
Understanding and Implementing Diagnostic Stewardship: A Guide for Resident Physicians in the Era of Antimicrobial Resistance

Abstract
:1. Introduction
2. Overview of Diagnostic Stewardship
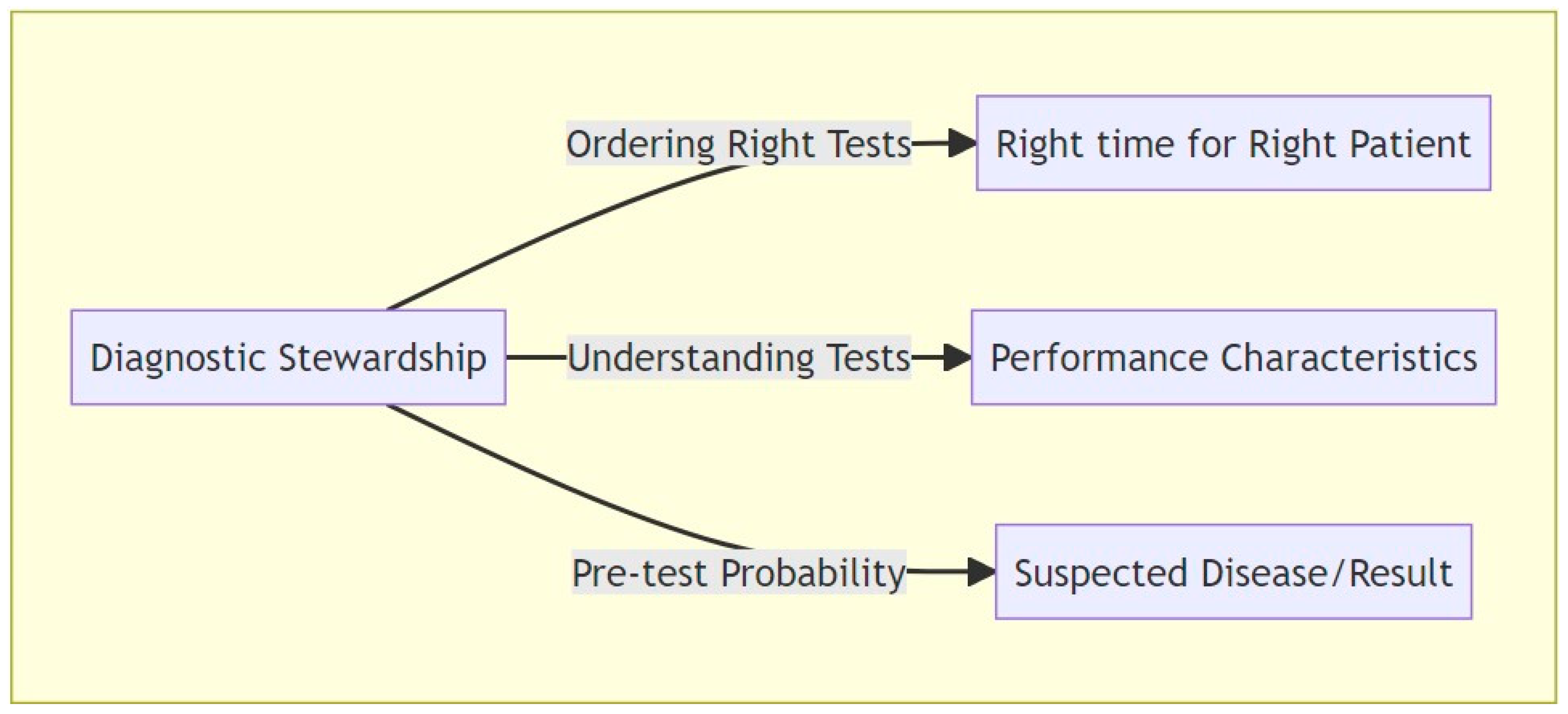
2.1. Understanding the Concept
2.2. Navigating Ambiguities
3. DS Applications
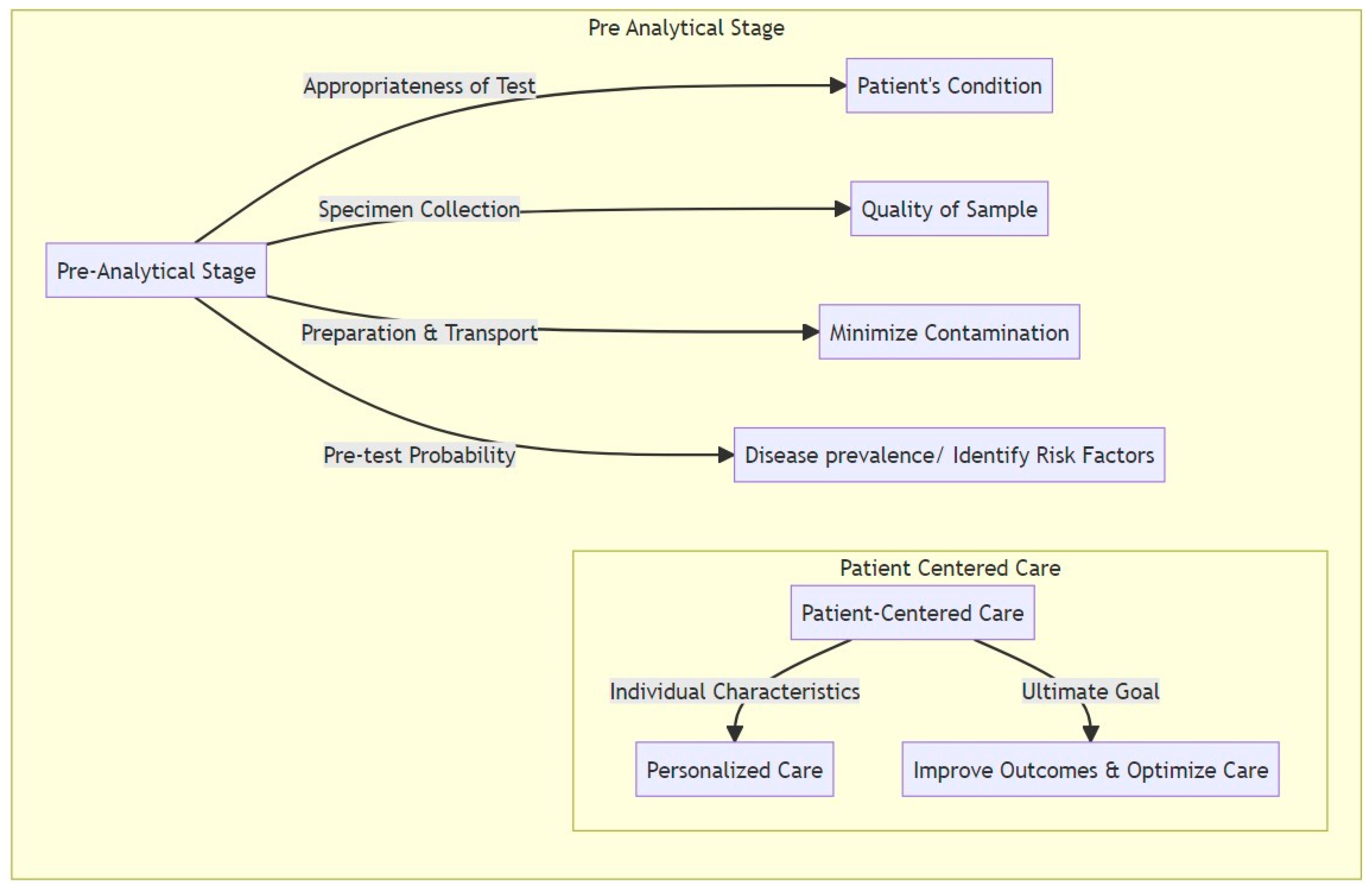
3.1. Pre-Analytical Domain
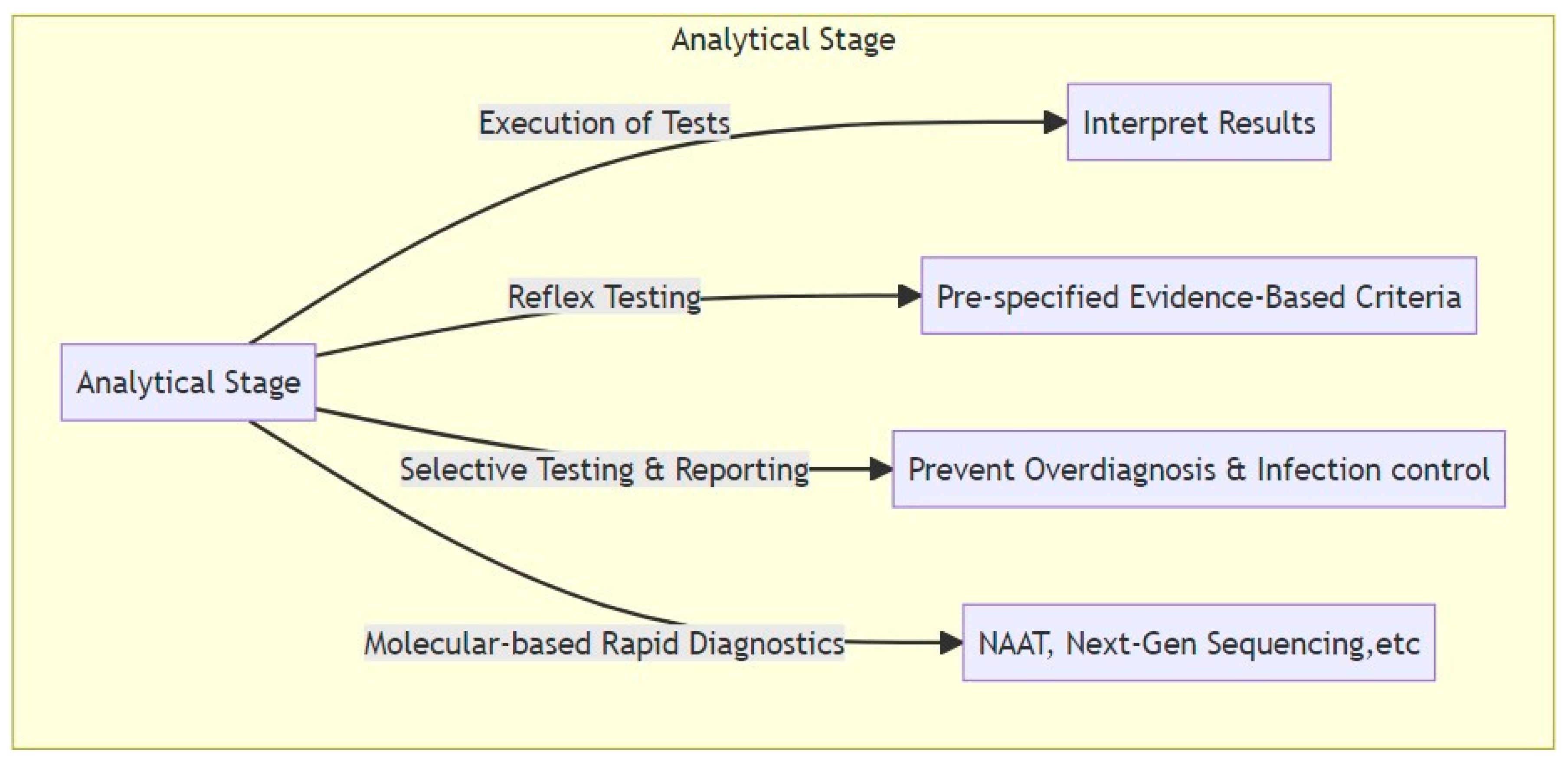
3.2. Analytical Domain
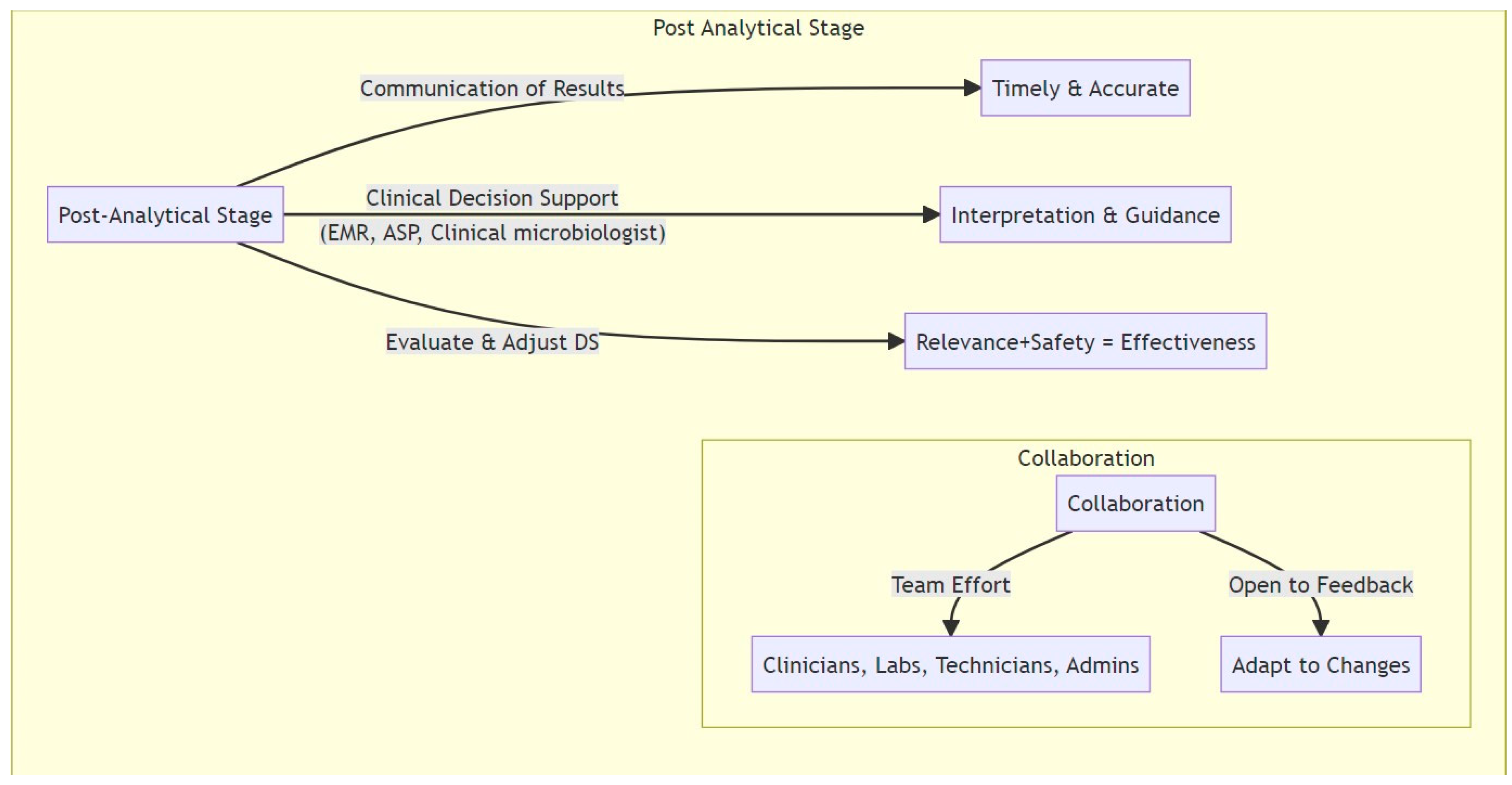
3.3. Post-Analytical Domain
4. Perspectives and Future Directions
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dadgostar, P.J.I.; Resistance, D. Antimicrobial Resistance: Implications and Costs. Infect. Drug Resist. 2019, 12, 3903–3910. [Google Scholar] [CrossRef]
- Patel, J.; Sridhar, D. The pandemic legacy of antimicrobial resistance in the USA. Lancet Microbe 2022, 3, e726–e727. [Google Scholar] [CrossRef] [PubMed]
- Tanne, J.H. COVID-19: Antimicrobial resistance rose dangerously in US during pandemic, CDC says. BMJ 2022, 378, o1755. [Google Scholar] [CrossRef]
- Majumder, A.A.; Rahman, S.; Cohall, D.; Bharatha, A.; Singh, K.; Haque, M.; Hilaire, M.G.-S. Antimicrobial Stewardship: Fighting Antimicrobial Resistance and Protecting Global Public Health. Infect. Drug Resist. 2020, 13, 4713–4738. [Google Scholar] [CrossRef] [PubMed]
- Morgan, D.J.; Malani, P.; Diekema, D.J. Diagnostic Stewardship-Leveraging the Laboratory to Improve Antimicrobial Use. JAMA 2017, 318, 607–608. [Google Scholar] [CrossRef] [PubMed]
- Curren, E.J.; Lutgring, J.D.; Kabbani, S.; Diekema, D.J.; Gitterman, S.; Lautenbach, E.; Morgan, D.J.; Rock, C.; Salerno, R.M.; McDonald, L.C. Advancing Diagnostic Stewardship for Healthcare-Associated Infections, Antibiotic Resistance, and Sepsis. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2022, 74, 723–728. [Google Scholar] [CrossRef]
- Mrazek, C.; Simundic, A.-M.; Salinas, M.; von Meyer, A.; Cornes, M.; Bauçà, J.M.; Nybo, M.; Lippi, G.; Haschke-Becher, E.; Keppel, M.H.; et al. Inappropriate use of laboratory tests: How availability triggers demand—Examples across Europe. Clin. Chim. Acta 2020, 505, 100–107. [Google Scholar] [CrossRef]
- Koch, C.; Roberts, K.; Petruccelli, C.; Morgan, D.J. The Frequency of Unnecessary Testing in Hospitalized Patients. Am. J. Med. 2018, 131, 500–503. [Google Scholar] [CrossRef]
- Zakhour, J.; Haddad, S.F.; Kerbage, A.; Wertheim, H.; Tattevin, P.; Voss, A.; Ünal, S.; Ouedraogo, A.S.; Kanj, S.S. Diagnostic stewardship in infectious diseases: A continuum of antimicrobial stewardship in the fight against antimicrobial resistance. Int. J. Antimicrob. Agents 2023, 62, 106816. [Google Scholar] [CrossRef] [PubMed]
