Surgical Site Infection Following Caesarean Section by Acinetobacter Species: A Report from a Hyperendemic Setting in the Brazilian Amazon Region

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Clinical Data Collection
2.2. Bacterial Isolates and Antimicrobial Susceptibility Testing
2.3. Acinetobacter Species Identification
2.4. Detection of Carbapenemase-Encoding Genes
2.5. Genotyping by rep-PCR and Multilocus Sequence Typing
2.6. Statistical Analysis
3. Results
3.1. Demographic and Clinical Data
3.2. Confirmation of Acinetobacter Species, Antimicrobial Susceptibility Testing, and Carbapenemase Gene Detection
3.3. Complications of Post-Caesarean SSI by Susceptible and Carbapenem-Resistant Acinetobacter spp.
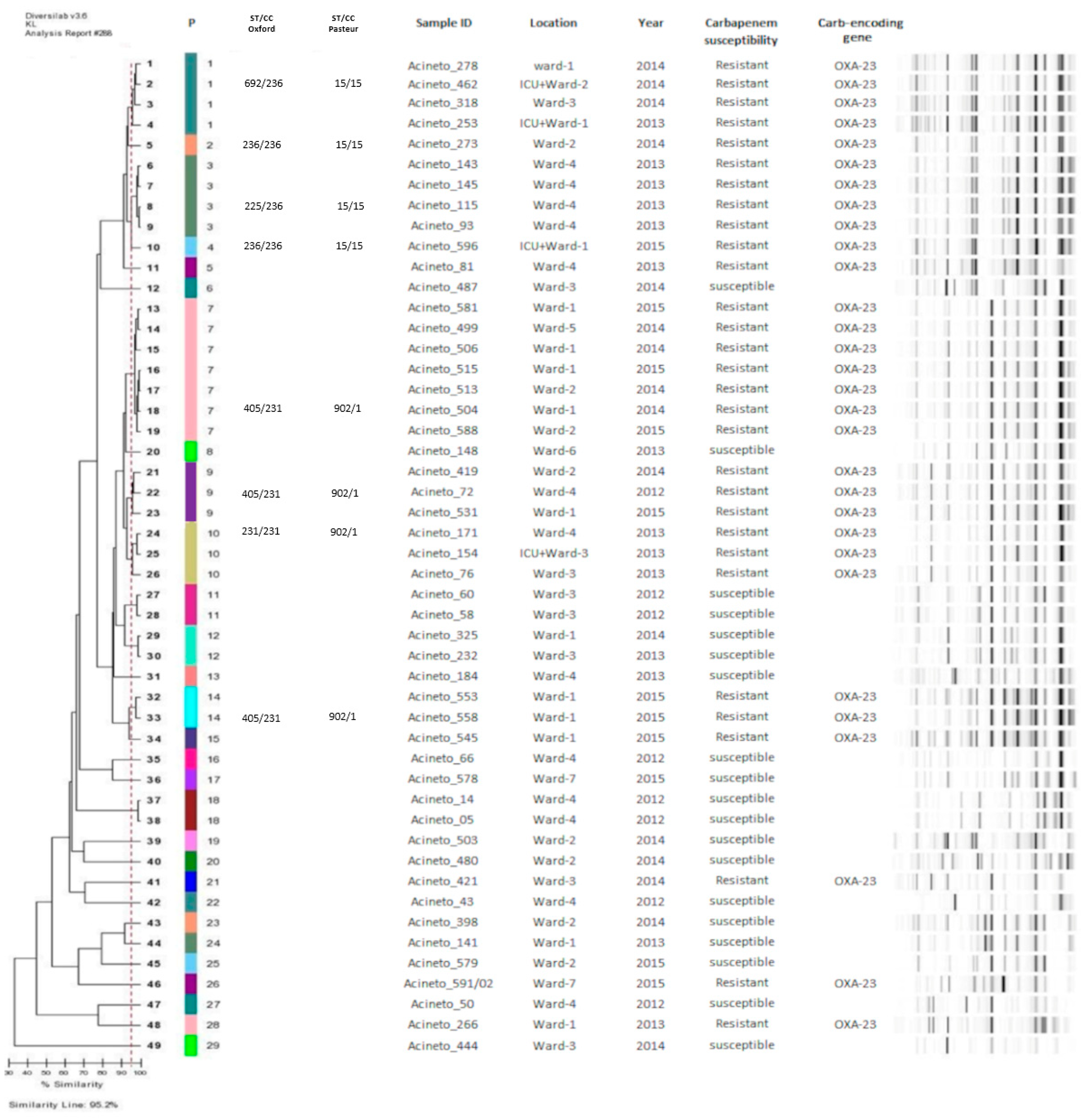
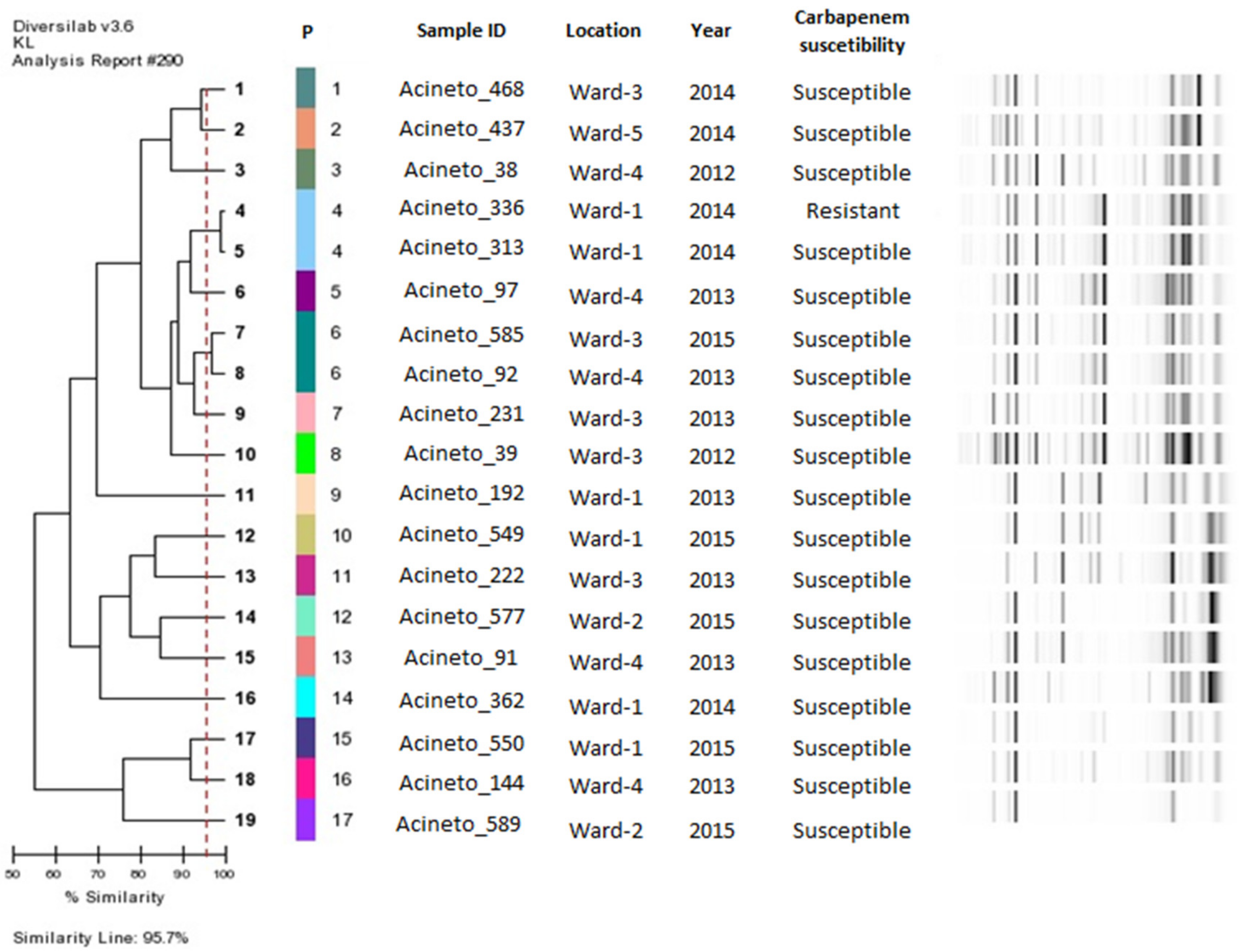
3.4. rep-PCR and MLST Genotyping
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Delamou, A.; Camara, B.S.; Sidibé, S.; Camara, A.; Dioubaté, N.; El Ayadi, A.M.; Tayler-Smith, K.; Beavogui, A.H.; Baldé, M.D.; Zachariah, R. Trends of and factors associated with cesarean section related surgical site infections in Guinea. J. Public Health Afr. 2019, 10, 31–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dillen, J.; Zwart, J.; Schutte, J. Van Roosmalen, J. Maternal sepsis: Epidemiology, etiology and outcome. Curr. Opin. Infect. Dis. 2010, 23, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Lapinsky, S.E. Obstetric Infections. Crit. Care Clin. 2013, 29, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Molina, G.; Weiser, T.G.; Lipsitz, S.R.; Esquivel, M.M.; Uribe-Leitz, T.; Azad, T.; Shah, N.; Semrau, K.; Berry, W.R.; Gawande, A.A.; et al. Relationship between cesarean delivery rate and maternal and neonatal mortality. J. Am. Med. Assoc. 2015, 314, 2263–2270. [Google Scholar] [CrossRef] [PubMed]
- Sway, A.; Nthumba, P.; Solomkin, J.; Tarchini, G.; Gibbs, R.; Ren, Y.; Wanyoro, A. Burden of surgical site infection following cesarean section in sub-Saharan Africa: A narrative review. Int. J. Womens Health. 2019, 11, 309–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeed, K.B.; Corcoran, P.; O’Riordan, M.; Greene, R.A. Risk factors for surgical site infection after cesarean delivery: A case-control study. Am. J. Infect. Control. 2018, 47, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Killian, C.A.; Graffunder, E.M.; Vinciguerra, T.J.; Venezia, R.A. Risk Factors for Surgical-Site Infections Following Cesarean Section. Infect. Control Hosp. Epidemiol. 2001, 22, 613–617. [Google Scholar] [CrossRef] [PubMed]
