
Use of Lung Ultrasound in Reducing Radiation Exposure in Neonates with Respiratory Distress: A Quality Management Project
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample and Variables Analyzed
2.2. Quality Management Project Design
- -
- All the doctors of the units have been trained in the use and interpretation of lung ultrasound.
- -
- A protocol for the performance of the imaging procedures has been established (Table 1)—also with training the staff for its use.
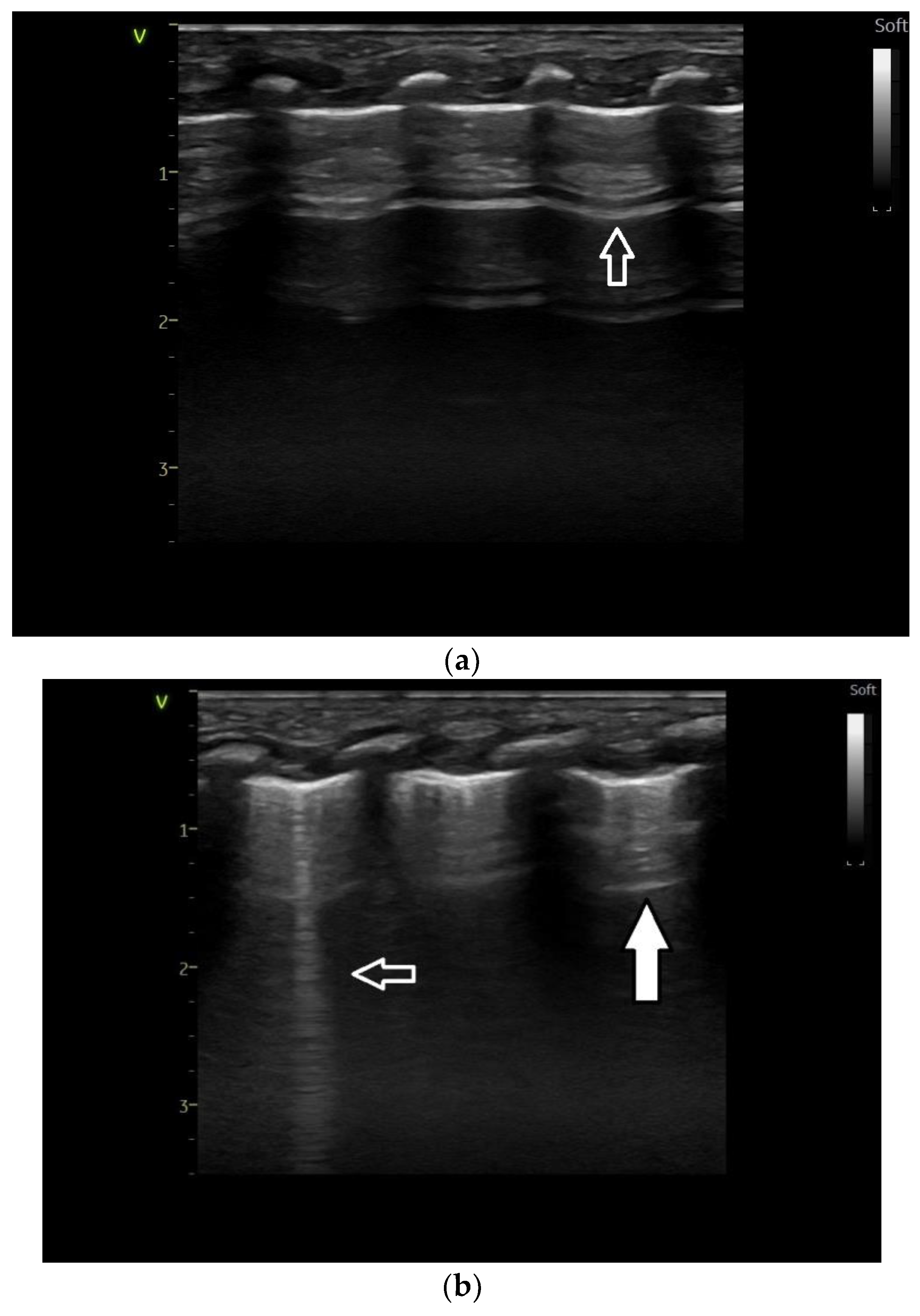
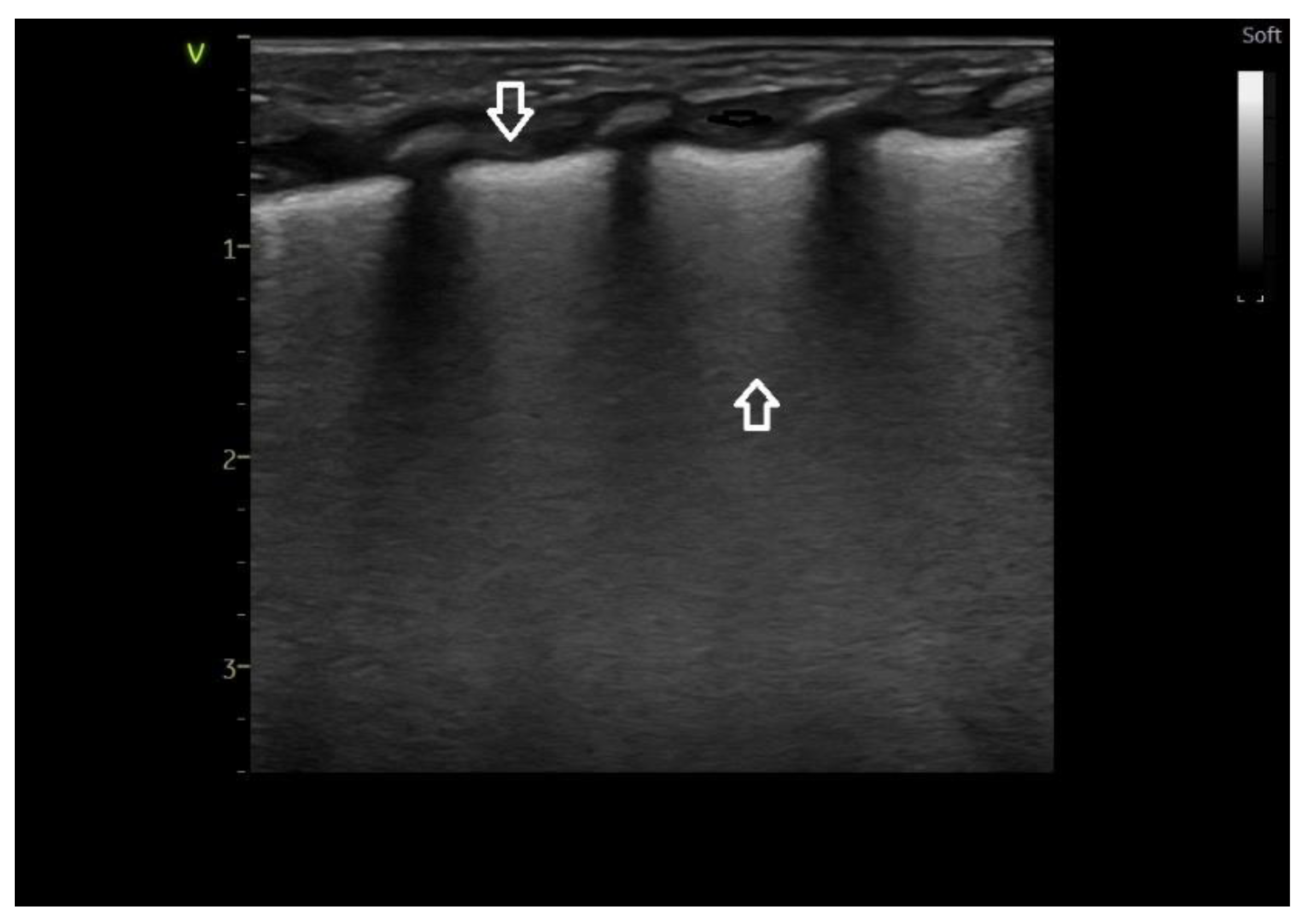
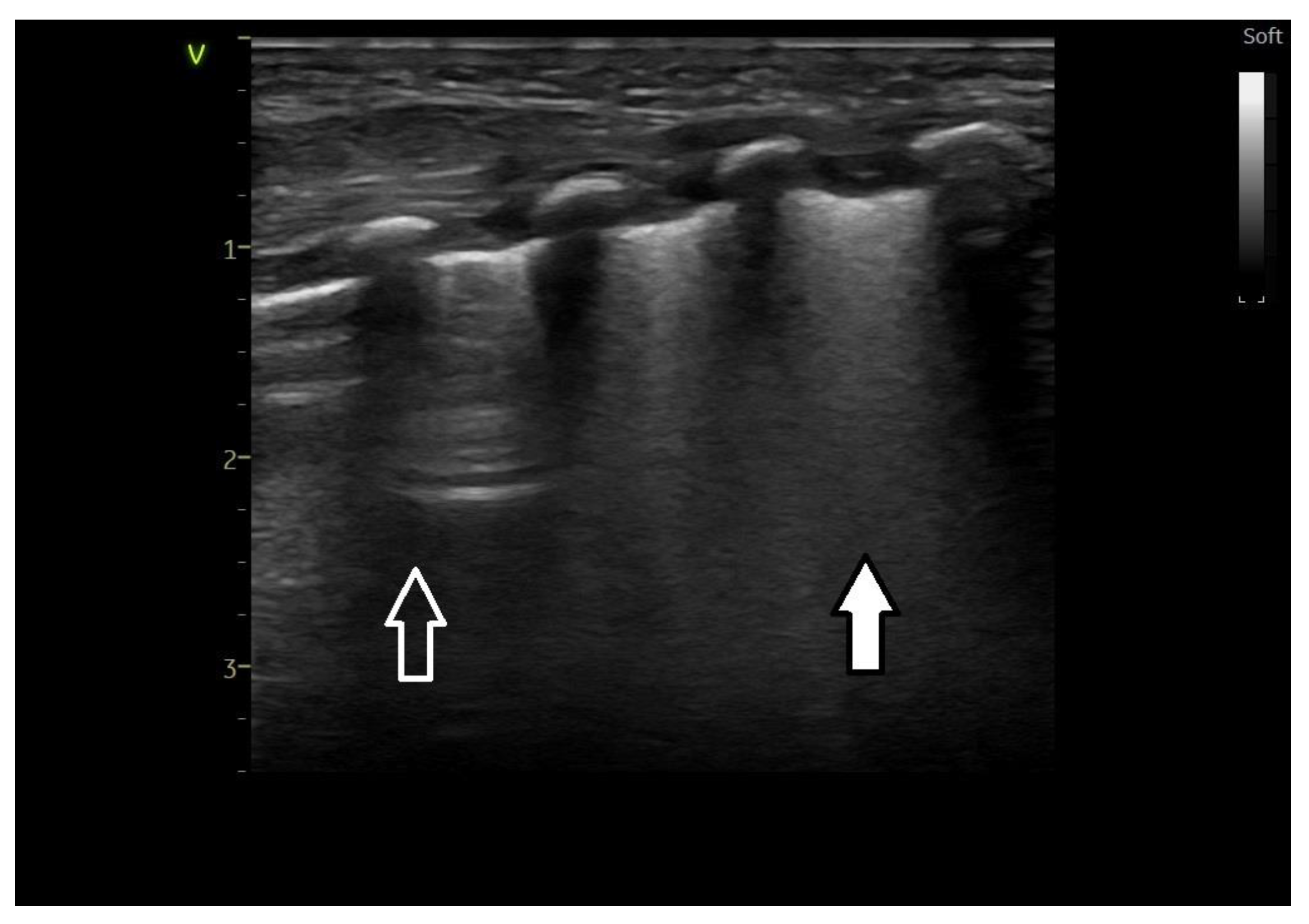
