
Effect of Physical Exercise Programs Based on Mobile Health and Ecological Momentary Assessment on the Physical and Mental Health, Cognitive Functions, and Social Environment of Adults in Developing Countries: A Systematic Review
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection and Eligibility Criteria
2.3. Data Extraction
2.4. Risk of Bias Assessment Tool
2.5. Strategy for Data Synthesis
3. Results
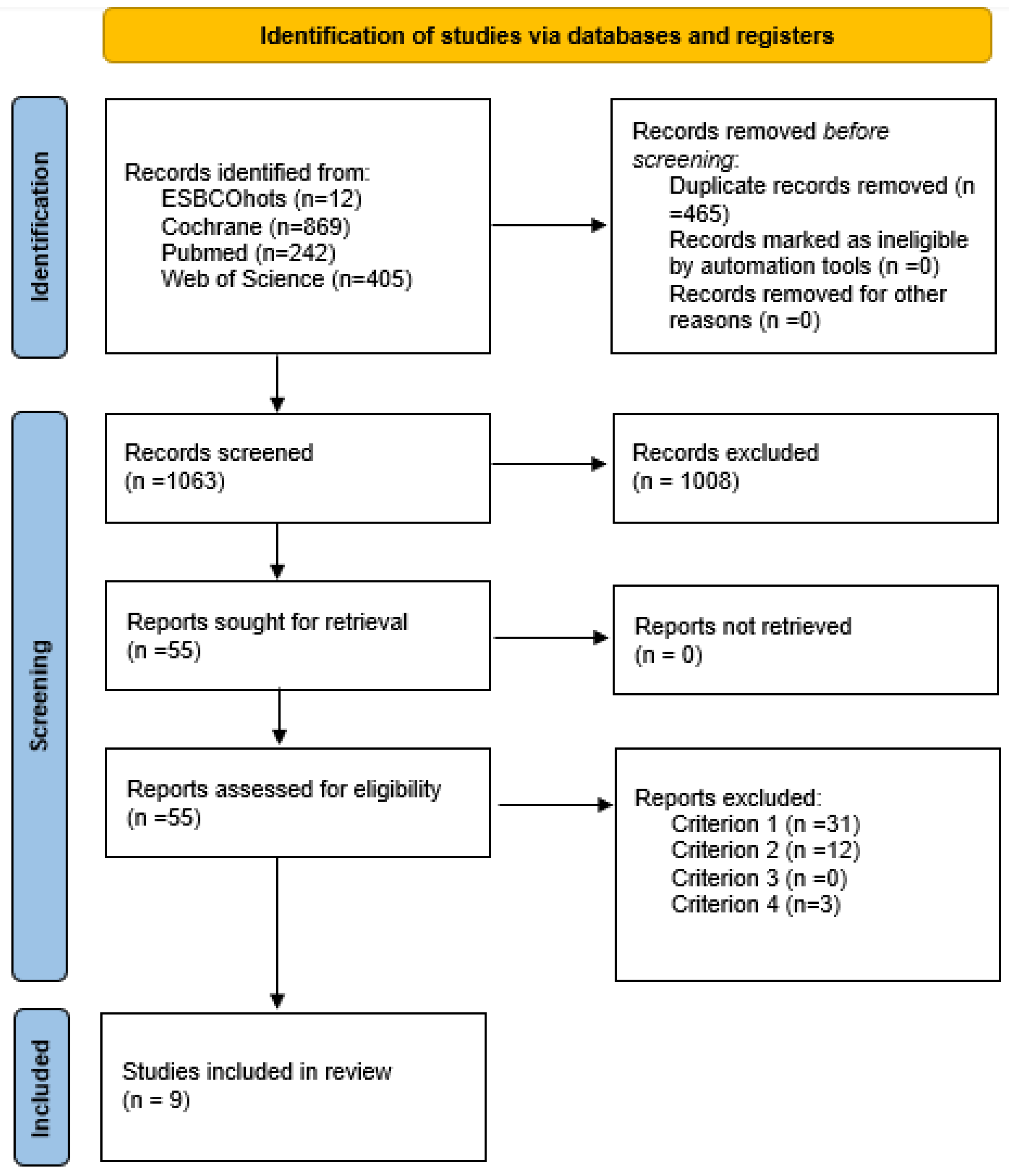
3.1. Selection of Studies
3.2. General Characteristics of the Included Studies
3.3. Characteristics of the Interventions
3.4. Study Variables and Outcomes
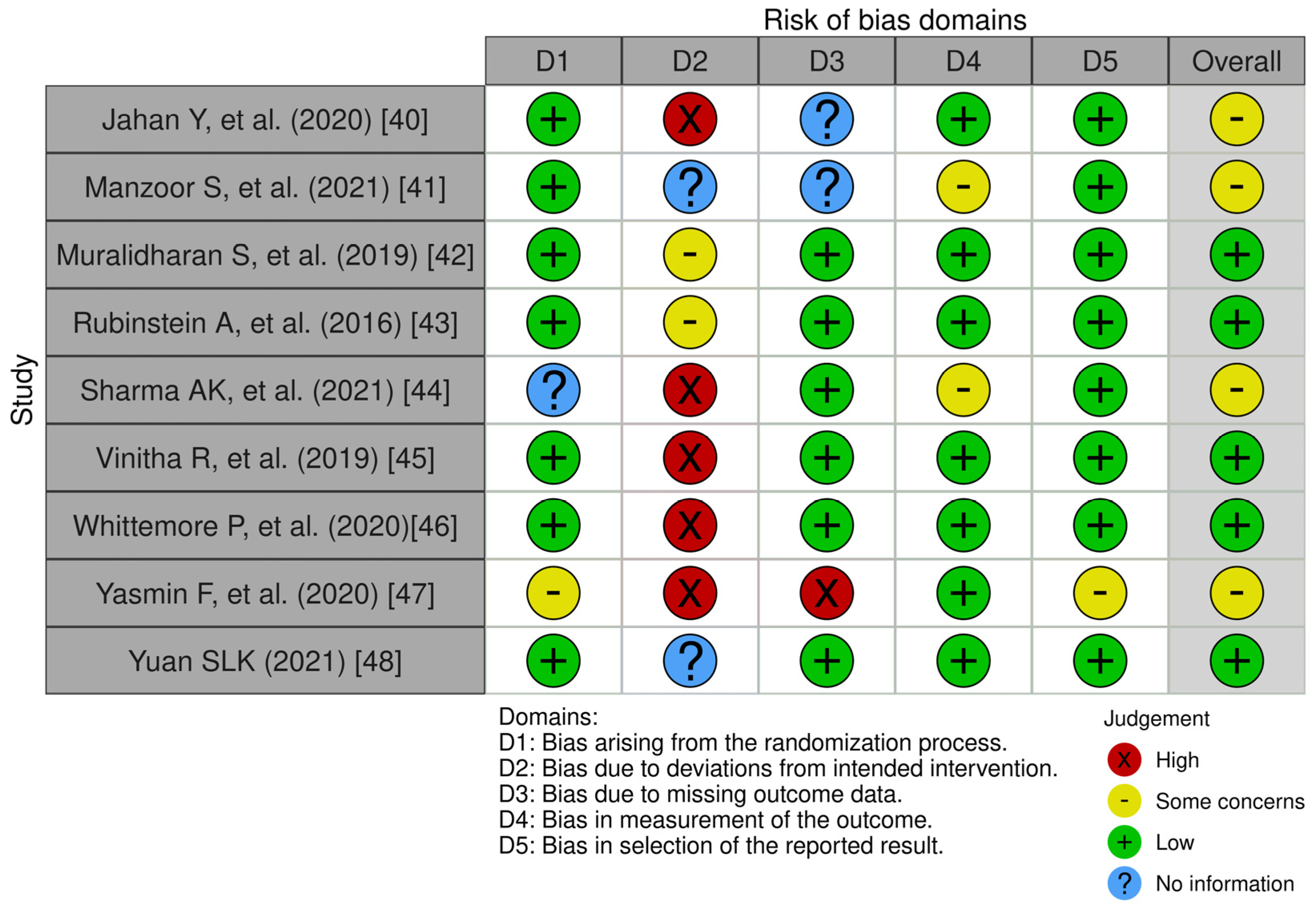
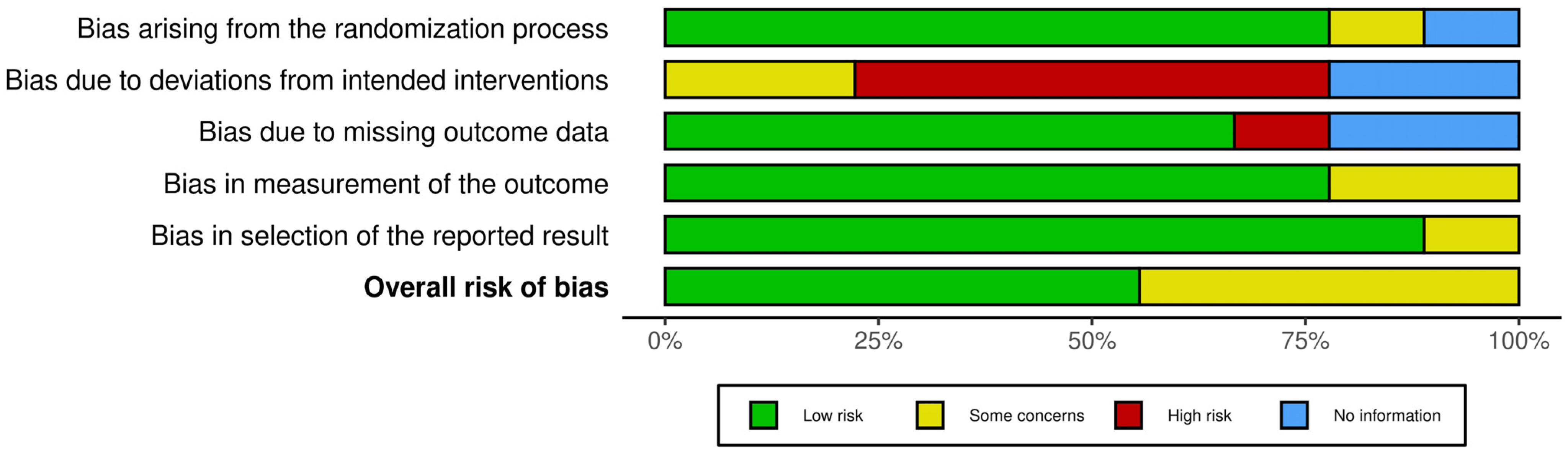
3.5. Risk of Bias Assessment
4. Discussion
4.1. Study Characteristics
4.2. Characteristics of mHealth and MEA Interventions
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pedersen, B.K.; Saltin, B. Exercise as medicine—Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports 2015, 25, 1–72. [Google Scholar] [CrossRef]
- Alvarez-Pitti, J.; Mallén, J.A.C.; Trabazo, R.L.; Lucía, A.; de Lara, D.L.; Aznar, L.A.M.; Martínez, G.R. Ejercicio físico como guillemotleft medicina guillemotright en enfermedades crónicas durante la infancia y la adolescencia. An. Pediatr. 2020, 92, 173.e1–173.e8. [Google Scholar] [CrossRef]
- Fiuza-Luces, C.; Santos-Lozano, A.; Joyner, M.; Carrera-Bastos, P.; Picazo, O.; Zugaza, J.L.; Izquierdo, M.; Ruilope, L.M.; Lucia, A. Exercise benefits in cardiovascular disease: Beyond attenuation of traditional risk factors. Nat. Rev. Cardiol. 2018, 15, 731–743. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef]
- Morán, F.E.; Morán, F.L.; Morán, F.J.; Albán, J. El tiempo en pantalla en el desarrollo de las actividades académicas y la salud de los estudiantes de educación superior en la modalidad en línea. Rev. Ibérica Sist. Tecnol. Inf. 2022, 5, 269–281. [Google Scholar]
- Battalio, S.L.; Conroy, D.E.; Dempsey, W.; Liao, P.; Menictas, M.; Murphy, S.; Nahum-Shani, I.; Qian, T.; Kumar, S.; Spring, B. Sense2Stop: A micro-randomized trial using wearable sensors to optimize a just-in-time-adaptive stress management intervention for smoking relapse prevention. Contemp. Clin. Trials 2021, 109, 106534. [Google Scholar] [CrossRef]
- Díaz-Martínez, X.; Petermann, F.; Leiva, A.M.; Garrido-Méndez, A.; Salas-Bravo, C.; Martínez, M.A.; Labraña, A.M.; Duran, E.; Valdivia-Moral, P.; Zagalaz, M.L.; et al. No cumplir con las recomendaciones de actividad física se asocia a mayores niveles de obesidad, diabetes, hipertensión y síndrome metabólico en población chilena. Rev. Médica Chile 2018, 146, 585–595. [Google Scholar] [CrossRef]
