
Exploring the Mediating Role of Sleep Deficit-Related Functional Status in Subacute Stroke Survivors

 , , , ,
, , , ,  and
and
Abstract
:1. Background
2. Methods
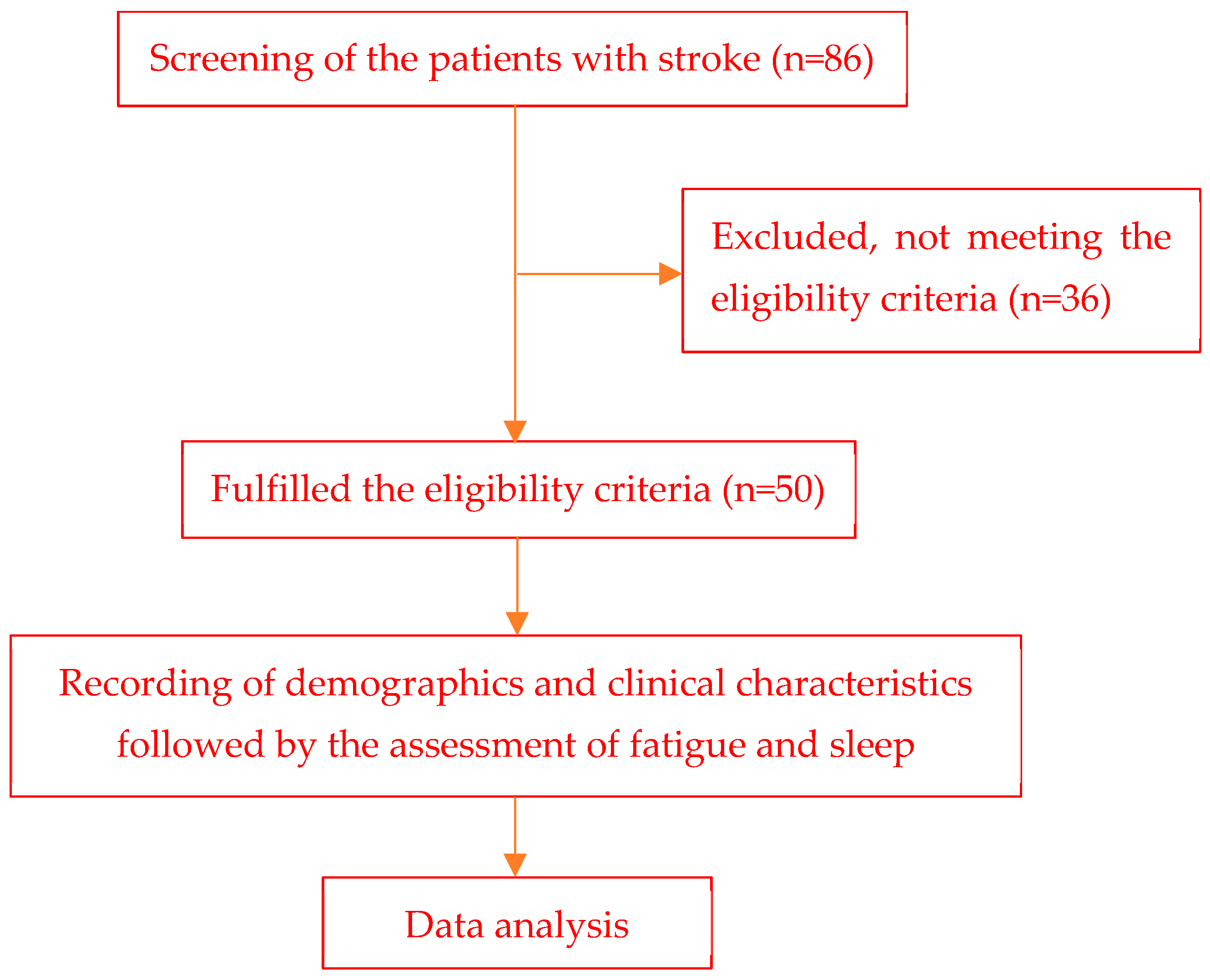
2.1. Participants, Design, and Setting
2.2. Study Protocol
2.3. Measures
2.3.1. Fatigue Severity Scale (FSS)
2.3.2. Epworth Sleepiness Scale (ESS)
2.3.3. Insomnia Severity Index (ISI)
2.3.4. Pittsburg Sleep Quality Index (PSQI)
2.3.5. Functional Outcomes of Sleep Questionnaire (FOSQ)
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PSF | Post-stroke fatigue |
| SFS | Sleepiness-related functional status |
| PSQI | Pittsburgh sleep quality index |
| ESS | Epworth sleepiness scale |
| ISI | Insomnia severity index |
| FOSQ | Functional outcome of the sleep questionnaire |
| FSS | Fatigue severity scale |
References
- Vassalli, A.; Dijk, D.J. Sleep function: Current questions and new approaches. Eur. J. Neurosci. 2009, 29, 1830–1841. [Google Scholar] [CrossRef]
- Miletínová, E.; Bušková, J. Functions of Sleep. Physiol. Res. 2021, 70, 177–182. [Google Scholar] [CrossRef]
- Medic, G.; Wille, M.; Hemels, M.E. Short- and long-term health consequences of sleep disruption. Nat. Sci. Sleep. 2017, 9, 151–161. [Google Scholar] [CrossRef]
- Sateia, M.J. International classification of sleep disorders-third edition: Highlights and modifications. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef]
- Baylan, S.; Griffiths, S.; Grant, N.; Broomfield, N.M.; Evans, J.J.; Gardani, M. Incidence and prevalence of post-stroke insomnia: A systematic review and meta-analysis. Sleep. Med. Rev. 2020, 49, 101222. [Google Scholar] [CrossRef]
- Eban-Rothschild, A.; Appelbaum, L.; de Lecea, L. Neuronal Mechanisms for Sleep/Wake Regulation and Modulatory Drive. Neuropsychopharmacology 2018, 43, 937–952. [Google Scholar] [CrossRef]
