Effects of Preconception Care and Periconception Interventions on Maternal Nutritional Status and Birth Outcomes in Low- and Middle-Income Countries: A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Objectives
2.2. Eligibility Criteria
2.2.1. Types of Studies
2.2.2. Types of Participants
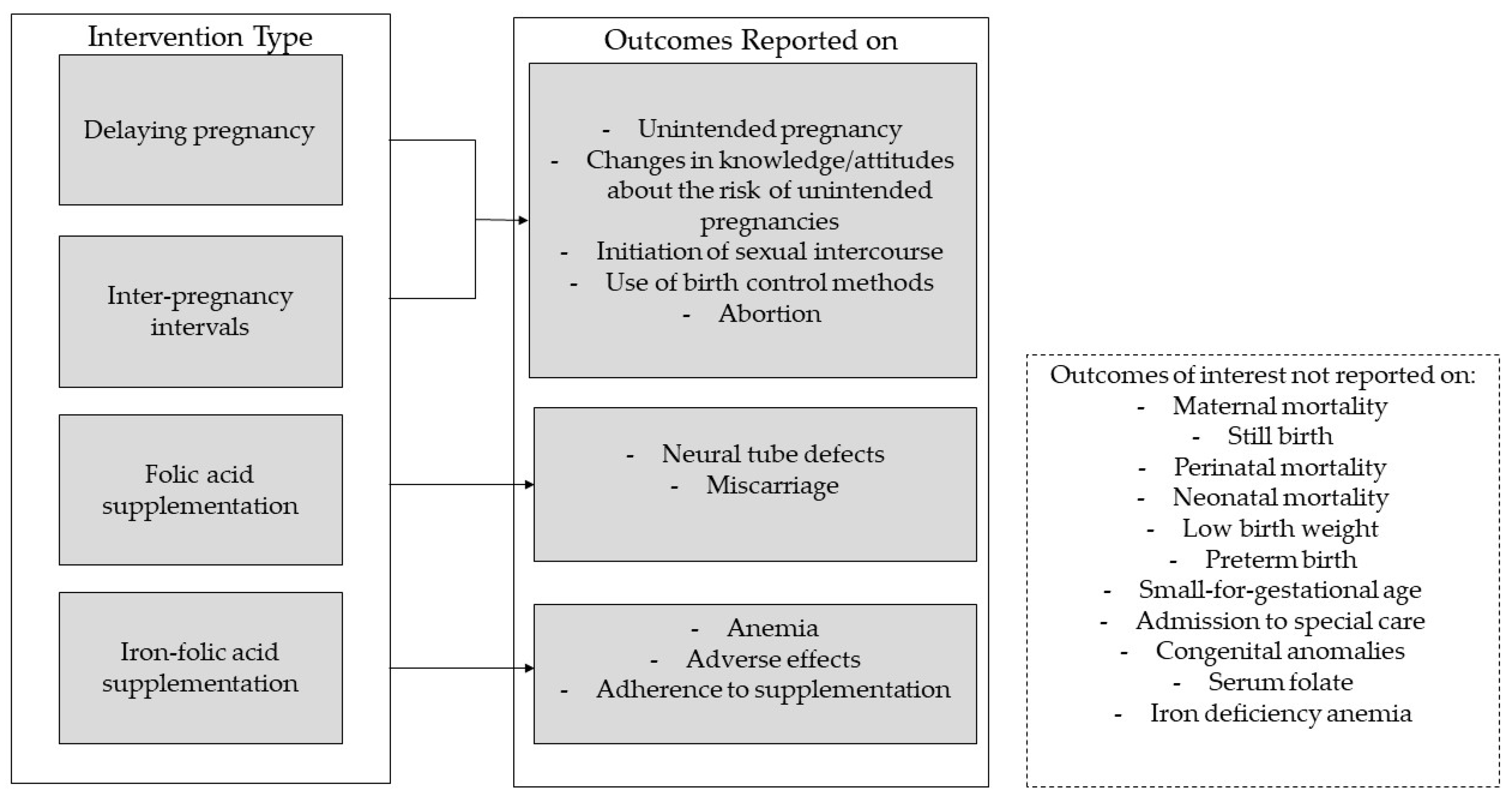
2.2.3. Types of Intervention
- Interventions to delay the age at first pregnancy, such as curriculum-based sex education, abstinence alone programs, interactive computer-based interventions, etc.
- ○
- Educational interventions and contraceptive promotion given to adolescents and young women at the community, school, or household level by parents, colleagues, teachers, health workers, or social workers.
- Interventions to optimize inter-pregnancy intervals, such as introducing family planning methods, abstinence alone programs, etc.
- ○
- Educational interventions and contraceptive promotion given to mothers of reproductive age at the community, school, or household level by parents, colleagues, teachers, health workers, or social workers.
- Periconception folic acid supplementation.
- ○
- Any folic acid supplementation given to either pubescent or menstruating women prior to conception that continued until the first trimester of pregnancy.
- Periconception iron folic acid.
- ○
- Any iron folic acid supplementation given to either pubescent or menstruating women prior to conception and/or continued until the first trimester of pregnancy.
2.2.4. Type of Outcome Measures
- Maternal: unintended pregnancy, anemia, and iron deficiency anemia.
- Neonatal: neural tube defects, still birth, perinatal mortality, neonatal mortality, and low birth weight.
- Maternal: reported changes in knowledge and attitudes about the risk of unintended pregnancies, initiation of sexual intercourse, use of birth control methods, serum folate, adverse effects, adherence to folic acid or iron folic acid supplementation, abortion or miscarriage, and maternal mortality.
- Neonatal: preterm birth, small-for-gestational age, other congenital anomalies, and special care admission due to any reason.
2.2.5. Duration of Follow-Up
2.3. Literature Search
2.4. Data Collection and Analysis
- Methods: study design and study duration.
- Details of study participants (age, socioeconomic status, parity): numbers randomized, and inclusion and exclusion criteria.
- Interventions: content, duration and timing of intervention, and comparisons.
- Outcomes and time point.
