
Interplay between the Human Microbiome and Biliary Tract Cancer: Implications for Pathogenesis and Therapy

1
The First Clinical Medical College, Lanzhou University, Lanzhou 730000, China
2
Department of General Surgery, The First Hospital of Lanzhou University, Lanzhou 730000, China
3
Department of General Surgery, The Second Hospital of Lanzhou University, Lanzhou 730000, China
*
Author to whom correspondence should be addressed.
Microorganisms 2023, 11(10), 2598; https://doi.org/10.3390/microorganisms11102598
Submission received: 29 August 2023
/
Revised: 12 October 2023
/
Accepted: 19 October 2023
/
Published: 20 October 2023
(This article belongs to the Section Gut Microbiota)
Abstract
:Biliary tract cancer, encompassing intrahepatic and extrahepatic cholangiocarcinoma as well as gallbladder carcinoma, stands as a prevalent malignancy characterized by escalating incidence rates and unfavorable prognoses. The onset of cholangiocarcinoma involves a multitude of risk factors and could potentially be influenced by microbial exposure. The human microbiome, encompassing the entirety of human microbial genetic information, assumes a pivotal role in regulating key aspects such as host digestion, absorption, immune responses, and metabolism. The widespread application of next-generation sequencing technology has notably propelled investigations into the intricate relationship between the microbiome and diseases. An accumulating body of evidence strongly suggests a profound interconnection between biliary tract cancer and the human microbiome. This article critically appraises the existing evidence pertaining to the microbiome milieu within patients afflicted by biliary tract cancer. Furthermore, it delves into potential mechanisms through which dysregulation of the human microbiome could contribute to the advancement of biliary tract cancer. Additionally, the article expounds on its role in the context of chemotherapy and immunotherapy for biliary tract cancer.
1. Introduction
Biliary tract cancer refers to a spectrum of invasive adenocarcinomas, including cholangiocarcinoma and gallbladder carcinoma [1]. Cholangiocarcinoma is further categorized into intrahepatic cholangiocarcinoma (ICC) and extrahepatic cholangiocarcinoma (the latter further divides into perihilar and distal cholangiocarcinoma). The incidence of biliary tract cancer exhibits variation across subgroups and geographic regions, exhibiting a notable rise over the years, particularly for ICC. In the United States, ICC’s incidence escalated from 0.44 to 1.18 cases per 100,000, while extrahepatic cholangiocarcinoma experienced a more modest increase from 0.95 to 10.2 per 100,000 over a 40-year period [2]. Cholangiocarcinoma has a poor prognosis and is usually identified at advanced stages. This typically occurs when the primary tumor reaches a substantial size, resulting in a sizable liver mass, or when jaundice develops due to obstruction in the biliary tree [3].
Epidemiological investigations have elucidated the involvement of multiple risk factors in the genesis of cholangiocarcinoma. Bile duct cysts, primary sclerosing cholangitis, hepatolithiasis, cholelithiasis, and choledocholithiasis all exhibit associations with cholangiocarcinoma [4]. In addition, the liver fluke Opisthorchis viverrini is the main cause of cholangiocarcinoma in Southeast Asia [5]. Host genetics, lifestyle choices, environmental exposures, and other factors also influence the course of cholangiocarcinoma [4]. The term “microbiome” pertains to the cumulative genetic makeup of microorganisms within a specific environment, carrying a pivotal role in immune regulation and safeguarding the host against pathogenic microbes [6]. Disruption of the gut microbiome has been implicated in an array of conditions, encompassing cancer and metabolic disorders [7,8].
The advent of next-generation sequencing (NGS) technology has made microbiome analysis more convenient, thereby fostering a substantial upsurge in research investigating the interplay between the human microbiome and cancer. Mounting evidence underscores the potential impact of the microbial milieu on individuals with biliary tract cancer [9]. Notably, individuals afflicted with biliary tract cancer often exhibit elevated levels of Enterobacteriaceae but diminished levels of Clostridia, including Faecalibacterium and Coprococcus. Enterobacteriaceae see enrichment within the fecal samples of those with biliary tract cancer, with over half of the Enterobacteriaceae identified in bile matching those present in fecal samples at the operational taxonomic unit (OTU) level. These findings collectively hint at the potential contribution of fecal microbiota dysbiosis to the development of biliary tract cancer [10]. Within this review, we delve into the intricate relationship between the digestive tract microbiome and biliary tract tumors, dissecting the role and significance of the digestive tract microbiome in the realm of biliary tract cancer treatment.
2. Biliary Tract Cancer and the Human Microbiome
2.1. The Microbiome and Intrahepatic Cholangiocarcinoma
Intrahepatic cholangiocarcinoma (ICC) stands as a highly malignant form of primary liver cancer, originating from the epithelial cells of intrahepatic bile ducts [1,11]. The scarcity of typical clinical symptoms leads to a mere 22% of patients qualifying for surgical intervention [12]. The emergence of cholangiocarcinoma is intricately tied to the carcinogenic influence of chronic biliary inflammation [13]. While primary sclerosing cholangitis, Caroli’s disease, and choledochal cysts share associations with all cholangiocarcinoma variants, cirrhosis, non-alcoholic fatty liver disease (NAFLD), and hepatitis B exhibit a stronger link with ICC [14].
Studies have unveiled a connection between the occurrence of ICC and gut dysbiosis [15,16,17]. Jia et al. analyzed gut microbiota and bile acid metabolism in patients with ICC, systematically demonstrating the relationship among gut microbiota, bile acid, and cytokine profiles. Comparatively, ICC displayed the highest α-diversity and β-diversity when juxtaposed against patients with hepatocellular carcinoma, liver cirrhosis, and healthy individuals. Notably enriched in ICC were Actinomyces, Lactobacillus, Peptostreptococcaceae, and Alloscardovia. Furthermore, the glycoursodeoxycholic acid and tauroursodeoxycholic acid (TUDCA) plasma-stool ratios were significantly increased in ICC, with the genera Lactobacillus and Alloscardovia exhibiting positive correlations with the TUDCA plasma-stool ratio. These biomarkers could be used to differentiate ICC from hepatocellular carcinoma (HCC) [18]. Deng et al. conducted a comprehensive analysis encompassing a cohort of 40 healthy volunteers, 143 HCC patients, and 46 cholangiocarcinoma patients based on fecal 16S rRNA sequencing. The cholangiocarcinoma group displayed increased gram-negative bacteria levels and inflammatory markers compared to the HCC group. They established the gut microbiome-based model for liver cancer prediction and screening, divulging a correlation between primary liver cancer-related gut microbiome characteristics and unfavorable inflammatory response markers [19]. Similarly, Zhang et al. explored a gut microbiota model covering the genera Burkholderia-Caballeronia-Paraburkholderia, Faecalibacterium, and Ruminococcus_1 (B-F-R) for early cholangiocarcinoma diagnosis [20]. Moreover, oral microbiota-targeted biomarkers have emerged as effective noninvasive diagnostic tools for cholangiocarcinoma [21]. In instances of mice afflicted with primary sclerosing cholangitis (PSC) and colitis, compromised gut barrier function facilitated the infiltration of gut-derived bacteria and lipopolysaccharides (LPS) into the liver. The intestinal microbiome spurred CXCL1 expression in hepatocytes via TLR4-dependent mechanisms, fostering the accumulation of CXCR2+ polymorphonuclear myeloid-derived suppressor cells (PMN-MDSC). This mechanism created an immunosuppressive environment in hepatocytes, thereby promoting ICC development [22]. Thus, the gut microbiome holds promise as a potential ICC biomarker.