- Zhao, Y. COVID-19 as a catalyst for educational change. Prospects 2020, 49, 29–33. [Google Scholar] [CrossRef]
- Casanca, C.H.; Ventocilla, N.A.; Vásquez, M.R. Estilo de vida saludable, nivel de glucosa e IMC en adultos del Valle de Amauta—Ate Vitarte—Lima—2020. Rev. Cient. Cienc. Salud 2020, 13, 20–33. [Google Scholar] [CrossRef]
- Delahanty, L.M.; Trief, P.M.; Cibula, D.A.; Weinstock, R.S. Barriers to weight loss and physical activity, and coach approaches to addressing barriers, in a real-world adaptation of the DPP lifestyle intervention: A process analysis. Diabetes Educ. 2019, 45, 596–606. [Google Scholar] [CrossRef]
- Farah, B.Q.; Prado, W.L.D.; Malik, N.; Lofrano-Prado, M.C.; de Melo, P.H.; Botero, J.P.; Cucato, G.G.; Correia, M.d.A.; Ritti-Dias, R.M. Barriers to physical activity during the COVID-19 pandemic in adults: A cross-sectional study. Sport Sci. Health 2021, 17, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Lopez, P.; Pinto, R.S.; Radaelli, R.; Rech, A.; Grazioli, R.; Izquierdo, M.; Cadore, E.L. Benefits of resistance training in physically frail elderly: A systematic review. Aging Clin. Exp. Res. 2018, 30, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Bernal-Jiménez, M.Á.; Calle-Pérez, G.; Gutiérrez-Barrios, A.; Gheorghe, L.; Solano-Mulero, A.M.; Rodríguez-Martín, A.; Tur, J.A.; Vázquez-García, R.; Santi-Cano, M.J. Lifestyle and Treatment Adherence Intervention after a Coronary Event Based on an Interactive Web Application (EVITE): Randomized Controlled Clinical Trial Protocol. Nutrients 2021, 13, 1818. [Google Scholar] [CrossRef] [PubMed]
- de Sevilla, G.; Barceló Guido, O.; De la Cruz, M.D.L.P.; Fernández, A.B.; Alejo, L.B.; Ramírez Goercke, M.I.; Pérez-Ruiz, M. Remotely supervised exercise during the COVID-19 pandemic versus in-person-supervised exercise in achieving long-term adherence to a healthy lifestyle. Int. J. Environ. Res. Public Health 2021, 18, 12198. [Google Scholar] [CrossRef] [PubMed]
- Zapata-Lamana, R.; Lalanza, J.F.; Losilla, J.-M.; Parrado, E.; Capdevila, L. mHealth technology for ecological momentary assessment in physical activity research: A systematic review. PeerJ 2020, 8, e8848. [Google Scholar] [CrossRef] [PubMed]
- Partridge, S.R.; McGeechan, K.; Hebden, L.; Balestracci, K.; Wong, A.T.Y.; Denney-Wilson, E.; Harris, M.F.; Phongsavan, P.; Bauman, A.; Allman-Farinelli, M. Effectiveness of a mHealth lifestyle program with telephone support (TXT2BFiT) to prevent unhealthy weight gain in young adults: Randomized controlled trial. JMIR mHealth uHealth 2015, 3, e4530. [Google Scholar] [CrossRef] [PubMed]
