
Antimicrobial Susceptibility Patterns and Genetic Diversity of Campylobacter spp. Isolates from Patients with Diarrhea in South Korea
Abstract
:1. Introduction
2. Materials and Methods
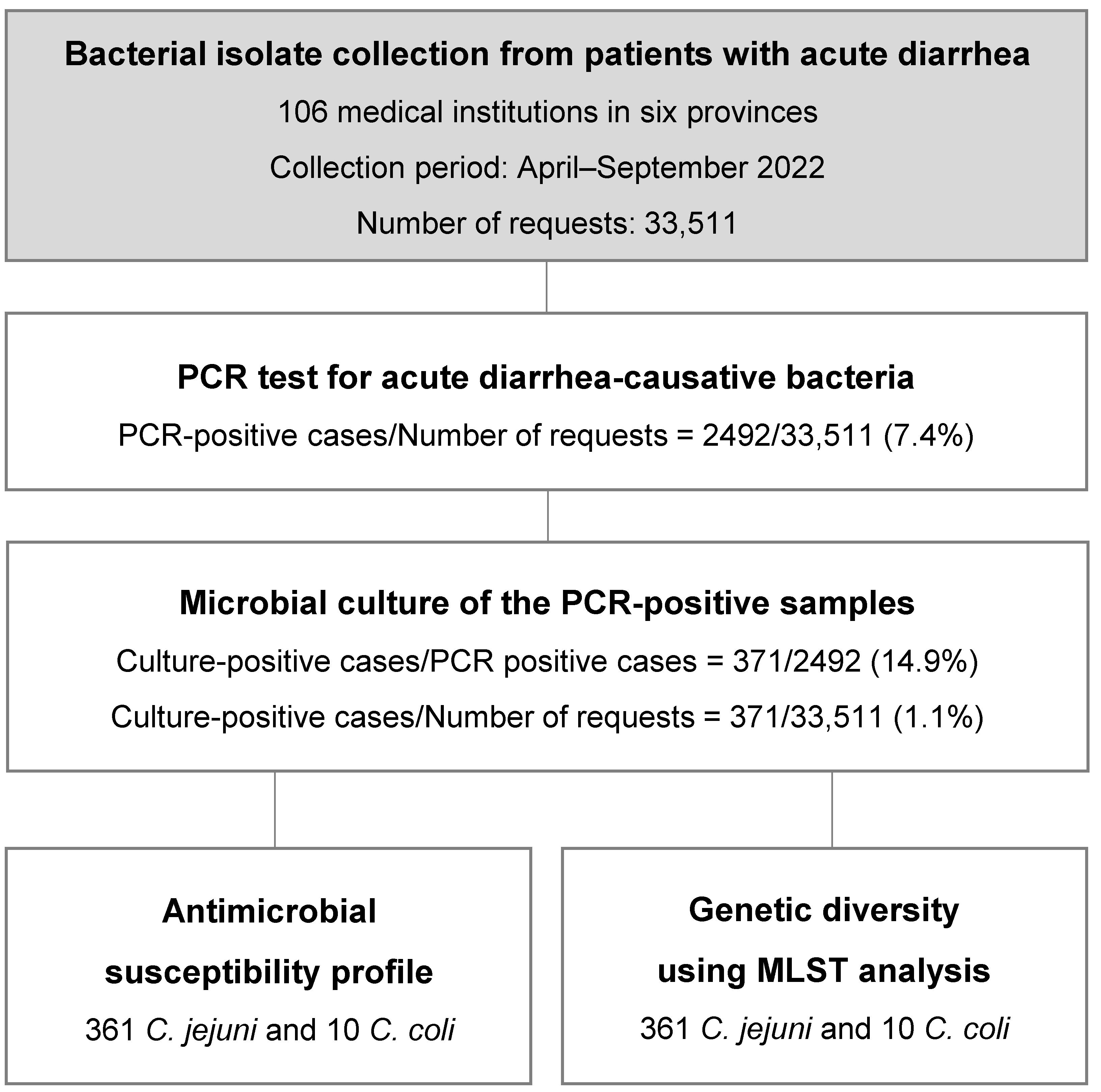
2.1. Bacterial Isolate Collection
2.2. Identification and Growth Conditions
2.3. Antimicrobial Resistance Testing
2.4. Clonal Population
2.5. Statistical Analysis
3. Results
3.1. Campylobacter spp. Isolation and Identification from Patients with Diarrhea
3.2. Campylobacter spp. Antimicrobial Resistance
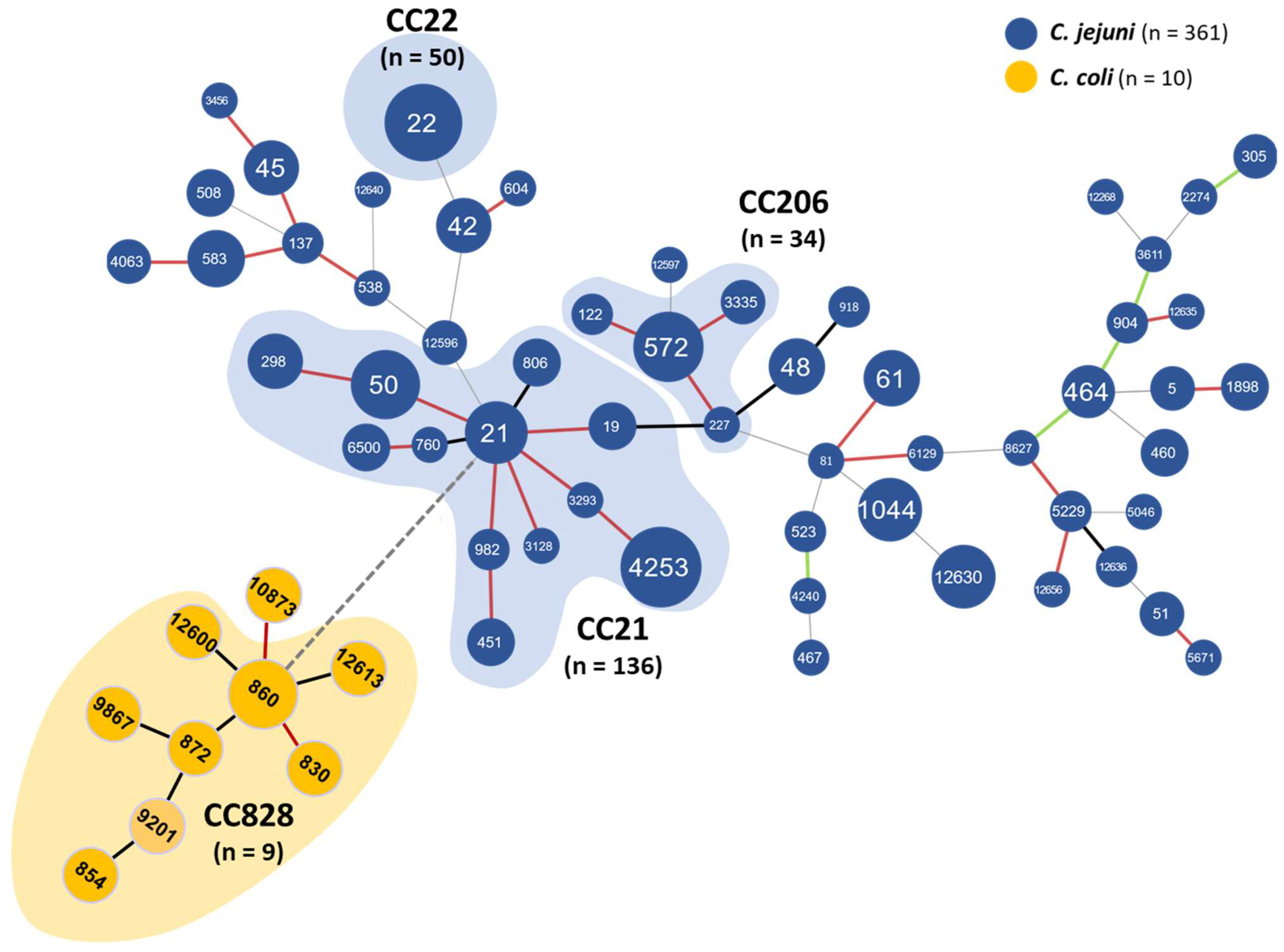
3.3. Campylobacter spp. Genetic Diversity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Burnham, P.M.; Hendrixson, D.R. Campylobacter jejuni: Collective components promoting a successful enteric lifestyle. Nat. Rev. Microbiol. 2018, 16, 551–565. [Google Scholar] [CrossRef] [PubMed]
- Elhadidy, M.; Ali, M.M.; El-Shibiny, A.; Miller, W.G.; Elkhatib, W.F.; Botteldoorn, N.; Dierick, K. Antimicrobial resistance patterns and molecular resistance markers of Campylobacter jejuni isolates from human diarrheal cases. PLoS ONE 2020, 15, e0227833. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Campylobacteriosis—Annual Epidemiological Report for 2021; ECDC: Stockholm, Sweden, 2022. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/campylobacteriosis-annual-epidemiological-report-2021.pdf (accessed on 31 October 2023).
