Respiratory Support Effects over Time on Regional Lung Ventilation Assessed by Electrical Impedance Tomography in Premature Infants

 ,
,
Abstract
:1. Introduction
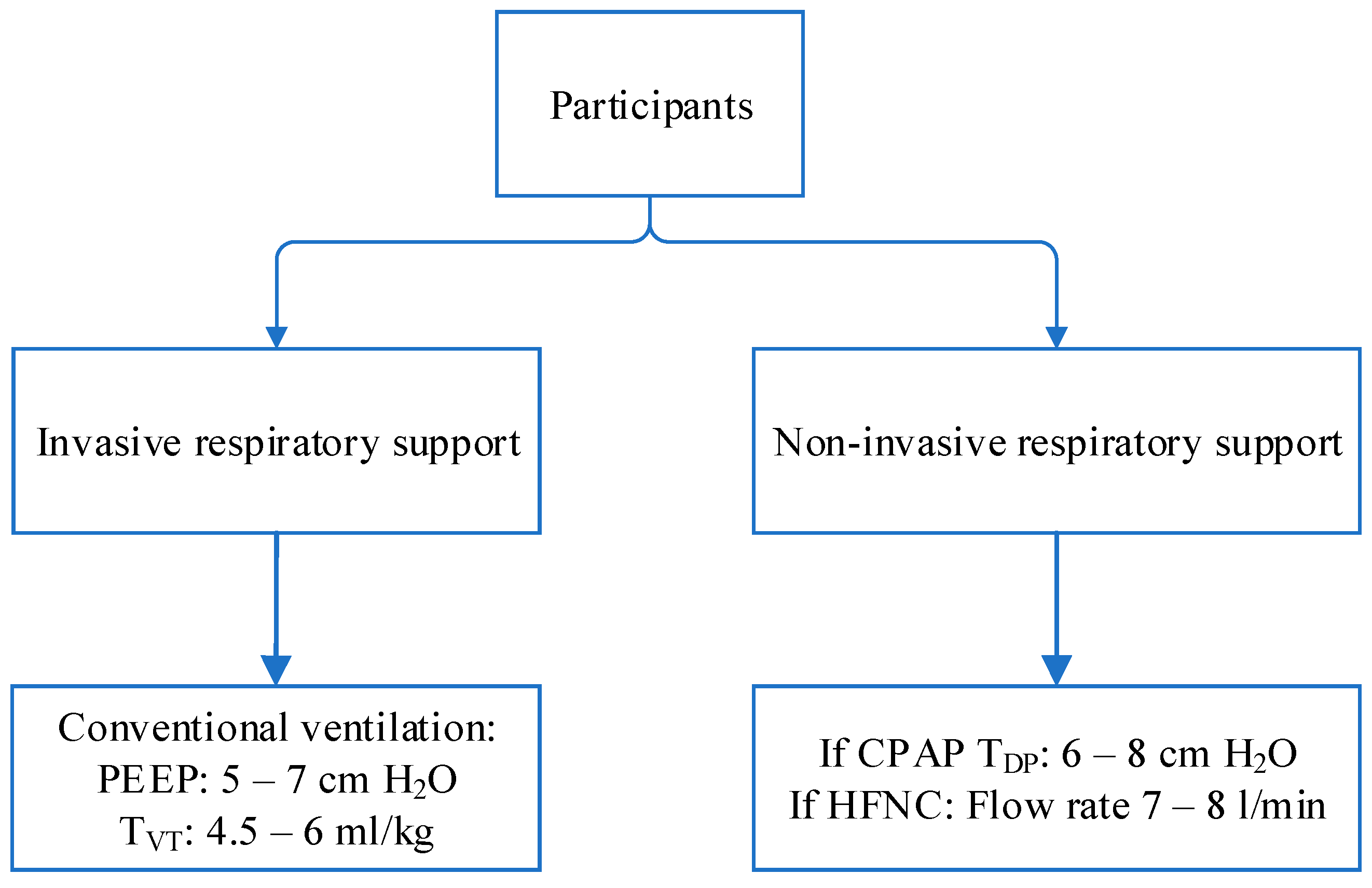
2. Materials and Methods
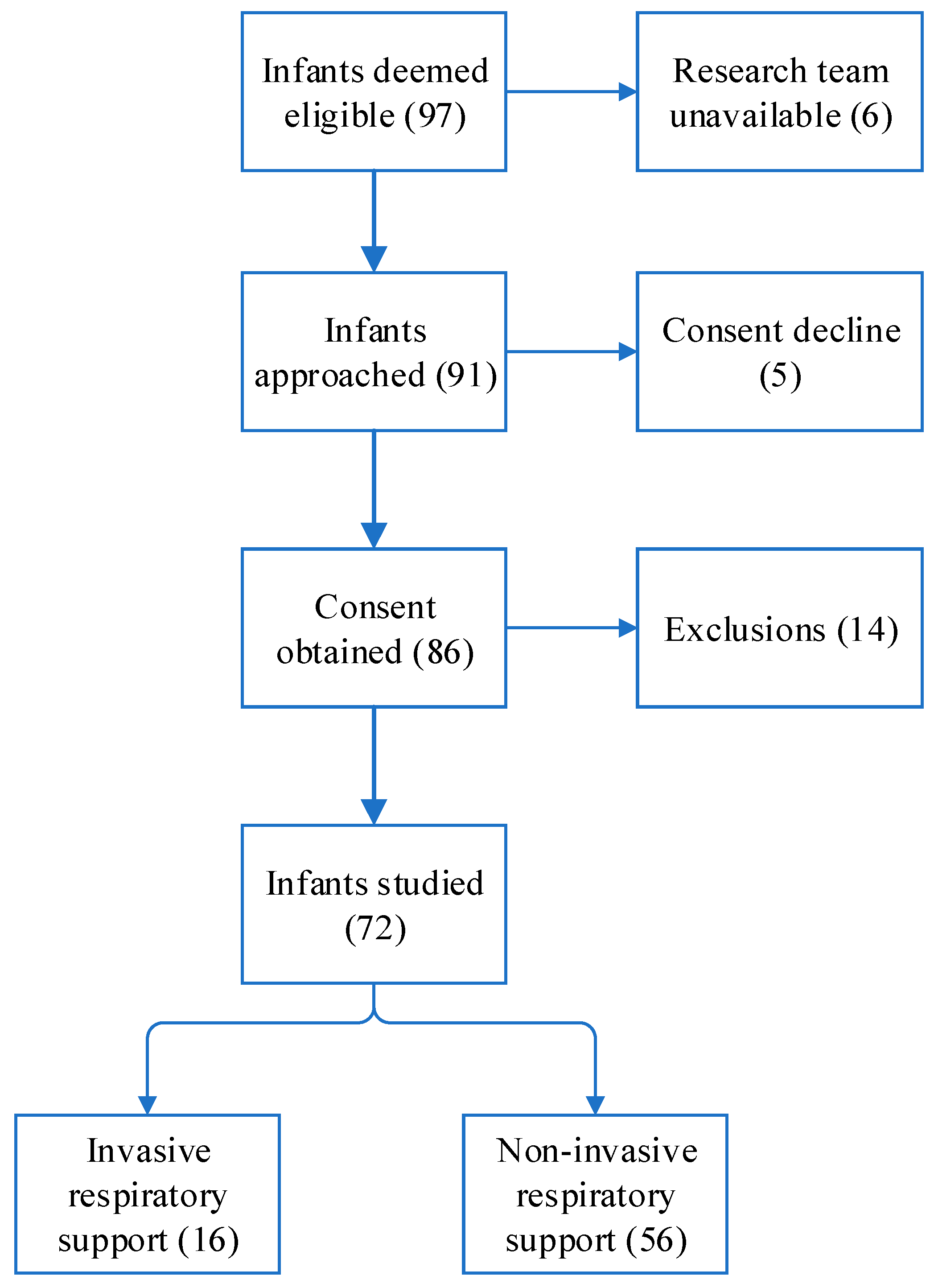
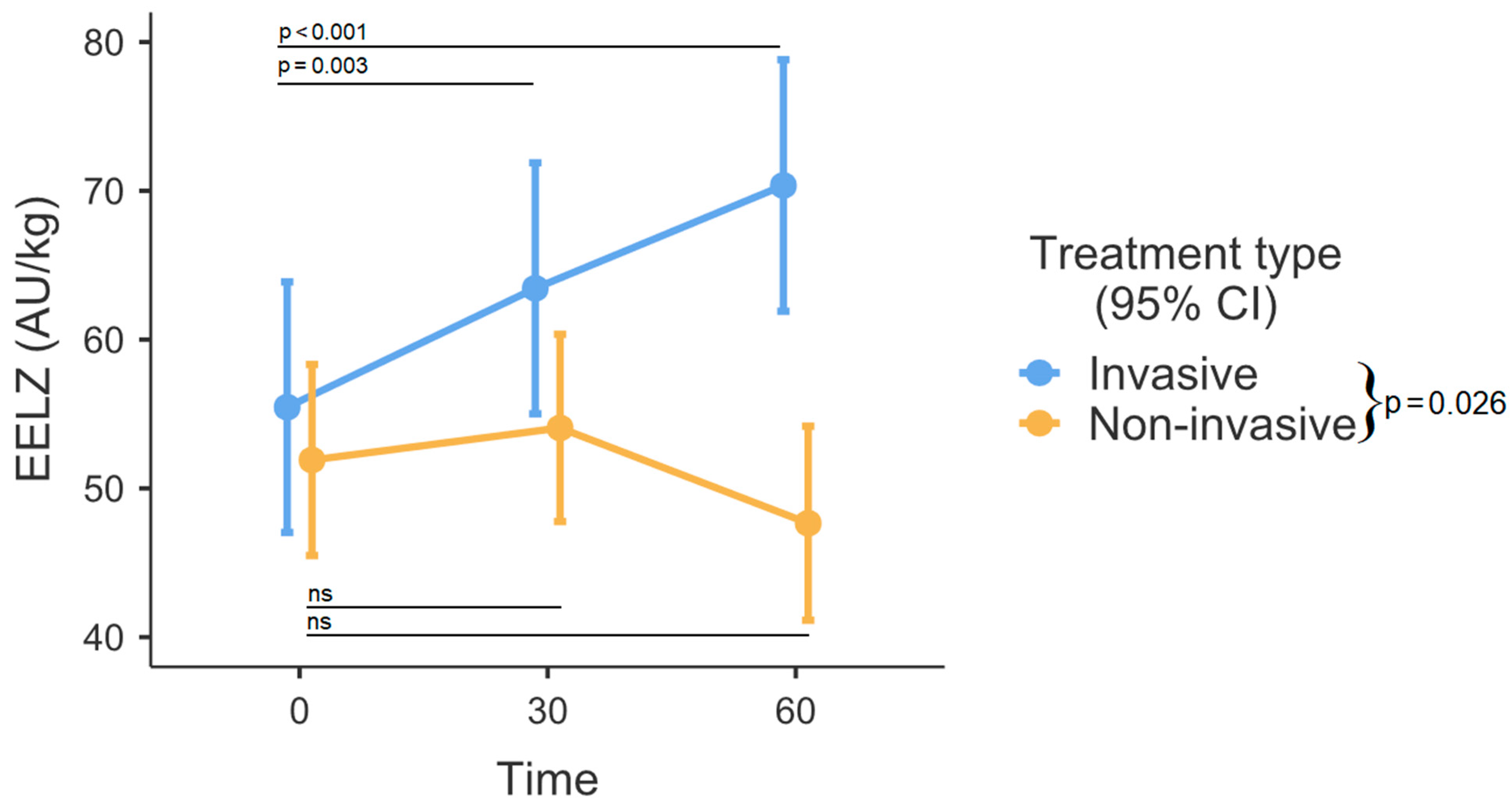
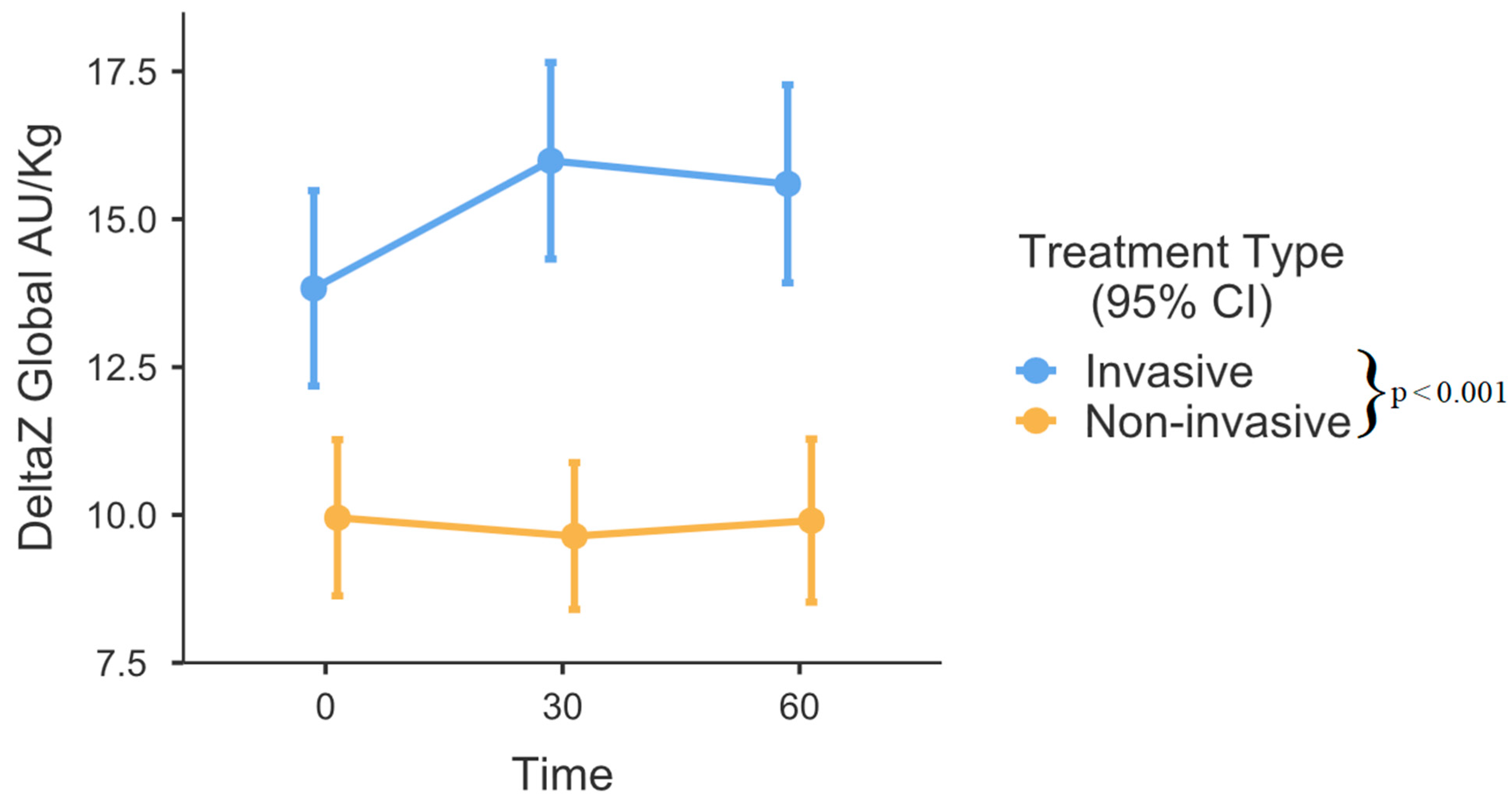
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sweet, D.G.; Carnielli, V.P.; Greisen, G.; Hallman, M.; Klebermass-Schrehof, K.; Ozek, E.; Pas, A.T.; Plavka, R.; Roehr, C.C.; Saugstad, O.D.; et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome: 2022 Update. Neonatology 2023, 120, 3–23. [Google Scholar] [CrossRef] [PubMed]
- Beltempo, M.; Isayama, T.; Vento, M.; Lui, K.; Kusuda, S.; Lehtonen, L.; Sjörs, G.; Håkansson, S.; Adams, M.; Noguchi, A.; et al. Respiratory Management of Extremely Preterm Infants: An International Survey. Neonatology 2018, 114, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Clark, R.H.; Gerstmann, D.R.; Jobe, A.H.; Moffitt, S.T.; Slutsky, A.S.; Yoder, B.A. Lung injury in neonates: Causes, strategies for prevention, and long-term consequences. J. Pediatr. 2001, 139, 478–486. [Google Scholar] [CrossRef] [PubMed]
- Kalikkot Thekkeveedu, R.; El-Saie, A.; Prakash, V.; Katakam, L.; Shivanna, B. Ventilation-Induced Lung Injury (VILI) in Neonates: Evidence-Based Concepts and Lung-Protective Strategies. J. Clin. Med. 2022, 11, 557. [Google Scholar] [CrossRef]
- Sefic Pasic, I.; Riera Soler, L.; Vazquez Mendez, E.; Castillo Salinas, F. Comparison between lung ultrasonography and chest X-ray in the evaluation of neonatal respiratory distress syndrome. J. Ultrasound 2022, 26, 435–448. [Google Scholar] [CrossRef] [PubMed]