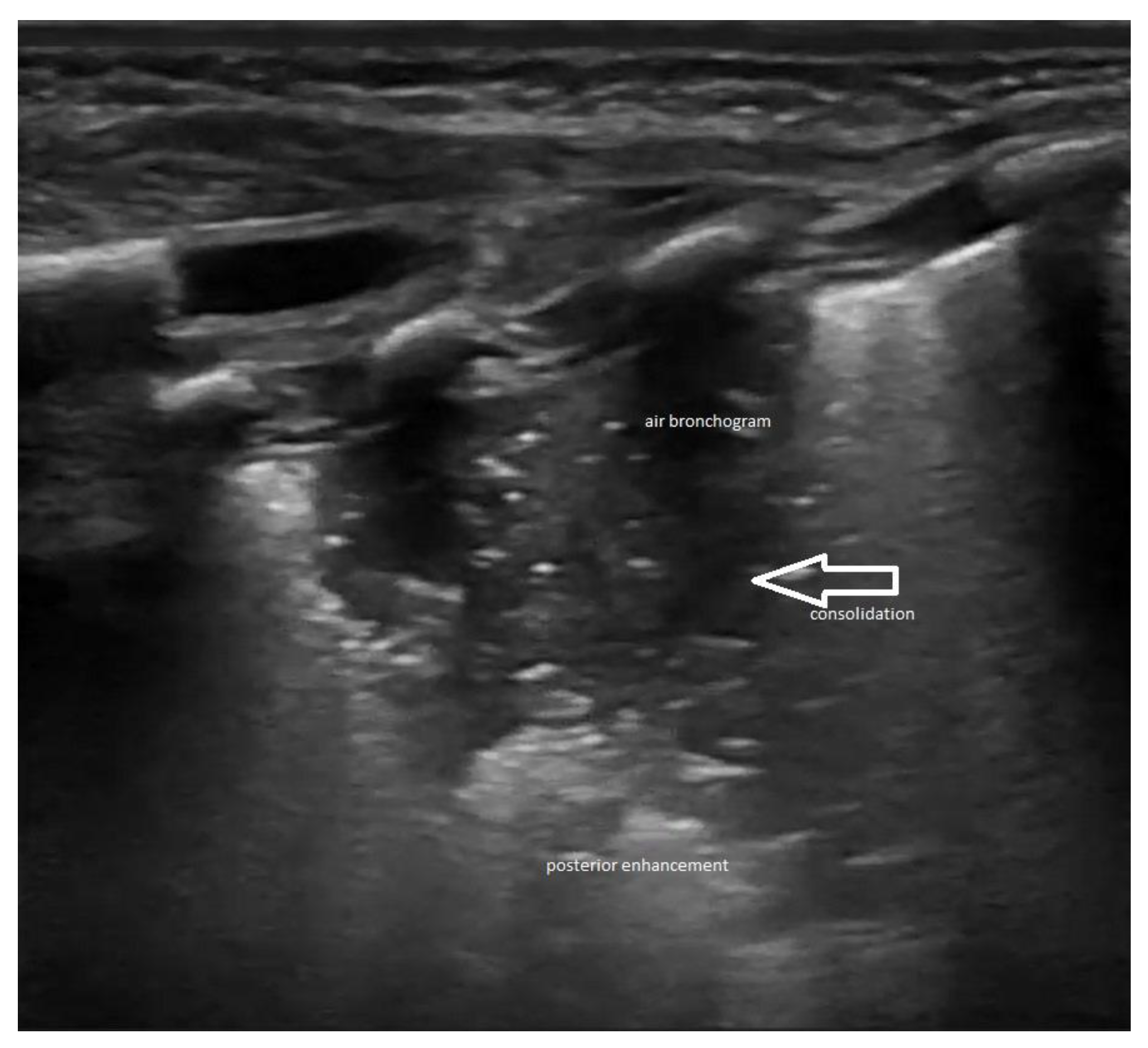
2.3. Lung Ultrasound Criteria/Findings
2.4. Statistics
3. Results
3.1. Correlations by Year of Study
3.2. Correlations between X-rays and Categories of Treatment Applied to Patients
4. Discussion
- -
- -
- The cost of an MRI in the NICU is far greater than the cost of a MRI, and this is not a technique to be used yet in all the neonates.
- -
- The aim of our project has been to decrease the use of the X-rays by using simple diagnostic and assessment methods, like clinical examination, history, blood gases and ultrasound, and MRI is obviously not a simple technique to be used in all the settings.