- Agboeze, J.; Onoh, R.C.; Umeora, O.U.J.; Paul, O. Ezeonu, Chukwuemeka Ukaegbe, Azubike, K. Onyebuchi CE, Ndukwe, E. Microbiological pattern of postcesarean wound infection at Federal Teaching Hospital, Abakaliki. Afr. J. Med. Health Sci. 2013, 12, 97–102. [Google Scholar]
- Yang, Y.; Lee, Y.; Tsai, W.; Kuo, S.; Sun, J.; Yang, C.; Chen, T.; Lin, J.; Fung, C.; Chang, F. Comparison between bacteremia caused by carbapenem resistant Acinetobacter baumannii and Acinetobacter nosocomialis. BMC Infect. Dis. 2013, 13, 311. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Prioritization of Pathogens to Guide Discovery, Research and Development of New Antibiotics for Drug-Resistant Bacterial Infections, Including Tuberculosis; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Durante-Mangoni, E.; Utili, R.; Zarrilli, R. Combination therapy in severe Acinetobacter baumannii infections: An update on the evidence to date. Future Microbiol. 2014, 9, 773–789. [Google Scholar] [CrossRef]
- Cosgaya, C.; Ratia, C.; Marí-Almirall, M.; Rubio, L.; Higgins, P.G.; Seifert, H.; Roca, I.; Vila, J. In vitro and in vivo Virulence Potential of the Emergent Species of the Acinetobacter baumannii (Ab) Group. Front. Microbiol. 2019, 10, 2429. [Google Scholar] [CrossRef]
- De Vos, D.; Pirnay, J.P.; Bilocq, F.; Jennes, S.; Verbeken, G.; Rose, T.; Keersebilck, E.; Bosmans, P.; Pieters, T.; Hing, M.; et al. Molecular epidemiology and clinical impact of acinetobacter calcoaceticus-baumannii complex in a belgian burn wound center. PLoS ONE 2016, 11, e0156237. [Google Scholar] [CrossRef] [PubMed]
- Hammerum, A.M.; Hansen, F.; Skov, M.N.; Stegger, M.; Andersen, P.S.; Holm, A.; Jakobsen, L.; Justesen, U.S. Investigation of a possible outbreak of carbapenem-resistant Acinetobacter baumannii in Odense, Denmark using PFGE, MLST and whole-genome-based SNPs. J. Antimicrob. Chemother. 2015, 70, 1965–1968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berriós-Torres, S.I.; Umscheid, C.A.; Bratzler, D.W.; Leas, B.; Stone, E.C.; Kelz, R.R.; Reinke, C.E.; Morgan, S.; Solomkin, J.S.; Mazuski, J.E.; et al. Centers for disease control and prevention guideline for the prevention of surgical site infection. JAMA Surg. 2017, 152, 784–791. [Google Scholar] [CrossRef]
