1. Introduction
Taste preference (TP) is one of the factors that affect the children’s food intake and eating habits [
1]. Humans can perceive 6 main basic tastes: (1) Sweet taste is caused by sugar and its derivatives such as fructose or lactose, but other substances such as amino acids and alcohol in fruit juices or alcoholic drinks can also activate the sensory cells that respond to sweetness; (2) Sour taste is mostly perceived via acidic solutions such as lemon juice or organic acids and is caused by hydrogen ions; (3) Salty taste is mainly perceived through foods containing table salt. Its chemical basis is the salt crystal, which consists of sodium and chloride. The sensation of saltiness can be caused by other mineral salts such as potassium or magnesium salts [
2]; (4) Bitter taste is brought by a variety of components such as 6-
n-propylthiouracil (PROP), sinigrin and goitrin, found in cruciferous vegetables (e.g., broccoli). There are 25 bitter taste receptors in humans but the most studied is
TAS2R38. Genetic variations in this receptor cause different responses in taste sensitivity to bitter compounds from one human to another [
3]; (5) Umami taste is caused by glutamic acid or aspartic acid and is similar to the taste of meat broth. It is also found in some plants, such as ripe tomatoes or asparagus [
4]; (6) Fatty taste, called Oleogustus, has been described as the sixth basic taste. The stimuli devoted to the detection of dietary fat taste are the Non-Esterified Fatty Acids (NEFA). In particular, medium and long-chain fatty acids have a distinct taste sensation compared to other basic tastes (sweet, bitter, sour and salty) [
5,
6].
Evidence for the influencing role of genetic and environmental factors on the development of TP is well established [
7]. Infants prefer the sweet taste and reject the sour and bitter tastes [
7], while the preference for salt appears at about 4 months postnatally [
8,
9]. TP are learned during contact with food and the eating environment. An infant’s experience with flavors begins in the mother’s womb and during lactation, when flavors from the mother’s diet are transmitted to her amniotic fluid, and later to her colostrum and milk. The infant-feeding method parents choose, whether it is breast or formula milk, will later influence their child-feeding practices [
10,
11] and the development of their children’s food preferences and food acceptance patterns [
12].
The fundamental role of breastfeeding on different physiological functions and on the infant’s early immunity has been recognized through international nutritional policies, such as the World Health Organization guidelines on early life feeding, which recommends the exclusive breastfeeding of infants up to the age of 6 months and at least for the first 4 months of life [
13]. Exclusive breastfeeding is crucial for the growth and development of infants [
14], has a long term impact in shaping children’s eating behaviors, and predicts the Body Mass Index (BMI) during childhood [
15] and later in adult life [
16]. Previous studies have pointed out the positive influence of breastfeeding duration on food variety and higher intake of fruits and vegetables in preschoolers [
17,
18], including in 4 European cohorts [
19] and in school-aged children [
20,
21]. Vital compounds in the human milk provide a specific taste, such as lactose for the sweet taste, glutamate for the umami or savory taste, sodium for the salty taste, urea for the bitter taste and long-chain fatty acids for the fatty taste [
22,
23].
The introduction of formula milk and other complementary foods represents a crucial period for establishing infants’ taste preferences and attitudes towards food, as well as for obesity prevention [
24]. Children who were fed exclusively with formula milk do not benefit from the rich flavor profile of their mother’s milk: their flavor experience is poorer as they don’t experience the flavors from the variety of foods in the mother’s diet. Various types and brands of formula milk products offer a diversity of flavors: milk-based formulas are described as having low levels of sweetness and ‘sour and cereal-type’; soy-based formulas are described as tasting sweeter, more sour and bitter, and having a ‘hay/beany’ odor, whereas the hydrolysate formulas are extremely unpalatable to adults due to their sourness and bitterness [
25]. Formula-fed infants learn to prefer the flavors associated with the formula milk they were fed and this has been found to influence taste preferences later in life [
3,
25]. Infant formulas might differ in protein, fat and carbohydrate composition and/or structure, and these differences may, in turn, affect growth, health outcomes and taste preferences [
26].
Scott et al. demonstrated that breastfeeding duration is directly associated with the food variety at two years of age [
18], independent of factors that are known to influence diet quality in children, such as maternal age and education [
27,
28]. Another study found that having been breastfed was positively associated with a healthier dietary pattern amongst older Australian children [
20]. Burnier et al. [
29] investigated longitudinal data from the Quebec Longitudinal Study of Child Development and observed that 3 or more months of exclusive breastfeeding appeared to be a predictive factor for the higher consumption of vegetables in preschool age children. Nicklaus and colleagues found that 2–8 year old children who were breastfed for at least three or more months were more likely to eat vegetables compared to those who were breastfed for a shorter time [
30]. A number of animal studies [
31,
32] and experimental studies in humans [
33,
34] indicated that breastfeeding is associated with a greater acceptability of new food and flavors during the weaning period. Breastfeeding can contribute towards reducing infants’ fears to try new foods and facilitate the transition from milk feeding to solid food eating with lower resistance. Consequently, this can lead to an intake of a higher food variety in breastfed children [
3,
21,
35,
36].