- Morjaria, S.; Chapin, K.C. Who to Test, When, and for What: Why Diagnostic Stewardship in Infectious Diseases Matters. J. Mol. Diagn. 2020, 22, 1109–1113. [Google Scholar] [CrossRef]
- Fabre, V.; Davis, A.; Diekema, D.J.; Granwehr, B.; Hayden, M.K.; Lowe, C.F.; Pfeiffer, C.D.; Sick-Samuels, A.C.; Sullivan, K.V.; Van Schooneveld, T.C.; et al. Principles of diagnostic stewardship: A practical guide from the Society for Healthcare Epidemiology of America Diagnostic Stewardship Task Force. Infect. Control. Hosp. Epidemiol. 2023, 44, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Voogt, J.J.; van Rensen, E.L.J.; van der Schaaf, M.F.; Noordegraaf, M.; Schneider, M.M.E. Building bridges: Engaging medical residents in quality improvement and medical leadership. Int. J. Qual. Health Care 2016, 28, 665–674. [Google Scholar] [CrossRef] [PubMed]
- Messacar, K.; Parker, S.K.; Todd, J.K.; Dominguez, S.R. Implementation of Rapid Molecular Infectious Disease Diagnostics: The Role of Diagnostic and Antimicrobial Stewardship. J. Clin. Microbiol. 2017, 55, 715–723. [Google Scholar] [CrossRef]
- Morgan, D.J.; Malani, P.N.; Diekema, D.J. Diagnostic Stewardship to Prevent Diagnostic Error. JAMA 2023, 329, 1255–1256. [Google Scholar] [CrossRef]
- Tamma, P.D.; Avdic, E.; Li, D.X.; Dzintars, K.; Cosgrove, S.E. Association of Adverse Events With Antibiotic Use in Hospitalized Patients. JAMA Intern. Med. 2017, 177, 1308–1315. [Google Scholar] [CrossRef]
- van den Bosch, C.M.; Hulscher, M.E.; Akkermans, R.P.; Wille, J.; Geerlings, S.E.; Prins, J.M. Appropriate antibiotic use reduces length of hospital stay. J. Antimicrob. Chemother. 2017, 72, 923–932. [Google Scholar] [CrossRef] [PubMed]
- Morgan, D.J.; Brownlee, S.; Leppin, A.L.; Kressin, N.; Dhruva, S.S.; Levin, L.; Landon, B.E.; Zezza, M.A.; Schmidt, H.; Saini, V.; et al. Setting a research agenda for medical overuse. BMJ 2015, 351, h4534. [Google Scholar] [CrossRef] [PubMed]
- McGlynn, E.A.; McDonald, K.M.; Cassel, C.K. Measurement Is Essential for Improving Diagnosis and Reducing Diagnostic Error: A Report From the Institute of Medicine. JAMA 2015, 314, 2501–2502. [Google Scholar] [CrossRef] [PubMed]
- Morgan, D.J.; Pineles, L.; Owczarzak, J.; Magder, L.; Scherer, L.; Brown, J.P.; Pfeiffer, C.; Terndrup, C.; Leykum, L.; Feldstein, D.; et al. Accuracy of Practitioner Estimates of Probability of Diagnosis Before and After Testing. JAMA Intern. Med. 2021, 181, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Korenstein, D.; Scherer, L.D.; Foy, A.; Pineles, L.; Lydecker, A.D.; Owczarzak, J.; Magder, L.; Brown, J.P.; Pfeiffer, C.D.; Terndrup, C.; et al. Clinician Attitudes and Beliefs Associated with More Aggressive Diagnostic Testing. Am. J. Med. 2022, 135, e182–e193. [Google Scholar] [CrossRef] [PubMed]