- Maciejewski, D.; Putowski, Z.; Czok, M.; Krzych, Ł.J. Electrical impedance tomography as a tool for monitoring mechanical ventilation. An introduction to the technique. Adv. Med. Sci. 2021, 66, 388–395. [Google Scholar] [CrossRef]
- Als, H.; Lawhon, G.; Duffy, F.H.; McAnulty, G.B.; Gibes-Grossman, R.; Blickman, J.G. Individualized developmental care for the very low-birth-weight preterm infant. Medical and neurofunctional effects. JAMA 1994, 272, 853–858. [Google Scholar] [CrossRef] [PubMed]
- Hysinger, E.B.; Ahlfeld, S.K. Respiratory support strategies in the prevention and treatment of bronchopulmonary dysplasia. Front. Pediatr. 2023, 11, 1087857. [Google Scholar] [CrossRef]
- Lampland, A.L.; Plumm, B.; Meyers, P.A.; Worwa, C.T.; Mammel, M.C. Observational Study of Humidified High-Flow Nasal Cannula Compared with Nasal Continuous Positive Airway Pressure. J. Pediatr. 2009, 154, 177–182.e2. [Google Scholar] [CrossRef]
- Subramaniam, P.; Ho, J.J.; Davis, P.G. Prophylactic or very early initiation of continuous positive airway pressure (CPAP) for preterm infants. Cochrane Database Syst. Rev. 2021, 10, CD001243. [Google Scholar] [CrossRef]
- Matlock, D.N.; Bai, S.; Weisner, M.D.; Comtois, N.; Beck, J.; Sinderby, C.; Courtney, S.E. Tidal volume transmission during non-synchronized nasal intermittent positive pressure ventilation via RAM® cannula. J. Perinatol. 2019, 39, 723–729. [Google Scholar] [CrossRef]
- Williams, E.E.; Dassios, T.; Hunt, K.A.; Greenough, A. Volumetric capnography pre- and post-surfactant during initial resuscitation of premature infants. Pediatr. Res. 2022, 91, 1551–1556. [Google Scholar] [CrossRef]
- Brinkman, J.E.; Toro, F.; Sharma, S. Physiology RD [Updated 2021 A 24]. IS [Internet]. TI (FL): SP 2022 J. Available online: https://www.ncbi.nlm.nih.gov/books/NBK482414/ (accessed on 24 November 2023).