Although research has shown that breastfeeding influences infants’ food acceptance [
22,
37,
38,
39], to our knowledge, no studies have examined whether it shapes taste preferences in later stages of life. This study seeks to fill this gap by examining how breastfeeding practices—in comparison to formula milk feeding—during infancy, affect food TP in later childhood and adolescence, in a population-based cohort of normal, healthy developing children aged 6 to 16 years old, in 7 European countries: Cyprus, Estonia, Germany, Hungary, Italy, Spain and Sweden.
To be exact, we examined the association between infant feeding practices duration (FP): (1) exclusive breastfeeding (EBF), (2) exclusive formula milk feeding (EFMF) and (3) combined strategy (BF&FMF), and taste preferences (TP) evaluated in our study: sweet, fatty and bitter. We further considered a latent class analysis to identify feeding patterns from a combination of feeding practices and food introduction, and their association with taste preferences.
4. Discussion
To our knowledge, this is the first study assessing the association between different infant FPs and children’s taste preferences in later stages in life which included retrospective and current data from 7 European countries. Our results indicate that European children were predominantly breastfed exclusively for at least 4 months, which is in line with the WHO guidelines [
13]. In addition, almost half of the subjects had a long duration of BF&FMF and only a minority (13%) was exclusively fed FM. The feeding strategy parents used seemed not to play a role in the development of taste preferences later in life, irrespective of whether it was EBF, EFMF or a combination. Using both single logistic regression analyses and LCA methods, in which latent profiles of all FP and introduction of complementary food categories were identified, a higher quality diet (HDAS) was observed to be associated with lower chances for a high sweet and high-fat taste preference and increased chances for high bitter taste preference. This suggests that current food choices can actually mold children’s preferences for sweet, fat and bitter tastes, independent of their infant feeding patterns. SES also seemed to play a role, as children who came from a lower SES background were more likely to prefer the fatty taste compared to those from a higher SES background. Our results indicate that a variation in food choice and parental education can affect children’s behaviors towards healthy food choices and preferences.
Our findings are supported by the current evidence, which suggests that children have innate preferences for sweet taste as signalers of high energy foods [
3,
8]. Further, Schwartz et al. reported that infants’ sweet acceptance was not related to longer durations of EBF [
22]. In a longitudinal study, Desor and colleagues measured the sweet preference in children at the age of 11–15 years and again when they were 19–25 years of age, and found that the preferred levels of sucrose decreased over time [
59]. Other studies have suggested that children learn to prefer flavors associated with a high dietary fat content [
60,
61]. Previous findings from the IDEFICS study indicated that children from low educational backgrounds tended to eat more high energy-dense foods, such as sugar-rich and fat-rich foods, compared to those whose parents had a high education [
62]. In contrast, children of parents with a higher education tended to eat more fruits and vegetables, generally eating less unhealthy foods. They were also more likely to eat breakfast on a daily basis, emphasizing the influence of parental education on children’s eating habits [
47,
63,
64,
65,
66,
67]. Furthermore, a higher number of fruits and vegetables at 14 months has been shown to increase the preference for these foods and improve the quality of the diet at 3.7 years of age [
68]. Our results, which are supported by the current evidence, suggest that taste preferences in children are learned via food experience and are significantly influenced by the food choice and diet literacy of parents. Thus, public health education programs should emphasize the role of food variety in shaping children’s preferences for bitter tasting foods in the long term. Particular attention needs to be paid to parents and other caretakers of low to medium socio-economic status families in order to help them reduce their children’s preferences for high energy-dense foods.