- Hueth, K.D.; Prinzi, A.M.; Timbrook, T.T. Diagnostic Stewardship as a Team Sport: Interdisciplinary Perspectives on Improved Implementation of Interventions and Effect Measurement. Antibiotics 2022, 11, 250. [Google Scholar] [CrossRef]
- Dyar, O.J.; Moran-Gilad, J.; Greub, G.; Pulcini, C. Diagnostic stewardship: Are we using the right term? Clin. Microbiol. Infect. 2019, 25, 272–273. [Google Scholar] [CrossRef]
- Freedman, D.B. Towards Better Test Utilization—Strategies to Improve Physician Ordering and Their Impact on Patient Outcomes. Ejifcc 2015, 26, 15–30. [Google Scholar]
- Ancker, J.S.; Edwards, A.; Nosal, S.; Hauser, D.; Mauer, E.; Kaushal, R. Effects of workload, work complexity, and repeated alerts on alert fatigue in a clinical decision support system. BMC Med. Inform. Decis. Mak. 2017, 17, 36. [Google Scholar] [CrossRef] [PubMed]
- Barry, C.; Kaufman, S.; Feinstein, D.; Kim, N.; Gandhi, S.; Nikolic, D.; Edmonston, T.B.; Bierl, C. Optimization of the Order Menu in the Electronic Health Record Facilitates Test Patterns Consistent With Recommendations in the Choosing Wisely Initiative. Am. J. Clin. Pathol. 2020, 153, 94–98. [Google Scholar] [CrossRef]
- Baron, E.J.; Miller, J.M.; Weinstein, M.P.; Richter, S.S.; Gilligan, P.H.; Thomson, R.B., Jr.; Bourbeau, P.; Carroll, K.C.; Kehl, S.C.; Dunne, W.M.; et al. A Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2013 Recommendations by the Infectious Diseases Society of America (IDSA) and the American Society for Microbiology (ASM)a. Clin. Infect. Dis. 2013, 57, e22–e121. [Google Scholar] [CrossRef] [PubMed]
- Debast, S.B.; Bauer, M.P.; Kuijper, E.J. European Society of Clinical Microbiology and Infectious Diseases: Update of the treatment guidance document for Clostridium difficile infection. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2014, 20 (Suppl. 2), 1–26. [Google Scholar] [CrossRef]
- Bertolino, L.; Patauner, F.; Gagliardi, M.; D’Amico, F.; Crivaro, V.; Bernardo, M.; Scherillo, I.; Bellitti, F.; Cusano, C.; Greco, R.; et al. Diagnostic and infection control strategies for Clostridioides difficile infections in a setting of high antimicrobial resistance prevalence. Le Infez. Med. 2021, 29, 70–78. [Google Scholar]
- Sullivan, K.V. Diagnostic Stewardship in Clinical Microbiology, Essential Partner to Antimicrobial Stewardship. Clin. Chem. 2021, 68, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Brose, S.F.; Binder, K.; Fischer, M.R.; Reincke, M.; Braun, L.T.; Schmidmaier, R. Bayesian versus diagnostic information in physician-patient communication: Effects of direction of statistical information and presentation of visualization. PLoS ONE 2023, 18, e0283947. [Google Scholar] [CrossRef]