- Dunton, G.F. Ecological momentary assessment in physical activity research. Exerc. Sport Sci. Rev. 2017, 45, 48. [Google Scholar] [CrossRef] [PubMed]
- Shiffman, S.; Stone, A.A.; Hufford, M.R. Ecological momentary assessment. Annu. Rev. Clin. Psychol. 2008, 4, 1–32. [Google Scholar] [CrossRef]
- Stone, A.A. Ecological Momentary Assessment in Survey Research. In The Palgrave Handbook of Survey Research; Vannette, D.L., Krosnick, J.A., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 221–226. [Google Scholar] [CrossRef]
- Liao, Y.; Intille, S.S.; Dunton, G.F. Using ecological momentary assessment to understand where and with whom adults’ physical and sedentary activity occur. Int. J. Behav. Med. 2015, 22, 51–61. [Google Scholar] [CrossRef]
- Caputo, E.L.; Reichert, F.F. Studies of physical activity and COVID-19 during the pandemic: A scoping review. J. Phys. Act. Health 2020, 17, 1275–1284. [Google Scholar] [CrossRef]
- Lee, M.; Lee, H.; Kim, Y.; Kim, J.; Cho, M.; Jang, J.; Jang, H. Mobile app-based health promotion programs: A systematic review of the literature. Int. J. Environ. Res. Public Health 2018, 15, 2838. [Google Scholar] [CrossRef] [PubMed]
- Buchholz, S.W.; Wilbur, J.; Ingram, D.; Fogg, L. Physical activity text messaging interventions in adults: A systematic review. Worldviews Evid.-Based Nurs. 2013, 10, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Davis, A.; Sweigart, R.; Ellis, R. A systematic review of tailored mHealth interventions for physical activity promotion among adults. Transl. Behav. Med. 2020, 10, 1221–1232. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.; Lee, J.-S.; Lee, S.-K. A technology-mediated interventional approach to the prevention of metabolic syndrome: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2021, 18, 512. [Google Scholar] [CrossRef] [PubMed]
- Cheatham, S.W.; Stull, K.R.; Fantigrassi, M.; Motel, I. The efficacy of wearable activity tracking technology as part of a weight loss program: A systematic review. J. Sports Med. Phys. Fit. 2018, 58, 534–548. [Google Scholar] [CrossRef] [PubMed]
- Romeo, A.; Edney, S.; Plotnikoff, R.; Curtis, R.; Ryan, J.; Sanders, I.; Crozier, A.; Maher, C. Can smartphone apps increase physical activity? Systematic review and meta-analysis. J. Med. Internet Res. 2019, 21, e12053. [Google Scholar] [CrossRef] [PubMed]