- Patel, J.B.; Weinstein, M.; Eliopoulos, G.; Jenkins, S.; Lewis, J.; Limbago, B. M100 Performance Standards for Antimicrobial Susceptibility Testing, 30th ed.; United State, Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2020; Volume 8. [Google Scholar] [CrossRef]
- Magiorakos, A.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La, S.B.; Gundi, V.A.K.B.; Khamis, A.; Raoult, D. Sequencing of the rpoB Gene and Flanking Spacers for Molecular Identification of Acinetobacter Species. J. Clin. Microbiol. 2006, 44, 827–832. [Google Scholar]
- Woodford, N.; Ellington, M.J.; Coelho, J.M.; Turton, J.F.; Ward, M.E.; Brown, S.; Amyes, S.G.; Livermore, D.M. Multiplex PCR for genes encoding prevalent OXA carbapenemases in Acinetobacter spp. Int. J. Antimicrob. Agents 2006, 27, 351–353. [Google Scholar] [CrossRef]
- Mendes, R.E.; Castanheira, M.; Toleman, M.A.; Sader, H.S.; Jones, R.N.; Walsh, T.R. Characterization of an integron carrying blaIMF-1 and a new aminoglycoside resistance gene, aac(6′)-31, and its dissemination among genetically unrelated clinical isolates in a Brazilian Hospital. Antimicrob. Agents Chemother. 2007, 51, 2611–2614. [Google Scholar] [CrossRef] [Green Version]
- Bartual, S.G.; Seifert, H.; Hippler, C.; Luzon, M.A.; Wisplinghoff, H.; Rodríguez-Valera, F. Development of a multilocus sequence typing scheme for characterization of clinical isolates of Acinetobacter baumannii. J. Clin. Microbiol. 2005, 43, 4382–4390. [Google Scholar] [CrossRef] [Green Version]
- Diancourt, L.; Passet, V.; Nemec, A.; Dijkshoorn, L.; Brisse, S. The population structure of Acinetobacter baumannii: Expanding multiresistant clones from an ancestral susceptible genetic pool. PLoS ONE 2010, 5, e10034. [Google Scholar] [CrossRef] [Green Version]
- ANVISA—Agência Nacional de Vigilância Sanitária. Boletim de Segurança do Paciente e Qualidade em Serviços de Saúde no 16: Avaliação dos indicadores nacionais das Infecções Relacionadas à Assistência à Saúde (IRAS) e Resistência microbiana do ano de 2016. Anvisa 2016, 16, 1–12. [Google Scholar]
- Bebell, L.M.; Ngonzi, J.; Bazira, J.; Fajardo, Y.; Boatin, A.A.; Siedner, M.J.; Bassett, I.V.; Nyehangane, D.; Nanjebe, D.; Jacquemyn, Y.; et al. Antimicrobial-resistant infections among postpartum women at a Ugandan referral hospital. PLoS ONE 2017, 12, e0175456. [Google Scholar] [CrossRef] [PubMed]
