
Intrauterine Transmission of Zika and Vertical Transfer of Neutralizing Antibodies Detected Immediately at Birth in Oaxaca, Mexico: An Analysis in the Context of Microcephaly

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
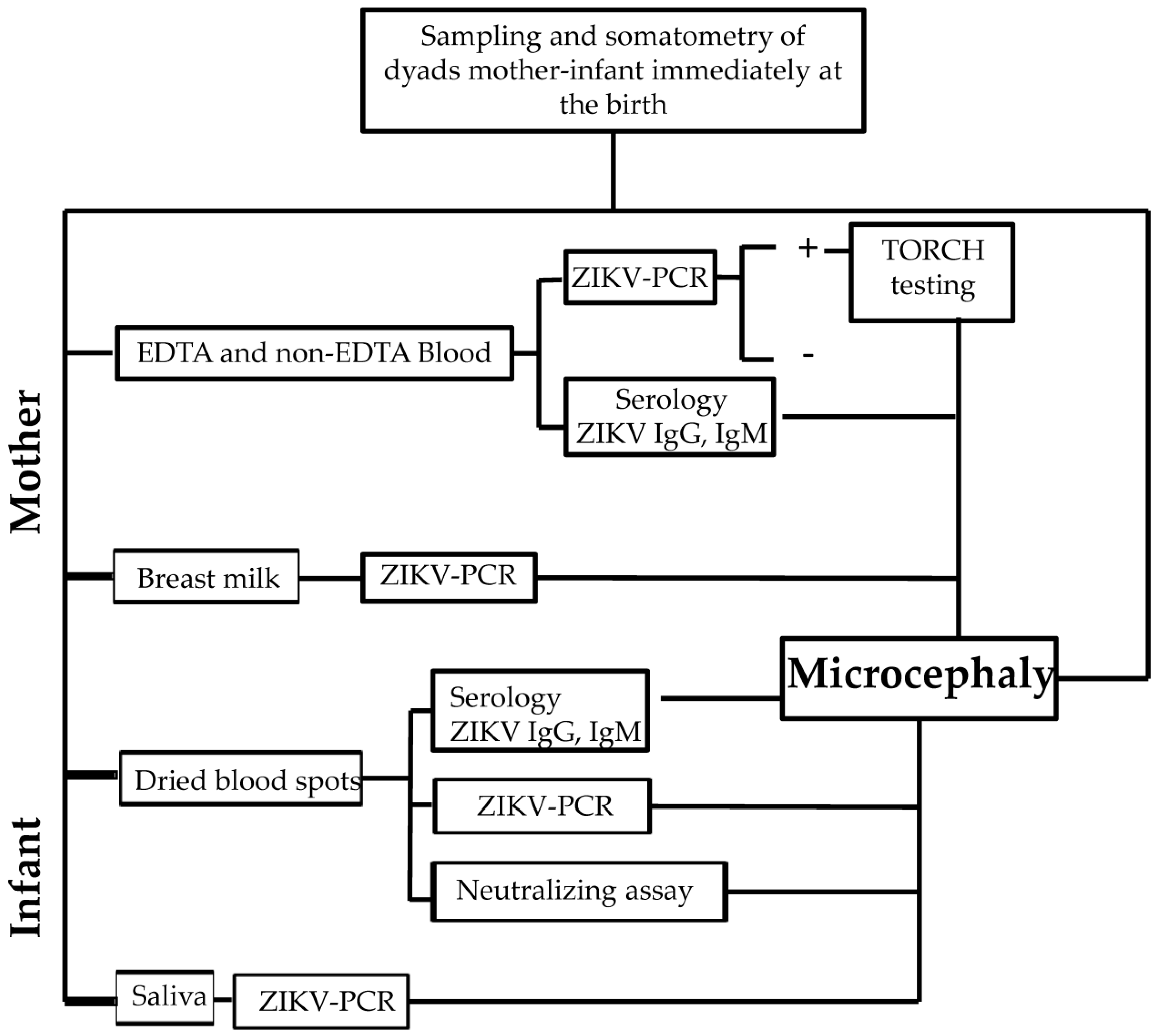
2.1. Study Design
2.2. Study Protocol and Samples
2.3. Serology
2.4. RT-PCR
2.5. TORCH
2.6. Titration of the ZIKV Strain
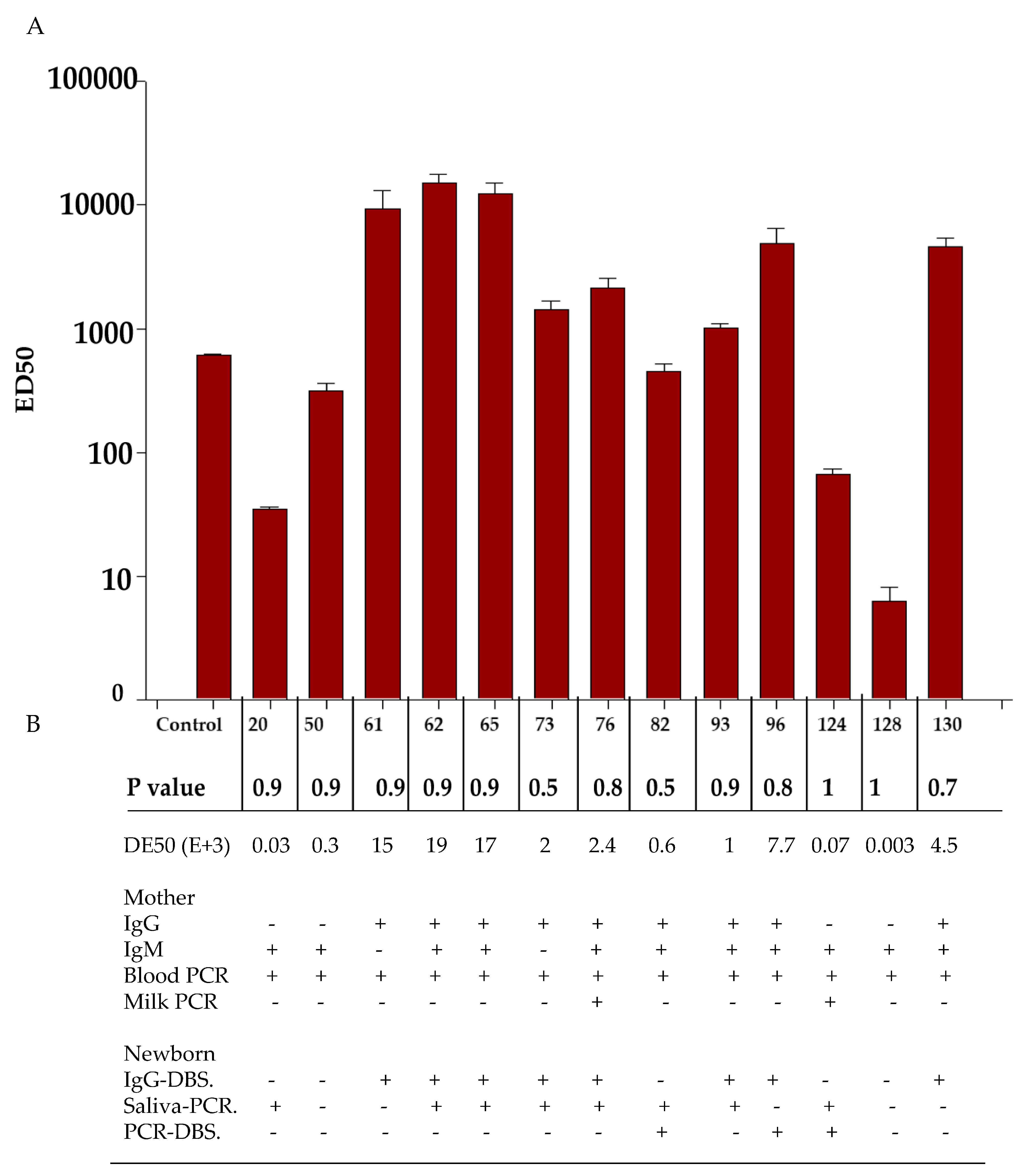
2.7. Neutralizing Assay
2.8. Variable Definitions
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sirohi, D.; Kuhn, R.J. Zika virus structure, maturation, and receptors. J. Infect. Dis. 2017, 216 (Suppl. S10), S935–S944. [Google Scholar] [CrossRef]
- Simpson, D.I. Zika virus infection in man. Trans. R. Soc. Trop. Med. Hyg. 1964, 58, 335–338. [Google Scholar] [CrossRef]
- Duffy, M.; Chen, T.; Hancock, W.; Powers, A.; Kool, J.; Lanciotti, R.; Pretrick, M.; Marfel, M.; Holzbauer, S.; Dubray, C.; et al. Zika Virus Outbreak on Yap Island, Federated States of Micronesia. N. Engl. J. Med. 2009, 360, 2536–2543. [Google Scholar] [CrossRef]
- Wikan, N.; Smith, D.R. Zika virus: History of a newly emerging arbovirus. Lancet Infect. Dis. 2016, 16, e119–e126. [Google Scholar] [CrossRef] [PubMed]
- Guanche-Garcell, H.; Gutiérrez García, F.; Ramirez Nodal, M.; Ruiz Lozano, A.; Pérez Díaz, C.R.; González Valdés, A.; Gonzalez Alvarez, L. Clinical relevance of Zika symptoms in the context of a Zika Dengue epidemic. J. Infect. Public Health 2020, 13, 173–176. [Google Scholar] [CrossRef]
