Effects of Leucine-Enriched Whey Protein Supplementation on Physical Function in Post-Hospitalized Older Adults Participating in 12-Weeks of Resistance Training Program: A Randomized Controlled Trial

 , ,
, , 
Abstract
:1. Introduction
2. Methods
2.1. Study Design
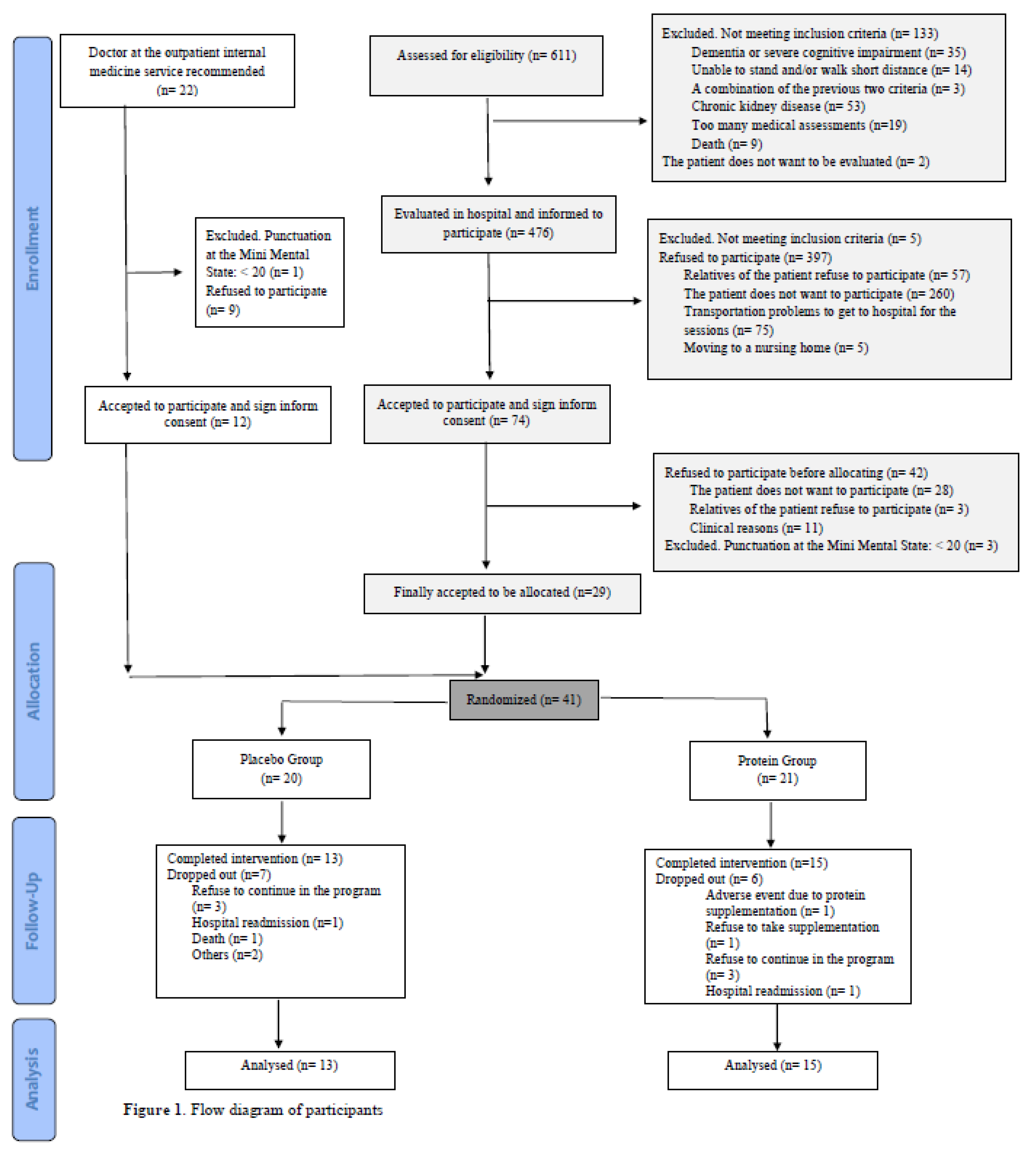
2.2. Participants
2.3. Randomization
2.4. Supplementation and Blinding
2.5. Design of the Resistance Training Program
2.6. Outcome Measures
2.7. Primary Outcome: Physical Function
2.8. Secondary Outcomes
2.8.1. Nutritional Assessment
2.8.2. Body Composition
2.8.3. Biochemical Parameters
2.9. Statistical Analysis
3. Results
3.1. Effects of the Intervention on Primary Outcomes: Physical Function
3.2. Effects of the Intervention on Secondary Outcomes
4. Discussion
Limitations and Strength
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fielding, R.A.; Vellas, B.; Evans, W.J.; Bhasin, S.; Morley, J.E.; Newman, A.B.; Abellan van Kan, G.; Andrieu, S.; Bauer, J.; Breuille, D.; et al. Sarcopenia: An undiagnosed condition in older adults. Current consensus definition: Prevalence, etiology, and consequences. International working group on sarcopenia. J. Am. Med. Dir. Assoc. 2011, 12, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Schaap, L.A.; van Schoor, N.M.; Lips, P.; Visser, M. Associations of sarcopenia definitions, and their components, with the incidence of recurrent falling and fractures: The Longitudinal Aging Study Amsterdam. J. Gerontol. 2018, 73, 1199–1204. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Heymsfield, S.B.; Ross, R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J. Am. Geriatr. Soc. 2002, 50, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Liperoti, R.; Fusco, D.; Mastropaolo, S.; Quattrociocchi, D.; Proia, A.; Tosato, M.; Bernabei, R.; Onder, G. Sarcopenia and mortality among older nursing home residents. J. Am. Med. Dir. Assoc. 2012, 13, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, W.K.; Williams, J.; Atherton, P.; Larvin, M.; Lund, J.; Narici, M. Sarcopenia, dynapenia, and the impact of advancing age on human skeletal muscle size and strength; a quantitative review. Front. Physiol. 2012, 11, 260. [Google Scholar] [CrossRef] [PubMed]
- Witard, O.C.; McGlory, C.; Hamilton, D.L.; Phillips, S.M. Growing older with health and vitality: A nexus of physical activity, exercise and nutrition. Biogerontology 2016, 17, 529–546. [Google Scholar] [CrossRef]
- Deutz, N.E.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznariç, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breen, L.; Phillips, S.M. Skeletal muscle protein metabolism in the elderly: Interventions to counteract the ‘anabolic resistance’ of ageing. Nutr. Metab. 2011, 8, 68. [Google Scholar] [CrossRef]