- Wieczorek, K.; Osek, J. Antimicrobial resistance mechanisms among Campylobacter. BioMed Res. Int. 2013, 2013, 340605. [Google Scholar] [CrossRef] [PubMed]
- Yao, B.; Xiao, L.; Jiang, Z.; Sheng, C.; Li, G.; Shao, Y.; Wei, W.; Jin, X.; Freng, L. Quantification of Cross-Contamination of Campylobacter jejuni during food preparation in a model kitchen in China. J. Food Protect. 2021, 84, 850–856. [Google Scholar] [CrossRef]
- Wasfy, M.; Oyofo, B.; Elgindy, A.; Churilla, A. Comparison of preservation media for storage of stool samples. J. Clin. Microbiol. 1995, 33, 2176–2178. [Google Scholar] [CrossRef]
- Kang, C.R.; Bang, J.H.; Il Cho, S.I. Campylobacter jejuni foodborne infection associated with cross-contamination: Outbreak in Seoul in 2017. Infect. Chemother. 2019, 51, 21–27. [Google Scholar] [CrossRef]
- Ryoo, E. Causes of acute gastroenteritis in Korean children between 2004 and 2019. Clin. Exp. Pediatr. 2021, 64, 260–268. [Google Scholar] [CrossRef]
- Allos, B.M. Campylobacter jejuni infections: Update on emerging issues and trends. Clin. Infect. Dis. 2001, 32, 1201–1206. [Google Scholar] [CrossRef]
- Tresse, O.; Alvarez-Ordóñez, A.; Connerton, I.F. Editorial: About the foodborne pathogen Campylobacter. Front. Microbiol. 2017, 8, 1908. [Google Scholar] [CrossRef]
- Zhang, P.; Zhang, X.; Liu, Y.; Jiang, J.; Shen, Z.; Chen, Q.; Ma, X. Multilocus sequence types and antimicrobial resistance of Campylobacter jejuni and C. coli isolates of human patients from Beijing, China, 2017–2018. Front. Microbiol. 2020, 11, 554784. [Google Scholar] [CrossRef]
- Iovine, N.M. Resistance mechanisms in Campylobacter jejuni. Virulence 2013, 4, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Sharifi, S.; Bakhshi, B.; Najar-Peerayeh, S. Significant contribution of the CmeABC efflux pump in high-level resistance to ciprofloxacin and tetracycline in Campylobacter jejuni and Campylobacter coli clinical isolates. Ann. Clin. Microbiol. Antimicrob. 2021, 20, 36. [Google Scholar] [CrossRef] [PubMed]
- Castanon, J.I.R. History of the use of antibiotic as growth promoters in European poultry feeds. Poult. Sci. 2007, 86, 2466–2471. [Google Scholar] [CrossRef] [PubMed]
- Wierup, M. The Swedish experience of the 1986-year ban of antimicrobial growth promoters, with special reference to animal health, disease prevention, productivity, and usage of antimicrobials. Microb. Drug Resist. 2001, 7, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Maron, D.F.; Smith, T.J.S.; Nachman, K.E. Restrictions on antimicrobial use in food animal production: An international regulatory and economic survey. Glob. Health 2013, 9, 48. [Google Scholar] [CrossRef] [PubMed]
- Kovač, J.; Čadež, N.; Stessl, B.; Stingl, K.; Gruntar, I.; Ocepek, M.; Trkov, M.; Wagner, M.; Smole Možina, S. High genetic similarity of ciprofloxacin-resistant Campylobacter jejuni in central Europe. Front. Microbiol. 2015, 6, 1169. [Google Scholar] [CrossRef] [PubMed]