- Bachmann, M.C.; Morais, C.; Bugedo, G.; Bruhn, A.; Morales, A.; Borges, J.B.; Costa, E.; Retamal, J. Electrical impedance tomography in acute respiratory distress syndrome. Crit. Care 2018, 22, 263. [Google Scholar] [CrossRef]
- Kastein, K.; Coe, K. Management of Air Leaks in the Newborn. Adv. Neonatal Care 2023, 23, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Hooper, S.B.; Siew, M.L.; Kitchen, M.J.; te Pas, A.B. Establishing functional residual capacity in the non-breathing infant. Semin. Fetal Neonatal Med. 2013, 18, 336–343. [Google Scholar] [CrossRef]
- Hough, J.; Trojman, A.; Schibler, A. Effect of time and body position on ventilation in premature infants. Pediatr. Res. 2016, 80, 499–504. [Google Scholar] [CrossRef]
- Mughal, M.M.; Culver, D.A.; Minai, O.A.; Arroliga, A.C. Auto-positive end-expiratory pressure: Mechanisms and treatment. Cleve Clin. J. Med. 2005, 72, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, N.; Jalal, K.; McDonough, J.M.; Monk, H.M.; Zhang, H.; Jensen, E.; Dysart, K.C.; Kirpalani, H.M.; Panitch, H.B. Identifying and treating intrinsic PEEP in infants with severe bronchopulmonary dysplasia. Pediatr. Pulmonol. 2019, 54, 1045–1051. [Google Scholar] [CrossRef]
- Sella, N.; Pettenuzzo, T.; Zarantonello, F.; Andreatta, G.; De Cassai, A.; Schiavolin, C.; Simoni, C.; Pasin, L.; Boscolo, A.; Navalesi, P. Electrical impedance tomography: A compass for the safe route to optimal PEEP. Respir. Med. 2021, 187, 106555. [Google Scholar] [CrossRef] [PubMed]
- Bamat, N.; Fierro, J.; Wang, Y.; Millar, D.; Kirpalani, H. Positive end-expiratory pressure for preterm infants requiring conventional mechanical ventilation for respiratory distress syndrome or bronchopulmonary dysplasia. Cochrane Database Syst. Rev. 2019, 2, CD004500. [Google Scholar] [CrossRef]