- -
- Although MRI is a promising and very accurate technique for the assessment of neonatal lungs, it is not yet passed into usual clinical practice, and it is not mentioned in the RDS guidelines like X-rays and ultrasound. Accordingly, since our goal has been to provide a model to be simple and replicated in all the units, we did not include lung MRI in our assessment protocol.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANOVA | analysis of variance |
| CPAP | continuous positive airway pressure |
| ET tube | endotracheal tube |
| Gy | Gray |
| HFOV | High-frequency oscillatory ventilation |
| H2O | water |
| IPPV | intermittent positive pressure ventilation |
| LU | lung ultrasound |
| MHz | megahertz |
| N | number |
| NICU | neonatal intensive care unit |
| NY | New York |
| RD | respiratory distress |
| RDS | respiratory distress syndrome |
| SIMV | synchronized intermittent mandatory ventilation |
| TTN | transient tachypnea of the newborn |
| WI | Wisconsin |
| Vs | versus |
| X-rays | radiograph |
References
- Rachuri, H.; Oleti, T.P.; Murki, S.; Subramanian, S.; Nethagani, J. Diagnostic Performance of Point of Care Ultrasonography in Identifying the Etiology of Respiratory Distress in Neonates. Indian J. Pediatr. 2017, 84, 267–270. [Google Scholar] [CrossRef]
- Liu, J.; Chen, X.X.; Li, X.W.; Chen, S.W.; Wang, Y.; Fu, W. Lung ultrasonography to diagnose transient tachypnea of the newborn. Chest 2016, 149, 1269–1275. [Google Scholar] [CrossRef]
- Ammirabile, A.; Buonsenso, D.; Di Mauro, A. Lung Ultrasound in Pediatrics and Neonatology: An Update. Healthcare 2021, 9, 1015. [Google Scholar] [CrossRef]
- Sweet, D.G.; Carnielli, V.P.; Greisen, G.; Hallman, M.; Klebermass-Schrehof, K.; Ozek, E.; Pas, A.T.; Plavka, R.; Roehr, C.C.; Saugstad, O.D.; et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome: 2022 Update. Neonatology 2023, 120, 3–23. [Google Scholar] [CrossRef]
- Don, S.; Whiting, B.R.; Rutz, L.J.; Apgar, B.K. New exposure indicators for digital radiography simplified for radiologists and technologists. Am. J. Roentgenol. 2012, 199, 1337–1341. [Google Scholar] [CrossRef]
- Makri, T.; Yakoumakis, E.; Papadopoulou, D.; Gialousis, G.; Theodoropoulos, V.; Sandilos, P.; Georgiou, E. Radiation risk assessment in neonatal radiographic examinations of the chest and abdomen: A clinical and Monte Carlo dosimetry study. Phys. Med. Biol. 2006, 51, 5023–5033. [Google Scholar] [CrossRef]
- Raimondi, F.; Yousef, N.; Rodriguez Fanjul, J.; De Luca, D.; Corsini, I.; Shankar-Aguilera, S.; Dani, C.; Di Guardo, V.; Lama, S.; Mosca, F.; et al. A multicenter lung ultrasound study on transient tachypnea of the neonate. Neonatology 2019, 115, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Raimondi, F.; Migliaro, F.; Corsini, I.; Meneghin, F.; Dolce, P.; Pierri, L.; Perri, A.; Aversa, S.; Nobile, S.; Lama, S.; et al. Lung Ultrasound Score Progress in Neonatal Respiratory Distress Syndrome. Pediatrics 2021, 147, e2020030528. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.-Q.; Qiu, R.-X.; Liu, J.; Zhang, L.; Ren, X.-L.; Qin, S.-J. Lung ultrasound completely replaced chest X-ray for diagnosing neonatal lung diseases: A 3-year clinical practice report from a neonatal intensive care unit in China. J. Matern.-Fetal Neonatal Med. 2020, 35, 3565–3572. [Google Scholar] [CrossRef] [PubMed]