- Parikh, R.; Mathai, A.; Parikh, S.; Chandra Sekhar, G.; Thomas, R. Understanding and using sensitivity, specificity and predictive values. Indian J. Ophthalmol. 2008, 56, 45–50. [Google Scholar] [CrossRef]
- Benson, S.; Schmidt, K.; Kleine-Borgmann, J.; Herbstreit, S.; Schedlowski, M.; Hollinderbäumer, A. Can positive expectations help to improve the learning of risk literacy? A cluster-randomized study in undergraduate medical students. BMC Med. Educ. 2022, 22, 416. [Google Scholar] [CrossRef] [PubMed]
- Kayalp, D.; Dogan, K.; Ceylan, G.; Senes, M.; Yucel, D. Can routine automated urinalysis reduce culture requests? Clin. Biochem. 2013, 46, 1285–1289. [Google Scholar] [CrossRef]
- Lee, A.L.H.; Leung, E.C.M.; Lee, M.K.P.; Lai, R.W.M. Diagnostic stewardship programme for urine culture: Impact on antimicrobial prescription in a multi-centre cohort. J. Hosp. Infect. 2021, 108, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Langford, B.J.; Leung, E.; Haj, R.; McIntyre, M.; Taggart, L.R.; Brown, K.A.; Downing, M.; Matukas, L.M. Nudging In MicroBiology Laboratory Evaluation (NIMBLE): A scoping review. Infect. Control. Hosp. Epidemiol. 2019, 40, 1400–1406. [Google Scholar] [CrossRef] [PubMed]
- Tebano, G.; Mouelhi, Y.; Zanichelli, V.; Charmillon, A.; Fougnot, S.; Lozniewski, A.; Thilly, N.; Pulcini, C. Selective reporting of antibiotic susceptibility testing results: A promising antibiotic stewardship tool. Expert Rev. Anti-Infect. Ther. 2020, 18, 251–262. [Google Scholar] [CrossRef]
- Le Dref, G.; Simon, M.; Bocquier, A.; Fougnot, S.; Kivits, J.; Duda, A.; Pulcini, C.; Thilly, N. Selective reporting of antibiotic susceptibility testing results for urine cultures: Feasibility and acceptability by general practitioners and laboratory professionals in France. JAC-Antimicrob. Resist. 2023, 5, dlad013. [Google Scholar] [CrossRef]
- Coupat, C.; Pradier, C.; Degand, N.; Hofliger, P.; Pulcini, C. Selective reporting of antibiotic susceptibility data improves the appropriateness of intended antibiotic prescriptions in urinary tract infections: A case-vignette randomised study. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 32, 627–636. [Google Scholar] [CrossRef]
- Johnson, L.S.; Patel, D.; King, E.A.; Maslow, J.N. Impact of microbiology cascade reporting on antibiotic de-escalation in cefazolin-susceptible Gram-negative bacteremia. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 1151–1157. [Google Scholar] [CrossRef]
- Han, J.H.; Nachamkin, I.; Coffin, S.E.; Gerber, J.S.; Fuchs, B.; Garrigan, C.; Han, X.; Bilker, W.B.; Wise, J.; Tolomeo, P.; et al. Use of a Combination Biomarker Algorithm To Identify Medical Intensive Care Unit Patients with Suspected Sepsis at Very Low Likelihood of Bacterial Infection. Antimicrob. Agents Chemother. 2015, 59, 6494–6500. [Google Scholar] [CrossRef]