- Hung, Y.; Wijnhoven, H.A.H.; Visser, M.; Verbeke, W. Appetite and Protein Intake Strata of Older Adults in the European Union: Socio-Demographic and Health Characteristics, Diet-Related and Physical Activity Behaviours. Nutrients 2019, 11, 777. [Google Scholar] [CrossRef]
- Lonnie, M.; Hooker, E.; Brunstrom, J.M.; Corfe, B.M.; Green, M.A.; Watson, A.W.; Williams, E.A.; Stevenson, E.J.; Penson, S.; Johnstone, A.M. Protein for Life: Review of Optimal Protein Intake, Sustainable Dietary Sources and the Effect on Appetite in Ageing Adults. Nutrients 2018, 10, 360. [Google Scholar] [CrossRef]
- Pennings, B.; Boirie, Y.; Senden, J.M.; Gijsen, A.P.; Kuipers, H.; van Loon, L.J. Whey protein stimulates postprandial muscle protein accretion more effectively than do casein and casein hydrolysate in older men. Am. J. Clin. Nutr. 2011, 93, 997–1005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaafsma, G. Advantages and limitations of the protein digestibility-corrected amino acid score (PDCAAS) as a method for evaluating protein quality in human diets. Br. J. Nutr. 2012, 108 (Suppl. 2), S333–S336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Vliet, S.; Burd, N.A.; van Loon, L.J. The Skeletal Muscle Anabolic Response to Plant- versus Animal-Based Protein Consumption. J. Nutr. 2015, 145, 1981–1991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pennings, B.; Groen, B.; de Lange, A.; Gijsen, A.P.; Zorenc, A.H.; Senden, J.M.; van Loon, L.J. Amino acid absorption and subsequent muscle protein accretion following graded intakes of whey protein in elderly men. Am. J. Physiol. Endocrinol. Metab. 2012, 302, E992–E999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luiking, Y.C.; Deutz, N.E.; Memelink, R.G.; Verlaan, S.; Wolfe, R.R. Postprandial muscle protein synthesis is higher after a high whey protein, leucine-enriched supplement than after a dairy-like product in healthy older people: A randomized controlled trial. Nutr. J. 2014, 13, 9. [Google Scholar] [CrossRef] [PubMed]
- Reidy, P.T.; Rasmussen, B.B. Role of Ingested Amino Acids and Protein in the Promotion of Resistance Exercise-Induced Muscle Protein Anabolism. J. Nutr. 2016, 146, 155–183. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.D.; Tsauo, J.Y.; Wu, Y.T.; Cheng, C.P.; Chen, H.C.; Huang, Y.C.; Chen, H.C.; Liou, T.H. Effects of protein supplementation combined with resistance exercise on body composition and physical function in older adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2017, 106, 1078–1109. [Google Scholar] [CrossRef]