- Mönninghoff, A.; Kramer, J.-N.; Hess, A.; Ismailova, K.; Teepe, G.; Car, L.T.; Müller-Riemenschneider, F.; Kowatsch, T. Long-term effectiveness of mHealth physical activity interventions: Systematic review and meta-analysis of randomized controlled trials. J. Med. Internet Res. 2021, 23, e26699. [Google Scholar] [CrossRef] [PubMed]
- Cotie, L.M.; Prince, S.A.; Elliott, C.G.; Ziss, M.C.; McDonnell, L.A.; Mullen, K.A.; Hiremath, S.; Pipe, A.L.; Reid, R.D.; Reed, J.L. The effectiveness of eHealth interventions on physical activity and measures of obesity among working-age women: A systematic review and meta-analysis. Obes. Rev. 2018, 19, 1340–1358. [Google Scholar] [CrossRef]
- Valentiner, L.S.; Thorsen, I.K.; Kongstad, M.B.; Brinkløv, C.F.; Larsen, R.T.; Karstoft, K.; Nielsen, J.S.; Pedersen, B.K.; Langberg, H.; Ried-Larsen, M. Effect of ecological momentary assessment, goal-setting and personalized phone-calls on adherence to interval walking training using the InterWalk application among patients with type 2 diabetes—A pilot randomized controlled trial. PLoS ONE 2019, 14, e0208181. [Google Scholar] [CrossRef]
- Kuijpers, W.; Groen, W.G.; Aaronson, N.K.; van Harten, W.H. A systematic review of web-based interventions for patient empowerment and physical activity in chronic diseases: Relevance for cancer survivors. J. Med. Internet Res. 2013, 15, e2281. [Google Scholar] [CrossRef]
- Laranjo, L.; Ding, D.; Heleno, B.; Kocaballi, B.; Quiroz, J.C.; Tong, H.L.; Chahwan, B.; Neves, A.L.; Gabarron, E.; Dao, K.P.; et al. Do smartphone applications and activity trackers increase physical activity in adults? Systematic review, meta-analysis and metaregression. Br. J. Sports Med. 2021, 55, 422–432. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-N.; Seo, K. Smartphone-based health program for improving physical activity and tackling obesity for young adults: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2020, 17, 15. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating guidance for reporting systematic reviews: Development of the PRISMA 2020 statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef] [PubMed]
- McGowan, J.; Sampson, M.; Salzwedel, D.M.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS peer review of electronic search strategies: 2015 guideline statement. J. Clin. Epidemiol. 2016, 75, 40–46. [Google Scholar] [CrossRef] [PubMed]
- OECD.org—OECD n.d. Available online: https://www.oecd.org/ (accessed on 18 March 2024).
- OMC | Desarrollo—¿Qué Países se Consideran Países en Desarrollo en la OMC? n.d. Available online: https://www.wto.org/spanish/tratop_s/devel_s/d1who_s.htm (accessed on 18 March 2024).