- Lee, K.S.; Dunn, M.S.; Fenwick, M.; Shennan, A.T. A comparison of underwater bubble continuous positive airway pressure with ventilator-derived continuous positive airway pressure in premature neonates ready for extubation. Biol. Neonate. 1998, 73, 69–75. [Google Scholar] [CrossRef]
- Mian, Q.N.; Pichler, G.; Binder, C.; O’Reilly, M.; Aziz, K.; Urlesberger, B.; Cheung, P.Y.; Schmölzer, G.M. Tidal volumes in spontaneously breathing preterm infants supported with continuous positive airway pressure. J. Pediatr. 2014, 165, 702–706.e1. [Google Scholar] [CrossRef]
- Liew, Z.; Fenton, A.C.; Harigopal, S.; Gopalakaje, S.; Brodlie, M.; O’Brien, C.J. Physiological effects of high-flow nasal cannula therapy in preterm infants. Arch. Dis. Child Fetal Neonatal Ed. 2020, 105, F87–F93. [Google Scholar] [CrossRef]
- Kuttysankaran, R.; Athiraman, N.; Fenton, A.C.; Ramaiah, S.M. Does the use of nasal continuous positive airway pressure increase the risk of a significant pneumothorax in late preterm and term infants? Pediatr. Neonatol. 2017, 58, 469–470. [Google Scholar] [CrossRef] [PubMed]
- Jeng, M.J.; Lee, Y.S.; Tsao, P.C.; Soong, W.J. Neonatal air leak syndrome and the role of high-frequency ventilation in its prevention. J. Chin. Med. Assoc. 2012, 75, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Alexiou, S.; Panitch, H.B. Physiology of non-invasive respiratory support. Semin. Fetal Neonatal Med. 2016, 21, 174–180. [Google Scholar] [CrossRef]
- El-Farghali, O.G. High-flow nasal cannula in neonates. Respir. Care 2017, 62, 641–642. [Google Scholar] [CrossRef] [PubMed]