- Poerio, A.; Galletti, S.; Baldazzi, M.; Martini, S.; Rollo, A.; Spinedi, S.; Raimondi, F.; Zompatori, M.; Corvaglia, L.; Aceti, A. Lung ultrasound features predict admission to the neonatal intensive care unit in infants with transient neonatal tachypnoea or respiratory distress syndrome born by caesarean section. Eur. J. Pediatr. 2020, 180, 869–876. [Google Scholar] [CrossRef] [PubMed]
- Raimondi, F.; Migliaro, F.; Corsini, I.; Meneghin, F.; Pierri, L.; Salomè, S.; Perri, A.; Aversa, S.; Nobile, S.; Lama, S.; et al. Neonatal Lung Ultrasound and Surfactant Administration. Chest 2021, 160, 2178–2186. [Google Scholar] [CrossRef] [PubMed]
- Riccabona, M. (Ed.) Pediatric Ultrasound: Requisites and Applications, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Liu, J.; Wang, Y.; Fu, W.; Yang, C.S.; Huang, J.J. The ‘Double Lung Point’: An Ultrasound Sign Diagnostic of Transient Tachypnea of the New-born. Medicine 2014, 91, e197–e202. [Google Scholar] [CrossRef] [PubMed]
- Corsini, I.; Parri, N.; Gozzini, E.; Coviello, C.; Leonardi, V.; Poggi, C.; Giacalone, M.; Bianconi, T.; Tofani, L.; Raimondi, F.; et al. Lung Ultrasound for the Differential Diagnosis of Respiratory Distress in Neonates. Neonatology 2018, 115, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Volpicelli, G.; Elbarbary, M.; Blaivas, M.; Lichtenstein, D.A.; Mathis, G.; Kirkpatrick, A.W.; Melniker, L.; Gargani, L.; Noble, V.E.; Via, G.; et al. International evidence-based recommendations for point of care lung ultrasound. Intensive Care Med. 2012, 38, 577–591. [Google Scholar] [CrossRef] [PubMed]
- Vergine, M.; Copetti, R.; Brusa, G.; Cattarossi, L. Lung Ultrasound Accuracy in Respiratory Distress Syndrome and Transient Tachypnea of the Newborn. Neonatology 2014, 106, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Ma, H.-R.; Fu, W. Lung Ultrasound to Diagnose Pneumonia in Neonates with Fungal Infection. Diagnostics 2022, 12, 1776. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Sterne, J.A.C. Chapter 8: Assessing risk of bias in included studies. In Cochrane Handbook for Systematic Reviews of Interventions Version 5.2.0 (Updated June 2017); Higgins, J.P.T., Churchill, R., Chandler, J., Cumpston, M.S., Eds.; Cochrane: Hoboken, NJ, USA, 2017. [Google Scholar]
- Ognean, L. (Ed.) Managementul Sindromului de Detresă Respiratorie Prin Deficit de Surfactant; Asociaţia de Neonatologie din România: Bucharest, Romania, 2023. [Google Scholar]
- Boiculese, L.V.; Dascalu, C. Informatica Medicala; Editura Venus: Bucuresti, Romania, 2001. [Google Scholar]
- Raimondi, F.; Migliaro, F.; Sodano, A.; Ferrara, T.; Lama, S.; Vallone, G.; Capasso, L. Use of neonatal chest ultrasound to predict noninvasive ventilation failure. Pediatrics 2014, 134, e1089–e1094. [Google Scholar] [CrossRef]
- Lichtenstein, D.A.; Mauriat, P. Lung ultrasound in the critically ill neonate. Curr. Pediatr. Rev. 2012, 8, 217–223. [Google Scholar] [CrossRef]
- Gislason-Lee, A.J. Patient X-ray Exposure and ALARA in the Neonatal Intensive Care Unit: Global Patterns. Pediatr. Neonatol. 2021, 62, 3–10. [Google Scholar] [CrossRef]
- Gilley, R.; David, L.R.; Leamy, B.; Moloney, D.; Moore, N.; England, A.; Waldron, M.; Maher, M.; McEntee, M.F. Establishing weight-based diagnostic reference lev-els for neonatal chest X-rays. Radiography 2023, 29, 812–817. [Google Scholar] [CrossRef]
- Armpilia, C.I.; Fife, I.A.J.; Croasdale, P.L. Radiation dose quantities and risk in neonates in a special care baby unit. Br. J. Radiol. 2002, 75, 590–595. [Google Scholar] [CrossRef]