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Jahan, Y.; Rahman, M.; Faruque, A.S.G.; Chisti, M.J.; Kazawa, K.; Matsuyama, R.; Moriyama, M. Awareness Development and Usage of Mobile Health Technology Among Individuals with Hypertension in a Rural Community of Bangladesh: Randomized Controlled Trial. J. Med. Internet Res. 2020, 22, e19137. [Google Scholar] [CrossRef]
- Manzoor, S.; Hisam, A.; Aziz, S.; Mashhadi, S.F.; Haq, Z.U. Effectiveness of Mobile Health Augmented Cardiac Rehabilitation on Behavioural Outcomes among Post-acute Coronary Syndrome Patients: A Randomised Controlled Trial. J. Coll. Physicians Surg. 2021, 31, 1148–1153. [Google Scholar] [CrossRef]
- Muralidharan, S.; Ranjani, H.; Anjana, R.M.; Jena, S.; Tandon, N.; Gupta, Y.; Ambekar, S.; Koppikar, V.; Jagannathan, N.; Allender, S.; et al. Engagement and Weight Loss: Results from the Mobile Health and Diabetes Trial. Diabetes Technol. Ther. 2019, 21, 507–513. [Google Scholar] [CrossRef]
- Rubinstein, A.; Miranda, J.J.; Beratarrechea, A.; Diez-Canseco, F.; Kanter, R.; Gutierrez, L.; Bernabé-Ortiz, A.; Irazola, V.; Fernandez, A.; Letona, P.; et al. Effectiveness of an mHealth intervention to improve the cardiometabolic profile of people with prehypertension in low-resource urban settings in Latin America: A randomised controlled trial. Lancet Diabetes Endocrinol. 2016, 4, 52–63. [Google Scholar] [CrossRef]
- Sharma, A.K.; Baig, V.N.; Ahuja, J.; Sharma, S.; Panwar, R.B.; Katoch, V.M.; Gupta, R. Efficacy of IVRS-based mHealth intervention in reducing cardiovascular risk in metabolic syndrome: A cluster randomized trial. Diabetes Metab. Syndr.-Clin. Res. Rev. 2021, 15, 102182. [Google Scholar] [CrossRef] [PubMed]
- Vinitha, R.; Nanditha, A.; Snehalatha, C.; Satheesh, K.; Susairaj, P.; Raghavan, A.; Ramachandran, A. Effectiveness of mobile phone text messaging in improving glycaemic control among persons with newly detected type 2 diabetes. Diabetes Res. Clin. Pract. 2019, 158, 107919. [Google Scholar] [CrossRef]
- Whittemore, R.; Vilar-Compte, M.; De La Cerda, S.; Delvy, R.; Jeon, S.; Burrola-Méndez, S.; Pardo-Carrillo, M.; Lozano-Marrufo, A.; Pérez-Escamilla, R. ¡Sí, Yo Puedo Vivir Sano Con Diabetes! A self-management randomized controlled pilot trial for low-income adults with type 2 diabetes in Mexico City. Curr. Dev. Nutr. 2020, 4, nzaa074. [Google Scholar] [CrossRef]
- Yasmin, F.; Nahar, N.; Banu, B.; Ali, L.; Sauerborn, R.; Souares, A. The influence of mobile phone-based health reminders on patient adherence to medications and healthy lifestyle recommendations for effective management of diabetes type 2: A randomized control trial in Dhaka, Bangladesh. BMC Health Serv. Res. 2020, 20, 520. [Google Scholar] [CrossRef]
- Yuan, S.L.K.; Couto, L.A.; Marques, A.P. Effects of a six-week mobile app versus paper book intervention on quality of life, symptoms, and self-care in patients with fibromyalgia: A randomized parallel trial. Braz. J. Phys. Ther. 2021, 25, 428–436. [Google Scholar] [CrossRef]
- Gür, F.; Gür, G.C.; Ayan, V. The Effect of the ERVE Smartphone App on Physical Activity, Quality of Life, Self-Efficacy, and Exercise Motivation for Inactive People: A Randomized Controlled Trial. Eur. J. Integr. Med. 2020, 39, 101198. [Google Scholar] [CrossRef]
- Fenton, S.; Burrows, T.L.; Collins, C.E.; Rayward, A.T.; Murawski, B.; Duncan, M.J. Efficacy of a Multi-Component m-Health Diet, Physical Activity, and Sleep Intervention on Dietary Intake in Adults with Overweight and Obesity: A Randomised Controlled Trial. Nutrients 2021, 13, 2468. [Google Scholar] [CrossRef] [PubMed]
- Al-Nawaiseh, H.K.; McIntosh, W.A.; McKyer, L.J. An-m-Health Intervention Using Smartphone App to Improve Physical Activity in College Students: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 7228. [Google Scholar] [CrossRef] [PubMed]
- Solar, C.; Nansubuga, A.; Murillo, J.; Ranker, L.; Borrelli, B.; Bowen, D.J.; Xuan, Z.; Kane, J.; Werntz, S.; Crouter, S.E.; et al. Mobile health plus community health worker support for weight management among public housing residents (Path to Health): A randomized controlled trial protocol. Contemp. Clin. Trials 2022, 119, 106836. [Google Scholar] [CrossRef]
- Vetrovsky, T.; Kral, N.; Pfeiferova, M.; Kuhnova, J.; Novak, J.; Wahlich, C.; Jaklova, A.; Jurkova, K.; Janek, M.; Omcirk, D.; et al. mHealth intervention delivered in general practice to increase physical activity and reduce sedentary behaviour of patients with prediabetes and type 2 diabetes (ENERGISED): Rationale and study protocol for a pragmatic randomised controlled trial. BMC Public Health 2023, 23, 613. [Google Scholar] [CrossRef]
- Jeganathan, V.S.; Golbus, J.R.; Gupta, K.; Luff, E.; Dempsey, W.; Boyden, T.; Rubenfire, M.; Mukherjee, B.; Klasnja, P.; Kheterpal, S.; et al. Virtual AppLication-supported Environment To INcrease Exercise (VALENTINE) during cardiac rehabilitation study: Rationale and design. Am. Heart J. 2022, 248, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Alòs, F.; Colomer, M.; Martin-Cantera, C.; Solís-Muñoz, M.; Bort-Roig, J.; Saigi, I.; Chirveches-Pérez, E.; Solà-Gonfaus, M.; Molina-Aragonés, J.M.; Puig-Ribera, A. Effectiveness of a healthcare-based mobile intervention on sedentary patterns, physical activity, mental well-being and clinical and productivity outcomes in office employees with type 2 diabetes: Study protocol for a randomized controlled trial. BMC Public Health 2022, 22, 1269. [Google Scholar] [CrossRef]