- Hough, J.L.; Johnston, L.; Brauer, S.G.; Woodgate, P.G.; Pham, T.M.T.; Schibler, A. Effect of body position on ventilation distribution in preterm infants on continuous positive airway pressure. Pediatr. Crit. Care Med. 2012, 13, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Becher, T.H.; Miedema, M.; Kallio, M.; Papadouri, T.; Karaoli, C.; Sophocleous, L.; Rahtu, M.; van Leuteren, R.W.; Waldmann, A.D.; Strodthoff, C.; et al. Prolonged Continuous Monitoring of Regional Lung Function in Infants with Respiratory Failure. Ann. Am. Thorac. Soc. 2022, 19, 991–999. [Google Scholar] [CrossRef]
- Lupton-Smith, A.; Argent, A.; Rimensberger, P.; Frerichs, I.; Morrow, B. Prone positioning improves ventilation homogeneity in children with acute respiratory distress syndrome. Pediatr. Crit. Care Med. 2017, 18, e229–e234. [Google Scholar] [CrossRef]
- Li, R.; Wu, Y.; Zhang, H.; Wang, A.; Zhao, X.; Yuan, S.; Yang, L.; Zou, X.; Shang, Y.; Zhao, Z. Effects of airway pressure release ventilation on lung physiology assessed by electrical impedance tomography in patients with early moderate-to-severe ARDS. Crit. Care 2023, 27, 178. [Google Scholar] [CrossRef]
- Taenaka, H.; Yoshida, T.; Hashimoto, H.; Firstiogusran, A.M.F.; Ishigaki, S.; Iwata, H.; Enokidani, Y.; Ebishima, H.; Kubo, N.; Koide, M.; et al. Personalized ventilatory strategy based on lung recruitablity in COVID-19-associated acute respiratory distress syndrome: A prospective clinical study. Crit. Care 2023, 27, 152. [Google Scholar] [CrossRef] [PubMed]
- Brandt, J.B.; Mahlknecht, A.; Werther, T.; Ullrich, R.; Hermon, M. Comparing ventilation modes by electrical impedance segmentography in ventilated children. J. Clin. Monit. Comput. 2022, 36, 1795–1803. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, S.; Leonhardt, S.; Ngo, C.; Bergmann, L.; Schrading, S.; Heimann, K.; Wagner, N.; Tenbrock, K. Electrical impedance tomography as possible guidance for individual positioning of patients with multiple lung injury. Clin. Respir. J. 2018, 12, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Riedel, T.; Kyburz, M.; Latzin, P.; Thamrin, C.; Frey, U. Regional and overall ventilation inhomogeneities in preterm and term-born infants. Intensive Care Med. 2009, 35, 144–151. [Google Scholar] [CrossRef]
- van Dijk, J.; Koopman, A.A.; Blokpoel, R.G.T.; Dijkstra, S.; Markhorst, D.G.; Burgerhof, J.G.; Kneyber, M.C. Global and Regional Tidal Volume Distribution in Spontaneously Breathing Mechanically Ventilated Children. Respir. Care 2022, 67, 383–393. [Google Scholar] [CrossRef]
- Armstrong, R.K.; Carlisle, H.R.; Davis, P.G.; Schibler, A.; Tingay, D.G. Distribution of tidal ventilation during volume-targeted ventilation is variable and influenced by age in the preterm lung. Intensive Care Med. 2011, 37, 839–846. [Google Scholar] [CrossRef]
- Romantsik, O.; Calevo, M.G.; Bruschettini, M. Head midline position for preventing the occurrence or extension of germinal matrix-intraventricular haemorrhage in preterm infants. Cochrane Database Syst. Rev. 2020, 7, CD012362. [Google Scholar] [CrossRef]
- Heinrich, S.; Schiffmann, H.; Frerichs, A.; Klockgether-Radke, A.; Frerichs, I. Body and head position effects on regional lung ventilation in infants: An electrical impedance tomography study. Intensive Care Med. 2006, 32, 1392–1398. [Google Scholar] [CrossRef]
- Koong Shiao, S.Y.P.; Brooker, J.; DiFiore, T. Desaturation events during oral feedings with and without a nasogastric tube in very low birth weight infants. Heart Lung 1996, 25, 236–245. [Google Scholar] [CrossRef]
