
Human Exposure to Naturally Occurring Bacillus anthracis in the Kars Region of Eastern Türkiye
 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Study Design
- (1)
- Individuals living in a village in Kars province that had a known history of animal or human anthrax infection and who were regularly involved in animal husbandry (rural dweller group);
- (2)
- Butchers who worked in an anthrax-endemic area;
- (3)
- Shepherds who worked in close contact with animals;
- (4)
- Leather workers who worked with potentially contaminated material;
- (5)
- Veterinarians (including animal health technicians) working in an anthrax-endemic area;
- (6)
- Individuals living in Kars city or one of five towns in the region: Arpaçay, Digor, Selim, Susuz, or Sarıkamış (urban dweller group);
- (7)
- Laboratory staff working in the Pathology and Microbiology departments at Kafkas University in Kars.
2.2. Demographic and Clinical Information
2.3. Serological Analyses
2.3.1. Optimised Enzyme Linked Immunosorbent Assay (ELISA) Method
- (1)
- The first 10 columns of each 96-well ELISA plate (Biosigma S.r.l, Coma, Italy) were coated with 100 µL recombinant antigen at 2 µg/mL in PBS. Both recombinant protective antigen (Lot 17115A5B) and lethal factor (Lot 1722B11B) were purchased from Quadratech Diagnostics Ltd. (Eastbourne BN21 3AW, UK);
- (2)
- A standard curve was constructed by adding human IgG (Sigma Code: I4506; Sigma Aldrich, Dorset SP8 4XT, UK) to the last two columns (11 and 12) to achieve a range of concentrations (0.5, 0.25, 0.125, and 0.0625 µg/mL), with each concentration represented in triplicate;
- (3)
- Following coating, plates were washed three times with 300 µL of PBS + 0.1% Tween-20 (PBST) per well (Wellwash Microplate Washer, Cat. No. N15777, ThermoFisher, Vantaa FI-01621, Finland) and then incubated at 37 °C for 1 h to block the wells;
- (4)
- Test samples (columns 1–8), positive control serum (column 9), and negative control serum (column 10) were defrosted and serially diluted 1 in 2 down the plate with PBST, with the first well containing a 1:10 dilution;
- (5)
- Following incubation, plates were washed three times with PBST;
- (6)
- A total of 100 µL anti-human IgG mouse monoclonal antibody (Jackson ImmunoResearch Lab. Inc., Cambridgeshire CB7 4EX, UK. Code: 209-035-088, Lot: 100924), diluted 1:1000 in PBST, was added to each well. Plates were then incubated for 1 h at 37 °C;
- (7)
- Following incubation, plates were washed three times with PBST using an automated plate washer;
- (8)
- Substrate solution was prepared as follows: 0.7 g sodium phosphate dibasic (Sigma Code: S5136-100G) and 0.5 g citric acid (Sigma Code: 27102) were dissolved in 100 mL of deionised water. One ABTS substrate tablet (Sigma Code: 1001235282, A9941, Lot: 071M8224V) was then added to this solution. Finally, 2.5 µL H2O2 (Sigma Code: H1009-100ML) was added to 10 mL of the substrate solution prior to use;
- (9)
- A total of 100 µL ABTS reagent with H2O2 was added to each well and the plates incubated at 37 °C for 30 min. The reaction was stopped by adding 100 µL 2% SDS (Sigma Code: L4390-100g) in deionised water, and the plates were read at 405 nm (SpectraMax Plus384 Absorbance Microplate Reader, Molecular Devices).
2.3.2. Determination of IgG Concentration
2.4. Statistical Analyses
2.4.1. Missing Data Points
2.4.2. Data Transformations
2.4.3. Stepwise Linear Regressions
2.4.4. Linear Discriminant Analysis
2.4.5. Stepwise Multiple Regressions Using Discriminant Factor
3. Results
3.1. Factors Associated with Anti-PA and Anti-LF IgG Concentration
- (1)
- the categories of living in a village with being a rural dweller by occupation;
- (2)
- time since infection with confirmed previous infection.
