26 | 0.31 | 0.34 | 0.25 | 0.27 | 0.33 | 0.33 | 0.24 | 0.03 |
| Percent Adherence | 30.37 | 13.23 | 30.37 | 12.75 | 32.00 | 14.35 | 28.60 | 12.99 | 30.50 | 12.69 | 0.17 |
| Number of OI past 6 months | 4.58 | 1.21 | 4.61 | 1.35 | 4.52 | 1.35 | 4.58 | 0.96 | 4.63 | 1.13 | 0.88 |
| Time since HIV diagnosis (Year) | 4.05 | 2.88 | 4.34 | 3.25 | 3.83 | 2.44 | 4.10 | 2.82 | 3.95 | 2.96 | 0.46 |
| Internalized Stigma | 2.30 | 0.25 | 2.24 | 0.41 | 2.30 | 0.16 | 2.33 | 0.19 | 2.32 | 0.15 | 0.02 |
| Summary CESD Depression | 9.18 | 3.08 | 9.12 | 3.11 | 9.09 | 3.06 | 9.16 | 3.13 | 9.35 | 3.04 | 0.88 |
| Summary Social Support | 1.08 | 0.22 | 1.13 | 0.41 | 1.06 | 0.12 | 1.06 | 0.08 | 1.06 | 0.08 | 0.004 |
| Summary Food Insecurity | 21.14 | 3.44 | 20.27 | 4.29 | 21.63 | 2.58 | 20.76 | 3.45 | 21.94 | 2.98 | 0.001 |
| Total MET 2 min/week | 4608.57 | 1663.57 | 4957.09 | 1873.23 | 4569.73 | 1416.82 | 4691.85 | 1718.60 | 4215.60 | 1539.27 | 0.001 |
| Body Mass Index kg/m2 | 20.10 | 4.17 | 19.81 | 3.78 | 20.20 | 3.97 | 20.55 | 4.67 | 19.86 | 4.16 | 0.38 |
| Weight (kg) | 46.25 | 10.37 | 45.30 | 9.66 | 46.42 | 9.65 | 47.43 | 11.22 | 45.84 | 10.86 | 0.33 |
| Height (cm) | 151.52 | 5.98 | 151.06 | 5.81 | 151.57 | 6.06 | 151.85 | 5.80 | 151.62 | 6.27 | 0.71 |
| Lean Muscle Mass (kg) | 33.96 | 6.89 | 33.53 | 6.62 | 33.95 | 6.69 | 34.70 | 7.11 | 33.66 | 7.11 | 0.46 |
| Fat Mass (kg) | 12.25 | 5.75 | 11.62 | 5.07 | 12.48 | 5.33 | 12.73 | 6.36 | 12.19 | 6.15 | 0.38 |
| Categorical Variables | Total Study Population | Asha (AS) Control | Nut. Educ + AS | Nut Supp + AS | Nut Educ + Supp+ AS | Chi | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (n = 600) | (n = 150) | (n = 150) | (n = 150) | (n = 150) | Square | |||||||
| Variable | Category | N | % | N | % | N | % | N | % | N | % | p-Value 1 |
| Marital | married | 238 | 39.67 | 51 | 34.00 | 67 | 44.67 | 53 | 35.33 | 67 | 44.67 | |
| Status | divorced | 54 | 9.00 | 12 | 8.00 | 15 | 10.00 | 12 | 8.00 | 15 | 10.00 | |
| widowed | 308 | 51.33 | 87 | 58.00 | 68 | 45.33 | 85 | 56.67 | 68 | 45.33 | 0.19 | |
| Education | None | 292 | 48.67 | 85 | 56.67 | 74 | 49.33 | 71 | 47.33 | 62 | 41.33 | |
| <5 years | 98 | 16.33 | 25 | 16.67 | 29 | 19.33 | 25 | 16.67 | 19 | 12.67 | ||
| 5–9 years | 123 | 20.50 | 24 | 16.00 | 31 | 20.67 | 33 | 22.00 | 35 | 23.33 | ||
| >10 years | 87 | 14.50 | 16 | 10.67 | 16 | 10.67 | 21 | 14.00 | 34 | 22.67 | 0.04 | |
| Religion | Hindu | 439 | 73.17 | 110 | 73.33 | 116 | 77.33 | 104 | 69.33 | 109 | 72.67 | |
| Muslim | 44 | 7.33 | 17 | 11.33 | 5 | 3.33 | 12 | 8.00 | 10 | 6.67 | ||
| Christian | 117 | 19.50 | 23 | 15.33 | 29 | 19.33 | 34 | 22.67 | 31 | 20.67 | 0.14 | |