- Morita, D.; Arai, H.; Isobe, J.; Maenishi, E.; Kumagai, T.; Maruyama, F.; Kuroda, T. Whole-genome and plasmid comparative analysis of Campylobacter jejuni from human patients in Toyama, Japan, from 2015 to 2019. Microbiol. Spectr. 2023, 11, e0265922. [Google Scholar] [CrossRef]
- Varga, C.; Guerin, M.T.; Brash, M.L.; Slavic, D.; Boerlin, P.; Susta, L. Antimicrobial resistance in Campylobacter jejuni and Campylobacter coli isolated from small poultry flocks in Ontario, Canada: A two-year surveillance study. PLoS ONE 2019, 14, e0221429. [Google Scholar] [CrossRef]
- Wei, B.; Cha, S.Y.; Kang, M.; Roh, J.H.; Seo, H.S.; Yoon, R.H.; Jang, H.K. Antimicrobial susceptibility profiles and molecular typing of Campylobacter jejuni and Campylobacter coli isolates from ducks in South Korea. Appl. Environ. Microbiol. 2014, 80, 7604–7610. [Google Scholar] [CrossRef]
- Kim, J.; Park, H.; Kim, J.; Kim, J.H.; Jung, J.I.; Cho, S.; Ryu, S.; Jeon, B. Comparative analysis of aerotolerance, antibiotic resistance, and virulence gene prevalence in Campylobacter jejuni isolates from retail raw chicken and duck meat in South Korea. Microorganisms 2019, 7, 433. [Google Scholar] [CrossRef]
- Quino, W.; Caro-Castro, J.; Hurtado, V.; Flores-León, D.; Gonzalez-Escalona, N.; Gavilan, R.G. Genomic analysis and antimicrobial resistance of Campylobacter jejuni and Campylobacter coli in Peru. Front. Microbiol. 2021, 12, 802404. [Google Scholar] [CrossRef] [PubMed]
- Ku, B.K.; Kim, H.J.; Lee, Y.J.; Kim, Y.I.; Choi, J.S.; Park, M.Y.; Kwon, J.W.; Nam, H.M.; Kim, Y.H.; Jung, S.C.; et al. Genetic characterization and antimicrobial susceptibility of Campylobacter spp. isolated from domestic and imported chicken meats and humans in Korea. Foodborne Pathog. Dis. 2011, 8, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.S.; Chen, B.H.; Teng, R.H.; Wang, Y.W.; Chang, J.H.; Liang, S.Y.; Tsao, C.S.; Hong, Y.P.; Sung, H.Y.; Chiou, C.S. Antimicrobial resistance in Campylobacter coli and Campylobacter jejuni from human campylobacteriosis in Taiwan, 2016 to 2019. Antimicrob. Agents Chemother. 2022, 66, e0173621. [Google Scholar] [CrossRef] [PubMed]
- Dingle, K.E.; Colles, F.M.; Wareing, D.R.; Ure, R.; Fox, A.J.; Bolton, F.E.; Bootsma, H.J.; Willems, R.J.; Urwin, R.; Maiden, M.C. Multilocus sequence typing system for Campylobacter jejuni. J. Clin. Microbiol. 2001, 39, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, M.; Sousa, A.; Ramirez, M.; Francisco, A.P.; Carriço, J.A.; Vaz, C. PHYLOViZ 2.0: Providing scalable data integration and visualization for multiple phylogenetic inference methods. Bioinformatics 2017, 33, 128–129. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.O.; Jung, S.M.; Na, H.Y.; Chung, G.T.; Yoo, C.K.; Seong, W.K.; Hong, S. Enteric bacteria isolated from diarrheal patients in Korea in 2014. Osong Public Health Res. Perspect. 2015, 6, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.-H.; Choi, O.-K.; Jeong, J.-A. Genetic analysis of Campylobacter jejuni isolates from diarrhea patients in Gyeonggi-do. Korean J. Microbiol. 2018, 54, 31–37. [Google Scholar]