3.2. Derivation of Optimised Composite Discriminant Factor
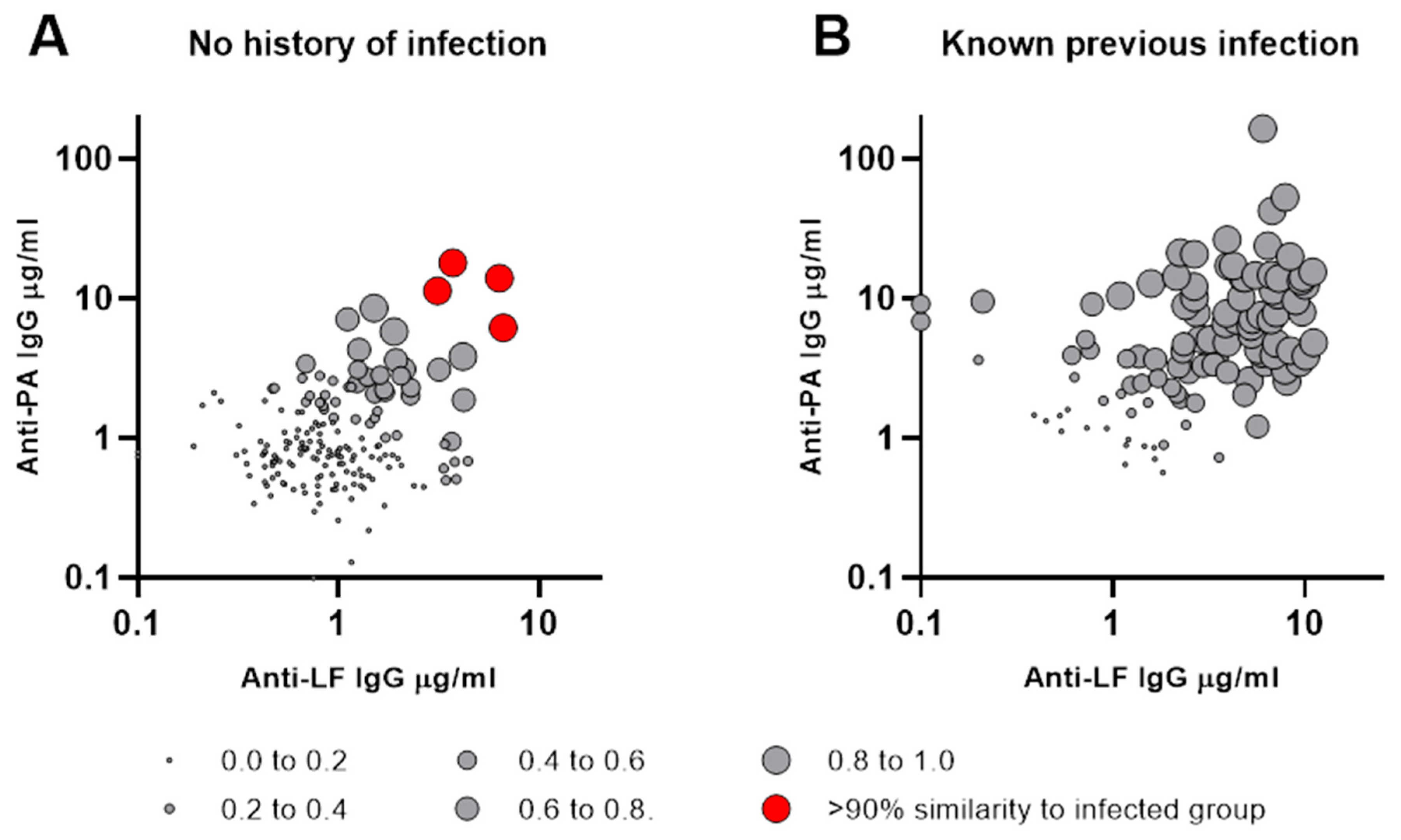
3.3. Antibody Concentration Profiles Typical of Previous Infection
3.4. Identification of Individuals with Probable Unrecognised Previous Infection
4. Discussion
5. Study Limitations
- (1)
- There were missing data points for some parameters for a few individuals in this study, but the statistical approaches used to account for these gaps in a dataset are well recognised as being able to satisfactorily eliminate any uncertainty caused;
- (2)
- Infected individuals were treated with antibiotics and as a consequence the resulting immune response may not fully reflect what happens when an infection resolves without any external intervention;
- (3)
- While an immune response indicates past exposure to a pathogen, it cannot be assumed that the individual would be protected from future infection. Further studies are required to determine whether this is indeed the case in the context of low-level exposure to anthrax spores. These studies should include, inter alia, measurement of lethal toxin neutralisation using the TNA assay [50,51], which is recognised by regulatory authorities as a surrogate for anthrax vaccine efficacy.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Beyer, W.; Bellan, S.; Eberle, G.; Ganz, H.H.; Getz, W.M.; Haumacher, R.; Hilss, K.A.; Kilian, W.; Lazak, J.; Turner, W.C.; et al. Distribution and molecular evolution of Bacillus anthracis genotypes in Namibia. PLoS Negl. Trop. Dis. 2012, 6, e1534. [Google Scholar] [CrossRef]
- Cote, C.K.; Welkos, S.L. Anthrax toxins in context of Bacillus anthracis spores and spore germination. Toxins 2015, 7, 3167–3178. [Google Scholar] [CrossRef] [PubMed]
- Ascenzi, P.; Visca, P.; Ippolito, G.; Spallarossa, A.; Bolognesi, M.; Montecucco, C. Anthrax toxin: A tripartite lethal combination. FEBS Lett. 2002, 531, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Leppla, S.H.; Robbins, J.B.; Schneerson, R.; Shiloach, J. Development of an improved vaccine for anthrax. J. Clin. Investig. 2002, 110, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Moayeri, M.; Leppla, S.H. Anthrax Toxins. In Bacillus anthracis and Anthrax; Bergman, N.H., Ed.; John Wiley & Sons Inc.: Hoboken, NJ, USA, 2011; Chapter 8; pp. 121–156. ISBN 978-0-470-41011-0. [Google Scholar]
- Strange, R.E.; Belton, F.C. Studies on a protective antigen produced in vitro from Bacillus anthracis: Purification and chemistry of the antigen. Br. J. Exp. Pathol. 1954, 35, 153–165. [Google Scholar] [PubMed]