- Spinelli, E.; Mauri, T.; Fogagnolo, A.; Scaramuzzo, G.; Rundo, A.; Grieco, D.L.; Grasselli, G.; Volta, C.A.; Spadaro, S. Electrical impedance tomography in perioperative medicine: Careful respiratory monitoring for tailored interventions. BMC Anesthesiol. 2019, 19, 140. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cohort (72) | Invasive (16) | Non-Invasive (56) | p-Value | |
|---|---|---|---|---|
| Postnatal age (days) | 6.0 (4.75) | 6 (6.5) | 6 (4) | NS |
| Gestational age (weeks) | 28.3 (±2.2) | 27.27 (±2.6) | 28.68 (±2.0) | NS |
| Birthweight (g) | 1089.9 (±268) | 1016.7 (±283) | 1117.2 (±261) | NS |
| Weight at the time of study (g) | 1101.3 (±234) | 1066.4 (±223) | 1114.2 (±240) | NS |
| Male (n/%) | 35 (48.61%) | 8 (50%) | 27 (48.21%) | NS |
| Inborn (n/%) | 72 (100%) | 16 (100%) | 56 (100%) | NS |
| Apgar score (1 min) | 8 (2.0) | 8 (3.0) | 8 (1.75) | NS |
| Apgar score (5 min) | 8 (1.0) | 8 (2.0) | 8 (1.0) | NS |
| Antenatal corticosteroids | NS | |||
| Complete (n/%) | 50 (69.44%) | 13 (81.25%) | 37 (66.07%) | |
| Incomplete (n/%) | 6 (8.33%) | 1 (6.25%) | 5 (8.93%) | |
| None (n/%) | 16 (22.22%) | 2 (12.5%) | 14 (25.0%) | |
| Chorioamnionitis (n/%) | 20 (27.77%) | 2 (12.5%) | 18 (32.14%) | NS |
| Resuscitation (n/%) | 19 (26.39%) | 4 (25.0%) | 15 (27.79%) | NS |
| Small for gestational age (n/%) | 13 (18.06%) | 1 (6.25%) | 12 (21.43%) | NS |
| Ductus arteriosus | ||||
| PDA (n/%) | 31 (43.05%) | 8 (50.0%) | 23 (41.07%) | NS |
| hsPDA (n/%) | 20 (27.78%) | 3 (18.75%) | 17 (30.36%) | NS |
| IVH | ||||
| Moderate (grade 1–2) (n/%) | 17 (23.61%) | 2 (12.5%) | 15 (26.78%) | NS |
| Severe (grade 3–4) (n/%) | 7 (9.72%) | 2 (12.5%) | 5 (8.93%) | NS |
| Surfactant (n/%) | 60 (83.33%) | 15 (93.75%) | 45 (80.36%) | NS |
| FiO2 | 0.21 (0.04) | 0.24 (0.07) | 0.21 (0.04) | NS |
| Respiratory rate | 48 (20) | 48 (14) | 50 (25.5) | NS |
| Hgb | 159.4 (±32.6) | 151 (±36.5) | 162.9 (±30.7) | NS |