- Thomas, D.K.; Quinn, M.A.; Saunders, D.H.; Greig, C.A. Protein Supplementation Does Not Significantly Augment the Effects of Resistance Exercise Training in Older Adults: A Systematic Review. J. Am. Med. Dir. Assoc. 2016, 17, 959.e1–959.e9. [Google Scholar] [CrossRef] [Green Version]
- Krumholz, H.M. Post-hospital syndrome--an acquired, transient condition of generalized risk. N. Engl. J. Med. 2013, 368, 100–102. [Google Scholar] [CrossRef]
- Deer, R.R.; Goodlett, S.M.; Fisher, S.R.; Baillargeon, J.; Dickinson, J.M.; Raji, M.; Volpi, E. A Randomized Controlled Pilot Trial of Interventions to Improve Functional Recovery After Hospitalization in Older Adults: Feasibility and Adherence. J. Gerontol. 2018, 73, 187–193. [Google Scholar] [CrossRef]
- Kaiser, M.J.; Bauer, J.M.; Ramsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.; Charlton, K.E.; Maggio, M.; et al. Validation of the Mini Nutritional Assessment short-form (MNA-SF): A practical tool for identification of nutritional status. J. Nutr. Health Aging 2009, 13, 782–788. [Google Scholar] [CrossRef]
- Soares Menezes, K.V.R.; Auger, C.; de Souza Menezes, W.R.; Guerra, R.O. Instruments to evaluate mobility capacity of older adults during hospitalization: A systematic review. Arch. Gerontol. Geriatr. 2017, 72, 67–79. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Martínez de la Iglesia, J.; Dueñas Herrero, R.; Onís Vilches, M.C.; Aguado Taberné, C.; Albert Colomer, C.; Luque Luque, R. Cross-cultural adaptation and validation of Pfeiffer’s test (Short Portable Mental Status Questionnaire [SPMSQ]) to screen cognitive impairment in general population aged 65 or older. Med. Clín. 2001, 117, 129–134. [Google Scholar] [CrossRef]
- Brzycki, M. Strength testing: Predicting a one-rep max from reps-to-fatigue. J. Phys. Educ. Recreat. Danc. 1993, 64, 88–90. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Development and validation of criterion-referenced clinically relevant fitness standards for maintaining physical independence in later years. Gerontologist 2013, 53, 255–267. [Google Scholar] [CrossRef]
- Guigoz, Y. The Mini Nutritional Assessment (MNA) review of the literature: What does it tell us? J. Nutr. Health Aging. 2006, 10, 466–485. [Google Scholar]
- Chumlea, W.C.; Roche, A.F.; Steinbaugh, M.L. Estimating stature from knee height for persons 60 to 90 years of age. J. Am. Geriatr. Soc. 1985, 33, 116–120. [Google Scholar] [CrossRef]
- Leenders, M.; Verdijk, L.B.; van der Hoeven, L.; van Kranenburg, J.; Nilwik, R.; van Loon, L.J. Elderly men and women benefit equally from prolonged resistance-type exercise training. J. Gerontol. 2013, 68, 769–779. [Google Scholar] [CrossRef]