- Abdelraheim, A.R.; Gomaa, K.; Ibrahim, E.M.; Mohammed, M.M.; Khalifa, E.M.; Youssef, A.M.; Abdelhakeem, A.K.; Hassan, H.; Abdelghany, A.; El Gelany, S. Intra-abdominal infection (IAI) following cesarean section: A retrospective study in a tertiary referral hospital in Egypt. BMC Pregnancy Childbirth 2019, 19, 1. [Google Scholar] [CrossRef] [Green Version]
- Miller, A.E.; Morgan, C.; Vyankandondera, J. Causes of puerperal and neonatal sepsis in resource-constrained settings and advocacy for an integrated community-based postnatal approach. Int. J. Gynecol. Obstet. 2013, 123, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.; Wloch, C.; Saei, A.; McDougall, C.; Harrington, P.; Charlett, A.; Lamagni, T.; Elgohari, S.; Sheridan, E. Inter-hospital comparison of rates of surgical site infection following caesarean section delivery: Evaluation of a multicentre surveillance study. J. Hosp. Infect. 2013, 84, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Warde, E.; Davies, E.; Ward, A. Control of a multidrug-resistant Acinetobacter baumannii outbreak. Br. J. Nurs. (Mark. Allen Publ.) 2019, 28, 242–248. [Google Scholar] [CrossRef]
- Saeed, K.B.; Corcoran, P.; Greene, R.A. Incisional surgical site infection following cesarean section: A national retrospective cohort study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 240, 256–260. [Google Scholar] [CrossRef]
- Clímaco, E.C.; de Pitondo-Silva, A.O.M.L.; Oliveira, M.G.; Medeiros, M.; Lincopan, N.; Darini, A.L.D.C. Clonal complexes 104, 109 and 113 playing a major role in the dissemination of OXA-carbapenemase-producing Acinetobacter baumannii in Southeast Brazil. Infect. Genet. Evol. 2013, 19, 127–133. [Google Scholar]
- Coelho-Souza, T.; Reis, J.N.; Martins, N.; Martins, I.S.; Menezes, A.O.; Reis, M.G.; Silva, N.O.; Dias, R.C.S.; Riley, L.W.; Moreira, B.M. Longitudinal surveillance for meningitis by Acinetobacter in a large urban setting in Brazil. Clin. Microbiol. Infect. 2013, 19, E241–E244. [Google Scholar] [CrossRef] [Green Version]
- Stietz, M.S.; Ramírez, M.S.; Vilacoba, E.; Merkier, A.K.; Limansky, A.S.; Centrón, D.; Catalano, M. Acinetobacter baumannii extensively drug resistant lineages in Buenos Aires hospitals differ from the international clones I-III. Infect. Genet. Evol. 2013, 14, 294–301. [Google Scholar] [CrossRef]