- Bohlen, L.C.; LaRowe, L.R.; Dunsiger, S.I.; Dionne, L.; Griffin, E.; Kim, A.E.; Marcus, B.H.; Unick, J.; Wu, W.-C.; Williams, D.M. Comparing a recommendation for self-paced versus moderate intensity physical activity for midlife adults: Rationale and design. Contemp. Clin. Trials 2023, 128, 107169. [Google Scholar] [CrossRef] [PubMed]
- Trull, T.J.; Ebner-Priemer, U.W. Using Experience Sampling Methods/Ecological Momentary Assessment (ESM/EMA) in Clinical Assessment and Clinical Research: Introduction to the Special Section. Psychol. Assess. 2009, 21, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Magallón-Neri, E.; Kirchner-Nebot, T.; Forns-Santacana, M.; Calderón, C.; Planellas, I. Ecological Momentary Assessment with smartphones for measuring mental health problems in adolescents. World J. Psychiatry 2016, 6, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Magallón-Neri, E.; Kirchner, T.; Forns, M.; Calderón, C.; Planellas, I. Ecological momentary assessment of contextual variables, satisfaction, and emotional and behavioral states of adolescents by level of victimization. Child Abus. Negl. 2018, 80, 268–276. [Google Scholar] [CrossRef] [PubMed]
- Palmier-Claus, J.E.; Myin-Germeys, I.; Barkus, E.; Bentley, L.; Udachina, A.; Delespaul, P.A.E.G.; Lewis, S.W.; Dunn, G. Experience sampling research in individuals with mental illness: Reflections and guidance. Acta Psychiatr. Scand. 2011, 123, 12–20. [Google Scholar] [CrossRef]
- Runyan, J.D.; Steinke, E.G. Virtues, ecological momentary assessment/intervention and smartphone technology. Front. Psychol. 2015, 6, 481. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Criteria | Description |
|---|---|
| (1) Population | Studies that included adults, men and women between 18 and 60 years old, with any health condition (healthy and with pathologies) who live in developing countries according to the classification established by the Organization for Cooperation and Development Economic (OCDE) [36] and developing countries in the WTO (World Trade Organization) [37]. |
| (2) Intervention | Studies that used interventions involving physical exercise programs carried out with mHealth in EMA modality for their prescription. |
| (3) Outcome variables | Studies that evaluated at least one of the following variables:
|
| (4) Study design | All articles with randomized controlled experimental designs which provide original data on the use of mHealth and EMA in physical exercise (criteria 1, 2 and 3) and are published in scientific journals. |
| Author (Year), Country | Population | Intervention Group | Control Group | Outcomes | Design Type | ||||
|---|---|---|---|---|---|---|---|---|---|
| Health Condition and Sample I/F (n°) | Gender M/F | (n°) ADH | (%) Age | (M) NSE | |||||
| Jahan Y, et al. (2020), Bangladesh. [40] | Adults with hypertension 420/4,12 | 59/361 | 72.7 | 52.9 | Low | The intervention group received SMS text messages and 5 months of health education along with a health education booklet. Text messages (SMS) were sent 5 times during the first month and once a week for the remaining 4 months (a total of 21 SMS text messages), along with questionnaires according to the DASH (Dietary Approaches to Stop Hypertensive) diet. | The control group received only face-to-face health education and not SMS text messages. They received the same health education pamphlet as the intervention group and were followed every month for up to 5 months (twice in the first month and once in the rest), but did not receive SMS text messages. | Physical activity Body weight Salt intake Fruit intake Vegetable intake Blood pressure Quality of life | Two-arm Randomized Controlled Study |
| Manzoor S, et al. (2021), Pakistan. [41] | Adults with coronary syndrome, 160/119 | 126/34 | 74.4 | 52.6 | Low | First phase of Mcard included individualized counseling; second phase, daytime mobile texting of standardized messages using an app especially and standard post-ACS care. (Counseling, short text messages and standard post-ACS care). Healthy eating (healthy eating assessment tool) and physical activity (IPAQ tool). | Standard care after myocardial infarction Standard care after myocardial infarction | Physical activity Healthy nutrition Measurement compliance Smoking Salt intake Blood pressure Body weight | Two-arm Randomized Controlled Study |
| Muralidharan S, et al. (2019), India. [42] | Adults at high risk of DM2 (pre-DM and/or obesity), 741/561 | 320/241 | - | 37.8 | Low, half | (mDiab) mobile health and diabetes program. It included video lessons, text messages, interactive text, and weekly coaching via calls and emails. The intervention was delivered via a mobile phone application along with weekly coach calls. | Control group received usual care Usual care | Physical activity Weight loss Diet | Randomized Controlled Three-armed study. |