- Pasic, Z.; Smajlovic, D.; Dostovic, Z.; Kojic, B.; Selmanovic, S. Incidence and types of sleep disorders in patients with stroke. Med. Arh. 2011, 65, 225–227. [Google Scholar] [CrossRef]
- Staub, F.; Bogousslavsky, J. Fatigue after stroke: A major but neglected issue. Cerebrovasc. Dis. 2001, 12, 75–81. [Google Scholar] [CrossRef]
- Ormstad, H.; Aass, H.C.D.; Amthor, K.-F.; Lund-Sørensen, N.; Sandvik, L. Serum levels of cytokines, glucose, and hemoglobin as possible predictors of poststroke depression, and association with poststroke fatigue. Int. J. Neurosci. 2012, 122, 682–690. [Google Scholar] [CrossRef]
- Kuppuswamy, A.; Clark, E.V.; Turner, I.F.; Rothwell, J.C.; Ward, N.S. Post-stroke fatigue: A deficit in corticomotor excitability? Brain 2015, 138 Pt 1, 136–148. [Google Scholar] [CrossRef]
- Viana, B.F.; Santos, T.M.; Pires, F.O. TRADITIONAL MODELS OF FATIGUE AND PHYSICAL PERFORMANCE. J. Phys. Educ. 2018, 29, e2915. [Google Scholar]
- Cumming, T.B.; Packer, M.; Kramer, S.F.; English, C. The prevalence of fatigue after stroke: A systematic review and meta-analysis. Int. J. Stroke 2016, 11, 968–977. [Google Scholar] [CrossRef]
- Schepers, V.P.; Visser-Meily, A.M.; Ketelaar, M.; Lindeman, E. Poststroke fatigue: Course and its relation to personal and stroke-related factors. Arch. Phys. Med. Rehabil. 2006, 87, 184–188. [Google Scholar] [CrossRef]
- Maaijwee, N.A.; Arntz, R.M.; Rutten-Jacobs, L.C.; Schaapsmeerders, P.; Schoonderwaldt, H.C.; van Dijk, E.J.; de Leeuw, F.E. Post-stroke fatigue and its association with poor functional outcome after stroke in young adults. J. Neurol. Neurosurg. Psychiatry 2015, 86, 1120–1126. [Google Scholar] [CrossRef]
- Vincent-Onabajo, G.; Adamu, A. Impact of Poststroke Fatigue on Health-Related Quality of Life of Nigerian Stroke Survivors. J. Stroke 2014, 16, 195–201. [Google Scholar] [CrossRef]