- Knight, D.B.; Rudin, S.D.; Bonomo, R.A.; Rather, P.N. Acinetobacter nosocomialis: Defining the role of efflux pumps in resistance to antimicrobial therapy, surface motility, and biofilm formation. Front. Microbiol. 2018, 9, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Nemec, A.; Radolfova-Krizova, L.; Maixnerova, M.; Sedo, O. Acinetobacter colistiniresistens sp. Nov. (formerly genomic species 13 sensu Bouvet and Jeanjean and genomic species 14 sensu Tjernberg and Ursing), isolated from human infections and characterized by intrinsic resistance to polymyxins. Int. J. Syst. Evol. Microbiol. 2017, 67, 2134–2141. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| N | % | |
|---|---|---|
| Gestational age (weeks) | ||
| Preterm (<37 weeks) | 25 | 36% |
| Full-term (37 to 41 weeks) | 36 | 52% |
| Post-term (>41 weeks) | 0 | 0% |
| N.I | 8 | 12% |
| Personal morbidities | ||
| Chronic noncommunicable diseases | 16 | 23% |
| Chronic communicable diseases | 3 | 4% |
| Infectious diseases | 4 | 6% |
| Anemia | 3 | 4% |
| No morbidities | 42 | 60% |
| N.I | 2 | 3% |
| Caesarean indication | ||
| CPD | 4 | 6% |
| Hypertensive diseases of pregnancy | 14 | 20% |
| PROM | 7 | 10% |
| Fetal distress | 14 | 20% |
| Fetal death | 2 | 3% |
| Sexually Transmitted Infections | 5 | 7% |
| Others | 19 | 28% |
| N.I | 4 | 6% |
| Sexually transmitted infections | ||
| Yes | 10 | 14% |
| No | 52 | 75% |
| N.I | 7 | 10% |
| Abortion | ||
| Yes | 13 | 19% |
| No | 55 | 80% |
| N.I | 1 | 1% |
| Gynecological complications | ||
| Yes | 35 | 51% |
| No | 28 | 41% |
| N.I | 6 | 9% |
| Age (years) | ||
| 12 a 19 | 20 | 29% |
| 20 a 35 | 45 | 65% |
| 36 a 46 | 4 | 6% |
| Marital status | ||
| Married | 6 | 9% |
| Single/unmarried | 12 | 17% |
| Stable union | 37 | 54% |
| N.I | 14 | 20% |
| Education level | ||
| Elementary and middle school | 27 | 40% |
| High school | 27 | 39% |
| University Education | 3 | 4% |
| N.I | 12 | 17% |
| Profession/occupation | ||
| Housewife | 30 | 43% |
| Student | 8 | 12% |
| Teacher | 2 | 3% |
| Autonomous | 2 | 3% |
| Others | 14 | 20% |
| N.I | 13 | 19% |
| Antimicrobial | A. baumannii (N = 49) | Non-A. baumannii (N = 20) | p-Value * | ||
|---|---|---|---|---|---|
| S | NS | S | NS | ||
| SAM | 18 | 31 | 19 | 1 | <0.0001 † |
| TZP | 17 | 32 | 17 | 3 | 0.0002 † |
| CTX | 1 | 48 | 3 | 17 | 0.0702 |
| CAZ | 15 | 34 | 19 | 1 | <0.0001 † |
| FEP | 15 | 34 | 19 | 1 | <0.0001 † |
| IMP | 19 | 30 | 19 | 1 | <0.0001 † |
| MEM | 19 | 30 | 19 | 1 | <0.0001 † |
| GEN | 17 | 32 | 20 | 0 | <0.0001 † |
| AMK | 33 | 16 | 20 | 0 | 0.0033 † |
| CIP | 15 | 34 | 20 | 0 | <0.0001 † |
| TIG | 49 | 0 | 20 | 0 | >0.9999 |