- Law, T.D.; Clark, L.A.; Clark, B.C. Resistance Exercise to Prevent and Manage Sarcopenia and Dynapenia. Annu. Rev. Gerontol. Geriatr. 2016, 36, 205–228. [Google Scholar] [CrossRef] [Green Version]
- Liao, C.D.; Lee, P.H.; Hsiao, D.J.; Huang, S.W.; Tsauo, J.Y.; Chen, H.C.; Liou, T.H. Effects of Protein Supplementation Combined with Exercise Intervention on Frailty Indices, Body Composition, and Physical Function in Frail Older Adults. Nutrients 2018, 10, 1916. [Google Scholar] [CrossRef]
- Deutz, N.E.P.; Ashurst, I.; Ballesteros, M.D.; Bear, D.E.; Cruz-Jentoft, A.J.; Genton, L.; Landi, F.; Laviano, A.; Norman, K.; Prado, C.M. The Underappreciated Role of Low Muscle Mass in the Management of Malnutrition. J. Am. Med. Dir. Assoc. 2019, 20, 22–27. [Google Scholar] [CrossRef] [Green Version]
- Koopman, R.; van Loon, L.J. Aging, exercise, and muscle protein metabolism. J. Appl. Physiol. 2009, 106, 2040–2048. [Google Scholar] [CrossRef]
- Pennings, B.; Koopman, R.; Beelen, M.; Senden, J.M.; Saris, W.H.; van Loon, L.J. Exercising before protein intake allows for greater use of dietary protein-derived amino acids for de novo muscle protein synthesis in both young and elderly men. Am. J. Clin. Nutr. 2011, 93, 322–331. [Google Scholar] [CrossRef]
- Tieland, M.; van de Rest, O.; Dirks, M.L.; van der Zwaluw, N.; Mensink, M.; van Loon, L.J.; de Groot, L.C. Protein supplementation improves physical performance in frail elderly people: A randomized, double-blind, placebo-controlled trial. J. Am. Med. Dir. Assoc. 2012, 13, 720–726. [Google Scholar] [CrossRef]
- Mori, H.; Tokuda, Y. Effect of whey protein supplementation after resistance exercise on the muscle mass and physical function of healthy older women: A randomized controlled trial. Geriatr. Gerontol. Int. 2018, 18, 1398–1404. [Google Scholar] [CrossRef] [Green Version]
- Verdijk, L.B.; Jonkers, R.A.; Gleeson, B.G.; Beelen, M.; Meijer, K.; Savelberg, H.H.; Wodzig, W.K.; Dendale, P.; van Loon, L.J. Protein supplementation before and after exercise does not further augment skeletal muscle hypertrophy after resistance training in elderly men. Am. J. Clin. Nutr. 2009, 89, 608–616. [Google Scholar] [CrossRef]
- Verhoeven, S.; Vanschoonbeek, K.; Verdijk, L.B.; Koopman, R.; Wodzig, W.K.; Dendale, P.; van Loon, L.J. Long-term leucine supplementation does not increase muscle mass or strength in healthy elderly men. Am. J. Clin. Nutr. 2009, 89, 1468–1475. [Google Scholar] [CrossRef]
- Slivka, D.; Raue, U.; Hollon, C.; Minchev, K.; Trappe, S. Single muscle fiber adaptations to resistance training in old (>80 yr) men: Evidence for limited skeletal muscle plasticity. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2008, 295, R273–R280. [Google Scholar] [CrossRef]