- Koike, H.; Chiba, A.; Katsuno, M. Emerging infection, vaccination, and Guillain–Barré syndrome: A review. Neurol. Ther. 2021, 10, 523–537. [Google Scholar] [CrossRef]
- Charniga, K.; Cucunubá, Z.M.; Walteros, D.M.; Mercado, M.; Prieto, F.; Ospina, M.; Nouvellet, P.; Donnelly, C.A. Descriptive analysis of surveillance data for Zika virus disease and Zika virus-associated neurological complications in Colombia, 2015–2017. PLoS ONE 2021, 16, e0252236. [Google Scholar] [CrossRef]
- Krauer, F.; Riesen, M.; Reveiz, L.; Oladapo, O.T.; Martínez-Vega, R.; Porgo, T.V.; Haefliger, A.; Broutet, N.J.; Low, N.; WHO Zika Causality Working Group Zika. Virus Infection as a Cause of Congenital Brain Abnormalities and Guillain–Barré Syndrome: Systematic Review. PLoS ONE 2017, 14, e1002203. [Google Scholar] [CrossRef]
- Fernandez, M.P.; Parra Saad, E.; Ospina Martinez, M.; Corchuelo, S.; Mercado Reyes, M.; Herrera, M.J.; Parra Saavedra, M.; Rico, A.; Fernandez, A.M.; Lee, R.K.; et al. Ocular histopathologic features of congenital Zika syndrome. JAMA Ophthalmol. 2017, 135, 1163–1169. [Google Scholar] [CrossRef] [PubMed]
- Collier, A.Y.; Borducchi, E.N.; Chandrashekar, A.; Moseley, E.; Peter, L.; Teodoro, N.S.; Nkolola, J.; Abbink, P.; Barouch, D.H. Sustained maternal antibody and cellular immune responses in pregnant women infected with Zika virus and mother to infant transfer of Zika-specific antibodies. Am. J. Reprod. Immunol. 2020, 84, e13288. [Google Scholar] [CrossRef]