- Hinkle, J.L.; Becker, K.J.; Kim, J.S.; Choi-Kwon, S.; Saban, K.L.; McNair, N.; Mead, G.E. Poststroke Fatigue: Emerging Evidence and Approaches to Management: A Scientific Statement for Healthcare Professionals From the American Heart Association. Stroke 2017, 48, e159–e170. [Google Scholar] [CrossRef]
- Fulk, G.D.; Boyne, P.; Hauger, M.; Ghosh, R.; Romano, S.; Thomas, J.; Slutzky, A.; Klingman, K. The Impact of Sleep Disorders on Functional Recovery and Participation Following Stroke: A Systematic Review and Meta-Analysis. Neurorehabil Neural Repair. 2020, 34, 1050–1061. [Google Scholar] [CrossRef]
- Richiardi, L.; Bellocco, R.; Zugna, D. Mediation analysis in epidemiology: Methods, interpretation and bias. Int. J. Epidemiol. 2013, 42, 1511–1519. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Fortier-Brochu, E.; Beaulieu-Bonneau, S.; Ivers, H.; Morin, C.M. Relations between sleep, fatigue, and health-related quality of life in individuals with insomnia. J. Psychosom. Res. 2010, 69, 475–483. [Google Scholar] [CrossRef]
- Kim, J.; Kim, Y.; Yang, K.I.; Kim, D.E.; Kim, S.A. The Relationship Between Sleep Disturbance and Functional Status in Mild Stroke Patients. Ann. Rehabil. Med. 2015, 39, 545–552. [Google Scholar] [CrossRef]
- Sonmez, I.; Karasel, S. Poor Sleep Quality I Related to Impaired Functional Status Following Stroke. J. Stroke Cerebrovasc. Dis. 2019, 28, 104349. [Google Scholar] [CrossRef]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef]
- Cumming, T.B.; Mead, G. Classifying post-stroke fatigue: Optimal cut-off on the Fatigue Assessment Scale. J. Psychosom. Res. 2017, 103, 147–149. [Google Scholar] [CrossRef]
- Valko, P.O.; Bassetti, C.L.; Bloch, K.E.; Held, U.; Baumann, C.R. Validation of the fatigue severity scale in a Swiss cohort. Sleep 2008, 31, 1601–1607. [Google Scholar] [CrossRef]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef]