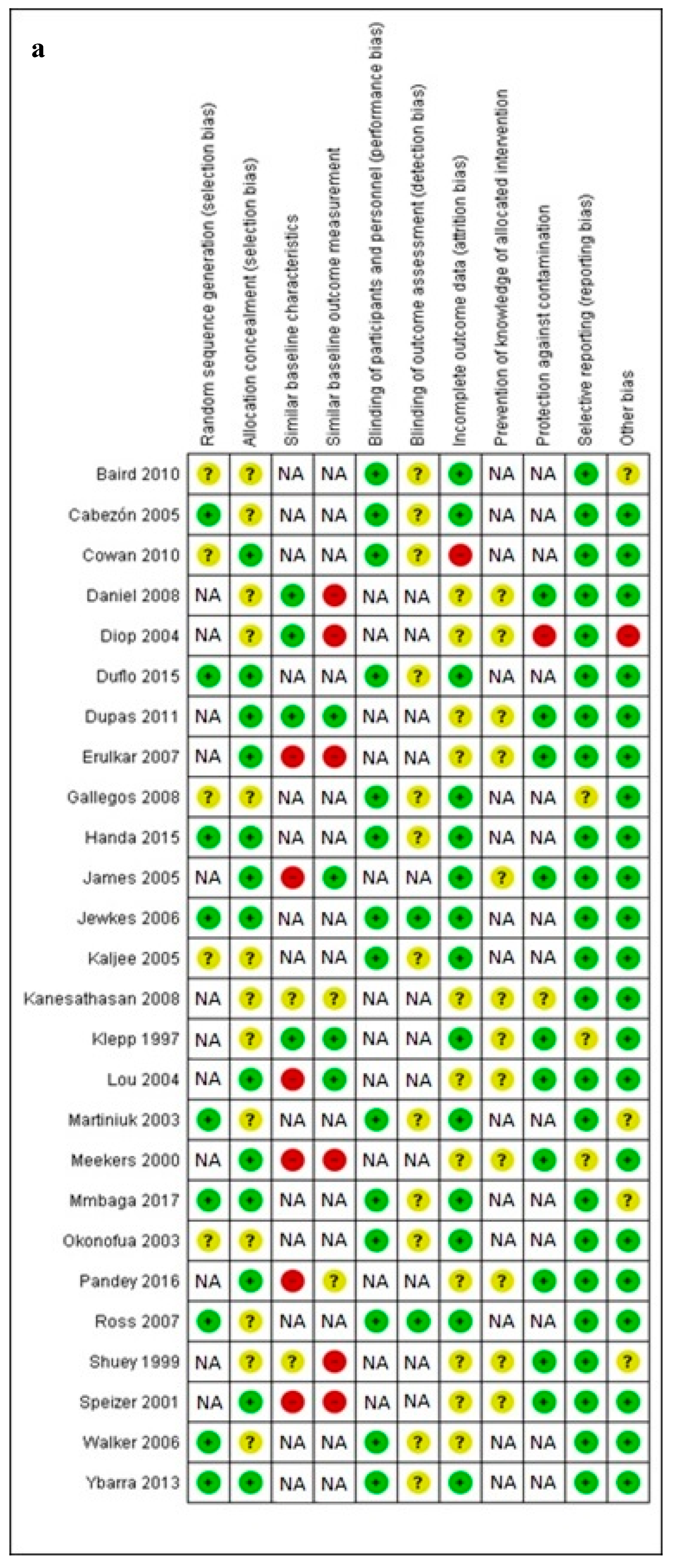
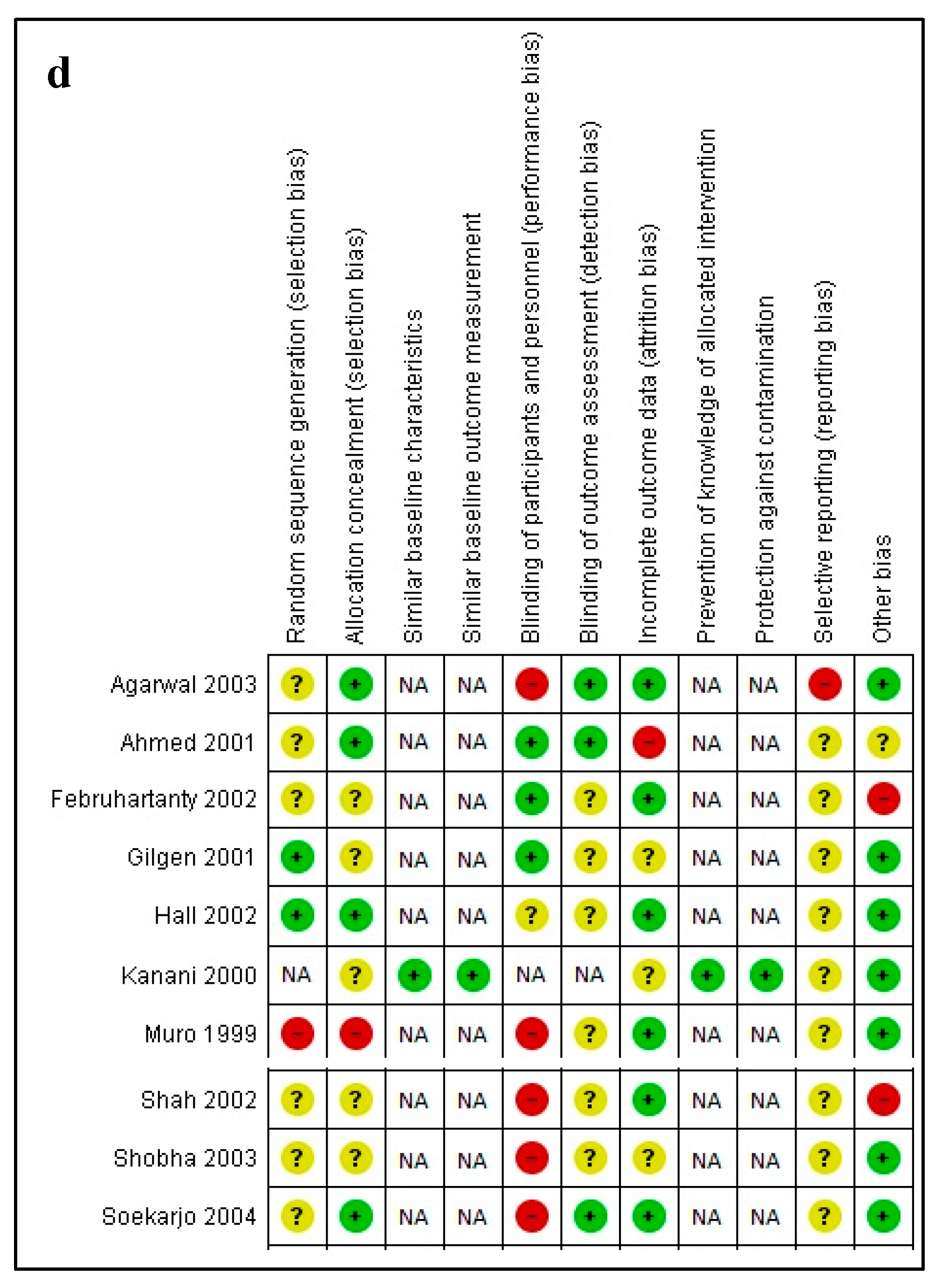
2.4.1. Assessment of Risk of Bias in Included Studies
- random sequence generation.
- allocation concealment.
- blinding of participants and personnel.
- blinding of outcome assessment for each outcome.
- incomplete outcome data.
- selective outcome reporting.
- other bias, such as validity of outcome measure and baseline comparability.
- random sequence generation
- allocation concealment
- baseline outcome measurements
- baseline characteristics
- incomplete outcome
- knowledge of the allocated interventions adequately prevented during the study
- protection against contamination
- selective outcome reporting
- other risks of bias.
2.4.2. Measures of Treatment Effect
2.4.3. Unit of Analysis Issues
2.4.4. Dealing with Missing Data
2.4.5. Assessment of Heterogeneity
2.4.6. Assessment of Reporting Biases
2.4.7. Data Synthesis
2.4.8. Assessment of Quality of Evidence
2.4.9. Subgroup Analysis and Investigation of Heterogeneity
- Setting (home, facility based, community level, school, work).
- Timing of intervention (preconception, peri-conception, prenatal, post-partum).
- Type of intervention (school-based education, abstinence-only program, contraceptive promotion, etc.).
2.4.10. Sensitivity Analysis
- Allocation concealment (adequate versus inadequate and/or unclear).
- Attrition (< 10% versus ≥ 10%).
- Imputed inter-correlation coefficients that were derived in different ways.