| Reading and carrying out guidelines on daily care based on mobility and healthy eating. Periodic messages (does not specify time). | |||||||||
| Rubinstein A, et al. (2016) Argentina, Guatemala, Perú. [43] | Adults with prehypertension. 637/553 | 295/342 | 84 | 43.6 | Low | Monthly motivational coaching calls and weekly personalized text messages on diet quality and physical activity based on the transtheoretical model. Monthly motivational coaching calls and weekly personalized text messages. | Usual care Usual care | Physical activity Body weight Fruits and vegetables Less intake of foods rich in sodium, fat, and sugar Blood pressure Waist circumference | Two-arm Randomized Controlled Study |
| Sharma AK, et al. (2021) Jaipur India. [44] | Adults with metabolic syndrome 1200/1012 | 468/544 | 60 | 40 | Low | mHealth group mobile health intervention in the form of daily one-way IVRS (interactive voice response system) audio clip in Hindi using a full automated system. Two messages promoting a healthy lifestyle and medical treatment were broadcast daily for 12 months and risk factors were reassessed. | Control group (standard care), provided by the local state government health center. | Physical activity Healthy diet Tobacco Waist circumference BMI Systolic pressure Fasting glucose Cholesterol | Two-arm Randomized Controlled Study |
| Vinitha R, et al. (2019) India. [45] | Adults with newly diagnosed type 2 diabetes. 248/218 | 168/80 | - | 43.3 | Half, high. | The recent physical activity questionnaire (RPAQ), A.F, was performed for the last 4 weeks, and sleep duration was also used. European Quality of Life Questionnaire 5 Dimension (EQ5D), 24 h recall diet, and text message acceptability questionnaires were completed at 6, 8, 12, and 24 months. They were counseled on an individual level about healthy behavioral changes to follow a pattern of a healthy diet and physical activity, and they also received 2 to 3 personalized educational text messages per week until the end of the study. | Control group, standard care advice only at the beginning. Standard. | Blood pressure glycemia LDL HbA1c | Two-arm Randomized Controlled Study |
| Whittemore P, et al. (2020) México. [46] | Low-income adults with type 2 diabetes. 85/82 | 58/27 | 89 | 55.5 | Low | DSME (Yes, I can!) program (diabetes self-management education program plus text message). It consisted of 7 weekly interactive group educational sessions on diabetes self-management and 6 months of daily texting/pictures. Physical activity was measured with the global physical activity questionnaire, which consists of 16 items that evaluate the frequency, intensity, and duration carried out at work and during transportation and free time, as well as sedentary behavior. | Standard DM2. Standard diabetes care | Two-arm Randomized Controlled Study | |
| Yasmin F, et al. (2020) Dhaka Bangladesh. [47] | Adults with type 2 diabetes, 320/273 | 71/249 | - | 52 | Low | Intervention group included mobile phone reminders and a 24/7 call center. Reminder system through interactive voice calls one or two days before scheduled hospital visits, a related information and suggestion service, and a 24/7 call center service. Average duration of each call was 10 min. | They only received regular hospital services. They only received regular hospital services. | Physical exercise Diet Tobacco and betel nut consumption Blood glucose | Two-arm Randomized Controlled Study |
| Yuan SLK, Couto LA, AP Trademarks (2021) Brasil. [48] | Adults with fibromyalgia, 40/36 | 1/39 | 40 | 43.3 | Low | ProFibro App Application Group (PAG). Program with aerobic, stretching, and strengthening exercises. Evaluated through the ProFibro App (PAG), participants received a 20-minute tutorial that guided them through the app’s features or book chapters. | Paper Book Group (PBG), a traditional paper book group with similar content, symptoms, and self-care agency for patients. 20-minute introductory tutorial that guided participants through app features or book chapters. | Physical activity Pain Quality of life | Two-arm Randomized Controlled Study |
| Author (Year), Country | Groups | Frequency | Exercise INTENSITY | Session Duration (Min) | Sessions per Day | Intervention Duration | Type of Exercise |
|---|---|---|---|---|---|---|---|
| Weekly Sessions | (n°) | (Months) | |||||
| Jahan Y, et al. (2020), Bangladesh. [40] | IG | 5 | - | 30 | - | 5 months | - |
| CG | - | - | - | - | - | ||
| Manzoor S, et al. (2021), Pakistan. [41] | IG | 3 | Low, moderate, high. | 20 | - | 6 months | Hike |
| CG | - | - | - | - | - | ||
| Muralidharan S, et al. (2019), India. [42] | IG | - | - | - | - | 3 months | They encouraged physical activity; the type of exercise, intensity and duration was not specified. |
| CG1 | - | - | - | - | - | ||
| CG2 | - | - | - | - | - | ||
| Rubinstein A, et al. (2016) Argentina, Guatemala, Peru. [43] | IG | - | - | - | - | 12 months | - |
| CG | - | - | - | - | - | - | |
| Sharma AK, et al. (2021) Jaipur India. [44] | IG | - | Moderate | - | - | 12 months | Physical activity in relation to work activity and free time activity. |