- Manzar, M.D.; Salahuddin, M.; Alamri, M.; Albougami, A.; Khan, M.Y.A.; Nureye, D.; Spence, D.W.; Pandi-Perumal, S.R. Psychometric properties of the Epworth sleepiness scale in Ethiopian university students. Health Qual. Life Outcomes 2019, 17, 30. [Google Scholar] [CrossRef]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Morin, C.M. Insomnia: Psychological Assessment and Management; Guilford Press: New York City, NY, USA, 1993. [Google Scholar]
- Manzar, M.D.; Jahrami, H.A.; Bahammam, A.S. Structural validity of the Insomnia Severity Index: A systematic review and meta-analysis. Sleep Med. Rev. 2021, 60, 101531. [Google Scholar] [CrossRef]
- Mamun, M.A.; Alimoradi, Z.; Gozal, D.; Manzar, M.D.; Broström, A.; Lin, C.Y.; Huang, R.Y.; Pakpour, A.H. Validating Insomnia Severity Index (ISI) in a Bangladeshi Population: Using Classical Test Theory and Rasch Analysis. Int. J. Environ. Res. Public. Health 2021, 19, 225. [Google Scholar] [CrossRef]
- Albougami, A.; Manzar, M.D. Insomnia severity index: A psychometric investigation among Saudi nurses. Sleep Breath. 2019, 23, 987–996. [Google Scholar] [CrossRef]
- Chasens, E.R.; Ratcliffe, S.J.; Weaver, T.E. Development of the FOSQ-10: A short version of the Functional Outcomes of Sleep Questionnaire. Sleep 2009, 32, 915–919. [Google Scholar] [CrossRef]
- Weaver, T.E.; Laizner, A.M.; Evans, L.K.; Maislin, G.; Chugh, D.K.; Lyon, K.; Smith, P.L.; Schwartz, A.R.; Redline, S.; Pack, A.I.; et al. An instrument to measure functional status outcomes for disorders of excessive sleepiness. Sleep 1997, 20, 835–843. [Google Scholar]
- Zhao, X.; Lynch, J.G., Jr.; Chen, Q. Reconsidering Baron and Kenny: Myths and Truths about Mediation Analysis. J. Consum. Res. 2010, 37, 197–206. [Google Scholar] [CrossRef]
- Baron, R.; Kenny, D. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Hayes, A.F. The PROCESS Macro for SPSS and SAS (Version 2.13) [Software]; Guilford: New York, NY, USA, 2013. [Google Scholar]