- Cartee, G.D.; Hepple, R.T.; Bamman, M.M.; Zierath, J.R. Exercise Promotes Healthy Aging of Skeletal Muscle. Cell Metab. 2016, 23, 1034–1047. [Google Scholar] [CrossRef] [Green Version]
- Atherton, P.J.; Kumar, V.; Selby, A.L.; Rankin, D.; Hildebrandt, W.; Phillips, B.E.; Williams, J.P.; Hiscock, N.; Smith, K. Enriching a protein drink with leucine augments muscle protein synthesis after resistance exercise in young and older men. Clin. Nutr. 2017, 36, 888–895. [Google Scholar] [CrossRef]
- Englund, D.A.; Kirn, D.R.; Koochek, A.; Zhu, H.; Travison, T.G.; Reid, K.F.; von Berens, Å.; Melin, M.; Cederholm, T.; Gustafsson, T.; et al. Nutritional Supplementation with Physical Activity Improves Muscle Composition in Mobility-Limited Older Adults, The VIVE2 Study: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Gerontol. 2017, 73, 95–101. [Google Scholar] [CrossRef]
- Wilkinson, D.J.; Bukhari, S.S.I.; Phillips, B.E.; Limb, M.C.; Cegielski, J.; Brook, M.S.; Rankin, D.; Mitchell, W.K.; Kobayashi, H.; Williams, J.P.; et al. Effects of leucine-enriched essential amino acid and whey protein bolus dosing upon skeletal muscle protein synthesis at rest and after exercise in older women. Clin. Nutr. 2018, 37, 2011–2021. [Google Scholar] [CrossRef]
- Morton, R.W.; Murphy, K.T.; McKellar, S.R.; Schoenfeld, B.J.; Henselmans, M.; Helms, E.; Aragon, A.A.; Devries, M.C.; Banfield, L.; Krieger, J.W.; et al. A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. Br. J. Sports Med. 2018, 52, 376–384. [Google Scholar] [CrossRef]
- Hou, L.; Lei, Y.; Li, X.; Huo, C.; Jia, X.; Yang, J.; Xu, R.; Wang, X. Effect of Protein Supplementation Combined with Resistance Training on Muscle Mass, Strength and Function in the Elderly: A Systematic Review and Meta-Analysis. J. Nutr. Health Aging 2019, 23, 451–458. [Google Scholar] [CrossRef]
- Wall, B.T.; Gorissen, S.H.; Pennings, B.; Koopman, R.; Groen, B.B.; Verdijk, L.B.; van Loon, L.J. Aging Is Accompanied by a Blunted Muscle Protein Synthetic Response to Protein Ingestion. PLoS ONE 2015, 10, e0140903. [Google Scholar] [CrossRef]
- Macnaughton, L.S.; Wardle, S.L.; Witard, O.C.; McGlory, C.; Hamilton, D.L.; Jeromson, S.; Lawrence, C.E.; Wallis, G.A.; Tipton, K.D. The response of muscle protein synthesis following whole-body resistance exercise is greater following 40 g than 20 g of ingested whey protein. Physiol. Rep. 2016, 4, e12893. [Google Scholar] [CrossRef]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Park, Y.; Choi, J.E.; Hwang, H.S. Protein supplementation improves muscle mass and physical performance in undernourished prefrail and frail elderly subjects: A randomized, double-blind, placebo-controlled trial. Am. J. Clin. Nutr. 2018, 108, 1026–1033. [Google Scholar] [CrossRef]