Beyond the digestive tract microbiome, other facets of the microflora within ICC patients have garnered attention. Chai et al. performed 16S rRNA sequencing, single-cell RNA sequencing (scRNA-seq), and multilayer validation on cholangiocarcinoma tissues. They verified the presence of microbial DNA in tissues via staining, fluorescence in situ hybridization (FISH), and transmission electron microscopy (TEM). Intratumoral bacteria manifest across multiple cell types, as evidenced by scRNA-seq [23]. Chng et al. found that a distinct and tissue-specific microbiome dominated by the families Dietziaceae, Pseudomonadaceae, and Oxalobacteraceae was observed in the bile duct tissues. Compared to paracancerous tissue and normal liver tissue, substantial variations in colonized flora were noted in bile duct carcinoma tissue, with Stenotrophomonas species showing a significant increase. The enrichment of specific enteric bacteria (Bifidobacteriaceae, Enterobacteriaceae, and Enterococcaceae) correlated with parasite-associated cholangiocarcinoma [24]. Moreover, intratumoral microbial composition held relevance in chemotherapy resistance within cholangiocarcinoma [25]. Lee et al. isolated bacterial-derived extracellular vesicles from the plasma of biliary tract cancer patients, dissecting microbiome composition via 16S rDNA metagenomic analysis. Microflora composition showed variable percentages from phylum to genus level. They formulated a predictive model for biliary tract cancer based on variations in blood microbial composition. However, blood microbiome exploration remains relatively nascent, necessitating further research to comprehend alterations and underlying mechanisms [26].
2.2. The Microbiome and Extrahepatic Cholangiocarcinoma
Choledocholithiasis exhibits a clear correlation with extrahepatic cholangiocarcinoma and serves as a potential risk factor for its development. This association may be attributed to biliary bacterial infections [14]. Jan Bednarsch et al. conducted a study involving intraoperative bile samples from patients with hilar cholangiocarcinoma to perform microbial cultures. The results indicated a substantial colonization of the bile ducts by bacteria. Among the most prevalent bacteria identified in the bile ducts were Enterococcus faecalis (38.8%, 31/80), Enterococcus faecium (32.5%, 26/80), Enterobacter cloacae (16.3%, 13/80), and Escherichia coli (11.3%, 9/80). Notably, reduced susceptibility of these bacteria to intraoperative antibiotic prophylaxis was identified as an independent predictor of postoperative abdominal infections [27]. Di Carlo et al. demonstrated that an unprecedented increase in E. coli within the bile of cholangiocarcinoma patients corresponded to decreased survival rates. This suggests that certain strains isolated from bile samples may be considered as contributing to the group of risk factors in the carcinogenesis and/or progression of hepatobiliary malignancies [28]. In addition, isolated biliary candidiasis may be associated with a poor prognosis in patients with unresectable cholangiocarcinoma [29].
The utilization of next-generation sequencing technology has greatly facilitated the exploration of the intestinal and biliary microflora. Extensive investigations have been conducted on the bile microbiome of individuals with extrahepatic cholangiocarcinoma [30,31,32]. These studies involve the collection of bile samples through ERCP from patients with cholangiocarcinoma and cholangiolithiasis for 16S rRNA sequencing analysis. The analysis outcomes revealed that the most abundant genera within the biliary microflora were Enterococcus, Streptococcus, Bacteroides, Klebsiella, and Pyramidobacter. In comparison to cholangiolithiasis cases, levels of Bacteroides, Geobacillus, Meiothermus, and Anoxybacillus genera were significantly elevated in the biliary microbiota of patients with extrahepatic cholangiocarcinoma [30,31]. Noteworthy discrepancies exist in the microbial communities present in the bile of choledocholithiasis and cholangiocarcinoma patients. These bacteria potentially play a partial role in the onset of cholangiocarcinoma and could serve as novel biomarkers for this condition [33].
Aviles-Jimenez et al. collected bile duct epithelial cells via brushing from 100 patients with extrahepatic cholangiocarcinoma and 100 patients with benign biliary diseases during ERCP. Their analysis of DNA extractions revealed reduced levels of Nesterenkonia but increased levels of Methylophilaceae, Fusobacterium, Prevotella, Actinomyces, Novosphingobium, and H. pylori in extrahepatic cholangiocarcinoma cases. They verified the potential role of H. pylori in the development of extrahepatic cholangiocarcinoma [34]. Miyabe et al. identified a distinctive microbial signature in the bile of patients with prolonged PSC duration or those with cholangiocarcinoma, suggesting a role for microbiota-driven inflammation in the pathogenesis or progression of perihilar cholangiocarcinoma [35]. Thus, the microbiome of the digestive tract emerges as a pivotal factor in the development of extrahepatic cholangiocarcinoma. Table 1 presents studies evaluating microbial composition in patients with biliary tract cancer.
2.3. The Microbiome and Gallbladder Cancer
Gallbladder cancer is a prevalent malignancy affecting the biliary tract, and its prognosis is notably grim when diagnosed at an advanced stage due to its aggressive nature and limited treatment avenues. Prolonged chronic inflammation plays a pivotal role in the development of gallbladder cancer, irrespective of whether it originates from gallstones or other sources [36]. Multiple studies have indicated a heightened risk of gallbladder cancer in the presence of bacterial infections. Notably, analysis of bile samples from gallbladder cancer patients revealed a substantial increase in bacterial taxa [37]. It is plausible that chronic bacterial infection of the bile, leading to the production of carcinogenic precursors, is among the causative factors underlying the emergence of gallbladder carcinoma [38]. The persistent presence of certain bacteria triggers chronic inflammation, giving rise to toxins and metabolites with carcinogenic potential. These elements contribute to the transformation of gallbladder epithelial cells [39].
Tsuchiya et al. conducted a study comparing bacteria found in bile samples from gallbladder cancer patients and those with cholelithiasis. The study highlighted that the incidence of bacterial infection in bile was 42.9 percent for gallbladder cancer patients, compared to 13.3 percent for cholelithiasis patients. The dominant species identified in the bile of gallbladder cancer patients included Fusobacterium nucleatum, Escherichia coli, and Enterobacter sp., while the bile from cholelithiasis patients primarily contained Escherichia coli, Salmonella sp., and Enterococcus gallinarum [40]. Another study hints at a potential correlation between a dysbiotic bile microbiome and the development of chronic calculous cholecystitis and gallbladder cancer. Patients with chronic cholecystitis and an imbalanced microbiome pattern exhibited larger gallstones and notable epithelial abnormalities, considered precancerous conditions. These findings suggest the potential involvement of Enterobacteriaceae, including Klebsiella, in gallbladder carcinogenesis [41].
The chronic presence of Salmonella typhi in gallbladder disease may contribute to the onset of gallbladder cancer [42]. Meta-analysis indicated that chronic Salmonella typhi infection correlated with an increased risk of gallbladder cancer, representing a significant risk factor for the condition [43,44]. Experimental evidence underscores the ability of Salmonella enterica to facilitate the transformation of genetically predisposed cells, ultimately acting as a causative agent of gallbladder cancer. This bacterium induces malignant transformation in susceptible mice, murine gallbladder organoids, and fibroblasts by triggering TP53 mutations and c-MYC amplification. Mechanistically, the activation of MAPK and AKT pathways, mediated by Salmonella enterica effectors released during infection, is instrumental in both initiating and sustaining transformation [45]. Beyond Bacillus typhoid, infection with specific strains of H. pylori has also been linked to an increased risk of biliary tract cancer [46,47]. Experimental data suggests that Helicobacter bilis infection activates transcription factors such as NFKB, leading to enhanced angiogenesis through VEGF production. The involvement of Helicobacter bilis infection may be significant in biliary tract malignancies [48].
In a study by Song et al., mucosal DNA extraction and metagenomic sequencing were employed to compare the microbiota between patients with chronic calculous cholecystitis and gallbladder cancer. This analysis revealed substantial differences in biliary microbial composition and gene function between the two groups. Peptostreptococcus stomatis and Enterococcus faecium were identified as potential contributors to the progression of gallbladder cancer [49]. Furthermore, a notable connection was established between the relative abundance of specific microbes and the overall survival prognosis of patients with pancreaticobiliary tract cancer [50]. Hence, targeting bacterial infections through anti-inflammatory treatments and hygiene practices could potentially mitigate the incidence of gallbladder cancer.

{kind=link}
Table 1.