- Iankova, I.; Thompson-Leduc, P.; Kirson, N.Y.; Rice, B.; Hey, J.; Krause, A.; Schonfeld, S.A.; DeBrase, C.R.; Bozzette, S.; Schuetz, P. Efficacy and Safety of Procalcitonin Guidance in Patients With Suspected or Confirmed Sepsis: A Systematic Review and Meta-Analysis. Crit. Care Med. 2018, 46, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Apisarnthanarak, A.; Bin Kim, H.; Moore, L.S.P.; Xiao, Y.; Singh, S.; Doi, Y.; Kwa, A.L.-H.; Ponnampalavanar, S.S.L.S.; Cao, Q.; Kim, S.-W.; et al. Utility and Applicability of Rapid Diagnostic Testing in Antimicrobial Stewardship in the Asia-Pacific Region: A Delphi Consensus. Clin. Infect. Dis. 2022, 74, 2067–2076. [Google Scholar] [CrossRef]
- Hogan, C.A.; Yang, S.; Garner, O.B.; Green, D.A.; Gomez, C.A.; Dien Bard, J.; Pinsky, B.A.; Banaei, N. Clinical Impact of Metagenomic Next-Generation Sequencing of Plasma Cell-Free DNA for the Diagnosis of Infectious Diseases: A Multicenter Retrospective Cohort Study. Clin. Infect. Dis. 2021, 72, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Beganovic, M.; Costello, M.; Wieczorkiewicz, S.M. Effect of Matrix-Assisted Laser Desorption Ionization-Time of Flight Mass Spectrometry (MALDI-TOF MS) Alone versus MALDI-TOF MS Combined with Real-Time Antimicrobial Stewardship Interventions on Time to Optimal Antimicrobial Therapy in Patients with Positive Blood Cultures. J. Clin. Microbiol. 2017, 55, 1437–1445. [Google Scholar] [CrossRef]
- Tiseo, G.; Arena, F.; Borre, S.; Campanile, F.; Falcone, M.; Mussini, C.; Pea, F.; Sganga, G.; Stefani, S.; Venditti, M. Diagnostic stewardship based on patient profiles: Differential approaches in acute versus chronic infectious syndromes. Expert Rev. Anti. Infect. Ther. 2021, 19, 1373–1383. [Google Scholar] [CrossRef]
- Tenderenda, A.; Łysakowska, M.; Dargiewicz, R.; Gawron-Skarbek, A. Blood Culture Contamination: A Single General Hospital Experience of 2-Year Retrospective Study. Int. J. Environ. Res. Public Health 2022, 19, 3009. [Google Scholar] [CrossRef]
- Rodrigues, C.; Siciliano, R.F.; Filho, H.C.; Charbel, C.E.; de Carvalho Sarahyba da Silva, L.; Baiardo Redaelli, M.; de Paula Rosa Passetti, A.P.; Franco, M.R.G.; Rossi, F.; Zeigler, R.; et al. The effect of a rapid molecular blood test on the use of antibiotics for nosocomial sepsis: A randomized clinical trial. J. Intensive Care 2019, 7, 37. [Google Scholar] [CrossRef] [PubMed]
- Osthoff, M.; Gürtler, N.; Bassetti, S.; Balestra, G.; Marsch, S.; Pargger, H.; Weisser, M.; Egli, A. Impact of MALDI-TOF-MS-based identification directly from positive blood cultures on patient management: A controlled clinical trial. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2017, 23, 78–85. [Google Scholar] [CrossRef]