- Darlow, H.M.; Belton, F.C.; Henderson, D.W. The use of anthrax antigen to immunise man and monkey. Lancet 1956, 268, 476–479. [Google Scholar] [CrossRef] [PubMed]
- Brachman, P.S.; Gold, H.; Plotkin, S.A.; Fekety, F.R.; Werrin, M.; Ingraham, N.R. Field evaluation of a human anthrax vaccine. Am. J. Public Health 1962, 52, 632–645. [Google Scholar] [CrossRef] [PubMed]
- Welkos, S.L.; Friedlander, A.M. Comparative safety and efficacy against Bacillus anthracis of protective antigen and live vaccines in mice. Microb. Pathog. 1988, 5, 127–139. [Google Scholar] [CrossRef]
- Pitt, M.L.M.; Little, S.; Ivins, B.E.; Fellows, P.; Boles, J.; Barth, J.; Hewetson, J.; Friedlander, A.M. In vitro correlate of immunity in an animal model of inhalational anthrax. J. Appl. Microbiol. 1999, 87, 304. [Google Scholar] [CrossRef]
- Pitt, M.; Little, S.; Ivins, B.; Fellows, P.; Barth, J.; Hewetson, J.; Gibbs, P.; Dertzbaugh, M.; Friedlander, A. In vitro correlate of immunity in a rabbit model of inhalational anthrax. Vaccine 2001, 19, 4768–4773. [Google Scholar] [CrossRef]
- Welkos, S.; Little, S.; Friedlander, A.; Fritz, D.; Fellows, P. The role of antibodies to Bacillus anthracis and anthrax toxin components in inhibiting the early stages of infection by anthrax spores. Microbiology 2001, 147, 1677–1685. [Google Scholar] [CrossRef] [PubMed]
- Pittman, P.R.; Kim-Ahn, G.; Pifat, D.Y.; Coonan, K.; Gibbs, P.; Little, S.; Pace-Templeton, J.G.; Myers, R.; Parker, G.W.; Friedlander, A.M. Anthrax vaccine: Immunogenicity and safety of a dose-reduction, route-change comparison study in humans. Vaccine 2002, 20, 1412–1420. [Google Scholar] [CrossRef] [PubMed]
- Saile, E.; Quinn, C.P. Anthrax Vaccines. In Bacillus Anthracis and Anthrax; Bergman, N.H., Ed.; John Wiley & Sons Inc.: Hoboken, NJ, USA, 2011; Chapter 14; pp. 269–293. ISBN 978-0-470-41011-0. [Google Scholar]
- Baillie, L. Can one size fit all? Towards a universal anthrax vaccine. Future Microbiol. 2013, 8, 295–297. [Google Scholar] [CrossRef] [PubMed]
- Lindeque, P.M.; Turnbull, P.C. Ecology and epidemiology of anthrax in the Etosha National Park, Namibia. Onderstepoort. J. Vet. Res. 1994, 61, 71–83. [Google Scholar] [PubMed]
- Turnbull, P.; Bowen, J.; Mann, J. Stubborn contamination with anthrax spores. Environ. Health 1996, 106, 171–173. [Google Scholar]
- Fasanella, A.; Scasciamacchia, S.; Garofolo, G.; Giangaspero, A.; Tarsitano, E.; Adone, R. Evaluation of the house fly Musca domestica as a mechanical vector for an anthrax. PLoS ONE 2010, 5, e12219. [Google Scholar] [CrossRef] [PubMed]
- Harrison, L.H.; Ezzell, J.W.; Abshire, T.G.; Kidd, S.; Kaufmann, A.F.; Center, V.L.I. Evaluation of serologic tests for diagnosis of anthrax after an outbreak of cutaneous anthrax in Paraguay. J. Infect. Dis. 1989, 160, 706–710. [Google Scholar] [CrossRef] [PubMed]