- Nielsen, H.L.; Ejlertsen, T.; Engberg, J.; Nielsen, H. High incidence of Campylobacter concisus in gastroenteritis in north Jutland, Denmark: A population-based study. Clin. Microbiol. Infect. 2013, 19, 445–450. [Google Scholar] [CrossRef]
- Same, R.G.; Tamma, P.D. Campylobacter infections in children. Pediatr. Rev. 2018, 39, 533–541. [Google Scholar] [CrossRef]
- Cho, H.; Lee, S.H.; Lee, J.H.; Lee, S.J.; Park, S.C. Epidemiologic and clinical features of Campylobacter Enteritis before and during COVID-19 in Korea. J. Korean Med. Sci. 2023, 6, 38. [Google Scholar] [CrossRef]
- Kim, Y.J.; Park, K.H.; Park, D.A.; Park, J.; Bang, B.W.; Lee, S.S.; Lee, E.J.; Lee, H.J.; Hong, S.K.; Kim, Y.R. Guideline for the antibiotic use in acute gastroenteritis. Infect. Chemother. 2019, 51, 217–243. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.J.; Seo, K.W.; Mo, I.P.; Lee, Y.J. Genetic characterization of fluoroquinolone resistance in Salmonella enterica serovar Gallinarum isolates from chicken in Korea. Avian Dis. 2019, 63, 584–590. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S.; Lee, M.Y.; Kim, S.J.; Jeon, S.E.; Cha, I.; Hong, S.; Chung, G.T.; Huh, M.J.; Kang, Y.H.; Yoo, C.K.; et al. High-level ciprofloxacin-resistant Campylobacter jejuni isolates circulating in humans and animals in Incheon, Republic of Korea. Zoonoses Public Health 2016, 63, 545–554. [Google Scholar] [CrossRef] [PubMed]
- Cha, I.; Kim, N.O.; Nam, J.G. Gentic diversity of Campylobacter jejuni isolates from Korea and travel-associated case from East and Southeast Asian countries. Jpn. J. Infect. Dis. 2014, 67, 409–494. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Kim, B.J.; Kwon, Y.H.; Hwang, I.Y.; Sung, G.H.; Park, E.H.; Jin, S.H. Antimicrobial susceptibility and genetic analysis of Campylobacter jejuni isolated from diarrhea patients in Busan. Ann. Clin. Microbiol. 2019, 22, 42–49. [Google Scholar] [CrossRef]
- Wei, B.; Cha, S.Y.; Yoon, R.; Kang, M.; Roh, J.; Seo, H.; Lee, J.; Jang, H. Prevalence and antimicrobial resistance of Campylobacter spp. isolated from retail chicken and duck meat in South Korea. Food Control 2016, 62, 63–68. [Google Scholar] [CrossRef]
- Aalipour, F.; Mirlohi, M.; Jalali, M. Determination of antibiotic consumption index for animal originated foods produced in animal husbandry in Iran, 2010. J. Environ. Health Sci. Eng. 2014, 12, 42. [Google Scholar] [CrossRef]
- Park, S.C.; Yun, H.I. Bioavailability and comparative pharmacokinetics of two enrofloxacin formulations in broiler chickens. Korean J. Vet. Clin. Med. 1997, 14, 195–200. [Google Scholar]
- Gratacós-Cubarsí, M.; García-Regueiro, J.A.; Castellari, M. Assessment of enrofloxacin and ciprofloxacin accumulation in pig and calf hair by HPLC and fluorimetric detection. Anal. Bioanal. Chem. 2007, 387, 1991–1998. [Google Scholar] [CrossRef]
- FDA. Final Decision of the Commissioner Docket No. 2000N21571 Withdrawal of Approval of the New Animal Drug Application for Enrofloxacin in Poultry [EB/OL]. 2002. Available online: http://www.fda.gov/AnimalVeterinary/SafetyHealth/RecallsWithdrawals/ucm042004.htm (accessed on 31 October 2023).