3. Results
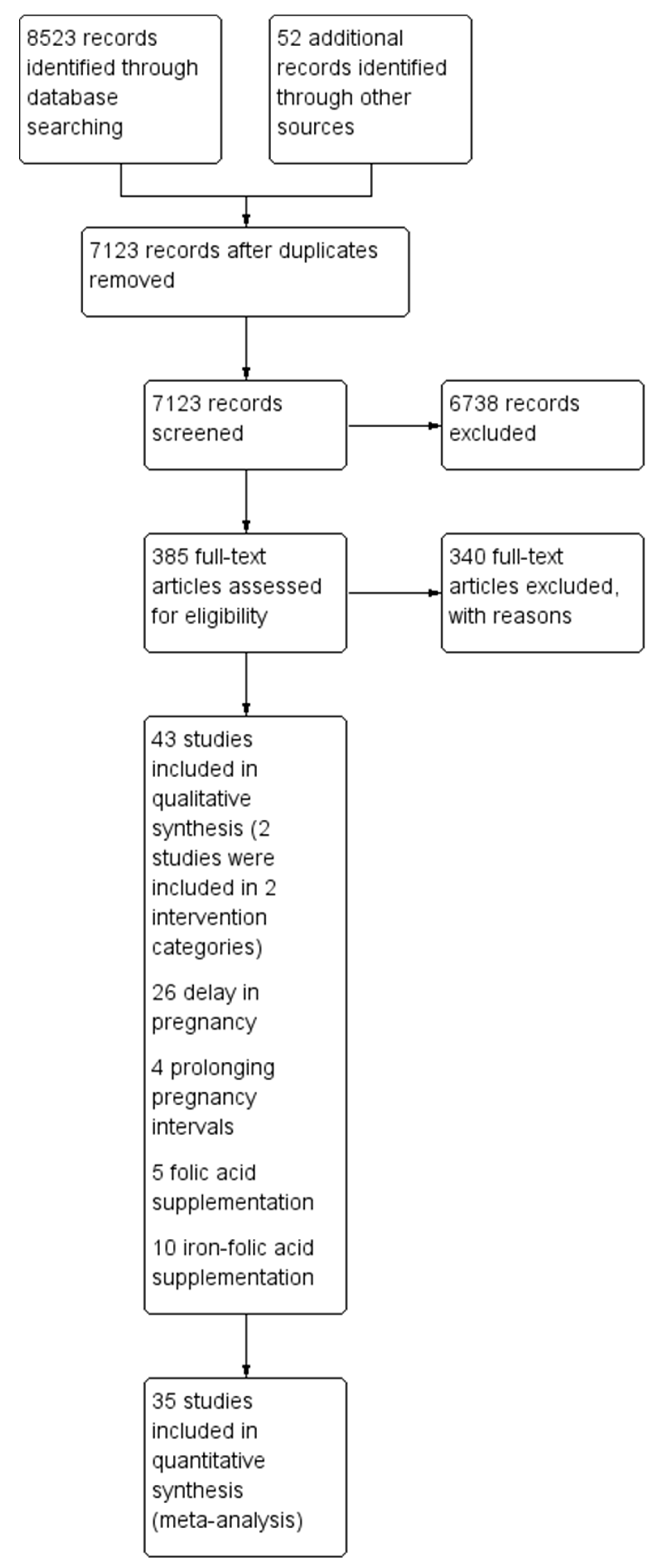
3.1. Study Selection
3.2. Delaying Pregnancy
3.2.1. Description of Studies
3.2.2. Risk of Bias
3.2.3. Effects of Interventions
3.3. Optimising Inter-Pregnancy Intervals
3.3.1. Description of Studies
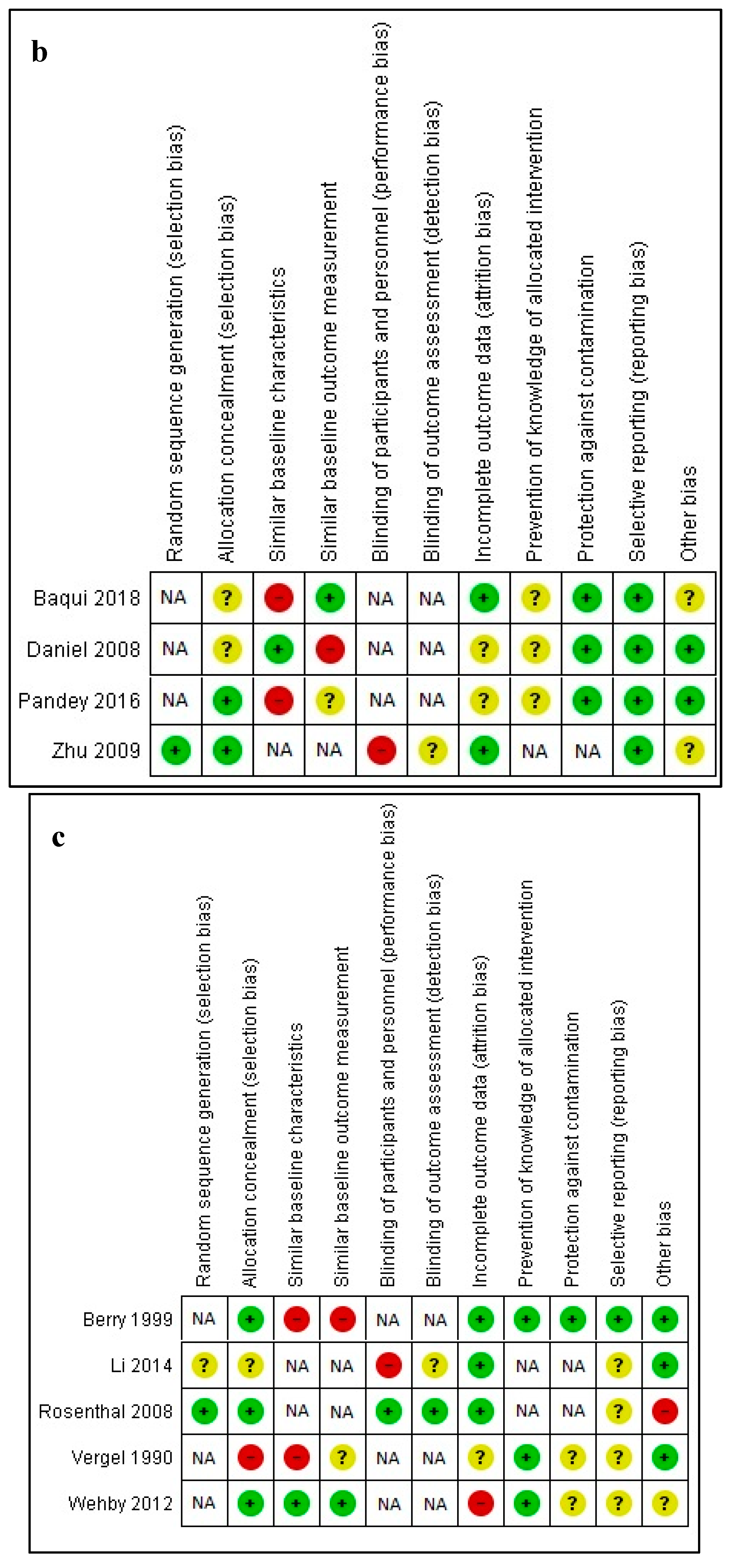
3.3.2. Risk of Bias
3.3.3. Effects of Interventions
3.4. Periconceptional Folic Acid Supplementation
3.4.1. Description of Studies
3.4.2. Risk of Bias
3.4.3. Effects of Interventions
3.5. Periconceptional Iron Folic Acid Supplementation
3.5.1. Description of Studies
3.5.2. Risk of Bias
3.5.3. Effects of Interventions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Appendix A
References
- Johnson, K.; Posner, S.F.; Biermann, J.; Cordero, J.F.; Atrash, H.K.; Parker, C.S.; Curtis, M.G. Recommendations to Improve Preconception Health and Health Care—United States: Report of the CDC/ATSDR Preconception Care Work Group and the Select Panel on Preconception Care. Morb. Mortal. Wkly. Rep. Recomm. Rep. 2006, 55, 1–23. [Google Scholar]
- World Health Organization. Meeting to Develop a Global Consensus on Preconception Care to Reduce Maternal and Childhood Mortality and Morbidity; 6–7 February 2012 Meeting Report; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Dean, S.; Rudan, I.; Althabe, F.; Girard, A.W.; Howson, C.; Langer, A.; Venkatraman, C.M. Setting research priorities for preconception care in low-and middle-income countries: Aiming to reduce maternal and child mortality and morbidity. PLoS Med. 2013, 10, e1001508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dean, S.V.; Imam, A.M.; Lassi, Z.S.; Bhutta, Z.A. Importance of intervening in the preconception period to impact pregnancy outcomes. In Maternal and Child Nutrition: The First 1000 Days; Karger Publishers: Basel, Switzerland, 2013; Volume 74, pp. 63–73. [Google Scholar]
- World Health Organization. Global Strategy for Women’s, Children’s and Adolescents’ Health [2016–2030); World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization. Individualized, Supportive Care Key to Positive Childbirth Experience, Says WHO; World Health Organisation: Geneva, Switzerland, 2018. [Google Scholar]
- World Health Organization. Adolescent Pregnancy: Key Facts; World Health Organisation: Geneva, Switzerland, 2018. [Google Scholar]
- Haldre, K.; Rahu, K.; Karro, H.; Rahu, M. Is a poor pregnancy outcome related to young maternal age? A study of teenagers in Estonia during the period of major socio-economic changes [from 1992 to 2002). Eur. J. Obstet. Gynecol. Reprod. Biol. 2007, 131, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Paranjothy, S.; Broughton, H.; Adappa, R.; Fone, D. Teenage pregnancy: Who suffers? Arch. Dis. Child. 2009, 94, 239–245. [Google Scholar] [CrossRef]
- World Health Organization. Adolescent Pregnancy: Unmet Needs and Undone Deeds; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Conde-Agudelo, A.; Rosas-Bermudez, A.; Castaño, F.; Norton, M.H. Effects of birth spacing on maternal, perinatal, infant, and child health: A systematic review of causal mechanisms. Stud. Fam. Plan. 2012, 43, 93–114. [Google Scholar] [CrossRef]
- Ramakrishnan, U.; Grant, F.; Goldenberg, T.; Zongrone, A.; Martorell, R. Effect of women’s nutrition before and during early pregnancy on maternal and infant outcomes: A systematic review. Paediat. Perinat. Epidemiol. 2012, 26, 285–301. [Google Scholar] [CrossRef]
- McCauley, M.E.; van den Broek, N.; Dou, L.; Othman, M. Vitamin A supplementation during pregnancy for maternal and newborn outcomes. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- De-Regil, L.M.; Palacios, C.; Lombardo, L.K.; Peña-Rosas, J.P. Vitamin D supplementation for women during pregnancy. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef] [Green Version]
- Balogun, O.O.; da Silva Lopes, K.; Ota, E.; Takemoto, Y.; Rumbold, A.; Takegata, M.; Mori, R. Vitamin supplementation for preventing miscarriage. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef]
- Dean, S.V.; Lassi, Z.S.; Imam, A.M.; Bhutta, Z.A. Preconception care: Promoting reproductive planning. Reprod. Health 2014, 11, S2. [Google Scholar] [CrossRef] [Green Version]
- Oringanje, C.; Meremikwu, M.M.; Eko, H.; Esu, E.; Meremikwu, A.; Ehiri, J.E. Interventions for preventing unintended pregnancies among adolescents. Cochrane Database Syst. Rev. 2009. [Google Scholar] [CrossRef]
- Schünemann, H.J.; Tugwell, P.; Reeves, B.C.; Akl, E.A.; Santesso, N.; Spencer, F.A.; Helfand, M. Non-randomized studies as a source of complementary, sequential or replacement evidence for randomized controlled trials in systematic reviews on the effects of interventions. Res. Synth. Methods 2013, 4, 49–62. [Google Scholar] [CrossRef] [PubMed]
- Lassi, Z.S.; Kedzior, S.; Das, J.K.; Bhutta, Z.A. Effects of preconception care and peri-conception interventions on maternal nutritional status and birth outcomes in low- and middle-income countries. The Campbell Collaboration Library of Systematic Reviews. Immunology 2019, 15. [Google Scholar] [CrossRef] [Green Version]
- Bank, W. World Bank List of Country Economies; World Bank: Washington, DC, USA, 2017; Available online: http://data.worldbank.org/about/country-classifications/countryand-lending-groups (accessed on 15 January 2018).
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions: The Cochrane Collaboration; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cochrane Effective Practice and Organisation of Care (EPOC). Suggested Risk of Bias Criteria for EPOC Reviews; EPOC Resources for review authors; EPOC: Oslo, Norway, 2017. [Google Scholar]
- Review Manager (RevMan); Computer program, Version 5.3; The Nordic Cochrane Centre, The Cochrane Collaboration: Copenhagen, Denmark, 2014.
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Jaeschke, R. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Baird, S.; Chirwa, E.; McIntosh, C.; Özler, B. The short-term impacts of a schooling conditional cash transfer program on the sexual behavior of young women. Health Econ. 2010, 19, 55–68. [Google Scholar] [CrossRef]
- Cabezón, C.; Vigil, P.; Rojas, I.; Leiva, M.E.; Riquelme, R.; Aranda, W.; García, C. Adolescent pregnancy prevention: An abstinence-centered randomized controlled intervention in a Chilean public high school. J. Adolesc. Health 2005, 36, 64–69. [Google Scholar] [CrossRef]
- Cowan, F.M.; Pascoe, S.J.; Langhaug, L.F.; Mavhu, W.; Chidiya, S.; Jaffar, S.; Woelk, G. The Regai Dzive Shiri project: Results of a randomized trial of an HIV prevention intervention for youth. AIDS 2010, 24, 2541–2552. [Google Scholar] [CrossRef] [Green Version]
- Daniel, E.E.; Masilamani, R.; Rahman, M. The effect of community-based reproductive health communication interventions on contraceptive use among young married couples in Bihar, India. Int. Fam. Plan. Perspect. 2008, 34, 189–197. [Google Scholar] [CrossRef]