- Özkurt, Z.; Parlak, M.; Tastan, R.; Dinler, U.; Saglam, Y.S.; Ozyurek, S.F. Anthrax in Eastern Turkey, 1992–2004. Emerg. Infect. Dis. 2005, 11, 1939–1941. [Google Scholar] [CrossRef]
- Baykam, N.; Ergonul, O.; Ulu, A.; Eren, S.; Celikbas, A.; Eroglu, M.; Dokuzoguz, B. Characteristics of cutaneous anthrax in Turkey. J. Infect. Dev. Ctries. 2009, 3, 599–603. [Google Scholar] [CrossRef]
- Doganay, M.; Metan, G. Human anthrax in Turkey from 1990 to 2007. Vector-Borne Zoonotic Dis. 2009, 9, 131–139. [Google Scholar] [CrossRef]
- Demiraslan, H.; Borlu, A.; Sahin, S.; Buyuk, F.; Karadag, Y.; Doganay, M.; Sahin, M. The epidemiological investigation and control of an anthrax outbreak in a village in Central Anatolia, Turkey. Pathog. Glob. Health 2017, 111, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Kutmanova, A.; Doganay, M.; Zholdoshev, S. Human anthrax in Kyrgyz Republic: Epidemiology and clinical features. J. Infect. Public Health 2020, 13, 1161–1165. [Google Scholar] [CrossRef] [PubMed]
- Doganay, M.; Dinc, G.; Kutmanova, A.; Baillie, L. Human anthrax: Update of the diagnosis and treatment. Diagnostics 2023, 13, 1056. [Google Scholar] [CrossRef] [PubMed]
- Doganay, M.; Demiraslan, H. Human anthrax as a re-emerging disease. Recent Pat. Anti-Infect. Drug Discov. 2015, 10, 10–29. [Google Scholar] [CrossRef] [PubMed]
- Heyworth, B.; Ropp, M.E.; Voos, U.G.; Meinel, H.I.; Darlow, H.M. Anthrax in the Gambia: An epidemiological study. Br. Med. J. 1975, 4, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Ozer, V.; Gunaydin, M.; Pasli, S.; Aksoy, F.; Gunduz, A. Gastrointestinal and cutaneous anthrax: Case series. Turk. J. Emerg. Med. 2018, 19, 76–78. [Google Scholar] [CrossRef] [PubMed]
- Nakanwagi, M.; Ario, A.R.; Kwagonza, L.; Aceng, F.L.; Mwesigye, J.; Bulage, L.; Buule, J.; Sendagala, J.N.; Downing, R.; Zhu, B.-P. Outbreak of gastrointestinal anthrax following eating beef of suspicious origin: Isingiro District, Uganda, 2017. PLoS Negl. Trop. Dis. 2020, 14, e0008026. [Google Scholar] [CrossRef] [PubMed]
- Kozytska, T.; Bassiouny, M.; Chechet, O.; Ordynska, D.; Galante, D.; Neubauer, H.; Wareth, G. Retrospective analysis of official data on anthrax in Europe with a special reference to Ukraine. Microorganisms 2023, 11, 1294. [Google Scholar] [CrossRef]
- 14/1/2012-28173; Animal Disease Compensation Regulations, Türkiye. Regulation on Compensated Animal Diseases and Compensation Rates. Ministry of Food, Agriculture and Livestock: Ankara, Türkiye, 2012.