- Nelson, J.M.; Chiller, T.M.; Powers, J.H.; Angulo, F.J. Fluoroquinolone-resistant Campylobacter species and the withdrawal of fluoroquinolones from use in poultry: A public health success story. Clin. Infect. Dis. 2007, 44, 977–980. [Google Scholar] [CrossRef]
- van Boven, M.; Veldman, K.T.; de Jong, M.C.; Mevius, D.J. Rapid selection of quinolone resistance in Campylobacter jejuni but not in Escherichia coli in individually housed broilers. J. Antimicrob. Chemother. 2003, 52, 719–723. [Google Scholar] [CrossRef] [PubMed]
- Agriculture, Food and Rural Affairs Quarantine Headquarters, Ministry of Agriculture, Food and Rural Affairs, Ministry of Food and Drug Safety. 2022 National Antibiotic Use and Resistance Monitoring: Animals, Livestock Products. 2022. Available online: https://ebook.qia.go.kr/20230901_131645 (accessed on 31 October 2023).
- DANMAP. Use of Antimicrobial Agents and Occurrence of Antimicrobial Resistance in Bacteria from Food Animals, Food and Humans in Denmark. 2013. Available online: http://www.danmap.org (accessed on 31 October 2023).
- Hur, E.S.; Park, P.H.; Kim, J.H.; Son, J.; Yun, H.; Lee, Y.; Choi, Y.; Yoon, M.; Lee, J. Genetic properties and antimicrobial resistance of Campylobacter jejuni isolates from diarrhea patients in Gyeonggi-do. Korean J. Microbiol. 2013, 49, 228–236. [Google Scholar] [CrossRef]
- One Health Antimicrobial Resistant Organism. Healthy and Happy with the Right Antibiotics. Available online: https://www.kdca.go.kr/nohas/en/common/main.do (accessed on 31 October 2023).
- Asakura, H.; Taguchi, M.; Ekawa, T.; Yamamoto, S.; Igimi, S. Continued widespread dissemination and increased poultry host fitness of Campylobacter jejuni ST-4526 and ST-4253 in Japan. J. Appl. Microbiol. 2013, 114, 1529–1538. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.Y.; Kwon, Y.K.; Wei, B.; Jang, H.K.; Lim, S.K.; Kim, C.H.; Jung, S.C.; Kang, M.S. Epidemiological relationships of Campylobacter jejuni strains isolated from humans and chickens in South Korea. J. Microbiol. 2017, 55, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Su-mi, J.; Byeong-hak, K.; Gyu-rak, H. Genotyping analysis of Campylobacter jejuni isolated from domestic diarrhea patients. Wkly. Health Illn. 2018, 11, 280–285. [Google Scholar]
- Zhang, T.; Luo, Q.; Chen, Y.; Li, T.; Wen, G.; Zhang, R.; Luo, L.; Lu, Q.; Ai, D.; Wang, H.; et al. Molecular epidemiology, virulence determinants and antimicrobial resistance of Campylobacter spreading in retail chicken meat in Central China. Gut Pathog. 2016, 8, 48. [Google Scholar] [CrossRef]
- Ocejo, M.; Oporto, B.; Lavín, J.L.; Hurtado, A. Whole genome-based characterisation of antimicrobial resistance and genetic diversity in Campylobacter jejuni and Campylobacter coli from ruminants. Sci. Rep. 2021, 11, 8998. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Campylobacter spp. | Acute Diarrhea Causative Bacteria PCR Test | Culture Test | |||