- Preacher, K.; Hayes, A. SPSS and SAS Procedures for Estimating Indirect Effects in Simple Mediation Models. Behav. Res. Methods Instrum. Comput. A J. Psychon. Soc. Inc. 2004, 36, 717–731. [Google Scholar] [CrossRef]
- Zhang, S.; Cheng, S.; Zhang, Z.; Wang, C.; Wang, A.; Zhu, W. Related risk factors associated with post-stroke fatigue: A systematic review and meta-analysis. Neurol. Sci. 2021, 42, 1463–1471. [Google Scholar] [CrossRef]
- Leppävuori, A.; Pohjasvaara, T.; Vataja, R.; Kaste, M.; Erkinjuntti, T. Insomnia in ischemic stroke patients. Cerebrovasc. Dis. 2002, 14, 90–97. [Google Scholar] [CrossRef]
- Kojic, B.; Dostovic, Z.; Vidovic, M.; Ibrahimagic, O.C.; Hodzic, R.; Iljazovic, A. Sleep Disorders in Acute Stroke. Mater. Sociomed. 2022, 34, 14–24. [Google Scholar] [CrossRef]
- Sterr, A.; Kuhn, M.; Nissen, C.; Ettine, D.; Funk, S.; Feige, B.; Umarova, R.; Urbach, H.; Weiller, C.; Riemann, D. Post-stroke insomnia in community-dwelling patients with chronic motor stroke: Physiological evidence and implications for stroke care. Sci. Rep. 2018, 8, 8409. [Google Scholar] [CrossRef]
- Byun, E.; Kohen, R.; Becker, K.J.; Kirkness, C.J.; Khot, S.; Mitchell, P.H. Stroke impact symptoms are associated with sleep-related impairment. Heart Lung 2020, 49, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Goldman, S.E.; Ancoli-Israel, S.; Boudreau, R.; Cauley, J.A.; Hall, M.; Stone, K.L.; Rubin, S.M.; Satterfield, S.; Simonsick, E.M.; Newman, A.B. Sleep problems and associated daytime fatigue in community-dwelling older individuals. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 1069–1075. [Google Scholar] [CrossRef] [PubMed]