Studies evaluating microbial composition in patients with biliary tract cancer.
| Author, Year | Biological Specimens | Sampling Methods | Tumor Site and Size | Main Conclusion |
|---|---|---|---|---|
| Chen, 2019 [30] | bile | ERCP | dCCA, 8 | Proteobacteria, Firmicutes, Bacteroidetes, and Actinobacteria are the most dominant phyla in the bile. Gemmatimonadetes, Nitrospirae, Chloroflexi, Latescibacteria, and Planctomycetes in the phylum increase in dCCA patients compared with the onset of common bile duct stones patients. |
| Avilés-Jiménez, 2016 [34] | biliary duct epithelial cells | Brushing during ERCP | eCCA, 100 | Phylum Proteobacteria dominated all samples (60.4% average). Nesterenkonia decreased, whereas Methylophilaceae, Fusobacterium, Prevotella, Actinomyces, Novosphingobium, and H. pylori increased in eCCA. Predicted associated functions showed an increased abundance of H. pylori virulence genes in eCCA. |
| Saab, 2021 [31] | bile | ERCP | eCCA, 28 | Proteobacteria did not significantly differ between eCCA patients and controls. The most abundant genera were Enterococcus, Streptococcus, Bacteroides, Klebsiella, and Pyramidobacter in eCCA’s biliary microbiota. Levels of Bacteroides, Geobacillus, Meiothermus, and Anoxybacillus genera were significantly higher in eCCA patients’ biliary microbiota, without an associated disease, in comparison with controls. |
| Li, 2022 [32] | bile | ERCP | pCCA, 14 dCCA, 9 | The top three biomarkers for pCCA at the genus level were Pseudomonas, Sphingomonas, and Halomonas; for dCCA, they were Streptococcus, Prevotella, and Halomonas. |
| Miyabe, 2022 [35] | Bile and stool | ERCP | CCA (mainly pCCA), 49 | Increased species richness and abundance of Fusobacteria were correlated with the duration of PSC and characterized the biliary microbiota in CCA. |
| Ito, 2022 [10] | Bile and stool | ERCP | iCCA, 12 eCCA, 12 GBC, 6 | A higher Enterobacteriaceae abundance and a lower Clostridia abundance, including that of Faecalibacterium and Coprococcus, in the BTC patients than in the other subjects. A bile-isolated strain possessed the carcinogenic bacterial colipolyketide synthase-encoding gene. |
| Di Carlo, 2019 [28] | bile | ERCP | CCA, 42 GBC, 5 | E. coli and P. aeruginosa were significant negative predictors of CCA. About GBC, there were no significant correlations with E. coli, K. pneumoniae, or P. aeruginosa. |
| Pomyen, 2023 [51] | stool | - | iCCA, 19 | Two Veillonella species were found to be more abundant in iCCA samples and could distinguish iCCA from HCC and healthy controls. Ruminococcus gnavus was depleted in iCCA patients and could distinguish HCC from iCCA samples. High Veillonella genus counts in the iCCA group were associated with enriched amino acid biosynthesis and glycolysis pathways. |
| Chai, 2023 [23] | tissues | surgery | iCCA, 99 | The most abundant bacterial orders include Burkholderiales, Pseudomonadales, Xanthomonadales, Bacillales, and Clostridiales. The content of Paraburkholderia fungorum was significantly higher in the paracancerous tissues. |
| Deng, 2022 [19] | fecal | - | CCA, 46 | Gammaproteobacteria were significantly higher in both gemcitabine- and cisplatin-resistance groups compared to sensitive groups. |
| Jia, 2020 [18] | stool and blood | - | iCCA, 28 | The abundances of four genera (Lactobacillus, Actinomyces, Peptostreptococcaceae, and Alloscardovia) were increased in patients with ICC compared with those in patients with hepatocellular carcinoma or liver cirrhosis and in healthy individuals. The glycoursodeoxycholic acid and tauroursodeoxycholic acid (TUDCA) plasma-stool ratios were obviously increased in patients with ICC. |
| Chng, 2016 [24] | tissue | - | CCA, 60 | A distinct, tissue-specific microbiome dominated by the bacterial families Dietziaceae, Pseudomonadaceae, and Oxalobacteraceae was observed in bile duct tissues. Several bacterial families, with a significant increase in Stenotrophomonas species distinguishing tumors from paired normals. |
3. The Effect of Dysbiosis on Biliary Tract Cancer and Its Precancerous Lesions
The impairment of intestinal barrier function facilitates the buildup of gut-derived bacteria and LPS within the portal vein. This process triggers the accumulation of myeloid-derived suppressor cells (MDSC) via TLR4-dependent mechanisms, thus fostering immune evasion and driving the advancement of CCA. Fecal microbiota transplantation (FMT) has been shown to encourage MDSC accumulation in the liver using fecal samples from mice with intestinal disorders. However, pre-treating donor mice with neomycin to eliminate gram-negative bacteria counters this effect. The MDSC induced by gram-negative bacteria assumes a pivotal role in amplifying cholangiocarcinoma progression [22,52].
Primary sclerosing cholangitis (PSC), an immune-associated cholangitis, is linked to a heightened risk of cholangiocarcinoma and gallbladder cancer [53,54]. Evidence indicates that the dysregulation of the microflora is implicated in the pathogenesis of PSC [55,56]. Patients with PSC display disruptions in the upper digestive tract and bile duct microbiota. Biliary dysbiosis is correlated with elevated levels of the proinflammatory and potentially cancerogenic agent taurolithocholic acid [57].
Over the past decade, an array of studies involving both humans and animal models have underscored the role of the microbiome in various segments of the gastrointestinal tract in the development of gallstone disease [58]. Changes in the gastrointestinal microbiome may reshape the pathogenesis of cholesterol gallstone formation. Alterations in the oral microbiome influence the expression of mucin genes via immune modulation. This, in turn, modifies the accumulation of mucin gel, thereby heightening the risk of bile supersaturation and ultimately accelerating the process of gallstone formation [59,60]. The presence of Helicobacter pylori infection contributes to the formation of cholecystic polyps and gallstones [61] and affects the pathophysiology of gallstone formation along with its associated complications such as cholecystitis, cholangitis, pancreatitis, and biliary cancer [62]. Intestinal bacteria (Clostridium, Bifidobacterium, Peptostreptococcus, Bacteroides, Eubacterium, and Escherichia coli) involved in bile acid oxidation and epimerization can disrupt enterohepatic circulation, culminating in gallstone formation [58,63]. Hence, the disruption of the human flora equilibrium propels the progression of biliary tract cancer and its precancerous lesions.
4. Potential Role of Microbes in Chemotherapy and Immunotherapy for Biliary Tract Cancer
Immunotherapy stands as a pivotal approach for treating malignant tumors; its efficacy is influenced by intestinal flora and environmental factors [64,65]. The significance of the gut microbiome in various metabolic and signaling pathways, as well as its role in carcinogenesis, has been somewhat underestimated. Presently, it garners widespread attention as a critical avenue to bolster immunotherapy responses [66]. Demonstrated effects of the microbiota on cancer initiation, progression, and treatment response have hinted at potential contributions to susceptibility to specific cancers and possibly influencing treatment outcomes [67,68]. The correlation between the gut microbiome and the response to immune checkpoint inhibitors (ICI) is emerging as an intriguing area. The gut microbiome is linked to tumor immune resistance. The strategic combination of probiotics with ICI may aid in reshaping the microbiome [69].