|---|---|---|---|---|---|
| No. of Requests | Positive Cases | Positive Rate (%) | Positive Cases | Isolation Rate (%) 1 | |
| Seoul | 3322 | 132 | 4.0% | 35 | 26.5 |
| Gyeonggi | 5877 | 555 | 9.4% | 88 | 15.9 |
| Chungcheong | 4539 | 254 | 5.6% | 39 | 10.9 |
| Jeolla | 8654 | 691 | 8.0% | 75 | 15.0 |
| Gyeongsang | 10,032 | 749 | 7.5% | 104 | 13.9 |
| Gangwon/Jeju | 1087 | 111 | 10.2% | 30 | 27.0 |
| Total | 33,511 | 2492 | 7.4% | 371 | 14.9% |
| Antimicrobial Agents 1 | Species | No. of Isolates with MIC (µg/mL) | MIC50/MIC90 2 (µg/mL) | Resistance Breakpoint 3 (µg/mL) | Resistance Rate (%) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ≤0.06 | 0.125 | 0.25 | 0.5 | 1 | 2 | 4 | 8 | 16 | 32 | 64 | |||||||
| Macrolides | AZI | C. jejuni | 359 | 1 | 1 | ≤0.06/0.125 | ≥0.5 | 0.3 | 0.53 | ||||||||
| C. coli | 9 | 1 | ≤0.06/0.125 | ≥1 | 10 | ||||||||||||
| ERY | C. jejuni | 58 | 179 | 101 | 21 | 1 | 1 | 0.25/0.5 | ≥8 | 0 | 0.53 | ||||||
| C. coli | 2 | 4 | 3 | 1 | 1/2 | ≥16 | 10 | ||||||||||
| Fluoroquinolones | CIP | C. jejuni | 53 | 6 | 4 | 2 | 39 | 114 | 123 | 18 | 2 | 8/16 | ≥1 | 82.6 | 83.3 | ||
| C. coli | 2 | 8 | 16/16 | ≥1 | 100 | ||||||||||||
| Quinolones | NAL | C. jejuni | 58 | 10 | 62 | 120 | 111 | 64/>64 | ≥32 | 64.1 | 64.9 | ||||||
| C. coli | 1 | 2 | 7 | >64/>64 | ≥32 | 90 | |||||||||||
| Lincosamides | CLI | C. jejuni | 303 | 47 | 9 | 1 | 1 | ≤0.06/0.25 | ≥1 | 0.6 | 0.8 | ||||||
| C. coli | 1 | 5 | 2 | 1 | 1 | 0.25/1 | ≥2 | 10 | |||||||||
| Phenicols | FFN | C. jejuni | 2 | 7 | 117 | 203 | 23 | 8 | 1 | 1/1 | ≥8 | 0 | 0 | ||||
| C. coli | 5 | 4 | 1 | 1/2 | ≥8 | 0 | |||||||||||
| Tetracyclines | TET | C. jejuni | 166 | 71 | 5 | 5 | 1 | 4 | 4 | 22 | 21 | 30 | 32 | 0.25/64 | ≥2 | 27.7 | 32.3 |
| C. coli | 2 | 1 | 1 | 2 | 4 | 64/>64 | ≥4 | 70 | |||||||||
| Aminoglycosides | GEN | C. jejuni | 201 | 154 | 5 | 1 | 0.25/0.5 | ≥4 | 0 | 0.53 | |||||||
| C. coli | 6 | 2 | 2 | 0.5/64 | ≥4 | 20 | |||||||||||
| Campylobacter spp. | MDR 1 Phenotype | Antimicrobial Resistance Profiles 2 | No. of Isolates | Rate (%) |
|---|---|---|---|---|
| C. jejuni (n = 361) | TET | 100 | 27.7 | |
| CLI | 2 | 0.55 | ||
| AZI | 1 | 0.27 | ||
| CIP, TET | 111 | 30.7 | ||
| CIP, NAL | 228 | 63.2 | ||
| AZI, CIP, NAL | 1 | 0.27 | ||
| CIP, NAL, TET | 82 | 22.7 | ||
| CIP, NAL, CLI | 1 | 0.27 | ||
| MDR | CIP, NAL, CLI, TET | 1 | 0.27 | |
| MDR | AZI, CIP, NAL, TET | 1 | 0.27 | |
| MDR | AZI, ERY, CIP, NAL, CLI, | 1 | 0.27 | |
| MDR | AZI, ERY, CIP, NAL, CLI, TET | 1 | 0.27 | |
| C. coli (n = 10) | TET | 7 | 70 | |
| GEN | 2 | 20 | ||
| AZI, ERY | 1 | 10 | ||
| CIP, TET | 7 | 70 | ||
| CIP, NAL | 10 | 100 | ||
| CIP, NAL, TET | 7 | 70 | ||
| MDR | CIP, NAL, TET, GEN | 2 | 20 | |
| MDR | AZI, ERY, CIP, NAL, CLI | 1 | 10 |