- Kunz Coyne Ashlan, J.; Casapao Anthony, M.; Isache, C.; Morales, J.; McCarter Yvette, S.; Jankowski Christopher, A. Influence of Antimicrobial Stewardship and Molecular Rapid Diagnostic Tests on Antimicrobial Prescribing for Extended-Spectrum Beta-Lactamase- and Carbapenemase-Producing Escherichia coli and Klebsiella pneumoniae in Bloodstream Infection. Microbiol. Spectr. 2021, 9, e00464-21. [Google Scholar] [CrossRef]
- Asker, D.; Awad, T.S.; Raju, D.; Sanchez, H.; Lacdao, I.; Gilbert, S.; Sivarajah, P.; Andes, D.R.; Sheppard, D.C.; Howell, P.L.; et al. Preventing Pseudomonas aeruginosa Biofilms on Indwelling Catheters by Surface-Bound Enzymes. ACS Appl. Bio Mater. 2021, 4, 8248–8258. [Google Scholar] [CrossRef] [PubMed]
- Cangui-Panchi, S.P.; Ñacato-Toapanta, A.L.; Enríquez-Martínez, L.J.; Reyes, J.; Garzon-Chavez, D.; Machado, A. Biofilm-forming microorganisms causing hospital-acquired infections from intravenous catheter: A systematic review. Curr. Res. Microb. Sci. 2022, 3, 100175. [Google Scholar] [CrossRef]
- Hall-Stoodley, L.; Stoodley, P.; Kathju, S.; Høiby, N.; Moser, C.; William Costerton, J.; Moter, A.; Bjarnsholt, T. Towards diagnostic guidelines for biofilm-associated infections. FEMS Immunol. Med. Microbiol. 2012, 65, 127–145. [Google Scholar] [CrossRef]
- Silva, N.B.S.; Marques, L.A.; Röder, D.D.B. Diagnosis of biofilm infections: Current methods used, challenges and perspectives for the future. J. Appl. Microbiol. 2021, 131, 2148–2160. [Google Scholar] [CrossRef] [PubMed]
- Cangui-Panchi, S.P.; Ñacato-Toapanta, A.L.; Enríquez-Martínez, L.J.; Salinas-Delgado, G.A.; Reyes, J.; Garzon-Chavez, D.; Machado, A. Battle royale: Immune response on biofilms—Host-pathogen interactions. Curr. Res. Immunol. 2023, 4, 100057. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Ye, Q.; Zhang, J.; Pang, R.; Gu, Q.; Ding, Y.; Wu, Q.; Wang, J. Multiplex PCR identification of the major Pseudomonas aeruginosa serogroups using specific novel target genes. LWT 2022, 163, 113567. [Google Scholar] [CrossRef]
- Usun Jones, S.; Kee, B.P.; Chew, C.H.; Yeo, C.C.; Abdullah, F.H.; Othman, N.; Chua, K.H.; Puah, S.M. Phenotypic and molecular detection of biofilm formation in clinical methicillin-resistant Staphylococcus aureus isolates from Malaysia. J. Taibah Univ. Sci. 2022, 16, 1142–1150. [Google Scholar] [CrossRef]
- Iorio, N.L.; Azevedo, M.B.; Frazao, V.H.; Barcellos, A.G.; Barros, E.M.; Pereira, E.M.; de Mattos, C.S.; dos Santos, K.R. Methicillin-resistant Staphylococcus epidermidis carrying biofilm formation genes: Detection of clinical isolates by multiplex PCR. Int. Microbiol. 2011, 14, 13–17. [Google Scholar] [CrossRef]