- Diop, N.J.; Bathidja, H.; Touré, I.D.; Dieng, T.; Mané, B. Improving the reproductive health of adolescents in Senegal. Front. Reprod. Health 2004. [Google Scholar] [CrossRef] [Green Version]
- Duflo, E.; Dupas, P.; Kremer, M. Education, HIV, and Early Fertility: Experimental Evidence from Kenya. Am. Econ. Rev. 2015, 105, 2757–2797. [Google Scholar] [CrossRef] [PubMed]
- Dupas, P. Do Teenagers Respond to HIV Risk Information? Evidence from a Field Experiment in Kenya. Am. Econ. J. Appl. Econ. 2011, 3, 1–34. [Google Scholar] [CrossRef] [Green Version]
- Erulkar, A.S.; Muthengi, E. Evaluation of Berhane Hewan A Pilot Program to Promote Education & Delay Marriage in Rural Ethiopia. Int. Perspect. Sex Reprod. Health 2007, 35, 6–14. [Google Scholar]
- Gallegos, E.C.; Villarruel, A.M.; Loveland-Cherry, C.; Ronis, D.L.; Zhou, Y. Intervention to reduce adolescents’ sexual risk behaviors: A randomized controlled trial. Salud Publica de Mexico 2008, 50, 59–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Handa, S.; Peterman, A.; Huang, C.; Halpern, C.; Pettifor, A.; Thirumurthy, H. Impact of the Kenya Cash Transfer for Orphans and Vulnerable Children on early pregnancy and marriage of adolescent girls. Soc. Sci. Med. 2015, 141, 36–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, S.; Reddy, P.S.; Ruiter, R.A.; Taylor, M.; Jinabhai, C.C.; Van Empelen, P.; Van Den Borne, B. The effects of a systematically developed photo-novella on knowledge, attitudes, communication and behavioural intentions with respect to sexually transmitted infections among secondary school learners in South Africa. Health Promot. Int. 2005, 20, 157–165. [Google Scholar] [CrossRef] [Green Version]
- Jewkes, R.; Nduna, M.; Levin, J.; Jama, N.; Dunkle, K.; Khuzwayo, N. A cluster randomized-controlled trial to determine the effectiveness of Stepping Stones in preventing HIV infections and promoting safer sexual behaviour amongst youth in the rural Eastern Cape, South Africa: Trial design, methods and baseline findings. Trop. Med. Int. Health 2006, 11, 3–16. [Google Scholar] [CrossRef]
- Kaljee, L.M.; Genberg, B.; Riel, R.; Cole, M.; Tho, L.H.; Thoa, L.T.K.; Minh, T.T. Effectiveness of a theory-based risk reduction HIV prevention program for rural Vietnamese adolescents. AIDS Educ. Prev. 2005, 17, 185–199. [Google Scholar] [CrossRef] [Green Version]
- Kanesathasan, A.; Cardinal, L.J.; Pearson, E.; Das Gupta, S.; Mukherjee, S.; Malhotra, A. Improving Youth Sexual and Reproductive Health through DISHA, an Integrated Program in India; International Center for Research on Women: Washington, DC, USA, 2008. [Google Scholar]
- Klepp, K.I.; Ndeki, S.S.; Leshabari, M.T.; Hannan, P.J.; Lyimo, B.A. AIDS education in Tanzania: Promoting risk reduction among primary school children. Am. J. Public Health 1997, 87, 1931–1936. [Google Scholar] [CrossRef]
- Lou, C.H.; Wang, B.; Shen, Y.; Gao, E.S. Effects of a community-based sex education and reproductive health service program on contraceptive use of unmarried youths in Shanghai. J. Adolesc. Health 2004, 34, 433–440. [Google Scholar] [CrossRef]
- Martiniuk, A.L.; O’Connor, K.S.; King, W.D. A cluster randomized trial of a sex education programme in Belize, Central America. Int. J. Epidemiol. 2003, 32, 131–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meekers, D. The Effectiveness of Targeted Social Marketing to Promote Adolescent Reproductive Health. J. HIV/AIDS Prev. Educ. Adolesc. Child. 2000, 3, 73–92. [Google Scholar] [CrossRef]
- Mmbaga, E.J.; Kajula, L.; Aarø, L.E.; Kilonzo, M.; Wubs, A.G.; Eggers, S.M.; Kaaya, S. Effect of the PREPARE intervention on sexual initiation and condom use among adolescents aged 12–14: A cluster randomised controlled trial in Dar es Salaam, Tanzania. BMC Public Health 2017, 17, 322. [Google Scholar] [CrossRef] [Green Version]
- Okonofua, F.E.; Coplan, P.; Collins, S.; Oronsaye, F.; Ogunsakin, D.; Ogonor, J.T.; Heggenhougen, K. Impact of an intervention to improve treatment-seeking behavior and prevent sexually transmitted diseases among Nigerian youths. Int. J. Infect. Dis. 2003, 7, 61–73. [Google Scholar] [CrossRef] [Green Version]
- Pandey, N.; Jejeebhoy, S.; Acharya, R.; Singh, S.K.; Srinivas, M. Effects of the PRACHAR Project’s Reproductive Health Training Programme for Adolescents: Findings from a Longitudinal Study; Population Council: New Delhi, India, 2016. [Google Scholar]
- Ross, D.A.; Changalucha, J.; Obasi, A.I.; Todd, J.; Plummer, M.L.; Cleophas-Mazige, B.; Grosskurth, H. Biological and behavioural impact of an adolescent sexual health intervention in Tanzania: A community-randomized trial. AIDS 2007, 21, 1943–1955. [Google Scholar] [CrossRef]
- Shuey, D.A.; Babishangire, B.B.; Omiat, S.; Bagarukayo, H. Increased sexual abstinence among in-school adolescents as a result of school health education in Soroti district, Uganda. Health Educ. Res. 1999, 14, 411–419. [Google Scholar] [CrossRef] [Green Version]
- Speizer, I.S.; Tambashe, B.O.; Tegang, S.P. An evaluation of the “Entre Nous Jeunes” peer-educator program for adolescents in Cameroon. Stud. Fam. Plan. 2001, 32, 339–351. [Google Scholar] [CrossRef]
- Walker, D.; Gutierrez, J.P.; Torres, P.; Bertozzi, S.M. HIV prevention in Mexican schools: Prospective randomised evaluation of intervention. BMJ 2006, 332, 1189–1194. [Google Scholar] [CrossRef] [Green Version]
- Ybarra, M.L.; Bull, S.S.; Prescott, T.L.; Korchmaros, J.D.; Bangsberg, D.R.; Kiwanuka, J.P. Adolescent abstinence and unprotected sex in CyberSenga, an Internet-based HIV prevention program: Randomized clinical trial of efficacy. PLoS ONE 2013, 8, e70083. [Google Scholar] [CrossRef]
- Baqui, A.H.; Ahmed, S.; Begum, N.; Khanam, R.; Mohan, D.; Harrison, M.; Ahmed, S. Impact of integrating a postpartum family planning program into a community-based maternal and newborn health program on birth spacing and preterm birth in rural Bangladesh. J. Glob. Health 2018, 8, 020406. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.L.; Zhang, W.H.; Cheng, Y.; Xu, J.; Xu, X.; Gibson, D.; Temmerman, M. Impact of post-abortion family planning services on contraceptive use and abortion rate among young women in China: A cluster randomised trial. Eur. J. Contracept. Reprod. Health Care 2009, 14, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Berry, R.J.; Li, Z.; Erickson, J.D.; Li, S.; Moore, C.A.; Wang, H.; Hong, S.X. Prevention of neural-tube defects with folic acid in China. China-U.S. collaborative project for neural tube defect prevention. N. Engl. J. Med. 1999, 341, 1485–1490. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.F.; Hu, N.S.; Tian, X.B.; Li, L.; Wang, S.M.; Xu, X.B.; Bao, J.H. Effect of daily milk supplementation on serum and umbilical cord blood folic acid concentrations in pregnant Han and Mongolian women and birth characteristics in China. Asia Pac. J. Clin. Nutr. 2014, 23, 567–574. [Google Scholar] [PubMed]