- Stokes, T.; Hector, A.J.; Morton, R.W.; McGlory, C.; Phillips, S.M. Recent Perspectives Regarding the Role of Dietary Protein for the Promotion of Muscle Hypertrophy with Resistance Exercise Training. Nutrients 2018, 10, 180. [Google Scholar] [CrossRef]
- Campbell, W.W.; Leidy, H.J. Dietary protein and resistance training effects on muscle and body composition in older persons. J. Am. Coll. Nutr. 2007, 26, 696S–703S. [Google Scholar] [CrossRef]
- Peterson, M.D.; Sen, A.; Gordon, P.M. Influence of resistance exercise on lean body mass in aging adults: A meta-analysis. Med. Sci. Sports Exerc. 2011, 43, 249–258. [Google Scholar] [CrossRef]


{kind=link}
| Nutritional Composition | Protein Supplement |
|---|---|
| Β-lactoglobulin (g/bottle) | 20 |
| L-Leucine (g/bottle) | 3 |
| Sodium saccharin (g/bottle) | 0.050 |
| Sucralose (g/bottle) | 0.030 |
| Lemon flavor 654500 (g/bottle) | 0.250 |
| Placebo supplement | |
| Maltodextrin (g/bottle) | 23 |
| Hydroxyethylcellulose (g/bottle) | 0.200 |
| Lemon flavor 654500 (g/bottle) | 0.250 |
| N | Placebo Group | N | Protein Group | p | |
|---|---|---|---|---|---|
| Age (years) | 13 | 81.7 (6.45) | 15 | 82.9 (5.59) | 0.607 |
| Women (N, %) | 13 | 7 (53.8) | 15 | 7 (46.7) | 0.717 |
| Body mass (kg) | 13 | 75.9 (17.95) | 15 | 68.0 (11.43) | 0.188 |
| BMI (Kg/m2) | 13 | 30.8 (6.53) | 15 | 27.4 (3.50) | 0.110 |
| Physical Function | |||||
| Handgrip (kg/body mass) | 13 | 0.3 (0.09) | 15 | 0.4 (0.09) | 0.063 |
| SFT chair stand test 30sec | 13 | 10.6 (4.17) | 15 | 12.3 (2.97) | 0.229 |
| SFT arm curl test 30sec | 13 | 13.5 (5.22) | 15 | 16.3 (3.92) | 0.137 |
| SFT 6MWT (m) | 13 | 314.8 (139.36) | 15 | 411.5 (80.40) | 0.040 |
| SPPB total punctuation | 13 | 8.7 (2.36) | 15 | 10.1 (1.58) | 0.089 |
| SPPB 5Squat | 13 | 14.7 (6.85) | 15 | 12.2 (2.86) | 0.232 |
| Body composition | |||||
| Waist to hip ratio | 13 | 1.00 (0.07) | 15 | 0.98 (0.09) | 0.459 |
| Lean mass arms (kg) | 13 | 2.3 (0.67) | 15 | 2.3 (0.44) | 0.897 |
| Lean mass legs (kg) | 13 | 6.8 (1.70) | 15 | 6.4 (1.08) | 0.441 |
| Lean mass trunk (kg) | 13 | 23.0 (4.83) | 15 | 21.5 (3.89) | 0.380 |
| Total lean mass (kg) | 13 | 45.2 (9.85) | 15 | 42.3 (6.63) | 0.391 |
| Fat mass arms (%) | 13 | 2.6 (0.96) | 15 | 2.4 (0.77) | 0.545 |
| Fat mass legs (%) | 13 | 5.8 (1.85) | 15 | 5.4 (1.84) | 0.603 |
| Fat mass trunk (%) | 13 | 17.1 (3.87) | 15 | 14.9 (3.03) | 0.124 |
| Total fat mass (%) | 13 | 35.4 (8.05) | 15 | 32.1 (6.84) | 0.259 |