- Virkki, R.; Juven, T.; Rikalainen, H.; Svedström, E.; Mertsola, J.; Ruuskanen, O. Differentiation of bacterial and viral pneumonia in children. Thorax 2002, 57, 438–441. [Google Scholar] [CrossRef] [PubMed]
- Moffa, M.A.; Bremmer, D.N.; Carr, D.; Buchanan, C.; Shively, N.R.; Elrufay, R.; Walsh, T.L. Impact of a Multiplex Polymerase Chain Reaction Assay on the Clinical Management of Adults Undergoing a Lumbar Puncture for Suspected Community-Onset Central Nervous System Infections. Antibiotics 2020, 9, 282. [Google Scholar] [CrossRef]
- Tansarli, G.S.; Chapin, K.C. Diagnostic test accuracy of the BioFire® FilmArray® meningitis/encephalitis panel: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 281–290. [Google Scholar] [CrossRef]
- Wilson, M.R.; Sample, H.A.; Zorn, K.C.; Arevalo, S.; Yu, G.; Neuhaus, J.; Federman, S.; Stryke, D.; Briggs, B.; Langelier, C.; et al. Clinical Metagenomic Sequencing for Diagnosis of Meningitis and Encephalitis. N. Engl. J. Med. 2019, 380, 2327–2340. [Google Scholar] [CrossRef] [PubMed]
- Caulder, L.; Beardsley, J.; Palavecino, E.; Dyke, E.V.; Johnson, J.; Ohl, C.; Luther, V.; Williamson, J. 1799. Impact of Real-Time Electronic Notifications to Pharmacists of Rapid Diagnostic Blood Culture Results. Open Forum Infect. Dis. 2018, 5, S510. [Google Scholar] [CrossRef]
- Claeys, K.C.; Johnson, M.D. Leveraging diagnostic stewardship within antimicrobial stewardship programmes. Drugs Context 2023, 12, 2022-9-5. [Google Scholar] [CrossRef]
- Timbrook, T.T.; Morton, J.B.; McConeghy, K.W.; Caffrey, A.R.; Mylonakis, E.; LaPlante, K.L. The Effect of Molecular Rapid Diagnostic Testing on Clinical Outcomes in Bloodstream Infections: A Systematic Review and Meta-analysis. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2017, 64, 15–23. [Google Scholar] [CrossRef]
- Morency-Potvin, P.; Schwartz David, N.; Weinstein Robert, A. Antimicrobial Stewardship: How the Microbiology Laboratory Can Right the Ship. Clin. Microbiol. Rev. 2016, 30, 381–407. [Google Scholar] [CrossRef]
- Schartz, W.; Bennett, N.; Aragon, L.; Kennedy, K.; Boyd, S.E.; Humphrey, M.; Essmyer, C. Templated Microbiology Comments with Candiduria to Enhance Antimicrobial Stewardship. Open Forum Infect. Dis. 2021, 8, S144. [Google Scholar] [CrossRef]
- McBride, J.; Schulz, L.; Fox, B.; Dipoto, J.; Sippel, N.; Osterby, K. Influence of a “No MRSA, No Pseudomonas ” Comment to a Respiratory Culture in Antibiotic Utilization During the Treatment of Lower Respiratory Tract Infection. Open Forum Infect. Dis. 2015, 2, 1500. [Google Scholar] [CrossRef]
- Musgrove, M.A.; Kenney, R.M.; Kendall, R.E.; Peters, M.; Tibbetts, R.; Samuel, L.; Davis, S.L. Microbiology Comment Nudge Improves Pneumonia Prescribing. Open Forum Infect. Dis. 2018, 5, ofy162. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.L.; Williams, S.; Schulkin, J. Statistical literacy of obstetrics-gynecology residents. J. Grad. Med. Educ. 2013, 5, 272–275. [Google Scholar] [CrossRef]