- Rosenthal, J.; Milla, G.; Flores, A.; Yon, M.; Pfeiffer, C.; Umana, E.; Barahona, F. Effect of different dosage and administrationschedules of folic acid on blood folate levels in a population of Honduran women of reproductive age. Public Health Nutr. 2008, 11, 822–830. [Google Scholar] [CrossRef] [PubMed]
- Vergel, R.G.; Sanchez, L.R.; Heredero, B.L.; Rodriguez, P.L.; Martinez, A.J. Primary prevention of neural tube defects with folic acid supplementation: Cuban Experiene. Prenat. Diagn. 1990, 10, 149–152. [Google Scholar] [CrossRef] [PubMed]
- Wehby, G.L.; Goco, N.; Moretti-Ferreira, D.; Felix, T.; Richieri-Costa, A.; Padovani, C.; Hartwell, T. Oral cleft prevention program[OCPP). BMC Pediatr. 2012, 12, 184. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, K.N.; Gomber, H.; Bisht, H.; Som, M. Anemia prophylaxis in adolescent school girls by weekly or daily iron-folate supplementation. Indian Pediatr. 2003, 40, 296–301. [Google Scholar]
- Ahmed, F.; Rahman, K.; Jackson, A.A. Concomitant supplemental vitamin A enhances the response to weekly supplemental iron and folic acid in anemic teenagers in urban Bangladesh. Am. J. Clin. Nutr. 2001, 74, 108–115. [Google Scholar] [CrossRef] [Green Version]
- Februhartanty, J.; Dillon, D.; Khusun, H. Will iron supplementation given during menstruation improve iron status better than weekly supplementation? Asia Pac. J. Clin. Nutr. 2002, 11, 36–41. [Google Scholar] [CrossRef]
- Gilgen, D.; Mascie-Taylor, C.G. The effect of weekly iron supplementation on anaemia and on iron deficiency among female tea pluckers in Bangladesh. J. Hum. Nutr. Diet. 2001, 14, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.; Roschnik, N.; Ouattara, F.; Touré, I.; Maiga, F.; Sacko, M.; Bendech, M.A. A randomised trial in Mali of the effectiveness of weekly iron supplements given by teachers on the haemoglobin concentrations of school children. Public Health Nutr. 2002, 5, 413–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanani, S.J.; Poojara, R.H. Supplementation with Iron and Folic Acid Enhances Growth in Adolescent Indian Girls. J. Nutr. 2000, 130, 425S–455S. [Google Scholar] [CrossRef] [PubMed]
- Muro, G.S.; Gross, U.; Gross, R.; Wahyuniar, L. Increase in compliance with weekly iron supplementation of adolescent girls by an accompanying communication programme in secondary schools in Dar-es-Salaam, Tanzania. Food Nutr. Bull. 1999, 20, 435–444. [Google Scholar] [CrossRef] [Green Version]
- Shah, B.K.; Gupta, P. Weekly vs daily iron and folic acidsupplementation in adolescent Nepalese girls. Arch. Pediatr. Adolesc. Med. 2002, 156, 131–135. [Google Scholar] [CrossRef] [Green Version]
- Shobha, S.; Sharada, D. Efficacy of twice weekly iron supplementation in anemic adolescent girls. Indian Pediatr. 2003, 40, 1186–1190. [Google Scholar]
- Soekarjo, D.D.; De Pee, S.; Kusin, J.A.; Schreurs, W.H.P.; Schultink, W.; Bloem, M.W. Effectiveness of weekly vitaminA (10,000 IU) and iron (60 mg) supplementation for adolescent boys and girls through schools in rural and urban East Java, Indonesia. Eur. J. Clin. Nutr. 2004, 58, 927–937. [Google Scholar] [CrossRef] [Green Version]
- Agha, S.; Van Rossem, R. Impact of a school-based peer sexual health intervention on normative beliefs, risk perceptions, and sexual behavior of Zambian adolescents. J. Adolesc. Health. 2004, 34, 441–452. [Google Scholar] [CrossRef]
- Drayton, V.L.; Montgomery, S.B.; Modeste, N.N.; Frye-Anderson, B.A.; McNeil, P. The impact of the Women’s Centre of Jamaica Foundation programme for adolescent mothers on repeat pregnancies. West Indian Med. J. 2000, 49, 316–326. [Google Scholar]
- Agarwal, S.S. Indian Council of Medical Research. Multicentric study of efficacy of periconceptional folic acid containing vitamin supplementation in prevention of open neural tube defects from India. Indian J. Med. Res. 2000, 112, 201–211. [Google Scholar]
- Angeles-Agdeppa, I.; Schultink, W.; Sastromidjojo, S.; Gross, R.; Karyadi, D. Weekly micronutrient supplementation to build iron stores in female Indonesian adolescents. Am. J. Clin. Nutr. 1997, 66, 177–183. [Google Scholar] [CrossRef]
- Jayatissa, R.; Piyasena, P. Adolescent school girls: Daily or weekly iron supplementation. Food Nutr. Bull. 1999, 20, 429–434. [Google Scholar] [CrossRef]
- Nguyen, P.; Grajeda, R.; Melgar, P.; Marcinkevage, J.; Flores, R.; Martorell, R. Weekly may be as efficacious as daily folic acid supplementation in improving folate status and lowering serum homocysteine concentrations in guatemalan women. J. Nutr. 2008, 138, 1491–1498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baird, S.; McIntosh, C.; Özler, B. Cash or condition? Evidence from a cash transfer experiment. Q. J. Econ. 2011, 126, 1709–1753. [Google Scholar] [CrossRef]
- Horjus, P.; Aguayo, V.M.; Roley, J.A.; Pene, M.C.; Meershoek, S.P. School-based iron and folic acid supplementation for adolescent girls: Findings from Manica Province, Mozambique. Food Nutr. Bull. 2005, 26, 281–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hindin, M.J.; Kalamar, A.M.; Thompson, T.-A.; Upadhyay, U.D. Interventions to Prevent Unintended and Repeat Pregnancy among Young People in Low- and Middle-Income Countries: A Systematic Review of the Published and Gray Literature. J. Adolesc. Health 2016, 59, S8–S15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitaker, R.; Hendry, M.; Rabeea’h Aslam, A.B.; Carter, B.; Charles, J.M.; Craine, N.; Rycroft-Malone, J. Intervention Now to Eliminate Repeat Unintended Pregnancy in Teenagers (INTERUPT): A systematic review of intervention effectiveness and cost-effectiveness, and qualitative and realist synthesis of implementation factors and user engagement. Health Technol. Assess. 2016, 20, 1. [Google Scholar] [CrossRef] [Green Version]
- Norton, M.; Chandra-Mouli, V.; Lane, C. Interventions for Preventing Unintended, Rapid Repeat Pregnancy Among Adolescents: A Review of the Evidence and Lessons From High-Quality Evaluations. Glob. Health Sci. Pract. 2017, 5, 547–570. [Google Scholar] [CrossRef] [Green Version]
- Salam, R.A.; Hooda, M.; Das, J.K.; Arshad, A.; Lassi, Z.S.; Middleton, P.; Bhutta, Z.A. Interventions to Improve Adolescent Nutrition: A Systematic Review and Meta-Analysis. J. Adolesc. Health 2016, 59, S29–S39. [Google Scholar] [CrossRef] [Green Version]
- Dean, S.V.; Lassi, Z.S.; Imam, A.M.; Bhutta, Z.A. Preconception care: Nutritional risks and interventions. Reprod. Health 2014, 11, S3. [Google Scholar] [CrossRef] [Green Version]
- De-Regil, L.M.; Peña-Rosas, J.P.; Fernández-Gaxiola, A.C.; Rayco-Solon, P. Effects and safety of periconceptional oral folate supplementation for preventing birth defects. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Gaxiola, A.C.; De-Regil, L.M. Intermittent iron supplementation for reducing anaemia and its associated impairments in menstruating women. Cochrane Database Syst. Rev. 2011. [Google Scholar] [CrossRef]