| PLT | 290 (166) | 290 (130) | 293.5 (189.8) | NS |
| Hct | 45.2 (±8.8) | 42.7 (±10.0) | 46.2 (±8.2) | NS |
| pH | 7.354 (±0.05) | 7.351 (±0.05) | 7.355 (±0.05) | NS |
| pCO2 | 44.1 (±7.4) | 43.9 (±6.8) | 42.1 (±6.8) | NS |
| HCO3 | 23.4 (3.4) | 24.0 (5.5) | 23.4 (3.3) | NS |
| Lac | 2.0 (0.88) | 2.1 (±0.8) | 1.9 (0.6) | NS |
| Time (Min) | 0 | 30 | 60 | p-Value |
|---|---|---|---|---|
| Anterior distribution (% with lower and upper 95% CI in brackets) | ||||
| Invasive | 47.1 (43.9, 50.3) | 44.6 (41.4, 47.9) | 47.1 (43.6, 50.1) | p = 0.005 |
| Non-invasive | 41.4 (39.0, 44.0) | 40.2 (37.8, 42.6) | 41.5 (38.7, 43.9) | |
| Left distribution (% with lower and upper 95% CI in brackets) | ||||
| Invasive | 45.3 (42.6, 47.9) | 41.2 (38.4, 43.7) | 41.7 (39.1, 44.5) | p < 0.001 |
| Non-invasive | 47.3 (45.5, 49.7) | 48.8 (46.7, 50.7) | 47.1 (45.6, 49.9) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Virsilas, E.; Valiulis, A.; Kubilius, R.; Peciuliene, S.; Liubsys, A. Respiratory Support Effects over Time on Regional Lung Ventilation Assessed by Electrical Impedance Tomography in Premature Infants. Medicina 2024, 60, 494. https://doi.org/10.3390/medicina60030494
Virsilas E, Valiulis A, Kubilius R, Peciuliene S, Liubsys A. Respiratory Support Effects over Time on Regional Lung Ventilation Assessed by Electrical Impedance Tomography in Premature Infants. Medicina. 2024; 60(3):494. https://doi.org/10.3390/medicina60030494
Chicago/Turabian StyleVirsilas, Ernestas, Arunas Valiulis, Raimondas Kubilius, Skaiste Peciuliene, and Arunas Liubsys. 2024. "Respiratory Support Effects over Time on Regional Lung Ventilation Assessed by Electrical Impedance Tomography in Premature Infants" Medicina 60, no. 3: 494. https://doi.org/10.3390/medicina60030494