- Angel, B.; Joshi, V. Distribution and seasonality of vertically transmitted dengue viruses in Aedes mosquitoes in arid and semi-arid areas of Rajasthan, India. J. Vector Borne Dis. 2008, 45, 56. [Google Scholar] [PubMed]
- Wongkoon, S.; Jaroensutasinee, M.; Jaroensutasinee, K. Distribution, seasonal variation & dengue transmission prediction in Sisaket, Thailand. Indian. J. Med. Res. 2013, 138, 347. [Google Scholar] [PubMed]
- Ramachandran, V.G.; Roy, P.; Das, S.; Mogha, N.S.; Bansal, A.K. Empirical model for estimating dengue incidence using temperature, rainfall, and relative humidity: A 19-year retrospective analysis in East Delhi. Epidemiol. Health 2016, 38, e2016052. [Google Scholar] [CrossRef] [PubMed]
- Stirnemann, J.; Villar, J.; Salomon, L.J.; Ohuma, E.; Ruyan, P.; Altman, D.G.; Nosten, F.; Craik, R.; Munim, S.; Cheikh Ismail, L.; et al. International estimated fetal weight standards of the INTERGROWTH-21st Project. Ultrasound Obstet. Gynecol. 2017, 49, 478–486. [Google Scholar] [CrossRef] [PubMed]
- Akanda, A.S.; Johnson, K.; Ginsberg, H.S.; Couret, J. Prioritizing Water Security in the Management of Vector-Borne Diseases: Lessons From Oaxaca, Mexico. GeoHealth 2020, 4, e2019GH000201. [Google Scholar] [CrossRef] [PubMed]
- Würsch, D.; Rojas-Montes, O.; Maldonado-Rodríguez, A.; Sevilla-Reyes, E.; Cevallos, A.M.; Sánchez-Burgos, G.; Chávez-Negrete, A.; Lira, R. Dried Serum Samples for Antibody Detection in Arthropod-Borne Virus Infections Are an Effective Alternative to Serum Samples. Am. J. Trop. Med. Hyg. 2023, 109, 933–936. [Google Scholar] [CrossRef] [PubMed]