Despite early clinical trials showing a relatively modest response rate of immunocheckpoint therapy (ICT) in cholangiocarcinoma [70], its therapeutic potential remains underexplored. Although potential MDSCs have been detected in cholangiocarcinoma, their exact role in its pathogenesis has remained unclear [52]. Recent studies have illuminated the potential of targeting MDSCs in other cancers to activate anti-tumor immune responses and amplify the effectiveness of ICTs [71,72]. Through the amalgamation of intestinal barrier dysfunction, the intestinal microbiome, and MDSC regulation, Zhang introduces a novel paradigm where inflammatory bowel diseases (IBD) and PSC may foster immunosuppression, thus molding the liver microenvironment conducive to cholangiocarcinoma progression [22]. The outcomes propose a variety of novel targets for intervening in cholangiocarcinoma growth, encompassing gram-negative intestinal bacteria, TLR4, CXCL1, CXCR2, and MDSCs themselves. This pivotal step in reversing the immunosuppressive microenvironment holds promise for heightening immunotherapy strategies, including ICT. In a study by Mao et al., the gut microbiome’s association with the clinical response to anti-PD-1 immunotherapy in hepatobiliary cancer patients was unveiled. Taxonomic signatures enriched in responders prove to be effective biomarkers for predicting clinical response and survival benefits from immunotherapy. This discovery offers a potential therapeutic target for modulating responses to cancer immunotherapy [73]. The microbiota may have exciting implications for therapeutic strategies for the microbiota-immune system axis in cholangiocarcinoma [74]. Microorganisms could potentially serve as drug targets for cholangiocarcinoma treatment, with fecal microbiota transplantation (FMT) potentially aiding in rectifying biological imbalances and optimizing anti-tumor immune responses. However, this therapeutic approach warrants further investigation.
5. The Role of Bacterial Metabolites in the Progression of Biliary Tract Cancer
In recent years, metabolomics has gained widespread utilization in hepatobiliary diseases, demonstrating significant advantages in understanding disease pathogenesis [75]. Analysis of the humoral metabolome is emerging as a promising diagnostic strategy, potentially linked to disease progression [76]. Bile acids are metabolized by enzymes produced by gut bacteria and are essential for maintaining a healthy gut microbiome and innate immunity. The liver–bile acid–microbiota axis plays an important role in gastrointestinal carcinogenesis [77,78]. Murakami et al. validated the connection between ICC and lipid metabolism as well as bile secretion, elucidating their participation in the metabolic reprogramming of ICC [79]. Furthermore, distinct alterations in plasma bile acid concentrations have been identified as potential diagnostic biomarkers for distinguishing cholangiocarcinoma from benign biliary diseases and healthy individuals [80]. Likewise, specific changes in serum metabolite levels contribute to the differentiation between ICC, HCC, and PSC [81].
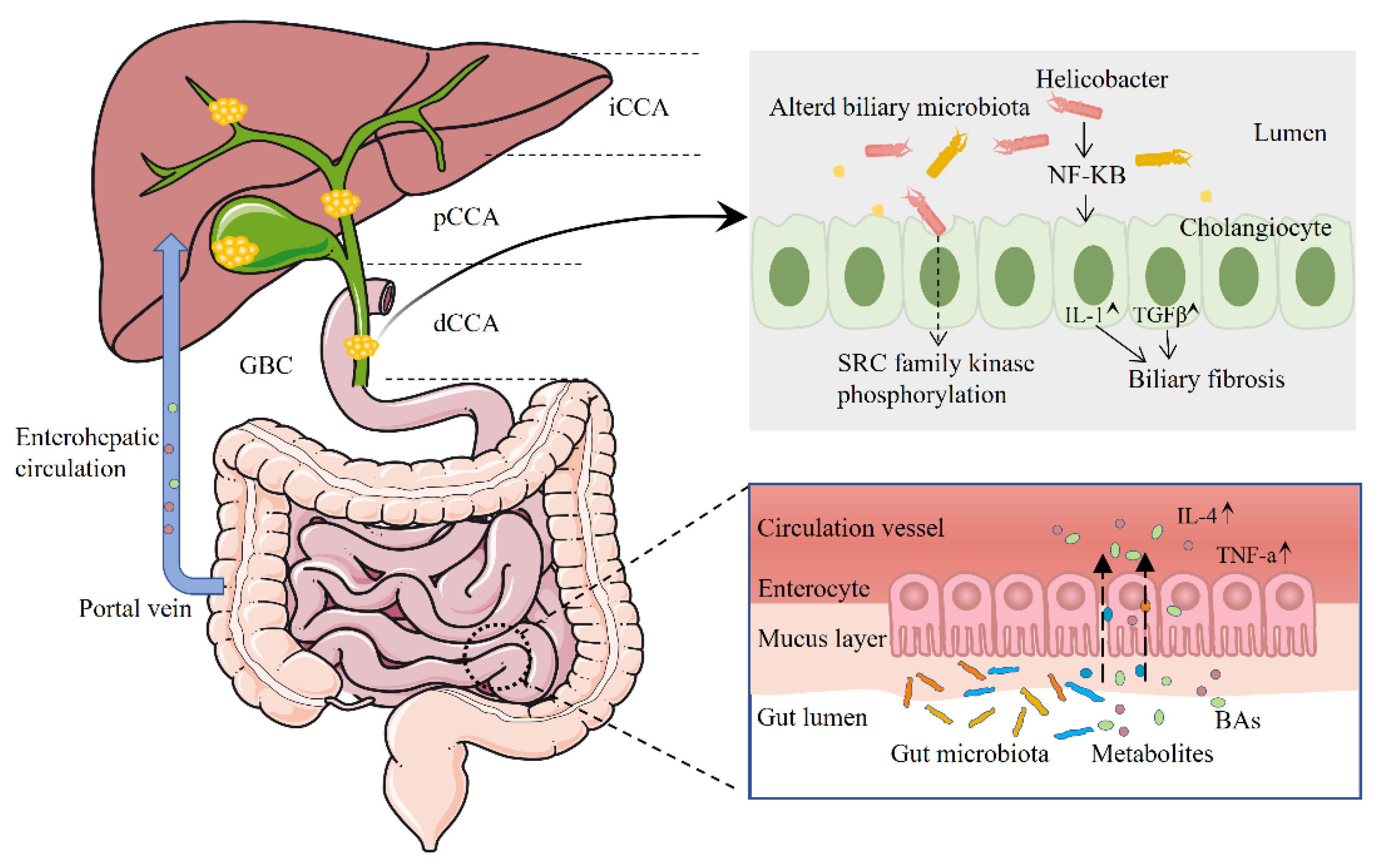
Liu et al. observed high expression of S1PR2 in both rat and human cholangiocarcinoma cells, as well as in human cholangiocarcinoma tissues. They revealed that conjugated bile acids can promote the aggressive growth of cholangiocarcinoma cells through S1PR2 signaling [82]. In another study, Li et al. conducted GC-MS-based metabolomics experiments on ICC and intrahepatic bile duct stone (IBDS) pathological tissues, along with ICC para-carcinoma tissues. Their findings emphasized that the metabolic disparities between IBDS and ICC mainly revolve around linoleic acid metabolic pathways. Perturbations in the linoleic acid pathway might contribute to the potential malignant transformation of intrahepatic bile duct stones into ICC [83]. Chai et al. discovered that results from both in vitro and in vivo experiments strongly support the idea that P. fungorum demonstrates anti-tumor activity by modulating alanine, aspartate, and glutamate metabolism [23]. Figure 1 shows the relationship between human microbiome, metabolites and biliary tract cancer. Research on microbial metabolites in hepatobiliary diseases has gradually attracted attention, contributing to the understanding of disease mechanisms.
6. Future Directions
The symbiotic microbial community within the human body represents a crucial element of human microbial equilibrium. Maintaining the stability of this microbial community might hold the key to averting tumorigenesis.
The current research on the microbiota in cholangiocarcinoma is constrained by factors such as sample quality and environmental interference. There can be significant biological variations among cholangiocarcinoma patients, including factors like tumor location, size, and differentiation level, leading to considerable variability in microbiota composition. Additionally, microbial communities are influenced by environmental factors such as diet and lifestyle, which may impact research outcomes. Microbiome profiling techniques may face limitations in terms of technical sensitivity and specificity, potentially resulting in the under-detection or misidentification of certain microorganisms. While alterations in microbiota composition associated with cholangiocarcinoma have been observed, further empirical evidence is needed to determine whether these microorganisms play a causal role or are merely correlated with the disease.