5. Strengths and Limitations
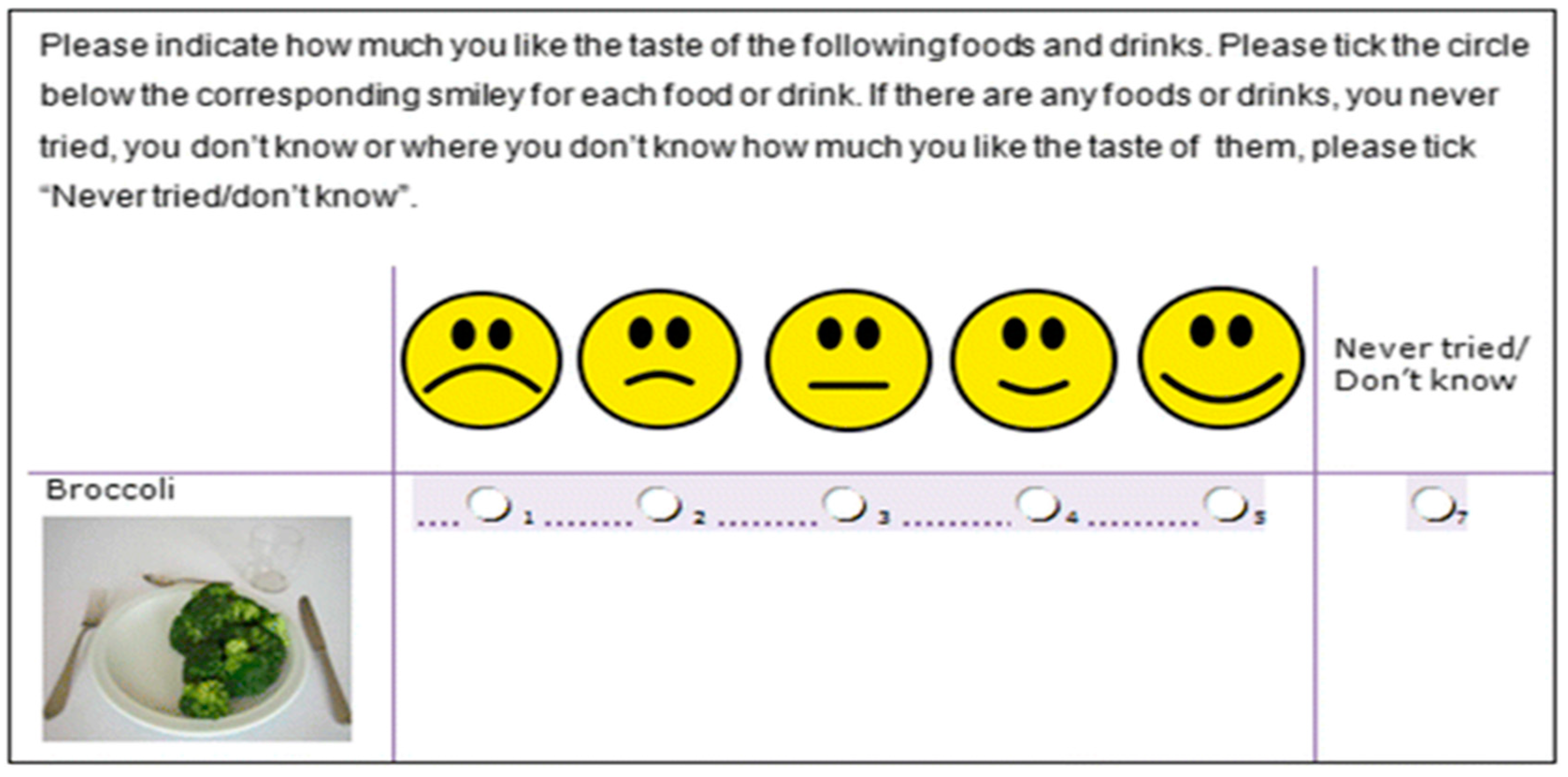
One of the main strengths of our study is the large sample size of 5526 children and adolescents from 7 European countries, which allowed us to have a detailed picture of FP and its potential association with taste preferences in later stages of life. The standardized protocol and the pre-test conducted in a subsample of children showed that the Food and Beverage Preference Questionnaire is a feasible instrument for assessing preferences of food and beverages in children and adolescents.
Furthermore, having information on covariates such as country of residence, age, sex, HDAS, the timing of the first introduction of complementary feeding, parental education level and migration status allowed us to make adjustments and to control for confounding.
Nevertheless, there are important methodological limits concerning our research. The scale of the taste preference was slightly limited as it was calculated based on measuring the food preference with only 5 points. This limited our ability to clearly distinguish between extreme taste preferences. Further, in the BF&FMF category, information on the proportion of actual formula milk and breastmilk feeding was not provided. Thus, we have to acknowledge this as a limitation as it hampers a critical discussion on the potential effects of a mixed strategy of feeding on taste preference.
Since mothers self-reported the details of their infants’ FP (age at starting and termination of infant feeding, the timing of the first introduction of complementary foods) and as adolescents tend to self-report a lower preference for energy-dense (fatty and sweet) foods and beverages [
69,
70], we cannot entirely exclude social desirability bias. As we used retrospective information on feeding practices, recall bias also potentially affected our data. The reproducibility testing of the early infant parameters showed a weak reproducibility of maternal reports on early infant nutrition, a further potential limitation [
71]. Nevertheless, research has shown that mothers recall breastfeeding duration accurately [
72,
73], while the recall of age at introduction of complementary food is less satisfactory [
73]. Moreover, the parents of half of our sample had a high educational status, a fact which might also bias the results with regard to socio-economic status. In addition, we did not have information on other confounding factors such as the role of the maternal diet during breastfeeding and the family diet, factors that have been found to influence taste preference and food intake in children [
3,
55,
74]. Lastly, our research was conducted using only cross-sectional data enriched with retrospective information. We strongly recommend further longitudinal research, e.g., through birth cohorts, that can evaluate the effects of FP during infancy and changes of taste preferences during different stages of life, particularly accounting for the interplay between food choice and socio-economic background.

 ,
, 



{kind=link}