- Atama, N.C.; Chestakova, I.V.; de Bruin, E.; van den Berg, T.J.; Munger, E.; Reusken, C.; Oude-Munnink, B.B.; van der Jeugd, H.; van den Brand, J.M.A.; Koopmans, M.P.G.; et al. Evaluation of the use of alternative sample types for mosquito-borne flavivirus surveillance: Using Usutu virus as a model. One Health 2022, 15, 100456. [Google Scholar] [CrossRef] [PubMed]
- Cardona-Ospina, J.A.; Stittleburg, V.; Millan-Benavidez, N.; Restrepo-Chica, J.; Key, A.; Rojas-Gallardo, D.M.; Piantadosi, A.; Collins, M.H.; Waggoner, J.J. Sensitive and Stable Molecular Detection of Dengue, Chikungunya, and Zika Viruses from Dried Blood Spots. Am. J. Trop. Med. Hyg. 2022, 107, 296–299. [Google Scholar] [CrossRef]
- Gorchakov, R.; Berry, R.M.; Patel, S.M.; El Sahly, H.M.; Ronca, S.E.; Murray, K.O. Optimizing PCR Detection of Zika Virus from Various Body Fluids. Am. J. Trop. Med. Hyg. 2019, 100, 427–433. [Google Scholar] [CrossRef]
- Lei, C.; Yang, J.; Hu, J.; Sun, X. On the Calculation of TCID50 for Quantitation of Virus Infectivity. Virol. Sin. 2021, 36, 141–144. [Google Scholar] [CrossRef]
- Baz, M. Zika Virus Isolation, Purification, and Titration. Methods Mol. Biol. 2020, 2142, 9–22. [Google Scholar]
- Quest Graph™ ED50 Calculator. AAT Bioquest, Inc. Available online: https://www.aatbio.com/tools/ed50-calculator (accessed on 9 February 2021).