- Hawker, G.A.; French, M.R.; Waugh, E.J.; Gignac, M.A.; Cheung, C.; Murray, B.J. The multidimensionality of sleep quality and its relationship to fatigue in older adults with painful osteoarthritis. Osteoarthr. Cartil. 2010, 18, 1365–1371. [Google Scholar] [CrossRef] [PubMed]
- Tomar, S.; Sharma, A.; Jain, A.; Sinha, V.D.; Gupta, I.D. Study of Fatigue and Associated Factors in Traumatic Brain Injury and Its Correlation with Insomnia and Depression. Asian J. Neurosurg. 2018, 13, 1061–1065. [Google Scholar] [CrossRef] [PubMed]
- Englander, J.; Bushnik, T.; Oggins, J.; Katznelson, L. Fatigue after traumatic brain injury: Association with neuroendocrine, sleep, depression and other factors. Brain Inj. 2010, 24, 1379–1388. [Google Scholar] [CrossRef] [PubMed]
- Kotterba, S.; Neusser, T.; Norenberg, C.; Bussfeld, P.; Glaser, T.; Dörner, M.; Schürks, M. Sleep quality, daytime sleepiness, fatigue, and quality of life in patients with multiple sclerosis treated with interferon beta-1b: Results from a prospective observational cohort study. BMC Neurol. 2018, 18, 123. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y.; Chun, M.H.; Kang, S.H.; Lee, J.A.; Kim, B.R.; Shin, M.J. Functional outcome in poststroke patients with or without fatigue. Am. J. Phys. Med. Rehabil. 2009, 88, 554–558. [Google Scholar] [CrossRef]
- Ponchel, A.; Bombois, S.; Bordet, R.; Hénon, H. Factors Associated with Poststroke Fatigue: A Systematic Review. Stroke Res. Treat. 2015, 2015, 347920. [Google Scholar] [CrossRef]
- Korostovtseva, L. Ischemic Stroke and Sleep: The Linking Genetic Factors. Cardiol. Ther. 2021, 10, 349–375. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Mean ± SD |
|---|---|
| Age (years) | 51.840 ± 7.03 |
| Gender (M/F) | 38/12 |
| Height (cm) | 167.44 ± 6.70 |
| Weight (kg) | 70.620 ± 8.13 |
| BMI (kg/m2) | 25.210 ± 2.73 |
| SBP (mmHg) | 134.800 ± 10.73 |
| DBP (mmHg) | 82.900 ± 5.35 |
| MMSE score | 26.740 ± 1.84 |
| Type of stroke (n, n%) | |
| Ischemic | 39 (78) |