- Poels, M.; Koster, M.P.; Boeije, H.R.; Franx, A.; Van Stel, H.F. Why do women not use preconception care? A systematic review on barriers and facilitators. Obstet. Gynecol. Surv. 2016, 71, 603–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Focus of Intervention | Study | Country | Intervention | Comparison | Outcomes |
|---|---|---|---|---|---|
| Delay the age at first pregnancy | Baird et al. 2010 [27] | Malawi | Conditional cash transfer as an incentive for school girls and young women to stay or return to school | Received no conditional cash transfer | Pregnancy, initiation of sexual intercourse, condom use |
| Cabezón et al. 2005 [28] | Chile | One 45-minute class per week for a year on health education, contraceptive education, skills- building, and abstinence | No intervention | Unintended pregnancy, preterm birth, spontaneous abortion | |
| Cowan et al. 2010 [29] | Zimbabwe | The Regai Dzive Shiri Intervention consisting of an in-school teaching program, training of nurses, raising awareness, and improving communication in the community about HIV prevention | Delayed implementation | Pregnancy | |
| Daniel et al. 2008 [30] | India | PRACHAR Project, which utilized a communication intervention approach | Comparison areas were chosen because their socioeconomic conditions and accessibility were similar to those of the intervention communities | Contraception use, related attitudes, and knowledge (toward early childbearing) | |
| Diop et al. 2004 [31] | Senegal | Three-level intervention, including community-based, clinic-based, and school-based interventions | A separate community served as the control site and did not receive any of the intervention components | Knowledge and attitudes towards reproductive health (e.g., contraception, initiation of sexual intercourse) | |
| Duflo et al. 2015 [32] | Kenya | Education subsidies and HIV prevention education focused on abstinence until marriage in schools; stand-alone education subsidy program | Control schools | Teenage pregnancy rate | |
| Dupas 2011 [33] | Kenya | Schools trained teachers for sexual and reproductive health education | Control schools did not receive any of the programs | Incidence of childbearing | |
| Erulkar & Methengi 2007 [34] | Ethiopia | The Berhane Hewan program with three components: (1) social mobilization and group formation by adult female mentors; (2) participation in non-formal education and livelihoods training for out of school girls, or support to remain in school; and (3) “community conversations” | A control village, selected because of its similar socioeconomic profile | Use of birth control methods, knowledge of reproductive health topics | |
| Gallegos et al. 2008 [35] | Mexico | Behavioral-educational intervention, which included two types of intervention: (1) reduction of HIV/AIDS risk and (2) health promotion | Control group was present, limited details were provided | Use of condoms | |
| Handa et al. 2015 [36] | Kenya | Monthly cash transfer to eligible households for the care and development of orphans and vulnerable residents within the household | Delayed entry into the program, due to budget constraints | Pregnancy (ever been, likelihood), initiation of sexual intercourse | |
| James et al. 2005 [37] | South Africa | Implementation of a photo-novella (Laduma) on knowledge, attitudes, communication, and behavioral intentions with respect to sexually transmitted infections | Did not read the photo-novella | Condom use | |
| Jewkes et al. 2006 [38] | South Africa | “Stepping Stones” is an HIV prevention approach that aims to improve sexual health through building stronger, more gender-equitable relationships with better communication between partners | Control arm communities attended a single session of about 3 h on HIV and safer sex | Condom use | |
| Kaljee et al. 2005 [39] | Vietnam | The Vietnamese Focus on Kids program, designed to teach youth new skills for decision-making and communication, as well as factual information related to reproductive health | Control youth received the intervention after collection of the 18-month follow-up data | Beliefs about condom use | |
| Kanesathasan et al. 2008 [40] | India | DISHA: The Development Initiative Supporting Healthy Adolescents: program, comprising of youth groups, peer education, and income generating opportunities/skills | Control sites | Knowledge and attitudes on contraception and reproductive health services; contraceptive prevalence | |
| Klepp et al. 1997 [41] | Tanzania | Ngao, a local HIV/AIDS education program. | Delayed-intervention comparison group | Initiation of sexual intercourse | |
| Lou et al. 2004 [42] | China | Community-based sex education and reproductive health service program. | Comparable site in socio-cultural, economic, and demographic characteristics; continued to provide standard program and services | Contraception use (including details of condom use) | |
| Martiniuk et al. 2003 [43] | Belize | Responsible sexuality education program | Classrooms were randomly allocated to the control arm | Knowledge and attitudes about the risk of unintended pregnancy | |
| Meekers 2000 [44] | South Africa | Targeted social marketing program and subsidized condoms | A separate control site | Knowledge and awareness of contraceptives | |
| Mmbaga 2017 [45] | Tanzania | PREPARE, consisting of three components implemented by teachers, peer educators, and healthcare providers (linking adolescents to information and services that may foster healthy sexuality) | Half of the primary schools were assigned to the control group based on their size and geographic location | Initiation of sexual intercourse, condom use | |
| Okonofua et al. 2003 [46] | Nigeria | Intervention consisted of community participation, peer education, public lectures, health clubs in the schools, and training of sexually transmitted diseases treatment providers, including those with no formal training | Randomly selected control schools that received no intervention | Condom use | |
| Pandey et al. 2016 [47] | India | PRACHAR Project’s reproductive health training program for adolescents, which consisted of three days of training and focused on addressing adolescents’ need for information, contraceptive supplies, parental and community support, and a youth-friendly health system | A cohort of similar young people who were not exposed to the program | Use of birth control methods (modern, condoms), knowledge and attitudes about the risk of unintended pregnancies | |