- Maldonado-Rodríguez, A.; Rojas-Montes, O.; Vazquez-Rosales, G.; Chávez-Negrete, A.; Rojas-Uribe, M.; Posadas-Mondragón, A.; Aguilar-Faisal, L.; Cevallos, A.M.; Xoconostle-Cazares, B.; Lira, R. Serum Dried Samples to Detect Dengue Antibodies: A Field Study. BioMed Res. Int. 2017, 2017, 7215259. [Google Scholar] [CrossRef]
- Centers for Diseases Control Prevention. Congenital Zika Syndrome & Other Birth Defects. Available online: https://www.cdc.gov/pregnancy/zika/testing-follow-up/zika-syndrome-birth-defects.html (accessed on 10 March 2023).
- INTERGROWTH-21st. 2018. Available online: http://intergrowth21.ndog.ox.ac.uk/es (accessed on 22 February 2018).
- Perret, C.; Chanthavanich, P.; Pengsaa, K.; Limkittikul, K.; Hutajaroen, P.; Bunn, J.E.; Brabin, B.J. Dengue infection during pregnancy and transplacental antibody transfer in Thai mothers. J. Infect. 2005, 51, 287–293. [Google Scholar] [CrossRef]
- Basurko, C.; Matheus, S.; Hildéral, H.; Everhard, S.; Restrepo, M.; Cuadro-Alvarez, E.; Lambert, V.; Boukhari, R.; Duvernois, J.P.; Favre, A.; et al. Estimating the risk of vertical transmission of dengue: A prospective study. Am. J. Trop. Med. Hyg. 2018, 98, 1826. [Google Scholar] [CrossRef] [PubMed]
- Grischott, F.; Puhan, M.; Hatz, C.; Schlagenhauf, P. Non-vector-borne transmission of Zika virus: A systematic review. Travel Med. Infect. Dis. 2016, 14, 313–330. [Google Scholar] [CrossRef] [PubMed]
- Compendio de Información Geográfica Municipal de los Estados Unidos Mexicanos, San Pedro Pochutla, Oaxaca Clave Geoestadística 20324. Instituto Nacional de Estadística y Geografía. Available online: https://www.inegi.org.mx (accessed on 9 February 2021).
- Consejo Nacional de Evaluación de la política de desarrollo Social (CONEVAL). Medición de la pobreza, Pobreza a nivel municipio 2019–2020. Available online: https://www.coneval.org.mx/Medicion/Paginas/Pobreza-municipio-2010-2020.aspx (accessed on 9 February 2021).
- Ali, S.; Gugliemini, O.; Harber, S.; Harrison, A.; Houle, L.; Ivory, J.; Kersten, S.; Khan, R.; Kim, J.; LeBoa, C.; et al. Environmental and social change drive the explosive emergence of Zika virus in the Americas. PLoS Negl. Trop. Dis. 2017, 11, e0005135. [Google Scholar] [CrossRef] [PubMed]
- Rees, E.E.; Petukhova, T.; Mascarenhas, M.; Pelcat, Y.; Ogden, N.H. Environmental and social determinants of population vulnerability to Zika virus emergence at the local scale. Parasites Vectors 2018, 11, 290. [Google Scholar] [CrossRef] [PubMed]
- Netto, E.M.; Moreira-Soto, A.; Pedroso, C.; Höser, C.; Funk, S.; Kucharski, A.J.; Rockstroh, A.; Kümmerer, B.M.; Sampaio, G.S.; Luz, E.; et al. High Zika virus seroprevalence in Salvador, northeastern Brazil limits the potential for further outbreaks. MBio 2017, 8, e01390-17. [Google Scholar] [CrossRef]