| Hemorrhagic | 11 (22) |
| Type of stroke syndrome (n, n%) | |
| Anterior cerebral artery | 9 (18) |
| Middle cerebral artery | 36 (72) |
| Posterior cerebral artery | 3 (6) |
| Lacunar syndrome | 2 (4) |
| Side of cerebrovascular accident (n, n%) | |
| Left | 26 (52) |
| Right | 24 (48) |
| Variable | Mean ± SD |
|---|---|
| FSS | 3.82 ± 1.71 |
| ESS | 11.46 ± 5.87 |
| ISI | 11.78 ± 6.94 |
| PSQI | 7.58 ± 3.64 |
| FOSQ | 16.60 ± 2.98 |
| Variables | FSS | |
|---|---|---|
| ρ | p | |
| ESS | 0.419 | 0.002 |
| ISI | 0.719 | 0.000 |
| PSQI | 0.586 | 0.000 |
| FOSQ | −0.516 | 0.000 |
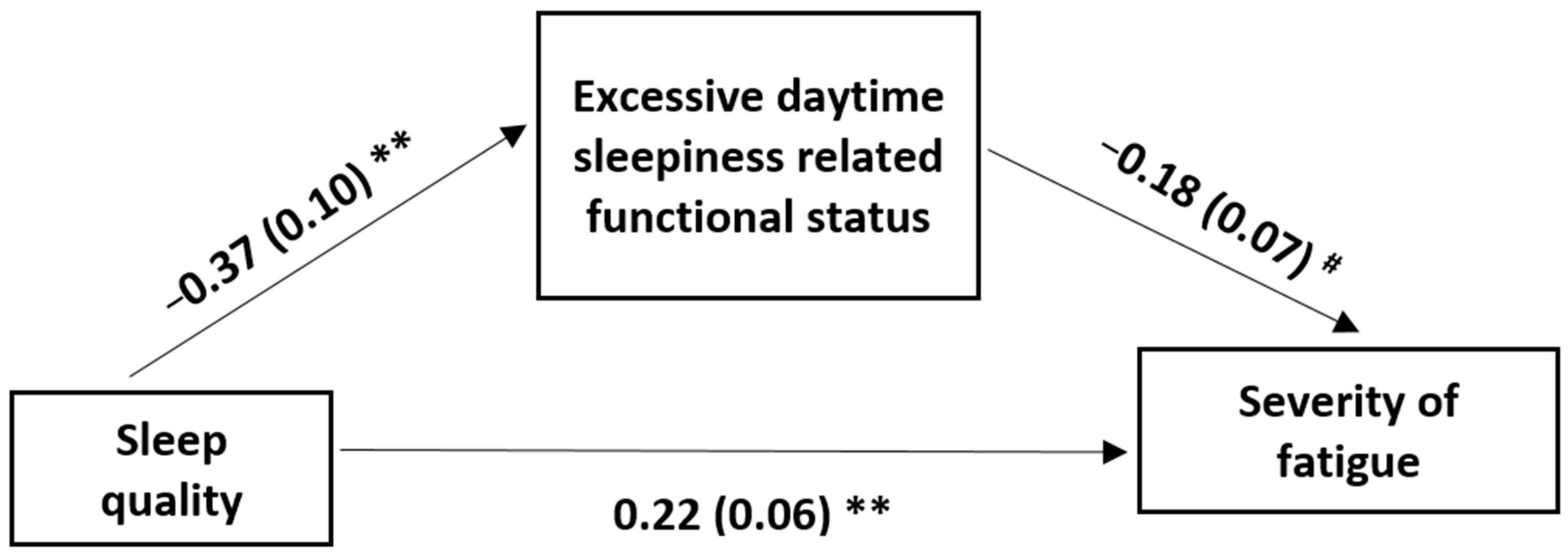
| Independent Variable | Outcome Variable | β | b | SE | 95% Bootstrapping CI | p Value | |
|---|---|---|---|---|---|---|---|
| LL | UL | ||||||
| Sleep Quality | Sleep deficit-related functional loss | −0.46 | −0.37 | 0.10 | −0.58 | −0.16 | <0.001 |
| Sleep deficit-related functional loss | Severity of fatigue | −0.31 | −0.18 | 0.07 | −0.32 | −0.03 | 0.016 |
| Sleep quality (direct effect) | Severity of fatigue | 0.46 | 0.22 | 0.06 | 0.10 | 0.33 | <0.001 |
| Types of Effect | b | SE | 95% Bootstrapping CI | p Value | |||
| LL | UL | ||||||
| Total effect | 0.28 | 0.05 | 0.17 | 0.39 | <0.001 | ||
| Indirect effect | 0.07 | 0.03 | 0.01 | 0.13 | - | ||
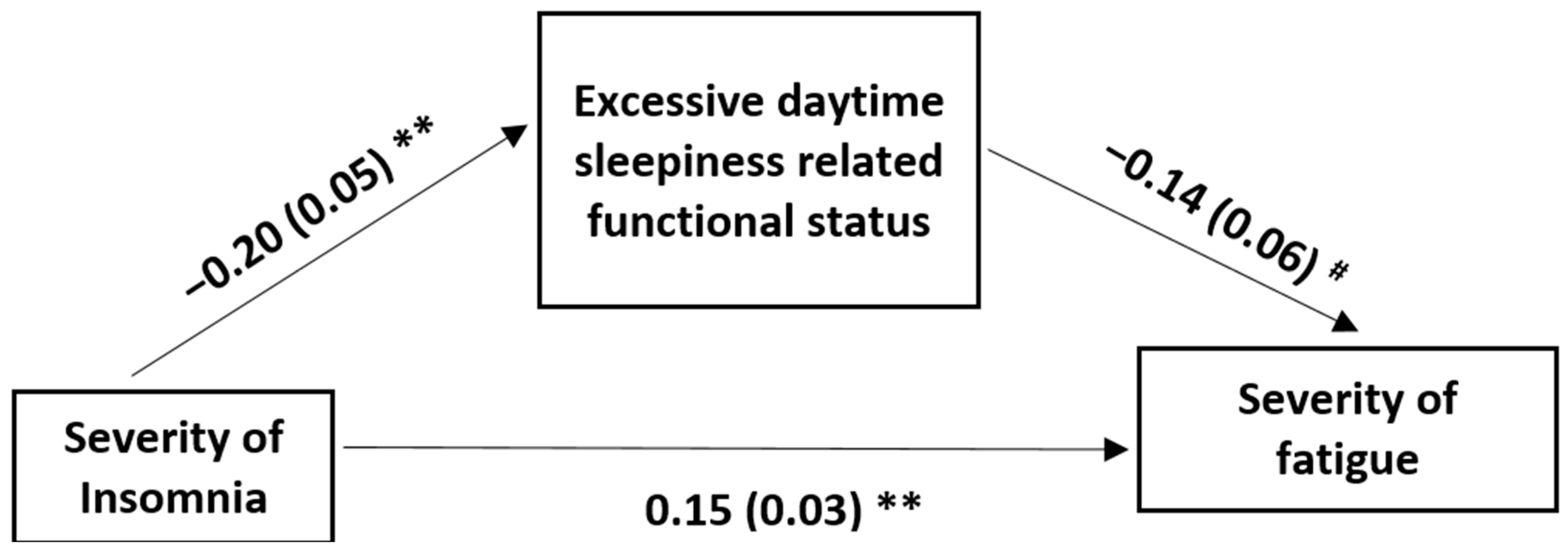
| Independent Variable | Outcome Variable | β | b | SE | 95% Bootstrapping CI | p Value | |
|---|---|---|---|---|---|---|---|
| LL | UL | ||||||
| Severity of insomnia | Sleep deficit-related functional loss | −0.46 | −0.20 | 0.05 | −0.31 | −0.09 | <0.001 |
| Sleep deficit-related functional loss | Severity of fatigue | −0.24 | −0.14 | 0.06 | −0.26 | −0.01 | 0.036 |
| Severity of insomnia (direct effect) | Severity of fatigue | 0.60 | 0.15 | 0.03 | 0.10 | 0.20 | <0.001 |
| Types of Effect | b | SE | 95% Bootstrapping CI | p Value | |||