The intestinal flora, potentially serving as a non-invasive diagnostic biomarker for cholangiocarcinoma, holds promise as a tool for early diagnosis, prediction, and even as a future therapeutic target in biliary tract cancer. This approach could enhance the prospects of successful treatment. Envisioned is the continuous enhancement of cancer chemotherapy and immunotherapy efficacy through the utilization of gut flora. Distinct shifts in gut flora composition might lead to the production of specific metabolites that could be identified and exploited for early diagnosis. However, comprehensive comprehension of the mechanisms behind microbial-driven carcinogenesis remains a priority. More clinical and fundamental investigations are imperative. Moving forward, large-scale cohort studies are necessary to deeply analyze the microbiome using a multi-omics approach. Simultaneously, heightened focus should be directed towards elucidating the functions of the microbiome and its metabolites to gain a deeper understanding of the mechanisms underlying microbiome-related carcinogenesis. This understanding can then be harnessed to refine strategies for preventing, diagnosing, and treating biliary tract cancer. As our understanding of the intricate connection between the microbiome and biliary tract cancer deepens, the microbiome is poised to become a pivotal factor in cancer prevention and treatment. However, further research is indispensable to fully grasping its role and translating this knowledge into effective clinical strategies.
Author Contributions
Conceptualization, C.Y. and C.D.; methodology, W.Z., C.Y. and C.D.; formal analysis, C.Y., Y.L. and C.D.; writing—original draft preparation, C.Y., H.S. and C.D.; writing—review and editing, C.Y., H.S. and C.D.; visualization, W.Z., C.Y. and C.D.; supervision, W.Z., C.Y. and C.D. All authors have read and agreed to the published version of the manuscript.
Funding
This work was financially supported by the National Natural Science Foundation of China (No. 82260555 and No. 32160255), the First Hospital of Lanzhou University Intra-Hospital Fund Youth Fund (ldyyyn2021-78), the Education Department of Gansu Province: Innovation Fund Project (2022B-027), and the Lanzhou talent innovation and entrepreneurship project (2022-3-42).
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
CCA, cholangiocarcinoma; dCCA, distal cholangiocarcinoma; E. coli, Escherichia coli; eCCA, extrahepatic cholangiocarcinoma; FISH, fluorescence in situ hybridization; FMT, Fecal microbiota transplantation; GBC, gallbladder carcinoma; H. pylori, helicobacter pylori; HCC, hepatocellular carcinoma; IBD, inflammatory bowel diseases; IBDS, intrahepatic bile duct stone; ICC/iCCA, intrahepatic cholangiocarcinoma; ICI, immune checkpoint inhibitors; ICT, immunocheckpoint therapy; LPS, lipopolysaccharides; MDSC, myeloid-derived suppressor cells; NAFLD, non-alcoholic fatty liver disease; NGS, next-generation sequencing; OUT, operational taxonomic unit; pCCA, perihilar cholangiocarcinoma; PMN-MDSC, polymorphonuclear myeloid-derived suppressor cells; PSC, primary sclerosing cholangitis; scRNA-seq, single-cell RNA sequencing; TEM, transmission electron microscopy; TUDCA, tauroursodeoxycholic acid.
References
- Valle, J.W.; Kelley, R.K.; Nervi, B.; Oh, D.Y.; Zhu, A.X. Biliary tract cancer. Lancet 2021, 397, 428–444. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.K.; Zhu, A.X.; Fuchs, C.S.; Brooks, G.A. Forty-Year Trends in Cholangiocarcinoma Incidence in the U.S.: Intrahepatic Disease on the Rise. Oncologist 2016, 21, 594–599. [Google Scholar] [CrossRef]
- Forner, A.; Vidili, G.; Rengo, M.; Bujanda, L.; Ponz-Sarvisé, M.; Lamarca, A. Clinical presentation, diagnosis and staging of cholangiocarcinoma. Liver Int 2019, 39 (Suppl. S1), 98–107. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.A.; Tavolari, S.; Brandi, G. Cholangiocarcinoma: Epidemiology and risk factors. Liver Int. 2019, 39 (Suppl. S1), 19–31. [Google Scholar] [CrossRef]
- Sripa, B.; Tangkawattana, S.; Brindley, P.J. Update on Pathogenesis of Opisthorchiasis and Cholangiocarcinoma. Adv. Parasitol. 2018, 102, 97–113. [Google Scholar]
- Honda, K.; Littman, D.R. The microbiota in adaptive immune homeostasis and disease. Nature 2016, 535, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Pedersen, O. Gut microbiota in human metabolic health and disease. Nat. Rev. Microbiol. 2021, 19, 55–71. [Google Scholar] [CrossRef]
- Sepich-Poore, G.D.; Zitvogel, L.; Straussman, R.; Hasty, J.; Wargo, J.A.; Knight, R. The microbiome and human cancer. Science 2021, 371, eabc4552. [Google Scholar] [CrossRef]
- Wheatley, R.C.; Kilgour, E.; Jacobs, T.; Lamarca, A.; Hubner, R.A.; Valle, J.W.; McNamara, M.G. Potential influence of the microbiome environment in patients with biliary tract cancer and implications for therapy. Br. J. Cancer 2022, 126, 693–705. [Google Scholar] [CrossRef]
- Ito, Z.; Koido, S.; Kato, K.; Odamaki, T.; Horiuchi, S.; Akasu, T.; Saruta, M.; Hata, T.; Kumagai, Y.; Fujioka, S.; et al. Dysbiosis of the Fecal and Biliary Microbiota in Biliary Tract Cancer. Cancers 2022, 14, 5379. [Google Scholar] [CrossRef]
- Zhang, H.; Yang, T.; Wu, M.; Shen, F. Intrahepatic cholangiocarcinoma: Epidemiology, risk factors, diagnosis and surgical management. Cancer Lett. 2016, 379, 198–205. [Google Scholar] [CrossRef]
- Wu, L.; Tsilimigras, D.I.; Paredes, A.Z.; Mehta, R.; Hyer, J.M.; Merath, K.; Sahara, K.; Bagante, F.; Beal, E.W.; Shen, F.; et al. Trends in the Incidence, Treatment and Outcomes of Patients with Intrahepatic Cholangiocarcinoma in the USA: Facility Type is Associated with Margin Status, Use of Lymphadenectomy and Overall Survival. World J. Surg. 2019, 43, 1777–1787. [Google Scholar] [CrossRef]
- Brindley, P.J.; Bachini, M.; Ilyas, S.I.; Khan, S.A.; Loukas, A.; Sirica, A.E.; Teh, B.T.; Wongkham, S.; Gores, G.J. Cholangiocarcinoma. Nat. Rev. Dis. Primers 2021, 7, 65. [Google Scholar] [CrossRef] [PubMed]
- Clements, O.; Eliahoo, J.; Kim, J.U.; Taylor-Robinson, S.D.; Khan, S.A. Risk factors for intrahepatic and extrahepatic cholangiocarcinoma: A systematic review and meta-analysis. J. Hepatol. 2020, 72, 95–103. [Google Scholar] [CrossRef]