- Saba-Villarroel, P.M.; Nurtop, E.; Pastorino, B.; Roca, Y.; Drexler, J.F.; Gallian, P.; Jaenisch, T.; Leparc-Goffart, I.; Priet, S.; Ninove, L.; et al. Zika virus epidemiology in Bolivia: A seroprevalence study in volunteer blood donors. PLoS Negl. Trop. Dis. 2018, 12, e0006239. [Google Scholar] [CrossRef] [PubMed]
- Zambrana, J.V.; Bustos Carrillo, F.; Burger-Calderon, R.; Collado, D.; Sanchez, N.; Ojeda, S.; Carey Monterrey, J.; Plazaola, M.; Lopez, B.; Arguello, S.; et al. Seroprevalence, risk factor, and spatial analyses of Zika virus infection after the 2016 epidemic in Managua, Nicaragua. Proc. Natl. Acad. Sci. USA 2018, 115, 9294–9299. [Google Scholar] [CrossRef]
- Secretaría de Salud. Boletín de Prensa. Enfermedad por Virus Zika. México. Available online: http://www.ssm.gob.mx/portal/page/vig_epid/10/2015/Boletin%20de%20Prensa%20Zika%20171115.pdf (accessed on 17 November 2015).
- Grajales-Muñiz, C.; Borja-Aburto, V.H.; Cabrera-Gaytán, D.A.; Rojas-Mendoza, T.; Arriaga-Nieto, L.; Vallejos-Parás, A. Zika virus: Epidemiological surveillance of the Mexican Institute of Social Security. PLoS ONE 2019, 14, e0212114. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Ávila, J.E.; Palacio-Mejía, L.S.; López-Gatell, H.; Alpuche-Aranda, C.M.; Molina-Vélez, D.; González-González, L.; Hernández-Ávila, M. Zika virus infection estimates, Mexico. Bull. World Health Organ. 2018, 96, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Pasquier, C.; Joguet, G.; Mengelle, C.; Chapuy-Regaud, S.; Pavili, L.; Prisant, N.; Izopet, J.; Bujan, L.; Mansuy, J.M. Kinetics of anti-ZIKV antibodies after Zika infection using two commercial enzyme-linked immunoassays. Diagn. Microbiol. Infect. Dis. 2018, 90, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Roth, N.M.; Reynolds, M.R.; Lewis, E.L.; Woodworth, K.R.; Godfred-Cato, S.; Delaney, A.; Akosa, A.; Valencia-Prado, M.; Lash, M.; Elmore, A.; et al. Zika-Associated Birth Defects Reported in Pregnancies with Laboratory Evidence of Confirmed or Possible Zika Virus Infection—U.S. Zika Pregnancy and Infant Registry, December 1, 2015–March 31, 2018. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Rice, M.E.; Galang, R.R.; Roth, N.M.; Ellington, S.R.; Moore, C.A.; Valencia-Prado, M.; Ellis, E.M.; Tufa, A.J.; Taulung, L.A.; Alfred, J.M.; et al. Vital Signs: Zika-Associated Birth Defects and Neurodevelopmental Abnormalities Possibly Associated with Congenital Zika Virus Infection—U.S. Territories and Freely Associated States, 2018. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 858–867. [Google Scholar] [CrossRef]
- Smoots, A.N.; Olson, S.M.; Cragan, J.; Delaney, A.; Roth, N.M.; Godfred-Cato, S.; Jones, A.M.; Nahabedian, J.F., 3rd; Fornoff, J.; Sandidge, T.; et al. Population-Based Surveillance for Birth Defects Potentially Related to Zika Virus Infection—22 States and Territories, January 2016–June 2017. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 67–71. [Google Scholar] [CrossRef]