- Gigerenzer, G.; Gaissmaier, W.; Kurz-Milcke, E.; Schwartz, L.M.; Woloshin, S. Helping Doctors and Patients Make Sense of Health Statistics. Psychol. Sci. Public Interest J. Am. Psychol. Soc. 2007, 8, 53–96. [Google Scholar] [CrossRef]
- Tiemens, B.; Wagenvoorde, R.; Witteman, C. Why Every Clinician Should Know Bayes’ Rule. Health Prof. Educ. 2020, 6, 320–324. [Google Scholar] [CrossRef]
- Jenny, M.A.; Keller, N.; Gigerenzer, G. Assessing minimal medical statistical literacy using the Quick Risk Test: A prospective observational study in Germany. BMJ Open 2018, 8, e020847. [Google Scholar] [CrossRef] [PubMed]
- Burnham, J.P.; Geng, E.; Venkatram, C.; Colditz, G.A.; McKay, V.R. Putting the Dissemination and Implementation in Infectious Diseases. Clin. Infect. Dis. 2020, 71, 218–225. [Google Scholar] [CrossRef]
- Feldstein, A.C.; Glasgow, R.E. A Practical, Robust Implementation and Sustainability Model (PRISM) for Integrating Research Findings into Practice. Jt. Comm. J. Qual. Patient Saf. 2008, 34, 228–243. [Google Scholar] [CrossRef] [PubMed]
- McCreight, M.S.; Rabin, B.A.; Glasgow, R.E.; Ayele, R.A.; Leonard, C.A.; Gilmartin, H.M.; Frank, J.W.; Hess, P.L.; Burke, R.E.; Battaglia, C.T. Using the Practical, Robust Implementation and Sustainability Model (PRISM) to qualitatively assess multilevel contextual factors to help plan, implement, evaluate, and disseminate health services programs. Transl. Behav. Med. 2019, 9, 1002–1011. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1. Understanding the Concept: |
|
|
| 2. Pre-Analytical Stage: |
|
|
|
|
| 3. Analytical Stage: |
|
|
|
|
| 4. Post-Analytical Stage: |
|
|
|
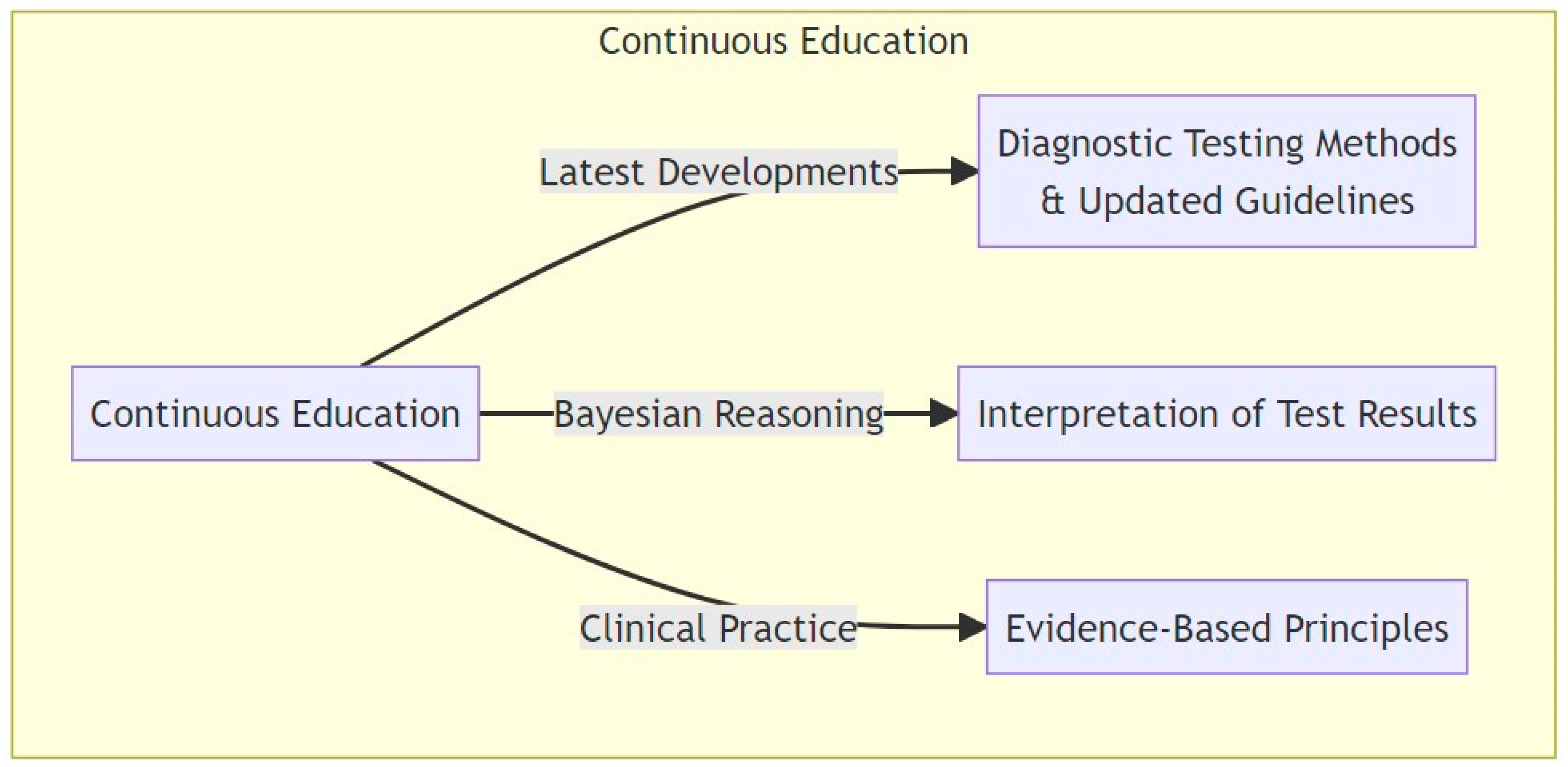
| 5. Continuous Education: |
|
|
|
| 6. Collaboration: |
|
|
| 7. Patient-Centered Care: |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schinas, G.; Dimopoulos, G.; Akinosoglou, K. Understanding and Implementing Diagnostic Stewardship: A Guide for Resident Physicians in the Era of Antimicrobial Resistance. Microorganisms 2023, 11, 2214. https://doi.org/10.3390/microorganisms11092214
Schinas G, Dimopoulos G, Akinosoglou K. Understanding and Implementing Diagnostic Stewardship: A Guide for Resident Physicians in the Era of Antimicrobial Resistance. Microorganisms. 2023; 11(9):2214. https://doi.org/10.3390/microorganisms11092214
Chicago/Turabian StyleSchinas, Georgios, George Dimopoulos, and Karolina Akinosoglou. 2023. "Understanding and Implementing Diagnostic Stewardship: A Guide for Resident Physicians in the Era of Antimicrobial Resistance" Microorganisms 11, no. 9: 2214. https://doi.org/10.3390/microorganisms11092214