| Ross et al. 2007 [48] | Tanzania | Community activities; teacher-led, peer-assisted sexual health education in years 5-7 of primary school; training and supervision of health workers to provide “youth-friendly” sexual health services; and peer condom social marketing | Standard activities | Condom use, initiation of sexual intercourse | |
| Shuey et al. 1999 [49] | Uganda | School health education program in primary schools, consisted of nine activities involving the community, parents, local leaders, teachers, students, and school health clubs | Students in the control country area were exposed to the standard school health and AIDS education program of Uganda | Abstinence | |
| Speizer et al. 2001 [50] | Cameroon | Peer education program that educated peer educators in information techniques for group discussions and on reproductive health-related topics | Comparison community, Mbalmayo | Knowledge (modern contraceptives), use of birth control methods (condom use, modern contraceptives) | |
| Walker et al. 2006 [51] | Mexico | Two interventions: (1) HIV education, skills- building, cultural values, contraceptive promotion (condoms); and (2) HIV education, skills-building, cultural values plus contraceptive education (education and communication plus condoms and their access) | Control students received the standard biology-based sex education | Initiation of sexual intercourse, use of birth control methods (condoms, hormonal contraceptive), condom use | |
| Ybarra et al. 2013 [52] | Uganda | CyberSenga, a five-hour online healthy sexuality program | Received standard program (e.g., school-delivered sexuality programming) | Condom use | |
| Optimizing inter-pregnancy intervals | Baqui et al. 2018 [53] | Uganda | Integrated post-partum family planning and maternal and newborn health interventions | Received maternal and newborn health interventions only | Preterm births, contraception use, subsequent pregnancy incidences |
| Daniel et al. 2008 [30] | India | PRACHAR Project, which utilized a communication intervention approach | Comparison areas were chosen because their socioeconomic conditions and accessibility were similar to those of the intervention communities | Contraception use, related attitudes and knowledge (toward early childbearing) | |
| Pandey et al. 2016 [47] | India | Prachar Project’s reproductive health training program for adolescents, which consists of three days of training and focused on addressing adolescents’ need for information, contraceptive supplies, parental and community support, and a youth-friendly health system | A cohort of similar young people who were not exposed to the program | Use of birth control methods (modern, condoms), knowledge and attitudes about the risk of unintended pregnancies | |
| Zhu et al. 2009 [54] | China | Two post-abortion family planning (FP) service packages: (1) package included provision of limited information and referral to existing FP services, and (2) comprehensive package with additional individual counselling, free provision of contraceptive materials, and involvement of the male partner | Comparison between the two interventions | Pregnancy, repeat abortion rate, use of birth control methods | |
| Peri-conceptional folic acid supplementation | Berry et al. 1999 [55] | China | Daily supplement containing 400 mg folic acid. Divided women who took folic acid pills according to the pattern of use based on the dates they started and stopped taking folic acid | No control, a comparison group | Neural tube defects, pregnancy outcome, pattern of use of folic acid pills |
| Li et al. 2014 [56] | China | Received folic acid but did not drink milk throughout the trial | Did not take folic acid tablets and did not drink milk throughout the trial | Serum folate concentrations | |
| Rosenthal et al. 2008 [57] | Honduras | Two supplementation groups: (1) daily dosage of 1000 μg (1 mg) folic acid, and (2) received a once-weekly dosage of 5000 μg (5 mg) | Control | Serum folate | |
| Vergel et al. 1990 [58] | Cuba | 5 mg folic acid/day for not less than one menstrual period before conception until the 10th week of pregnancy. (1) Fully supplemented: those who followed a full regime, and (2) partially supplemented | No supplementation, patients were in early stage of pregnancy | Pregnancy outcome (miscarriage, neural tube defects) | |
| Wehby et al. 2012 [59] | Brazil | Received either a single pill of 4000 μg (4 mg) folic acid or 400 μg (0.4 mg) of folic acid daily to be continued until the end of the first trimester | Historical control group | Serum folate, red blood cell folate | |
| Peri-conceptional iron-folic acid supplementation | Agarwal et al. 2003 [60] | India | Weekly or daily iron-folate (100 mg elemental iron, 500 µg of folic) | No supplementation for first 100 days, then same as daily group | Anemia, hemoglobin concentration, plasma ferritin |
| Ahmed et al. 2001 [61] | Bangladesh | Iron + folic acid (120 mg elemental Fe, 3.5 mg folic acid) | Placebo | Anemia, iron deficiency, adherence to supplementation | |
| Februhartanty et al. 2001 [62] | Indonesia | Two groups: (1) received a weekly iron tablet and (2) took an iron tablet for four consecutive days during their menstrual cycle. Iron tablet included 60 mg of elemental iron and 0.25 mg folic acid in the form of 200 mg ferrous sulphate | Placebo | Prevalence of anemia | |
| Gilgen et al. 2001 [63] | Bangladesh | Received weekly iron supplementation (200 mg ferrous fumarate and 200 mg folic acid) for 24 weeks | Placebo manufactured by the same company | Anemia | |
| Hall et al. 2002 [64] | Mali | Received weekly for tablets providing 65 mg iron and 0.25 mg folic acid for 10 weeks | No iron tablets were given | Prevalence of anemia, adherence to supplementation | |
| Kanani & Poojara 2000 [65] | India | Received iron folic acid tablets for 3 months (60 mg elemental iron + 0.5 mg folic acid per day) | Placebo supplement | Adherence to supplementation | |
| Muro et al. 1999 [66] | Tanzania | Iron-folic acid only (iron sulphate 65 mg and folic acid 0.25 mg) | No intervention | Anemia, adherence to supplementation, adverse effects | |
| Shah & Gupta2002 [67] | Nepal | Weekly vs daily iron-folic acid supplementation: (1) once daily for 90–100 days and (2) once weekly for 14 weeks; 350 mg ferrous sulfate and 1.5 mg folic acid combination | No supplementation | Anemia | |
| Shobha & Sharada 2003 [68] | India | Daily vs twice-weekly iron for a duration of 12 weeks; 60 mg iron, 0.5 mg folic acid | No pure control, comparison between duration | Adverse effects | |
| Soekarjo et al. 2004 [69] | Indonesia | Weekly 60 mg elemental iron (as ferrous sulphate) plus 250 mg folate | No supplementation | Anemia, adverse effects |
| Education Compared to No Intervention for Delaying Pregnancy | ||||||
|---|---|---|---|---|---|---|