| Body | <18.5 kg/m2 | 234 | 39.00 | 59 | 39.33 | 57 | 38.00 | 55 | 36.67 | 63 | 42.00 | |
| Mass | 18.5–22.9 | 228 | 38.00 | 63 | 42.00 | 54 | 36.00 | 57 | 38.00 | 54 | 36.00 | |
| Index | 23–27.49 | 103 | 17.17 | 24 | 16.00 | 30 | 20.00 | 23 | 15.33 | 26 | 17.33 | |
| WHO-Asian | 27.5+ | 35 | 5.83 | 4 | 2.67 | 9 | 6.00 | 15 | 10.00 | 7 | 4.67 | 0.35 |
| Body | <18.5 kg/m2 | 234 | 39.00 | 59 | 39.33 | 57 | 38.00 | 55 | 36.67 | 63 | 42.00 | |
| Mass | 18.5–24.99 | 281 | 46.83 | 75 | 50.00 | 73 | 48.67 | 69 | 46.00 | 64 | 42.67 | |
| Index | 25.0–29.99 | 69 | 11.50 | 13 | 8.67 | 16 | 10.67 | 20 | 13.33 | 20 | 13.33 | |
| WHO-Int | 30+ | 16 | 2.67 | 3 | 2.00 | 4 | 2.67 | 5 | 3.33 | 4 | 2.69 | 0.61 |
| Primary Outcome: Lean Mass | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Group Means | Time Effects | |||||||||
| Asha (AS) | Nut Educ | Nut Supp. | Nut Educ + | Time Effects | ||||||
| Control | + AS | + AS | Nut Supp. + AS | (within Subjects) | ||||||
| Mean | Std Dev | Mean | Std Dev | Mean | Std Dev | Mean | Std Dev | p-Value | ||
| Baseline Lean Mass | 33.52 | 6.62 | 33.95 | 6.70 | 34.70 | 7.11 | 33.66 | 7.12 | ||
| 6 Month Lean Mass | 35.28 | 6.24 | 35.78 | 6.75 | 38.10 | 7.16 | 38.17 | 6.82 | 4.52 | 0.001 |
| 12 month Lean Mass | 36.25 | 6.23 | 36.99 | 6.58 | 39.29 | 7.05 | 39.45 | 6.62 | 5.79 | 0.001 |
| 18 month Lean Mass | 37.03 | 6.28 | 37.92 | 6.60 | 40.13 | 7.05 | 40.45 | 6.60 | 6.79 | 0.000 |
| Group and Time Effects | ||||||||||
| p-value | p-value | p-value | p-value | |||||||
| Group Effects (between subjects) | ||||||||||
| 21.73 | 0.001 | 20.86 | 0.001 | 20.33 | 0.001 | |||||
| Time by Group: | ||||||||||
| 6 months | −1.11 | 0.001 | −2.68 | 0.001 | −2.76 | 0.001 | ||||
| 12 months | −1.20 | 0.001 | −2.75 | 0.001 | −3.06 | 0.001 | ||||
| 18 months | −1.36 | 0.001 | −2.82 | 0.001 | −3.28 | 0.001 | ||||
| Type 3 Tests of Fixed Effects | F-value | p-value | ||||||||
| Time | 1342.45 | 0.001 | ||||||||
| Group | 6.31 | 0.003 | ||||||||
| Time by Group | 37.00 | 0.001 | ||||||||
| Overall Maximum Likelihood | ||||||||||
| Ratio Test for Adjusted Model | ||||||||||
| DF | Chi Sq | p-value | ||||||||
| 7 | 4721.28 | 0.001 | ||||||||
| Secondary Outcome: Fat Mass | ||||||||||
| Group Means | Time Effects | |||||||||
| Asha (AS) | Nut Educ | Nut Supp. | Nut Educ + | Time Effects | ||||||
| Control | +AS | +AS | Nut Educ + AS | (within subjects) | ||||||
| Mean | Std Dev | Mean | Std Dev | Mean | Std Dev | Mean | Std Dev | p-value | ||
| Baseline Fat Mass | 11.62 | 5.07 | 12.48 | 5.33 | 12.73 | 6.36 | 12.19 | 6.15 | ||
| 6 month Fat Mass | 12.19 | 5.09 | 13.55 | 5.28 | 14.79 | 6.89 | 13.91 | 5.89 | 1.72 | 0.0001 |