- Donadieu, J.; Zeghnoun, A.; Roudier, C.; Maccia, C.; Pirard, P.; André, C.; Adamsbaum, C.; Kalifa, G.; Legmann, P.; Jarreau, P.-H. Cumulative effective doses delivered by radiographs to preterm infants in a neonatal intensive care unit. Pediatrics 2006, 117, 882–888. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.-C. Radiation Safety in the Neonatal Intensive Care Unit: Too Little or Too Much Concern? Pediatr. Neonatol. 2010, 51, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Fanjul, J.; Benet, N.; de Lliria, C.R.G.; Porta, R.; Guinovart, G.; Bobillo-Pérez, S. Lung Ultrasound Protocol Decreases Radiation in Newborn Population without Side Effects: A Quality Improvement Project. Med. Intensiv. (Engl. Ed.) 2023, 47, 16–22. [Google Scholar] [CrossRef]
- Raschetti, R.; Yousef, N.; Vigo, G.; Marseglia, G.; Centorrino, R.; Ben-Ammar, R.; Shankar-Aguilera, S.; De Luca, D. Ecography-guided surfactant therapy to improve timeliness of surfactant replacement: A quality improvement project. J. Pediatr. 2019, 212, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Kurepa, D.; Zaghloul, N.; Watkins, L.; Liu, J. Neonatal lung ultrasound exam guidelines. J. Perinatol. 2018, 38, 11–22. [Google Scholar] [CrossRef] [PubMed]
- del Vecchio, A.; Salerno, S.; Barbagallo, M.; Chirico, G.; Campoleoni, M.; Cannatà, V.; Genovese, E.; Granata, C.; Magistrelli, A.; Tomà, P. Italian Inter-Society Expert Panel Position on Radiological Exposure in Neonatal Intensive Care Units. Ital. J. Pediatr. 2020, 46, 159. [Google Scholar] [CrossRef] [PubMed]
- Whitby, E.; Gaunt, T. Fetal lung MRI and features predicting post-natal outcome: A scoping review of the current literature. Br. J. Radiol. 2023, 96, 20220344. [Google Scholar] [CrossRef]
- Hahn, A.D.; Higano, N.S.; Walkup, L.L.; Thomen, R.P.; Cao, X.; Merhar, S.L.; Tkach, J.A.; Woods, J.C.; Fain, S.B. Pulmonary MRI of neonates in the intensive care unit using 3D ultrashort echo time and a small footprint MRI system. J. Magn. Reson. Imaging 2017, 45, 463–471. [Google Scholar] [CrossRef]
- Higano, N.S.; Spielberg, D.R.; Reck, R.J.; Schapiro, A.H.; Walkup, L.L.; Hahn, A.D.; Tkach, J.A.; Kingma, P.S.; Merhar, S.L.; Fain, S.B.; et al. Neonatal Pulmonary Magnetic Resonance Imaging of Bronchopulmonary Dysplasia Predicts Short-Term Clinical Outcomes. Am. J. Resp. Crit. Care Med. 2018, 198, 1302–1311. [Google Scholar] [CrossRef]
- Hysinger, E.B.; Higano, N.S.; Critser, P.J.; Woods, J.C. Imaging in Neonatal Respiratory Disease. Paediatr. Respir. Rev. 2022, 43, 44–52. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Lung ultrasound
|
| Parameters | Year of Study | One-Way ANOVA Test | ||
|---|---|---|---|---|
| 2021 | 2022 * | 2023 ** | ||
| Gestational age | ||||
| mean ± SD | 35.55 ± 1.80 | 34.92 ± 2.12 d | 36.14 ± 11.87 d,b | 0.012 |
| median | 35 | 35 | 36 | |
| limits | 32–39 | 30–39 | 30–39 | |
| Birth weight | ||||
| mean ± SD | 2680 ± 562.56 | 2504 ± 621.79 d | 2803 ± 535.10 d,c | 0.043 |
| median | 2670 | 2420 | 2890 | |
| limits | 1230–3500 | 1410–7592 | 1500–3670 | |
| Parameters | Year of Study | Chi-Square Test Likelihood Ratio | |||||
|---|---|---|---|---|---|---|---|
| 2021 (n = 29) | 2022 (n = 53) | p Value for Chi2 Test 2022 vs. 2021 | 2023 (n = 43) | p Value for Chi2 Test 2023 vs. 2021 | p Value for Chi2 Test 2023 vs. 2022 | ||
| Male | 24 (82.8%) | 30 (56.6%) | 0.018 | 22 (51.2%) | 0.007 | 0.597 | 0.013 |
| CPAP | 18 (62.1%) | 44 (83.0%) | 0.036 | 35 (81.4%) | 0.070 | 0.837 | 0.087 |
| VM | 16 (55.2%) | 18 (34.0%) | 0.064 | 14 (32.6%) | 0.058 | 0.885 | 0.110 |