| LL | UL | ||||||
| Total effect | 0.18 | 0.02 | 0.13 | 0.23 | <0.001 | ||
| Indirect effect | 0.03 | 0.02 | 0.002 | 0.06 | - | ||
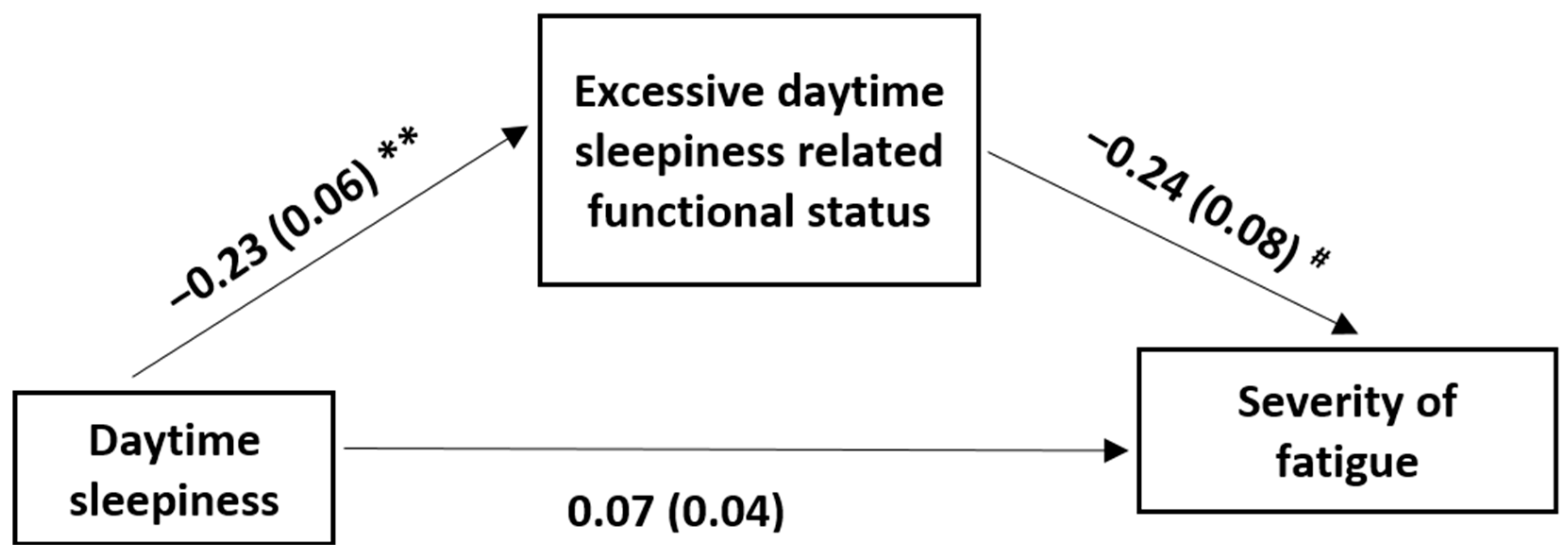
| Independent Variable | Outcome Variable | β | b | SE | 95% Bootstrapping CI | p Value | |
|---|---|---|---|---|---|---|---|
| LL | UL | ||||||
| Daytime sleepiness | Sleep deficit-related functional loss | −0.45 | −0.23 | 0.06 | −0.36 | −0.10 | <0.001 |
| Sleep deficit-related functional loss | Severity of fatigue | −0.41 | −0.24 | 0.08 | −0.39 | −0.08 | 0.016 |
| Daytime sleepiness (direct effect) | Severity of fatigue | 0.23 | 0.07 | 0.04 | −0.01 | 0.15 | 0.092 |
| Types of Effect | b | SE | 95% Bootstrapping CI | p Value | |||
| LL | UL | ||||||
| Total effect | 0.12 | 0.04 | 0.05 | 0.20 | 0.002 | ||
| Indirect effect | 0.05 | 0.02 | 0.01 | 0.10 | - | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumar, S.; Parveen, S.; Manzar, M.D.; Alghadir, A.H.; Khan, M.; Al-Quliti, K.W.; Spence, D.W.; Pandi-Perumal, S.R.; Bahammam, A.S.; Noohu, M.M. Exploring the Mediating Role of Sleep Deficit-Related Functional Status in Subacute Stroke Survivors. Medicina 2024, 60, 422. https://doi.org/10.3390/medicina60030422
Kumar S, Parveen S, Manzar MD, Alghadir AH, Khan M, Al-Quliti KW, Spence DW, Pandi-Perumal SR, Bahammam AS, Noohu MM. Exploring the Mediating Role of Sleep Deficit-Related Functional Status in Subacute Stroke Survivors. Medicina. 2024; 60(3):422. https://doi.org/10.3390/medicina60030422
Chicago/Turabian StyleKumar, Sunil, Sarah Parveen, Md Dilshad Manzar, Ahmad H. Alghadir, Masood Khan, Khalid Wasel Al-Quliti, David Warren Spence, Seithikurippu R. Pandi-Perumal, Ahmed S. Bahammam, and Majumi M. Noohu. 2024. "Exploring the Mediating Role of Sleep Deficit-Related Functional Status in Subacute Stroke Survivors" Medicina 60, no. 3: 422. https://doi.org/10.3390/medicina60030422