| Patient or population: delaying at the age at first pregnancy Setting: Low- and middle-income countries (LMICs) Intervention: education Comparison: no intervention | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | No. of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with no intervention | Risk with Education | |||||
| Unintended pregnancy | Study population | RR = 0.42 (0.07 to 2.36) | 490 (2 studies) | ⊕⊕⊝⊝ LOW 1 2 | ||
| 122 per 1000 | 132 per 1000 (41 to 420) | |||||
| *The risk in the intervention group (and its 95% confidence interval) was based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio; OR: odds ratio. | ||||||
| GRADE Working Group grades of evidence: High certainty: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: We are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: Our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: We have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
| Education + Referral Services + Training of Service Providers + Counselling + Provision of Contraception + Involvement of Male Partner Compared to Education + Referral Services in Pregnancy | ||||||
|---|---|---|---|---|---|---|
| Patient or population: pregnancy Setting: LMICs Intervention: education + referral services + training of service providers + counselling + provision of contraception + involvement of male partner Comparison: education + referral services | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | No. of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with education + referral services | Risk with education + referral services + training of service providers + counselling + provision of contraception + involvement of male partner | |||||
| Unintended pregnancies | Study population | RR = 0.32 (0.01 to 7.45) | 45 (1 randomized controlled trial (RCT)) | ⊕⊕⊕⊝ MODERATE 1 2 | ||
| 45 per 1000 | 15 per 1000 (0 to 339) | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio; OR: odds ratio. | ||||||
| GRADE Working Group grades of evidence: High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.Moderate certainty: We are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: Our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: We have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
| Folic Acid Compared to Placebo for Periconceptional Women | ||||||
|---|---|---|---|---|---|---|
| Patient or population: periconceptional womenSetting: LMICs Intervention: Folic acid Comparison: Placebo | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | No. of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with placebo | Risk with folic acid | |||||
| Neural tube defects | Study population | RR = 0.53 (0.41 to 0.67) | 248,056 (2 RCTs) | ⊕⊝⊝⊝ VERY LOW 1 2 | ||
| 2 per 1000 | 1 per 1000 (1 to 1) | |||||
| *The risk in the intervention group (and its 95% confidence interval) was based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio; OR: odds ratio. | ||||||
| GRADE Working Group grades of evidence: High certainty: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: We are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: Our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: We have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
| Iron Folic Acid Compared to Placebo for Periconceptional Women | ||||||
|---|---|---|---|---|---|---|
| Patient or population: periconceptional women Setting: LMICs Intervention: Iron folic acid Comparison: Placebo | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | No. of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with placebo | Risk with iron-folic acid | |||||
| Anemia – RCTs | Study population | RR = 0.66 (0.53 to 0.81) | 3430 (6 RCTs) | ⊕⊝⊝⊝ VERY LOW 1 2 3 | ||
| 565 per 1000 | 350 per 1000 (288 to 429) | |||||
| Anemia—Weekly supplementation | Study population | RR = 0.70 (0.55 to 0.88) | 2661 (6 RCTs) | ⊕⊝⊝⊝ VERY LOW 1 2 6 | ||
| 488 per 1000 | 332 per 1000 (273 to 405) | |||||
| Anemia—Daily supplementation | Study population | RR = 0.49 (0.21 to 1.12) | 1532 (2 RCTs) | ⊕⊝⊝⊝ VERY LOW 1 2 7 | ||
| 417 per 1000 | 213 per 1000 (133 to 338) | |||||
| Anemia—8 weeks of weekly supplementation | Study population | RR = 1.17 (0.55 to 1.67) | 159(1 RCTs) | ⊕⊝⊝⊝ VERY LOW4 5 8 | ||
| 249 per 1000 | 237 per 1000 (142 to 394) | |||||
| Anemia—10 weeks of weekly supplementation | Study population | RR = 0.75 (0.64 to 0.88) | 552 (1 RCT) | ⊕⊕⊝⊝ VERY LOW 4 9 | ||
| 609 per 1000 | 456 per 1000 (389 to 536) | |||||
| Anemia—12 weeks of weekly supplementation | Study population | RR = 0.39 (0.27 to 0.57) | 145 (1 RCTs) | ⊕⊝⊝⊝ VERY LOW 1 2 4 7 | ||
| 398 per 1000 | 187 per 1000 (108 to 327) | |||||
| Anemia—14 weeks of weekly supplementation | Study population | RR = 0.21 (0.11 to 0.39) | 139 (1 RCT) | ⊕⊕⊝⊝ LOW 4 10 | ||
| 653 per 1000 | 137 per 1000 (72 to 255) | |||||
| Anemia—16 weeks of weekly supplementation | Study population | RR = 0.89 (0.79 to 0.99) | 1386 (1 RCT) | ⊕⊕⊕⊝ MODERATE 9 | ||
| 504 per 1000 | 448 per 1000 (398 to 499) | |||||
| Anemia—24 weeks of weekly supplementation | Study population | RR = 0.85 (0.77 to 0.94) | 280 (1 RCT) | ⊕⊕⊝⊝ LOW 4 11 | ||
| 915 per 1000 | 778 per 1000 (704 to 860) | |||||
| Anemia—School | Study population | RR = 0.66 (0.51to 0.86) | 3005 (4 RCTs) | ⊕⊝⊝⊝ VERY LOW 1 2 12 | ||
| 459 per 1000 | 257 per 1000 (206 to 326) | |||||
| Anemia—Work | Study population | RR = 0.59 (0.24 to 1.43) | 425 (2 RCTs) | ⊕⊝⊝⊝ VERY LOW 4 13 14 | ||
| 863 per 1000 | 509 per 1000 (207 to 1000) | |||||
| *The risk in the intervention group (and its 95% confidence interval) was based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio; OR: odds ratio. | ||||||
| GRADE Working Group grades of evidence: High certainty: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: We are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: Our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: We have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lassi, Z.S.; Kedzior, S.G.E.; Tariq, W.; Jadoon, Y.; Das, J.K.; Bhutta, Z.A. Effects of Preconception Care and Periconception Interventions on Maternal Nutritional Status and Birth Outcomes in Low- and Middle-Income Countries: A Systematic Review. Nutrients 2020, 12, 606. https://doi.org/10.3390/nu12030606
Lassi ZS, Kedzior SGE, Tariq W, Jadoon Y, Das JK, Bhutta ZA. Effects of Preconception Care and Periconception Interventions on Maternal Nutritional Status and Birth Outcomes in Low- and Middle-Income Countries: A Systematic Review. Nutrients. 2020; 12(3):606. https://doi.org/10.3390/nu12030606
Chicago/Turabian StyleLassi, Zohra S., Sophie G. E. Kedzior, Wajeeha Tariq, Yamna Jadoon, Jai K. Das, and Zulfiqar A. Bhutta. 2020. "Effects of Preconception Care and Periconception Interventions on Maternal Nutritional Status and Birth Outcomes in Low- and Middle-Income Countries: A Systematic Review" Nutrients 12, no. 3: 606. https://doi.org/10.3390/nu12030606