- Norman, P.S.; Ray, J.G.; Brachman, P.S.; Plotkin, S.A.; Pagano, J.S. Serologic testing for anthrax antibodies in workers in a goat hair processing mill. Am. J. Epidemiol. 1960, 72, 32–37. [Google Scholar] [CrossRef]
- Plotkin, S.A.; Brachman, P.S.; Utell, M.; Bumford, F.H.; Atchison, M.M. An epidemic of inhalation anthrax, the first in the twentieth century: I. Clinical features. Am. J. Med. 1960, 29, 992–1001. [Google Scholar] [CrossRef]
- Wattiau, P.; Klee, S.R.; Fretin, D.; Van Hessche, M.; Ménart, M.; Franz, T.; Chasseur, C.; Butaye, P.; Imberechts, H. Occurrence and genetic diversity of Bacillus anthracis strains isolated in an active wool-cleaning factory. Appl. Environ. Microbiol. 2008, 74, 4005–4011. [Google Scholar] [CrossRef] [PubMed]
- Wattiau, P.; Govaerts, M.; Frangoulidis, D.; Fretin, D.; Kissling, E.; Van Hessche, M.; China, B.; Poncin, M.; Pirenne, Y.; Hanquet, G. Immunologic response of unvaccinated workers exposed to anthrax, Belgium. Emerg. Infect. Dis. 2009, 15, 1637–1640. [Google Scholar] [CrossRef] [PubMed]
- Kissling, E.; Wattiau, P.; China, B.; Poncin, M.; Fretin, D.; Pirenne, Y.; Hanquet, G. B. anthracis in a wool-processing factory: Seroprevalence and occupational risk. Epidemiol. Infect. 2012, 140, 879–886. [Google Scholar] [CrossRef] [PubMed]
- Wikipedia Kars Description. 2023. Available online: https://en.wikipedia.org/wiki/Kars (accessed on 13 January 2023).
- Kadanalı, A.; Topluoğlu, S.; Aktaş, D.; Şahin, M.; Akbulut, A.; Kılıç, S.; Çetinkaya, B.; Parlak, E.; Dinç, G.; Gülyaz, V.; et al. Current situation report of anthrax in Turkey. Turk Hij. Den. Biyol. Derg. [Turk. Bull. Hyg. Exp. Biol.] 2020, 77 (Suppl 2), 1–20. [Google Scholar] [CrossRef]
- Ingram, R.J.; Metan, G.; Maillere, B.; Doganay, M.; Ozkul, Y.; Kim, L.U.; Baillie, L.; Dyson, H.; Williamson, E.D.; Chu, K.K.; et al. Natural exposure to cutaneous anthrax gives long-lasting T cell immunity encompassing infection-specific epitopes. J. Immunol. 2010, 184, 3814–3821. [Google Scholar] [CrossRef] [PubMed]
- Laws, T.R.; Kuchuloria, T.; Chitadze, N.; Little, S.F.; Webster, W.M.; Debes, A.K.; Saginadze, S.; Tsertsvadze, N.; Chubinidze, M.; Rivard, R.G.; et al. A comparison of the adaptive immune response between recovered anthrax patients and individuals receiving three different anthrax vaccines. PLoS ONE 2016, 11, e0148713. [Google Scholar] [CrossRef] [PubMed]
- Dumas, E.K.; Demiraslan, H.; Ingram, R.J.; Sparks, R.M.; Muns, E.; Zamora, A.; Larabee, J.; Garman, L.; Ballard, J.D.; Boons, G.-J.; et al. Toxin-neutralizing antibodies elicited by naturally acquired cutaneous anthrax are elevated following severe disease and appear to target conformational epitopes. PLoS ONE 2020, 15, e0230782. [Google Scholar] [CrossRef]
- Pittman, P.R.; Cavicchia, M.; Kingsbury, J.; Johnson, N.; Barrera-Oro, J.; Schmader, T.; Korman, L.; Quinn, X.; Ranadive, M. Anthrax vaccine adsorbed: Further evidence supporting continuing the vaccination series rather than restarting the series when doses are delayed. Vaccine 2014, 32, 5131–5139. [Google Scholar] [CrossRef]
- Dumas, E.K.; Garman, L.; Cuthbertson, H.; Charlton, S.; Hallis, B.; Engler, R.J.; Choudhari, S.; Picking, W.D.; James, J.A.; Farris, A.D. Lethal Factor antibodies contribute to Lethal Toxin neutralization in recipients of Anthrax Vaccine Precipitated. Vaccine 2017, 35, 3416–3422. [Google Scholar] [CrossRef]