- Herraez, E.; Romero, M.R.; Macias, R.I.R.; Monte, M.J.; Marin, J.J.G. Clinical relevance of the relationship between changes in gut microbiota and bile acid metabolism in patients with intrahepatic cholangiocarcinoma. Hepatobiliary Surg. Nutr. 2020, 9, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Rao, B.; Ren, T.; Wang, X.; Wang, H.; Zou, Y.; Sun, Y.; Liu, S.; Ren, Z.; Yu, Z. Dysbiosis in the Human Microbiome of Cholangiocarcinoma. Front. Physiol. 2021, 12, 715536. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Li, J.; Jin, C.; Yang, J.; Zheng, C.; Chen, K.; Xie, Y.; Yang, Y.; Bo, Z.; Wang, J.; et al. Association of gut microbiome and primary liver cancer: A two-sample Mendelian randomization and case-control study. Liver Int. 2022, 43, 221–233. [Google Scholar] [CrossRef]
- Jia, X.; Lu, S.; Zeng, Z.; Liu, Q.; Dong, Z.; Chen, Y.; Zhu, Z.; Hong, Z.; Zhang, T.; Du, G.; et al. Characterization of Gut Microbiota, Bile Acid Metabolism, and Cytokines in Intrahepatic Cholangiocarcinoma. Hepatology 2020, 71, 893–906. [Google Scholar] [CrossRef]
- Deng, T.; Li, J.; He, B.; Chen, B.; Liu, F.; Chen, Z.; Zheng, J.; Shi, Z.; Zhang, T.; Deng, L.; et al. Gut microbiome alteration as a diagnostic tool and associated with inflammatory response marker in primary liver cancer. Hepatol. Int. 2022, 16, 99–111. [Google Scholar] [CrossRef]
- Zhang, T.; Zhang, S.; Jin, C.; Lin, Z.; Deng, T.; Xie, X.; Deng, L.; Li, X.; Ma, J.; Ding, X.; et al. A Predictive Model Based on the Gut Microbiota Improves the Diagnostic Effect in Patients with Cholangiocarcinoma. Front. Cell. Infect. Microbiol. 2021, 11, 751795. [Google Scholar] [CrossRef]
- Rao, B.C.; Zhang, G.Z.; Zou, Y.W.; Ren, T.; Ren, H.Y.; Liu, C.; Yu, Z.J.; Ren, Z.G. Alterations in the human oral microbiome in cholangiocarcinoma. Mil. Med. Res. 2022, 9, 62. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Ma, C.; Duan, Y.; Heinrich, B.; Rosato, U.; Diggs, L.P.; Ma, L.; Roy, S.; Fu, Q.; Brown, Z.J.; et al. Gut Microbiome Directs Hepatocytes to Recruit MDSCs and Promote Cholangiocarcinoma. Cancer Discov. 2021, 11, 1248–1267. [Google Scholar] [CrossRef] [PubMed]
- Chai, X.; Wang, J.; Li, H.; Gao, C.; Li, S.; Wei, C.; Huang, J.; Tian, Y.; Yuan, J.; Lu, J.; et al. Intratumor microbiome features reveal antitumor potentials of intrahepatic cholangiocarcinoma. Gut Microbes 2023, 15, 2156255. [Google Scholar] [CrossRef] [PubMed]
- Chng, K.R.; Chan, S.H.; Ng, A.H.Q.; Li, C.; Jusakul, A.; Bertrand, D.; Wilm, A.; Choo, S.P.; Tan, D.M.Y.; Lim, K.H.; et al. Tissue Microbiome Profiling Identifies an Enrichment of Specific Enteric Bacteria in Opisthorchis viverrini Associated Cholangiocarcinoma. EBioMedicine 2016, 8, 195–202. [Google Scholar] [CrossRef]
- Sitthirak, S.; Suksawat, M.; Phetcharaburanin, J.; Wangwiwatsin, A.; Klanrit, P.; Namwat, N.; Khuntikeo, N.; Titapun, A.; Jarearnrat, A.; Sangkhamanon, S.; et al. Chemotherapeutic resistant cholangiocarcinoma displayed distinct intratumoral microbial composition and metabolic profiles. PeerJ 2022, 10, e13876. [Google Scholar] [CrossRef]
- Lee, H.; Lee, H.K.; Min, S.K.; Lee, W.H. 16S rDNA microbiome composition pattern analysis as a diagnostic biomarker for biliary tract cancer. World J. Surg. Oncol. 2020, 18, 19. [Google Scholar] [CrossRef]
- Bednarsch, J.; Czigany, Z.; Heij, L.R.; Luedde, T.; van Dam, R.; Lang, S.A.; Ulmer, T.F.; Hornef, M.W.; Neumann, U.P. Bacterial bile duct colonization in perihilar cholangiocarcinoma and its clinical significance. Sci. Rep. 2021, 11, 2926. [Google Scholar] [CrossRef] [PubMed]
- Di Carlo, P.; Serra, N.; D’Arpa, F.; Agrusa, A.; Gulotta, G.; Fasciana, T.; Rodolico, V.; Giammanco, A.; Sergi, C. The microbiota of the bilio-pancreatic system: A cohort, STROBE-compliant study. Infect. Drug Resist. 2019, 12, 1513–1527. [Google Scholar] [CrossRef]
- Kim, I.H.; Choi, J.K.; Lee, D.G.; Lee, I.S.; Hong, T.H.; You, Y.K.; Chun, H.J.; Lee, M.A. Clinical significance of isolated biliary candidiasis in patients with unresectable cholangiocarcinoma. Hepatobiliary Pancreat. Dis. Int. 2016, 15, 533–539. [Google Scholar] [CrossRef]
- Chen, B.; Fu, S.W.; Lu, L.; Zhao, H. A Preliminary Study of Biliary Microbiota in Patients with Bile Duct Stones or Distal Cholangiocarcinoma. Biomed. Res. Int. 2019, 2019, 1092563. [Google Scholar] [CrossRef] [PubMed]
- Saab, M.; Mestivier, D.; Sohrabi, M.; Rodriguez, C.; Khonsari, M.R.; Faraji, A.; Sobhani, I. Characterization of biliary microbiota dysbiosis in extrahepatic cholangiocarcinoma. PLoS ONE 2021, 16, e0247798. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Chu, J.; Su, F.; Ding, X.; Zhang, Y.; Dou, L.; Liu, Y.; Ke, Y.; Liu, X.; Liu, Y.; et al. Characteristics of bile microbiota in cholelithiasis, perihilar cholangiocarcinoma, distal cholangiocarcinoma, and pancreatic cancer. Am. J. Transl. Res. 2022, 14, 2962–2971. [Google Scholar]
- Dangtakot, R.; Intuyod, K.; Ahooja, A.; Wongwiwatchai, J.; Hanpanich, P.; Lulitanond, A.; Chamgramol, Y.; Pinlaor, S.; Pinlaor, P. Profiling of Bile Microbiome Identifies District Microbial Population between Choledocholithiasis and Cholangiocarcinoma Patients. Asian Pac. J. Cancer Prev. 2021, 22, 233–240. [Google Scholar] [CrossRef]
- Avilés-Jiménez, F.; Guitron, A.; Segura-López, F.; Méndez-Tenorio, A.; Iwai, S.; Hernández-Guerrero, A.; Torres, J. Microbiota studies in the bile duct strongly suggest a role for Helicobacter pylori in extrahepatic cholangiocarcinoma. Clin. Microbiol. Infect. 2016, 22, 178.e111–178.e122. [Google Scholar] [CrossRef]
- Miyabe, K.; Chandrasekhara, V.; Wongjarupong, N.; Chen, J.; Yang, L.; Johnson, S.; Chia, N.; Walther-Antonio, M.; Yao, J.Z.; Harrington, S.C.; et al. Potential Role of Inflammation-Promoting Biliary Microbiome in Primary Sclerosing Cholangitis and Cholangiocarcinoma. Cancers 2022, 14, 2120. [Google Scholar] [CrossRef] [PubMed]
- Roa, J.C.; García, P.; Kapoor, V.K.; Maithel, S.K.; Javle, M.; Koshiol, J. Gallbladder cancer. Nat. Rev. Dis. Primers 2022, 8, 69. [Google Scholar] [CrossRef] [PubMed]
- Sharma, N.; Yadav, M.; Tripathi, G.; Mathew, B.; Bindal, V.; Falari, S.; Pamecha, V.; Maras, J.S. Bile multi-omics analysis classifies lipid species and microbial peptides predictive of carcinoma of gallbladder. Hepatology 2022, 76, 920–935. [Google Scholar] [CrossRef]
- Sharma, V.; Chauhan, V.S.; Nath, G.; Kumar, A.; Shukla, V.K. Role of bile bacteria in gallbladder carcinoma. Hepatogastroenterology 2007, 54, 1622–1625. [Google Scholar]