- Felix, A.C.; Souza, N.C.S.; Figueiredo, W.M.; Costa, A.A.; Inenami, M.; da Silva, R.M.G.; Levi, J.E.; Pannuti, C.S.; Romano, C.M. Cross reactivity of commercial anti-dengue immunoassays in patients with acute Zika virus infection. J. Med. Virol. 2017, 89, 1477–1479. [Google Scholar] [CrossRef]
- Suy, A.; Sulleiro, E.; Rodó, C.; Vázquez, É.; Bocanegra, C.; Molina, I.; Esperalba, J.; Sánchez-Seco, M.P.; Boix, H.; Pumarola, T.; et al. Prolonged Zika Virus Viremia during Pregnancy. N. Engl. J. Med. 2016, 375, 2611–2613. [Google Scholar] [CrossRef]
- Villalobos-Sánchez, E.; Burciaga-Flores, M.; Zapata-Cuellar, L.; Camacho-Villegas, T.A.; Elizondo-Quiroga, D.E. Possible Routes for Zika Virus Vertical Transmission in Human Placenta: A Comprehensive Review. Viral Immunol. 2022, 35, 392–403. [Google Scholar] [CrossRef]
- Owie, S.R. Blood sample volumes in child health research: Review of safe limits. Bull. World Health Organ. 2011, 89, 46–53. [Google Scholar]
- Langerak, T.; Mumtaz, N.; Tolk, V.I.; van Gorp, E.C.; Martina, B.E.; Rockx, B.; Koopmans, M.P. The possible role of cross-reactive dengue virus antibodies in Zika virus pathogenesis. PLoS Pathog. 2019, 15, e1007640. [Google Scholar] [CrossRef]
- Hattakam, S.; Elong Ngono, A.; McCauley, M.; Shresta, S.; Yamabhai, M. Repeated exposure to dengue virus elicits robust cross neutralizing antibodies against Zika virus in residents of Northeastern Thailand. Sci. Rep. 2021, 11, 9634. [Google Scholar] [CrossRef]
- Montoya, M.; Collins, M.; Dejnirattisai, W.; Katzelnick, L.C.; Puerta-Guardo, H.; Jadi, R.; Schildhauer, S.; Supasa, P.; Vasana-wathana, S.; Malasit, P. Longitudinal analysis of antibody cross-neutralization following Zika virus and dengue virus infection in Asia and the Americas. J. Infect. Dis. 2018, 218, 536–545. [Google Scholar] [CrossRef]
- Besnard, M.; Lastère, S.; Teissier, A.; Cao-Lormeau, V.M.; Musso, D. Evidence of perinatal transmission of Zika virus, French Polynesia December 2013 and January 2014. Euro Surveill. 2014, 9, 20751. [Google Scholar]
- Singh, T.; Lopez, C.A.; Giuberti, C.; Dennis, M.L.; Itell, H.L.; Heimsath, H.J.; Webster, H.S.; Roark, H.K.; Merçon de Vargas, P.R.; Hall, A.; et al. Efficient transplacental IgG transfer in women infected with Zika virus during pregnancy. PLoS Negl. Trop. Dis. 2019, 13, e0007648. [Google Scholar] [CrossRef] [PubMed]
- Blohm, G.M.; Lednicky, J.A.; Márquez, M.; White, S.K.; Loeb, J.C.; Pacheco, C.A.; Nolan, D.J.; Paisie, T.; Salemi, M.; Rodríguez-Morales, A.J.; et al. Evidence for Mother-to-Child Transmission of Zika Virus Through Breast Milk. Clin. Infect. Dis. 2018, 66, 1120–1121. [Google Scholar] [CrossRef] [PubMed]
- Furuya, A.K.M.; Hunt, D.; George, K.S.; Dupuis, A.P., 2nd; Kramer, L.D.; Shi, P.Y.; Wong, S. Use of the immunoglobulin G avidity assay to differentiate between recent Zika and past dengue virus infections. Clin. Sci. 2019, 133, 859–867. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | N | Median | Min | Max |