| Campylobacter spp. | Clonal Complex (CC) | ST | No. of Isolates | Rate (%) | |
|---|---|---|---|---|---|
| C. jejuni (n = 361) | CC21 (n = 136) | 19 | 4 | 37.7% | |
| 21 | 15 | ||||
| 50 | 26 | ||||
| 298 | 8 | ||||
| 451 | 4 | ||||
| 760 | 1 | ||||
| 806 | 4 | ||||
| 982 | 2 | ||||
| 3128 | 1 | ||||
| 3293 | 1 | ||||
| 4253 | 66 | ||||
| 6500 | 4 | ||||
| CC22 (n = 50) | 22 | 50 | 13.8% | ||
| CC206 (n = 34) | 122 | 2 | 9.4% | ||
| 227 | 1 | ||||
| 572 | 28 | ||||
| 3335 | 3 | ||||
| CC45 (n = 22) | 45 | 8 | 6.0% | ||
| 137 | 2 | ||||
| 538 | 1 | ||||
| 583 | 10 | ||||
| 3456 | 1 | ||||
| CC658 (n = 19) | 523 | 2 | 5.3% | ||
| 1044 | 17 | ||||
| CC354 (n = 17) | 12630 | 17 | 4.7% | ||
| CC48 (n = 11) | 48 | 9 | 3.0% | ||
| 918 | 2 | ||||
| CC61 (n = 11) | 61 | 9 | 3.0% | ||
| 81 | 1 | ||||
| 6129 | 1 | ||||
| CC42 (n = 9) | 42 | 8 | 2.5% | ||
| 604 | 1 | ||||
| CC464 (n = 8) | 464 | 7 | 2.2% | ||
| 8627 | 1 | ||||
| CC353 (n = 7) | 5 | 3 | 1.9% | ||
| 1898 | 4 | ||||
| CC443 (n = 4) | 51 | 3 | 1.1% | ||
| 5671 | 1 | ||||
| CC460 (n = 4) | 460 | 4 | 1.1% | ||
| CC508 (n = 4) | 508 | 4 | 1.1% | ||
| CC607 (n = 4) | 904 | 2 | 1.1% | ||
| 3611 | 1 | ||||
| 12635 | 1 | assign | |||
| CC283 (n = 3) | 4063 | 3 | 0.8% | ||
| CC574 (n = 3) | 305 | 2 | 0.8% | ||
| 12630 | 1 | ||||
| CC362 (n = 3) | 12596 | 3 | assign | 0.8% | |
| NT 1 (n = 2) | 12636 | 2 | assign | 0.5% | |
| CC49 (n = 1) | 467 | 1 | 0.2% | ||
| CC1034 (n = 1) | 12640 | 1 | assign | 0.2% | |
| NT (n = 1) | 12268 | 1 | 0.2% | ||
| NT (n = 1) | 12597 | 1 | assign | 0.2% | |
| NT (n = 1) | 12656 | 1 | assign | 0.2% | |
| NT (n = 1) | 2274 | 1 | 0.2% | ||
| NT (n = 1) | 4240 | 1 | 0.2% | ||
| NT (n = 1) | 5046 | 1 | 0.2% | ||
| NT (n = 2) | 5229 | 2 | 0.5% | ||
| C. coli (n = 10) | CC828 (n = 9) | 830 | 1 | 90% | |
| 854 | 1 | ||||
| 860 | 2 | ||||
| 872 | 1 | ||||
| 9201 | 1 | ||||
| 9867 | 1 | ||||
| 12600 | 1 | assign | |||
| 12613 | 1 | assign | |||
| NT (n = 1) | 10873 | 1 | 10% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.Y.; An, D.; Jeong, H.; Kim, J. Antimicrobial Susceptibility Patterns and Genetic Diversity of Campylobacter spp. Isolates from Patients with Diarrhea in South Korea. Microorganisms 2024, 12, 94. https://doi.org/10.3390/microorganisms12010094
Kim SY, An D, Jeong H, Kim J. Antimicrobial Susceptibility Patterns and Genetic Diversity of Campylobacter spp. Isolates from Patients with Diarrhea in South Korea. Microorganisms. 2024; 12(1):94. https://doi.org/10.3390/microorganisms12010094
Chicago/Turabian StyleKim, So Yeon, Dongheui An, Hyemi Jeong, and Jonghyun Kim. 2024. "Antimicrobial Susceptibility Patterns and Genetic Diversity of Campylobacter spp. Isolates from Patients with Diarrhea in South Korea" Microorganisms 12, no. 1: 94. https://doi.org/10.3390/microorganisms12010094