| CPAP followed by VM | 5 (17.2%) | 9 (17.0%) | 0.976 | 6 (14.0%) | 0.706 | 0.686 | 0.901 |
| Pulmonary Rx | 19 (65.5%) | 33 (62.3%) | 0.771 | 18 (41.9%) | 0.050 | 0.048 | 0.067 |
| Associated pathologies | |||||||
| SDR | 21 (72.4%) | 44 (83.0%) | 0.260 | 31 (72.1%) | 0.976 | 0.200 | 0.359 |
| TTN | 5 (17.2%) | 8 (15.1%) | 0.800 | 7 (16.3%) | 0.915 | 0.874 | 0.967 |
| Congenital pneumonia | 3 (10.3%) | 1 (1.9%) | 0.091 | 0 (0%) | 0.032 | 0.368 | 0.045 |
| Meconium aspiration | 0 (0%) | 1 (1.9%) | 0.459 | 1 (2.3%) | 0.412 | 0.882 | 0.580 |
| Pneumothorax | 1 (3.4%) | 0 (0%) | 0.176 | 5 (11.6%) | 0.221 | 0.011 | 0.014 |
| Lung Rx Number | 2021 (n = 29) | 2022 * (n = 53) | 2023 ** (n = 43) | Chi-Square Test Likelihood Ratio |
|---|---|---|---|---|
| 0 | 10 (34.5%) | 19 (35.8%) d | 25 (58.1%) c,c | 0.146 |
| 1 | 13 (44.8%) | 19 (35.8%) d | 7 (16.3%) b,c | |
| 2 | 4 (13.8%) | 8 (15.1%) d | 5 (11.6%) d,d | |
| 3 | 2 (6.9%) | 3 (5.7%) d | 5 (11.6%) d,d | |
| ≥4 | 0 (0.0%) | 4 (7.6%) d | 1 (2.3%) d,d |
| N | Mean | Std. Deviation | Std. Error | 95% Confidence Interval for Mean | Minimum | Maximum | ||
|---|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||||
| 2021 | 18 | 0.67 | 0.907 | 0.214 | 0.22 | 1.12 | 0 | 3 |
| 2022 | 44 | 1.02 | 1.320 | 0.199 | 0.62 | 1.42 | 0 | 6 |
| 2023 | 35 | 0.57 | 1.065 | 0.180 | 0.21 | 0.94 | 0 | 4 |
| Total | 97 | 0.79 | 1.172 | 0.119 | 0.56 | 1.03 | 0 | 6 |
| N | Mean | Std. Deviation | Std. Error | 95% Confidence Interval for Mean | Minimum | Maximum | ||
|---|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||||
| 2021 | 5 | 1.80 | 0.837 | 0.374 | 0.76 | 2.84 | 1 | 3 |
| 2022 | 9 | 2.33 | 1.732 | 0.577 | 1.00 | 3.66 | 1 | 6 |
| 2023 | 6 | 2.50 | 1.049 | 0.428 | 1.40 | 3.60 | 1 | 4 |
| Total | 20 | 2.25 | 1.333 | 0.298 | 1.63 | 2.87 | 1 | 6 |
| N | Mean | Std. Deviation | Std. Error | 95% Confidence Interval for Mean | Minimum | Maximum | ||
|---|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||||
| 2021 | 16 | 1.50 | 0.730 | 0.183 | 1.11 | 1.89 | 1 | 3 |
| 2022 | 18 | 2.11 | 1.410 | 0.332 | 1.41 | 2.81 | 1 | 6 |
| 2023 | 14 | 2.21 | 0.975 | 0.261 | 1.65 | 2.78 | 1 | 4 |
| Total | 48 | 1.94 | 1.119 | 0.161 | 1.61 | 2.26 | 1 | 6 |
| Parameter | 2021 | 2022 | 2023 |
|---|---|---|---|
| N | 29 | 53 | 43 |
| Pulmonary X-ray | 19 | 33 | 18 |
| Radiation dose (mean = 9 Gy × cm2) | 171 | 297 | 162 |
| Radiation dose/ventilated patient (including CPAP) | 5.89 | 5.6 | 3.76 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nemes, A.F.; Toma, A.I.; Dima, V.; Serboiu, S.C.; Necula, A.I.; Stoiciu, R.; Ulmeanu, A.I.; Marinescu, A.; Ulmeanu, C. Use of Lung Ultrasound in Reducing Radiation Exposure in Neonates with Respiratory Distress: A Quality Management Project. Medicina 2024, 60, 308. https://doi.org/10.3390/medicina60020308
Nemes AF, Toma AI, Dima V, Serboiu SC, Necula AI, Stoiciu R, Ulmeanu AI, Marinescu A, Ulmeanu C. Use of Lung Ultrasound in Reducing Radiation Exposure in Neonates with Respiratory Distress: A Quality Management Project. Medicina. 2024; 60(2):308. https://doi.org/10.3390/medicina60020308
Chicago/Turabian StyleNemes, Alexandra Floriana, Adrian Ioan Toma, Vlad Dima, Sorina Crenguta Serboiu, Andreea Ioana Necula, Roxana Stoiciu, Alexandru Ioan Ulmeanu, Andreea Marinescu, and Coriolan Ulmeanu. 2024. "Use of Lung Ultrasound in Reducing Radiation Exposure in Neonates with Respiratory Distress: A Quality Management Project" Medicina 60, no. 2: 308. https://doi.org/10.3390/medicina60020308