- Nath, G.; Gulati, A.K.; Shukla, V.K. Role of bacteria in carcinogenesis, with special reference to carcinoma of the gallbladder. World J. Gastroenterol. 2010, 16, 5395–5404. [Google Scholar] [CrossRef] [PubMed]
- Tsuchiya, Y.; Loza, E.; Villa-Gomez, G.; Trujillo, C.C.; Baez, S.; Asai, T.; Ikoma, T.; Endoh, K.; Nakamura, K. Metagenomics of Microbial Communities in Gallbladder Bile from Patients with Gallbladder Cancer or Cholelithiasis. Asian Pac. J. Cancer Prev. 2018, 19, 961–967. [Google Scholar] [PubMed]
- Choi, S.J.; Kim, Y.; Jeon, J.; Gwak, H.J.; Kim, M.; Kang, K.; Kim, Y.; Jeong, J.; Jung, Y.K.; Lee, K.G.; et al. Association of Microbial Dysbiosis with Gallbladder Diseases Identified by Bile Microbiome Profiling. J. Korean Med. Sci. 2021, 36, e189. [Google Scholar] [CrossRef] [PubMed]
- Walawalkar, Y.D.; Gaind, R.; Nayak, V. Study on Salmonella Typhi occurrence in gallbladder of patients suffering from chronic cholelithiasis-a predisposing factor for carcinoma of gallbladder. Diagn. Microbiol. Infect. Dis. 2013, 77, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Koshiol, J.; Wozniak, A.; Cook, P.; Adaniel, C.; Acevedo, J.; Azócar, L.; Hsing, A.W.; Roa, J.C.; Pasetti, M.F.; Miquel, J.F.; et al. Salmonella enterica serovar Typhi and gallbladder cancer: A case-control study and meta-analysis. Cancer Med. 2016, 5, 3310–3235. [Google Scholar] [CrossRef]
- Nagaraja, V.; Eslick, G.D. Systematic review with meta-analysis: The relationship between chronic Salmonella typhi carrier status and gall-bladder cancer. Aliment. Pharmacol. Ther. 2014, 39, 745–750. [Google Scholar] [CrossRef] [PubMed]
- Scanu, T.; Spaapen, R.M.; Bakker, J.M.; Pratap, C.B.; Wu, L.E.; Hofland, I.; Broeks, A.; Shukla, V.K.; Kumar, M.; Janssen, H.; et al. Salmonella Manipulation of Host Signaling Pathways Provokes Cellular Transformation Associated with Gallbladder Carcinoma. Cell Host Microbe 2015, 17, 763–774. [Google Scholar] [CrossRef]
- Zhou, D.; Wang, J.D.; Weng, M.Z.; Zhang, Y.; Wang, X.F.; Gong, W.; Quan, Z.W. Infections of Helicobacter spp. in the biliary system are associated with biliary tract cancer: A meta-analysis. Eur. J. Gastroenterol. Hepatol. 2013, 25, 447–454. [Google Scholar] [CrossRef]
- Murphy, G.; Michel, A.; Taylor, P.R.; Albanes, D.; Weinstein, S.J.; Virtamo, J.; Parisi, D.; Snyder, K.; Butt, J.; McGlynn, K.A.; et al. Association of seropositivity to Helicobacter species and biliary tract cancer in the ATBC study. Hepatology 2014, 60, 1963–1971. [Google Scholar] [CrossRef]
- Takayama, S.; Takahashi, H.; Matsuo, Y.; Okada, Y.; Takeyama, H. Effect of Helicobacter bilis infection on human bile duct cancer cells. Dig. Dis. Sci. 2010, 55, 1905–1910. [Google Scholar] [CrossRef]
- Song, X.; Wang, X.; Hu, Y.; Li, H.; Ren, T.; Li, Y.; Liu, L.; Li, L.; Li, X.; Wang, Z.; et al. A metagenomic study of biliary microbiome change along the cholecystitis-carcinoma sequence. Clin. Transl. Med. 2020, 10, e97. [Google Scholar] [CrossRef]
- Kirishima, M.; Yokoyama, S.; Matsuo, K.; Hamada, T.; Shimokawa, M.; Akahane, T.; Sugimoto, T.; Tsurumaru, H.; Ishibashi, M.; Mataki, Y.; et al. Gallbladder microbiota composition is associated with pancreaticobiliary and gallbladder cancer prognosis. BMC Microbiol. 2022, 22, 147. [Google Scholar] [CrossRef]
- Pomyen, Y.; Chaisaingmongkol, J.; Rabibhadana, S.; Pupacdi, B.; Sripan, D.; Chornkrathok, C.; Budhu, A.; Budhisawasdi, V.; Lertprasertsuke, N.; Chotirosniramit, A.; et al. Gut dysbiosis in Thai intrahepatic cholangiocarcinoma and hepatocellular carcinoma. Sci. Rep. 2023, 13, 11406. [Google Scholar] [CrossRef] [PubMed]
- Chagani, S.; Kwong, L.N. Cholangiocarcinoma Risk Factors Open the Floodgates for Gut Microbes and Immunosuppressive Myeloid Cells. Cancer Discov. 2021, 11, 1014–1015. [Google Scholar] [CrossRef]
- Dyson, J.K.; Beuers, U.; Jones, D.E.J.; Lohse, A.W.; Hudson, M. Primary sclerosing cholangitis. Lancet 2018, 391, 2547–2559. [Google Scholar] [CrossRef] [PubMed]
- Horsley-Silva, J.L.; Carey, E.J.; Lindor, K.D. Advances in primary sclerosing cholangitis. Lancet Gastroenterol. Hepatol. 2016, 1, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Özdirik, B.; Müller, T.; Wree, A.; Tacke, F.; Sigal, M. The Role of Microbiota in Primary Sclerosing Cholangitis and Related Biliary Malignancies. Int. J. Mol. Sci. 2021, 22, 6975. [Google Scholar] [CrossRef] [PubMed]
- Little, R.; Wine, E.; Kamath, B.M.; Griffiths, A.M.; Ricciuto, A. Gut microbiome in primary sclerosing cholangitis: A review. World J. Gastroenterol. 2020, 26, 2768–2780. [Google Scholar] [CrossRef]
- Liwinski, T.; Zenouzi, R.; John, C.; Ehlken, H.; Ruhlemann, M.C.; Bang, C.; Groth, S.; Lieb, W.; Kantowski, M.; Andersen, N.; et al. Alterations of the bile microbiome in primary sclerosing cholangitis. Gut 2020, 69, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Grigor’eva, I.N.; Romanova, T.I. Gallstone Disease and Microbiome. Microorganisms 2020, 8, 835. [Google Scholar] [CrossRef]
- Fremont-Rahl, J.J.; Ge, Z.; Umana, C.; Whary, M.T.; Taylor, N.S.; Muthupalani, S.; Carey, M.C.; Fox, J.G.; Maurer, K.J. An analysis of the role of the indigenous microbiota in cholesterol gallstone pathogenesis. PLoS ONE 2013, 8, e70657. [Google Scholar] [CrossRef]
- Wang, H.H.; Portincasa, P.; Afdhal, N.H.; Wang, D.Q. Lith genes and genetic analysis of cholesterol gallstone formation. Gastroenterol. Clin. N. Am. 2010, 39, 185–207. [Google Scholar] [CrossRef]
- Xu, M.Y.; Ma, J.H.; Yuan, B.S.; Yin, J.; Liu, L.; Lu, Q.B. Association between Helicobacter pylori infection and gallbladder diseases: A retrospective study. J. Gastroenterol. Hepatol. 2018, 33, 1207–1212. [Google Scholar] [CrossRef]
- Fatemi, S.M.; Doosti, A.; Shokri, D.; Ghorbani-Dalini, S.; Molazadeh, M.; Tavakoli, H.; Minakari, M.; Tavakkoli, H. Is There a Correlation between Helicobacter Pylori and Enterohepatic Helicobacter Species and Gallstone Cholecystitis? Middle East J. Dig. Dis. 2018, 10, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Urdaneta, V.; Casadesús, J. Interactions between Bacteria and Bile Salts in the Gastrointestinal and Hepatobiliary Tracts. Front. Med. 2017, 4, 163. [Google Scholar] [CrossRef]