| COL | 48 | 1 | 20 | 0 | >0.9999 |
| Complications | Carbapenem Resistant (N = 31) n (%) | Carbapenem Susceptible (N = 38) n (%) | p-Value * |
|---|---|---|---|
| Re-suture time (hours) | |||
| >1 | 2 (6%) | 2 (5%) | 1.0000 |
| <1 | 25 (81%) | 30 (79%) | |
| Number of re-sutures | |||
| 1 | 17 (55%) | 33 a (87%) | 0.0007 † |
| 2 | 12 a (39%) | 2 (5%) | |
| Other surgeries | |||
| Yes | 12 a (39%) | 4 (11%) | 0.0091 † |
| No | 19 (61%) | 34 a (89%) | |
| Prolonged wound healing (days) | |||
| 1–20 | 9 b (29%) | 25 a (66%) | 0.0044 † |
| 21–40 | 18 a (58%) | 10 b (26%) | |
| 41–62 | 2 (6%) | 0 | |
| Culture (days) | |||
| 4–20 | 15 (48%) | 32 a (84%) | 0.0003 † |
| 21–40 | 9 a (29%) | 2 b (5%) | |
| 41–62 | 5 a (16%) | 0 b | |
| Sepsis | |||
| Yes | 4 a (13%) | 0 | 0.0364 † |
| No | 27 (87%) | 38 a (100%) | |
| Wound dehiscence | |||
| Yes | 23 (74%) | 30 (79%) | 0.7760 |
| Not | 8 (26%) | 8 (21%) | |
| Hospitalization (days) | |||
| 6–30 | 13 (42%) | 29 a (76%) | 0.0060 † |
| >30 | 18 a (58%) | 9 (24%) | |
| Antibiotic use (days) | |||
| 3–11 | 0 b | 8 a (21%) | 0.0003 † |
| 12–36 | 21 (68%) | 28 (74%) | |
| > | 10 a (32%) | 2 b (5%) | |
| Antibiotic therapy | |||
| Adequate | 2 (6%) | 35 a (92%) | <0.0001 † |
| Inadequate | 29 a (94%) | 3 (8%) | |
| Nº of antimicrobials used in the therapy | |||
| 1–3 | 8 b (25.8%) | 16 (42.1%) | |
| 4–6 | 19 (61.3%) | 22 (57.9%) | 0.0271 † |
| >6 | 4 (12.9%) | 0 b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cabral, B.G.; Brasiliense, D.M.; Furlaneto, I.P.; Rodrigues, Y.C.; Lima, K.V.B. Surgical Site Infection Following Caesarean Section by Acinetobacter Species: A Report from a Hyperendemic Setting in the Brazilian Amazon Region. Microorganisms 2021, 9, 743. https://doi.org/10.3390/microorganisms9040743
Cabral BG, Brasiliense DM, Furlaneto IP, Rodrigues YC, Lima KVB. Surgical Site Infection Following Caesarean Section by Acinetobacter Species: A Report from a Hyperendemic Setting in the Brazilian Amazon Region. Microorganisms. 2021; 9(4):743. https://doi.org/10.3390/microorganisms9040743
Chicago/Turabian StyleCabral, Blenda Gonçalves, Danielle Murici Brasiliense, Ismari Perini Furlaneto, Yan Corrêa Rodrigues, and Karla Valéria Batista Lima. 2021. "Surgical Site Infection Following Caesarean Section by Acinetobacter Species: A Report from a Hyperendemic Setting in the Brazilian Amazon Region" Microorganisms 9, no. 4: 743. https://doi.org/10.3390/microorganisms9040743