| CG | - | - | - | - | - | - | |
| Vinitha R, et al. (2019) India. [45] | IG | - | - | - | - | 24 months | - |
| CG | - | - | - | - | - | - | |
| Whittemore P, et al. (2020) México. [46] | IG | - | - | - | - | 6 months | - |
| CG | - | - | - | - | - | - | |
| Yasmin F, et al. (2020) Dhaka Bangladesh. [47] | IG | 5 | - | 30 min | 1 | 12 months | The patient was considered adherent if he walked 30 min per day or 150 min in a week (according to the WHO). |
| CG | - | - | - | - | - | - | |
| Yuan SLK, Couto LA, AP Trademarks (2021) Brasil. [48] | IG | - | - | - | - | 1 month and a half | Graduated aerobic, stretching, and strengthening exercise program. |
| CG | - | - | - | - | - | - |
| Physical and Metabolic Health | Mental Health | Cognition | Social | |||||
|---|---|---|---|---|---|---|---|---|
| Author (Year) | Groups | Physical Activity | Anthropometric Measurements | Nutrition | Medical Variables | Quality of Life | ||
| Jahan Y, et al. (2020), Bangladesh. [40] | IG | * | Body weight monitoring * | Salt intake * Fruit intake * Vegetable intake * | Blood pressure monitoring * | Quality of life * | - | - |
| CG | * | Body weight monitoring * | Salt intake * Fruit intake * Vegetable intake * | Blood pressure monitoring * | Quality of life * | - | - | |
| Manzoor S, et al. (2021), Pakistan. [41] | IG | * | Weight = | Healthy nutrition * Salt consumption * Smoking * | Self-monitoring of BP * Medication compliance * | - | - | - |
| CG | - | - | Healthy nutrition * | - | - | - | - | |
| Muralidharan S, et al. (2019), India. [42] | IG | * | Weight * | Diet * | - | - | - | - |
| CG1 | - | Weight = | - | - | - | - | - | |
| CG2 | - | Weight = | - | - | - | - | - | |
| Rubinstein A, et al. (2016) Argentina, Guatemala, Perú. [43] | IG | = | Body weight * Body Mass Index (BMI). * Waist circumference = | Improvement in diet quality * Fruits and vegetables * Lower intake of foods rich in sodium and fat * | Systolic Pressure = Diastolic Pressure = Net Pressure = | - | - | - |
| GC | - | - | - | Blood pressure * | - | - | - | |
| Sharma AK, et al. (2021) Jaipur India. [44] | IG | * | Weight * Waist circumference (HC). * Body Mass Index (BMI). * | Healthy diet * Tobacco * | Blood pressure * Fasting glucose * Total cholesterol * Triglycerides * HDL Cholesterol * LDL Cholesterol * | - | - | - |
| CG | * | Weight * Waist circumference (HC). * Body Mass Index (BMI). * | Healthy diet * Tobacco * | Blood pressure * Fasting glucose * Total cholesterol * Triglycerides * HDL Cholesterol * LDL Cholesterol * | - | - | - | |
| Vinitha R, et al. (2019) India. [45] | IG | * | - | Diet * | Blood pressure * Blood glucose * LDL Cholesterol * Glycosylated hemoglobin (HbA1c) * | Quality of life * | - | - |
| CG | - | - | - | Blood pressure * Blood glucose * LDL Cholesterol * Glycosylated hemoglobin (HbA1c) * | - | - | - | |
| Whittemore P, et al. (2020) México. [46] | IG | * | - | - | Systolic and diastolic BP * Glycosylated hemoglobin (HbA1c) * | Depressive symptoms * Self-efficacy * | - | - |
| CG | - | - | - | - | - | - | - | |
| Yasmin F, et al. (2020) Dhaka Bangladesh. [47] | IG | * | - | Diet (CHO, proteins, fats). * Intake of fruits and vegetables * Smokeless tobacco, chewing tobacco and betel nut * Tobacco or cigarette smoke * | Fasting blood glucose level * Blood glucose level 2 h after breakfast * | - | - | - |
| CG | = | - | Diet (CHO, proteins, fats). = Intake of fruits and vegetables = Smokeless tobacco, chewing tobacco, and betel nut = Tobacco or cigarette smoke = | Fasting blood glucose level = Blood glucose level 2 h after breakfast = | - | - | - | |
| Yuan SLK (2021) [48] | IG | * | - | - | Pain * Severity of symptoms * | Quality of life * | Self-care * | - |
| CG | * | - | - | Pain * Severity of symptoms * | Quality of life * | Self-care * | - | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flores Aniotz, A.; Reyes-Molina, D.; Cigarroa, I.; García-Merino, S.; Rubio Alonso, M.; Pérez Ruiz, M.; Zapata-Lamana, R. Effect of Physical Exercise Programs Based on Mobile Health and Ecological Momentary Assessment on the Physical and Mental Health, Cognitive Functions, and Social Environment of Adults in Developing Countries: A Systematic Review. Medicina 2024, 60, 578. https://doi.org/10.3390/medicina60040578
Flores Aniotz A, Reyes-Molina D, Cigarroa I, García-Merino S, Rubio Alonso M, Pérez Ruiz M, Zapata-Lamana R. Effect of Physical Exercise Programs Based on Mobile Health and Ecological Momentary Assessment on the Physical and Mental Health, Cognitive Functions, and Social Environment of Adults in Developing Countries: A Systematic Review. Medicina. 2024; 60(4):578. https://doi.org/10.3390/medicina60040578
Chicago/Turabian StyleFlores Aniotz, Alejandro, Daniel Reyes-Molina, Igor Cigarroa, Sonia García-Merino, Margarita Rubio Alonso, Margarita Pérez Ruiz, and Rafael Zapata-Lamana. 2024. "Effect of Physical Exercise Programs Based on Mobile Health and Ecological Momentary Assessment on the Physical and Mental Health, Cognitive Functions, and Social Environment of Adults in Developing Countries: A Systematic Review" Medicina 60, no. 4: 578. https://doi.org/10.3390/medicina60040578