| 12 month Fat Mass | 12.29 | 4.86 | 13.71 | 5.11 | 14.76 | 6.56 | 13.97 | 5.85 | 1.78 | 0.0001 |
| 18 month Fat Mass | 12.62 | 4.78 | 13.96 | 4.99 | 15.01 | 6.55 | 14.35 | 5.74 | 2.16 | 0.0001 |
| Group and Time Effects | ||||||||||
| p-value | p-value | p-value | p-value | |||||||
| Group Effects (between subjects) | 2.01 | 0.56 | 2.36 | 0.53 | 1.83 | 0.6764 | ||||
| Time by Group: | ||||||||||
| 6 months | 0.34 | 0.14 | −0.64 | 0.002 | −1.15 | 0.001 | ||||
| 12 months | 0.25 | 0.28 | −0.54 | 0.010 | −1.11 | 0.001 | ||||
| 18 months | 0.12 | 0.61 | −0.67 | 0.001 | −1.15 | 0.001 | ||||
| Type 3 Tests of Fixed Effects | F-value | p-value | ||||||||
| Time | 204.47 | 0.001 | ||||||||
| Group | 5.36 | 0.001 | ||||||||
| Time by Group | 8.44 | 0.001 | ||||||||
| Overall Maximum Likelihood | ||||||||||
| Ratio Test for Adjusted Model | ||||||||||
| DF | Chi Sq | p-value | ||||||||
| 7 | 4395.62 | 0.001 | ||||||||
| Secondary Outcome: Weight (kg) | ||||||||||
| Group Means | Time Effects | |||||||||
| Asha (AS) | Nut Educ | Nut Supp. | Nut Educ + | Time Effects | ||||||
| Control | + AS | + AS | Nut Supp. + AS | (within subjects) | ||||||
| Mean | Std Dev | Mean | Std Dev | Mean | Std Dev | Mean | Std Dev | p-value | ||
| Baseline Weight (kg) | 45.30 | 9.66 | 46.42 | 9.65 | 47.43 | 11.22 | 45.84 | 10.86 | ||
| 6 Month Weight | 47.47 | 9.56 | 49.33 | 9.63 | 52.89 | 11.02 | 52.08 | 10.74 | 6.24 | 0.001 |
| 12 month Weight | 48.54 | 9.51 | 50.70 | 9.56 | 54.06 | 11.02 | 53.56 | 10.70 | 7.72 | 0.001 |
| 18 month Weight | 49.66 | 9.46 | 51.88 | 9.52 | 55.14 | 10.99 | 54.80 | 10.61 | 6.24 | 0.001 |
| Group and Time Effects | ||||||||||
| p-value | p-value | p-value | p-value | |||||||
| Group Effects (between subjects) | 22.21 | 0.002 | 23.38 | 0.001 | 21.82 | 0.0021 | ||||
| Time by Group: | ||||||||||
| 6 months | −0.78 | 0.001 | −3.33 | 0.001 | −4.06 | 0.001 | ||||
| 12 months | −1.09 | 0.001 | −3.44 | 0.001 | −4.48 | 0.003 | ||||
| 18 months | −1.24 | 0.001 | −3.50 | 0.001 | −4.60 | 0.001 | ||||
| Type 3 Tests of Fixed Effects | F-value | p-value | ||||||||
| Time | 8127.26 | 0.001 | ||||||||
| Group | 7.69 | 0.003 | ||||||||
| Time by Group | 209.08 | 0.001 | ||||||||
| Overall Maximum Likelihood | ||||||||||
| Ratio Test for Adjusted Model | ||||||||||
| DF | Chi Sq | p-value | ||||||||
| 7 | 8237.26 | 0.001 | ||||||||
| Adherence < 30% (n = 258) | Adherence > 30% (n = 342) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intervention Group by Time Effects | Intervention Group by Time Effects | ||||||||||||
| Nut Educ | Nut Supp. | Nut Educ & Supp | Nut Educ. | Nut Supp. | Nut Educ & Supp | Interaction | |||||||