| Nutritional Status | |||||
| MNA score | 13 | 23.1 (3.82) | 15 | 24.5 (2.11) | 0.273 |
| Normal nutritional status (N, %) | 13 | 4 (30.8) | 15 | 11 (73.3) | 0.064 |
| At risk of malnutrition (N, %) | 13 | 8 (61.5) | 15 | 4 (26.7) | |
| Malnourished (N, %) | 13 | 1 (7.7) | 15 | 0 (0) | |
| Biomarkers | |||||
| Creatinine (mg/dL) | 10 | 1.1 (0.48) | 15 | 0.9 (0.35) | 0.401 |
| Albumin (g/dL) | 13 | 4.0 (0.39) | 15 | 4.0 (0.31) | 0.994 |
| Prealbumin (mg/dL) | 12 | 22.2 (6.63) | 14 | 23.3 (4.31) | 0.613 |
| Placebo-Group | Protein-Group | Differences between Groups | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Pre | Post | p | N | Pre | Post | p | Δ Placebo | Δ Protein | p | |
| Primary outcome | |||||||||||
| Physical function | |||||||||||
| Handgrip (kg/body mass) | 13 | 0.3 (0.09) | 0.3 (0.09) | 0.775 | 15 | 0.4 (0.09) | 0.4 (0.09) | 0.651 | 0.0 (0.03) | -0.0 (0.06) | 0.971 |
| SFT chair stand test 30sec | 13 | 10.6 (4.17) | 13.5 (4.59) | 0.003 | 15 | 12.3 (2.97) | 14.4 (3.22) | <0.001 | 2.8 (2.79) | 2.1 (1.53) | 0.480 |
| SFT arm curl test 30sec | 13 | 13.5 (5.22) | 21.9 (4.66) | <0.001 | 15 | 16.3 (3.92) | 23.5 (4.53) | <0.001 | 8.4 (5.74) | 7.2 (4.86) | 0.724 |
| SFT 6min WT (m) | 13 | 314.8 (139.36) | 375.0 (128.39) | 0.002 | 15 | 411.5 (80.4) | 455.1 (81.77) | 0.005 | 60.2 (53.67) | 43.6 (51.2) | 0.959 |
| SPPB total score | 13 | 8.7 (2.36) | 10.3 (1.89) | 0.001 | 15 | 10.1 (1.58) | 11.3 (0.96) | 0.002 | 1.6 (1.39) | 1.2 (1.21) | 0.634 |
| SPPB 5Squat | 13 | 14.7 (6.85) | 10.6 (3.67) | 0.005 | 15 | 12.2 (2.86) | 10.0 (2.81) | 0.004 | −4.1 (4.32) | –2.2 (2.4) | 0.491 |
| Secondary outcomes | |||||||||||
| Body composition | |||||||||||
| Body mass (kg) | 13 | 75.9 (17.95) | 75.6 (18.31) | 0.621 | 15 | 68.0 (11.43) | 68.3 11.07) | 0.500 | −0.3 (2.24) | 0.3 (1.60) | 0.471 |
| BMI (kg/m2) | 13 | 30.8 (6.54) | 30.7 (6.64) | 0.575 | 15 | 27.4 (3.5) | 27.5 (3.37) | 0.453 | −0.3 (2.24) | 0.3 (1.60) | 0.493 |
| Waist to hip ratio | 13 | 1.00 (0.07) | 1.00 (0.08) | 0.818 | 15 | 0.98 (0.09) | 0.96 (0.08) | 0.255 | −0.0 (0.06) | −0.0 (0.05) | 0.400 |
| Lean mass arms (kg) | 13 | 2.3 (0.67) | 2.3 (0.41) | 0.937 | 15 | 2.3 (0.44) | 2.2 (0.41) | 0.049 | 0.0 (0.36) | −0.1 (0.24) | 0.088 |
| Lean mass legs (kg) | 13 | 6.8 (1.7) | 6.9 (1.45) | 0.630 | 15 | 6.4 (1.08) | 6.5 (1.04) | 0.260 | 0.1 (0.64) | 0.1 (0.34) | 0.756 |
| Lean mass trunk (kg) | 13 | 23.0 (4.83) | 22.6 (4.47) | 0.212 | 15 | 21.5 (3.88) | 21.7 (3.61) | 0.198 | −0.4 (1.21) | 0.2 (0.67) | 0.128 |
| Total lean mass (kg) | 13 | 45.2 (9.85) | 44.7 (8.54) | 0.545 | 15 | 42.3 (6.63) | 42.5 (6.61) | 0.458 | −0.4 (2.52) | 0.2 (1.02) | 0.611 |