- Routy, B.; Le Chatelier, E.; Derosa, L.; Duong, C.P.M.; Alou, M.T.; Daillère, R.; Fluckiger, A.; Messaoudene, M.; Rauber, C.; Roberti, M.P.; et al. Gut microbiome influences efficacy of PD-1-based immunotherapy against epithelial tumors. Science 2018, 359, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Sivan, A.; Corrales, L.; Hubert, N.; Williams, J.B.; Aquino-Michaels, K.; Earley, Z.M.; Benyamin, F.W.; Lei, Y.M.; Jabri, B.; Alegre, M.L.; et al. Commensal Bifidobacterium promotes antitumor immunity and facilitates anti-PD-L1 efficacy. Science 2015, 350, 1084–1089. [Google Scholar] [CrossRef] [PubMed]
- Trifylli, E.M.; Koustas, E.; Papadopoulos, N.; Sarantis, P.; Aloizos, G.; Damaskos, C.; Garmpis, N.; Garmpi, A.; Karamouzis, M.V. An Insight into the Novel Immunotherapy and Targeted Therapeutic Strategies for Hepatocellular Carcinoma and Cholangiocarcinoma. Life 2022, 12, 665. [Google Scholar] [CrossRef]
- Helmink, B.A.; Khan, M.A.W.; Hermann, A.; Gopalakrishnan, V.; Wargo, J.A. The microbiome, cancer, and cancer therapy. Nat. Med. 2019, 25, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Silveira, M.A.D.; Bilodeau, S.; Greten, T.F.; Wang, X.W.; Trinchieri, G. The gut-liver axis: Host microbiota interactions shape hepatocarcinogenesis. Trends Cancer 2022, 8, 583–597. [Google Scholar] [CrossRef]
- Koustas, E.; Sarantis, P.; Papavassiliou, A.G.; Karamouzis, M.V. The Resistance Mechanisms of Checkpoint Inhibitors in Solid Tumors. Biomolecules 2020, 10, 666. [Google Scholar] [CrossRef]
- Piha-Paul, S.A.; Oh, D.Y.; Ueno, M.; Malka, D.; Chung, H.C.; Nagrial, A.; Kelley, R.K.; Ros, W.; Italiano, A.; Nakagawa, K.; et al. Efficacy and safety of pembrolizumab for the treatment of advanced biliary cancer: Results from the KEYNOTE-158 and KEYNOTE-028 studies. Int. J. Cancer 2020, 147, 2190–2198. [Google Scholar] [CrossRef]
- Liao, W.; Overman, M.J.; Boutin, A.T.; Shang, X.; Zhao, D.; Dey, P.; Li, J.; Wang, G.; Lan, Z.; Li, J.; et al. KRAS-IRF2 Axis Drives Immune Suppression and Immune Therapy Resistance in Colorectal Cancer. Cancer Cell 2019, 35, 559–572. [Google Scholar] [CrossRef] [PubMed]
- Highfill, S.L.; Cui, Y.; Giles, A.J.; Smith, J.P.; Zhang, H.; Morse, E.; Kaplan, R.N.; Mackall, C.L. Disruption of CXCR2-mediated MDSC tumor trafficking enhances anti-PD1 efficacy. Sci. Transl. Med. 2014, 6, 237ra267. [Google Scholar] [CrossRef] [PubMed]
- Mao, J.; Wang, D.; Long, J.; Yang, X.; Lin, J.; Song, Y.; Xie, F.; Xun, Z.; Wang, Y.; Wang, Y.; et al. Gut microbiome is associated with the clinical response to anti-PD-1 based immunotherapy in hepatobiliary cancers. J. Immunother. Cancer 2021, 9, e003334. [Google Scholar] [CrossRef] [PubMed]
- Elvevi, A.; Laffusa, A.; Gallo, C.; Invernizzi, P.; Massironi, S. Any Role for Microbiota in Cholangiocarcinoma? A Comprehensive Review. Cells 2023, 12, 370. [Google Scholar] [CrossRef]
- Beyoğlu, D.; Idle, J.R. The metabolomic window into hepatobiliary disease. J. Hepatol. 2013, 59, 842–858. [Google Scholar] [CrossRef]
- Miolo, G.; Muraro, E.; Caruso, D.; Crivellari, D.; Ash, A.; Scalone, S.; Lombardi, D.; Rizzolio, F.; Giordano, A.; Corona, G. Pharmacometabolomics study identifies circulating spermidine and tryptophan as potential biomarkers associated with the complete pathological response to trastuzumab-paclitaxel neoadjuvant therapy in HER-2 positive breast cancer. Oncotarget 2016, 7, 39809–39822. [Google Scholar] [CrossRef] [PubMed]
- Jia, W.; Xie, G.; Jia, W. Bile acid-microbiota crosstalk in gastrointestinal inflammation and carcinogenesis. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 111–128. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, A.; Debelius, J.; Brenner, D.A.; Karin, M.; Loomba, R.; Schnabl, B.; Knight, R. The gut-liver axis and the intersection with the microbiome. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 397–411. [Google Scholar] [CrossRef]
- Murakami, Y.; Kubo, S.; Tamori, A.; Itami, S.; Kawamura, E.; Iwaisako, K.; Ikeda, K.; Kawada, N.; Ochiya, T.; Taguchi, Y.H. Comprehensive analysis of transcriptome and metabolome analysis in Intrahepatic Cholangiocarcinoma and Hepatocellular Carcinoma. Sci. Rep. 2015, 5, 16294. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Yang, Z.; Shi, Z.; Zhu, Z.; Li, C.; Du, Z.; Zhang, Y.; Wang, Z.; Jiao, Z.; Tian, X.; et al. Analysis of bile acid profile in plasma to differentiate cholangiocarcinoma from benign biliary diseases and healthy controls. J. Steroid Biochem. Mol. Biol. 2021, 205, 105775. [Google Scholar] [CrossRef]
- Banales, J.M.; Iñarrairaegui, M.; Arbelaiz, A.; Milkiewicz, P.; Muntané, J.; Muñoz-Bellvis, L.; La Casta, A.; Gonzalez, L.M.; Arretxe, E.; Alonso, C.; et al. Serum Metabolites as Diagnostic Biomarkers for Cholangiocarcinoma, Hepatocellular Carcinoma, and Primary Sclerosing Cholangitis. Hepatology 2019, 70, 547–562. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Zhao, R.; Zhou, X.; Liang, X.; Campbell, D.J.; Zhang, X.; Zhang, L.; Shi, R.; Wang, G.; Pandak, W.M.; et al. Conjugated bile acids promote cholangiocarcinoma cell invasive growth through activation of sphingosine 1-phosphate receptor 2. Hepatology 2014, 60, 908–918. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Lu, J.; Lv, S.; Sun, S.; Liu, C.; Xu, F.; Sun, H.; Yang, J.; Wang, X.; Zhong, X.; et al. Linoleic acid pathway disturbance contributing to potential cancerization of intrahepatic bile duct stones into intrahepatic cholangiocarcinoma. BMC Gastroenterol. 2022, 22, 269. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Association between the human microbiome, metabolites and biliary tract cancer.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ye, C.; Dong, C.; Lin, Y.; Shi, H.; Zhou, W. Interplay between the Human Microbiome and Biliary Tract Cancer: Implications for Pathogenesis and Therapy. Microorganisms 2023, 11, 2598. https://doi.org/10.3390/microorganisms11102598
AMA Style
Ye C, Dong C, Lin Y, Shi H, Zhou W. Interplay between the Human Microbiome and Biliary Tract Cancer: Implications for Pathogenesis and Therapy. Microorganisms. 2023; 11(10):2598. https://doi.org/10.3390/microorganisms11102598
Chicago/Turabian StyleYe, Cheng, Chunlu Dong, Yanyan Lin, Huaqing Shi, and Wence Zhou. 2023. "Interplay between the Human Microbiome and Biliary Tract Cancer: Implications for Pathogenesis and Therapy" Microorganisms 11, no. 10: 2598. https://doi.org/10.3390/microorganisms11102598
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.