|---|---|---|---|---|
| Mother | ||||
| Age (years) | 126 | 23 | 14 | 40 |
| Infant | ||||
| Female | 65 (52%) | |||
| Male | 61 (48%) | |||
| Gestational age | ||||
| Preterm (<37 WG*) | 4 (3%) | |||
| To term (37–41 WG*) | 120 (95%) | |||
| Post-term (≥41 WG*) | 2 (2%) | |||
| IgG+/IgM+ | IgG+/IgM− | IgG−/IgM+ | IgG−/IgM− | |
|---|---|---|---|---|
| PCR+ | 7/25 (28%) | 1/6 (0.8%) | 5/11(45.5%) | 0 |
| PCR− | 18/25 (18.3%) | 5/6 (4.8%) | 6/11 (54.5%) | 84/126 (66.6%) |
| MOTHER | INFANT | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| IgG | IgM | Blood—PCR | Saliva—PCR | IgG DBS | |||||||
| + | − | + | − | + | − | + | − | + | − | ||
| Microcephaly | YES | 9 | 14 | 14 | 9 | 7 | 16 | 5 | 18 | 2 | 21 |
| NO | 27 | 76 | 25 | 78 | 6 | 97 | 3 | 100 | 4 | 99 | |
| Pair | HC * | Mother | RT PCR | Serology IgG | RT-PCR Infant | ED50 | |||
|---|---|---|---|---|---|---|---|---|---|
| IgG | IgM | Blood | BM | Infant | Saliva | DBS | |||
| 61 | 76 | + | − | + | − | + | − | − | 15 × 103 |
| 62 | 85 | + | + | + | + | + | + | − | 19 × 103 |
| 65 | 80 | + | + | + | − | + | + | − | 17 × 103 |
| 73 | 6 | + | − | + | − | + | + | − | 2 × 103 |
| 82 | 33 | + | + | + | − | + | + | + | 0.06 × 103 |
| 93 | 6 | + | + | + | − | + | + | − | 1 × 103 |
| 96 | 93 | + | + | + | − | + | − | + | 7.7 × 103 |
| 130 | 75 | + | + | + | − | + | − | − | 4.5 × 103 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Porras-García, A.; Villanueva-García, D.; Arnaud-Rios, R.; García-Lemus, N.; Castillo-Romero, A.; Mejía-Flores, M.; Contreras, L.E.; Hernández-Castillo, L.; Jiménez-Hernández, E.; Mejía-Aranguré, J.M.; et al. Intrauterine Transmission of Zika and Vertical Transfer of Neutralizing Antibodies Detected Immediately at Birth in Oaxaca, Mexico: An Analysis in the Context of Microcephaly. Microorganisms 2024, 12, 423. https://doi.org/10.3390/microorganisms12030423
Porras-García A, Villanueva-García D, Arnaud-Rios R, García-Lemus N, Castillo-Romero A, Mejía-Flores M, Contreras LE, Hernández-Castillo L, Jiménez-Hernández E, Mejía-Aranguré JM, et al. Intrauterine Transmission of Zika and Vertical Transfer of Neutralizing Antibodies Detected Immediately at Birth in Oaxaca, Mexico: An Analysis in the Context of Microcephaly. Microorganisms. 2024; 12(3):423. https://doi.org/10.3390/microorganisms12030423
Chicago/Turabian StylePorras-García, Alfredo, Dina Villanueva-García, Rafael Arnaud-Rios, Nadia García-Lemus, Angélica Castillo-Romero, Mariana Mejía-Flores, Luis Erik Contreras, Liliana Hernández-Castillo, Elva Jiménez-Hernández, Juan Manuel Mejía-Aranguré, and et al. 2024. "Intrauterine Transmission of Zika and Vertical Transfer of Neutralizing Antibodies Detected Immediately at Birth in Oaxaca, Mexico: An Analysis in the Context of Microcephaly" Microorganisms 12, no. 3: 423. https://doi.org/10.3390/microorganisms12030423