| p-Value 1 | p-Value | p-Value | p-Value | p-Value | p-Value | p-Value 2 | |||||||
| Primary Outcome | |||||||||||||
| Lean Mass | |||||||||||||
| 6 months | −1.42 | 0.0001 | −2.98 | 0.0001 | −3.07 | 0.0001 | −0.86 | 0.0210 | −2.45 | 0.0001 | −2.51 | 0.0001 | |
| 12 months | −1.46 | 0.0001 | −2.99 | 0.0001 | −3.48 | 0.0001 | −0.99 | 0.0080 | −2.56 | 0.0001 | −2.73 | 0.0001 | |
| 18 months | −1.60 | 0.0001 | −3.07 | 0.0001 | −3.84 | 0.0001 | −1.17 | 0.0017 | −2.61 | 0.0001 | −2.84 | 0.0001 | 0.9032 |
| Secondary Outcomes | |||||||||||||
| Fat Mass | |||||||||||||
| 6 months | 0.59 | 0.0751 | −0.50 | 0.1779 | −1.12 | 0.0018 | 0.12 | 0.7132 | −0.73 | 0.0029 | −1.67 | 0.0001 | |
| 12 months | 0.45 | 0.1690 | −0.57 | 0.1275 | −0.97 | 0.0068 | 0.07 | 0.8225 | −0.52 | 0.0355 | −1.22 | 0.0001 | |
| 18 months | 0.29 | 0.3850 | −0.75 | 0.0447 | −0.93 | 0.0097 | −0.03 | 0.9195 | −0.62 | 0.0112 | −1.34 | 0.0001 | 0.5491 |
| Weight (kg) | |||||||||||||
| 6 months | −0.84 | 0.0001 | −3.49 | 0.0001 | −4.50 | 0.0001 | −0.74 | 0.0001 | −3.18 | 0.0001 | −3.72 | 0.0001 | |
| 12 months | −1.13 | 0.0001 | −3.69 | 0.0001 | −4.89 | 0.0001 | −1.07 | 0.0001 | −3.23 | 0.0001 | −4.15 | 0.0001 | |
| 18 months | −1.31 | 0.0001 | −3.82 | 0.0001 | −5.08 | 0.0001 | −1.21 | 0.0001 | −3.22 | 0.0001 | −4.22 | 0.0001 | 0.0239 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carpenter, C.L.; Kapur, K.; Ramakrishna, P.; Pamujula, S.; Yadav, K.; Giovanni, J.E.; Julian, O.; Ekstrand, M.L.; Sinha, S.; Nyamathi, A.M. Lean Mass Improvement from Nutrition Education and Protein Supplementation among Rural Indian Women Living with HIV/AIDS: Results from Cluster Randomized Factorial Trial at 18-Month Follow-Up. Nutrients 2022, 14, 179. https://doi.org/10.3390/nu14010179
Carpenter CL, Kapur K, Ramakrishna P, Pamujula S, Yadav K, Giovanni JE, Julian O, Ekstrand ML, Sinha S, Nyamathi AM. Lean Mass Improvement from Nutrition Education and Protein Supplementation among Rural Indian Women Living with HIV/AIDS: Results from Cluster Randomized Factorial Trial at 18-Month Follow-Up. Nutrients. 2022; 14(1):179. https://doi.org/10.3390/nu14010179
Chicago/Turabian StyleCarpenter, Catherine L., Kavita Kapur, Padma Ramakrishna, Suresh Pamujula, Kartik Yadav, Jennifer E. Giovanni, Olivia Julian, Maria L. Ekstrand, Sanjeev Sinha, and Adeline M. Nyamathi. 2022. "Lean Mass Improvement from Nutrition Education and Protein Supplementation among Rural Indian Women Living with HIV/AIDS: Results from Cluster Randomized Factorial Trial at 18-Month Follow-Up" Nutrients 14, no. 1: 179. https://doi.org/10.3390/nu14010179