| Fat mass arms (%) | 13 | 2.6 (0.96) | 2.6 (0.85) | 0.808 | 15 | 2.4 (0.77) | 2.3 (0.92) | 0.291 | −0.0 (0.56) | −0.1 (0.41) | 0.575 |
| Fat mass legs (%) | 13 | 5.8 (1.85) | 5.9 (2.07) | 0.165 | 15 | 5.4 (1.84) | 5.5 (1.69) | 0.506 | 0.2 (0.45) | 0.1 (0.46) | 0.549 |
| Fat mass trunk (%) | 13 | 17.1 (3.86) | 16.7 (3.31) | 0.448 | 15 | 14.9 (3.03) | 15.7 (2.61) | 0.061 | −0.4 (1.86) | 0.7 (1.31) | 0.297 |
| Total fat mass (%) | 13 | 35.4 (8.05) | 35.2 (7.53) | 0.728 | 15 | 32.1 (6.84) | 32.7 (6.64) | 0.092 | −0.2 (1.91) | 0.6 (1.31) | 0.357 |
| Nutritional status | |||||||||||
| MNA score | 13 | 23.1 (3.8) | 25.3 (2.2) | 0.010 | 15 | 24.5 (2.1) | 26.2 (1.6) | 0.019 | 2.2 (2.6) | 1.7 (2.5) | 0.512 |
| Normal nutritional status (N. %) | 13 | 4(30.8) | 9(69.3) | 0.123 | 15 | 11(73.3) | 14(93.4) | 0.533 | |||
| At risk of malnutrition (N. %) | 13 | 8(61.6) | 4(30.8) | 15 | 4(26.7) | 1(6.7) | |||||
| Malnourished (N. %) | 13 | 1(7.7) | 0 | 15 | 0 | 0 | |||||
| Biomarkers | |||||||||||
| Creatinine (mg/dL) | 10 | 1.1 (0.48) | 1.1 (0.37) | 0.664 | 15 | 0.9 (0.35) | 0.9 (0.32) | 0.595 | 0.0 (0.21) | 0.0 (0.14) | 0.438 |
| Albumin (g/dL) | 13 | 3.9 (0.39) | 4.1 (0.31) | 0.189 | 15 | 3.9 (0.31) | 4.0 (0.26) | 0.499 | 0.1 (0.22) | 0.0 (0.15) | 0.331 |
| Prealbumin (mg/dL) | 12 | 22.2 (6.63) | 20.5 (4.48) | 0.221 | 14 | 23.3 (4.31) | 21.3 (4.17) | 0.019 | −1.6 (4.36) | −1.9 (2.77) | 0.916 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amasene, M.; Besga, A.; Echeverria, I.; Urquiza, M.; Ruiz, J.R.; Rodriguez-Larrad, A.; Aldamiz, M.; Anaut, P.; Irazusta, J.; Labayen, I. Effects of Leucine-Enriched Whey Protein Supplementation on Physical Function in Post-Hospitalized Older Adults Participating in 12-Weeks of Resistance Training Program: A Randomized Controlled Trial. Nutrients 2019, 11, 2337. https://doi.org/10.3390/nu11102337
Amasene M, Besga A, Echeverria I, Urquiza M, Ruiz JR, Rodriguez-Larrad A, Aldamiz M, Anaut P, Irazusta J, Labayen I. Effects of Leucine-Enriched Whey Protein Supplementation on Physical Function in Post-Hospitalized Older Adults Participating in 12-Weeks of Resistance Training Program: A Randomized Controlled Trial. Nutrients. 2019; 11(10):2337. https://doi.org/10.3390/nu11102337
Chicago/Turabian StyleAmasene, Maria, Ariadna Besga, Iñaki Echeverria, Miriam Urquiza, Jonatan R. Ruiz, Ana Rodriguez-Larrad, Mikel Aldamiz, Pilar Anaut, Jon Irazusta, and Idoia Labayen. 2019. "Effects of Leucine-Enriched Whey Protein Supplementation on Physical Function in Post-Hospitalized Older Adults Participating in 12-Weeks of Resistance Training Program: A Randomized Controlled Trial" Nutrients 11, no. 10: 2337. https://doi.org/10.3390/nu11102337