- Dyson, E.H.; Simpson, A.J.; Gwyther, R.J.; Cuthbertson, H.; Patient, D.H.; Matheson, M.; Gregg, A.; Hepburn, M.J.; Hallis, B.; Williamson, E.D. Serological responses to Anthrax Vaccine Precipitated (AVP) increase with time interval between booster doses. Vaccine 2022, 40, 6163–6178. [Google Scholar] [CrossRef]
- Doganay, M. Anthrax. In Infectious Diseases, 4th ed.; Cohen, J., Powderly, W.G., Opal, S.M., Eds.; Elsevier: Beijing, China, 2017. [Google Scholar]
- Turnbull, P.C.B. WHO Guidance: Anthrax in Humans and Animals, 4th ed.; WHO: Geneva, Switzerland, 2008; Available online: https://www.who.int/publications/i/item/9789241547536 (accessed on 28 July 2023).
- Perelle, S.; Scalzo, S.; Kochi, S.; Mock, M.; Popoff, M.R. Immunological and functional comparison between Clostridium perfringens iota toxin, C. spiroforme toxin, and anthrax toxins. FEMS Microbiol. Lett. 1997, 146, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Sardar, N.; Aziz, M.W.; Mukhtar, N.; Yaqub, T.; Anjum, A.A.; Javed, M.; Ashraf, M.A.; Tanvir, R.; Wolfe, A.J.; Schabacker, D.S.; et al. One Health assessment of Bacillus anthracis incidence and detection in anthrax-endemic areas of Pakistan. Microorganisms 2023, 11, 2462. [Google Scholar] [CrossRef] [PubMed]
- National Research Council. Reopening Public Facilities after a Biological Attack: A Decision Making Framework; The National Academies Press: Washington, DC, USA, 2005. [Google Scholar] [CrossRef]
- Li, H.; Soroka, S.D.; Taylor, T.H.; Stamey, K.L.; Stinson, K.W.; Freeman, A.E.; Abramson, D.R.; Desai, R.; Cronin, L.X.; Oxford, J.W.; et al. Standardized, mathematical model-based and validated in vitro analysis of anthrax lethal toxin neutralization. J. Immunol. Methods 2008, 333, 89–106. [Google Scholar] [CrossRef] [PubMed]
- Ngundi, M.M.; Meade, B.D.; Lin, T.-L.; Tang, W.-J.; Burns, D.L. Comparison of three anthrax toxin neutralization assays. Clin. Vaccine Immunol. 2010, 17, 895–903. [Google Scholar] [CrossRef]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/). Content includes material subject to © Crown copyright (2023), Dstl. This material is licensed under the terms of the Open Government Licence except where otherwise stat-ed. To view this licence, visit http://www.nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: [email protected]
Share and Cite
Buyuk, F.; Dyson, H.; Laws, T.R.; Celebi, O.; Doganay, M.; Sahin, M.; Baillie, L. Human Exposure to Naturally Occurring Bacillus anthracis in the Kars Region of Eastern Türkiye. Microorganisms 2024, 12, 167. https://doi.org/10.3390/microorganisms12010167
Buyuk F, Dyson H, Laws TR, Celebi O, Doganay M, Sahin M, Baillie L. Human Exposure to Naturally Occurring Bacillus anthracis in the Kars Region of Eastern Türkiye. Microorganisms. 2024; 12(1):167. https://doi.org/10.3390/microorganisms12010167
Chicago/Turabian StyleBuyuk, Fatih, Hugh Dyson, Thomas R. Laws, Ozgur Celebi, Mehmet Doganay, Mitat Sahin, and Les Baillie. 2024. "Human Exposure to Naturally Occurring Bacillus anthracis in the Kars Region of Eastern Türkiye" Microorganisms 12, no. 1: 167. https://doi.org/10.3390/microorganisms12010167