
Seroepidemiology of Herpes Simplex Viruses Type 1 and 2 in Pregnant Women in Croatia

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
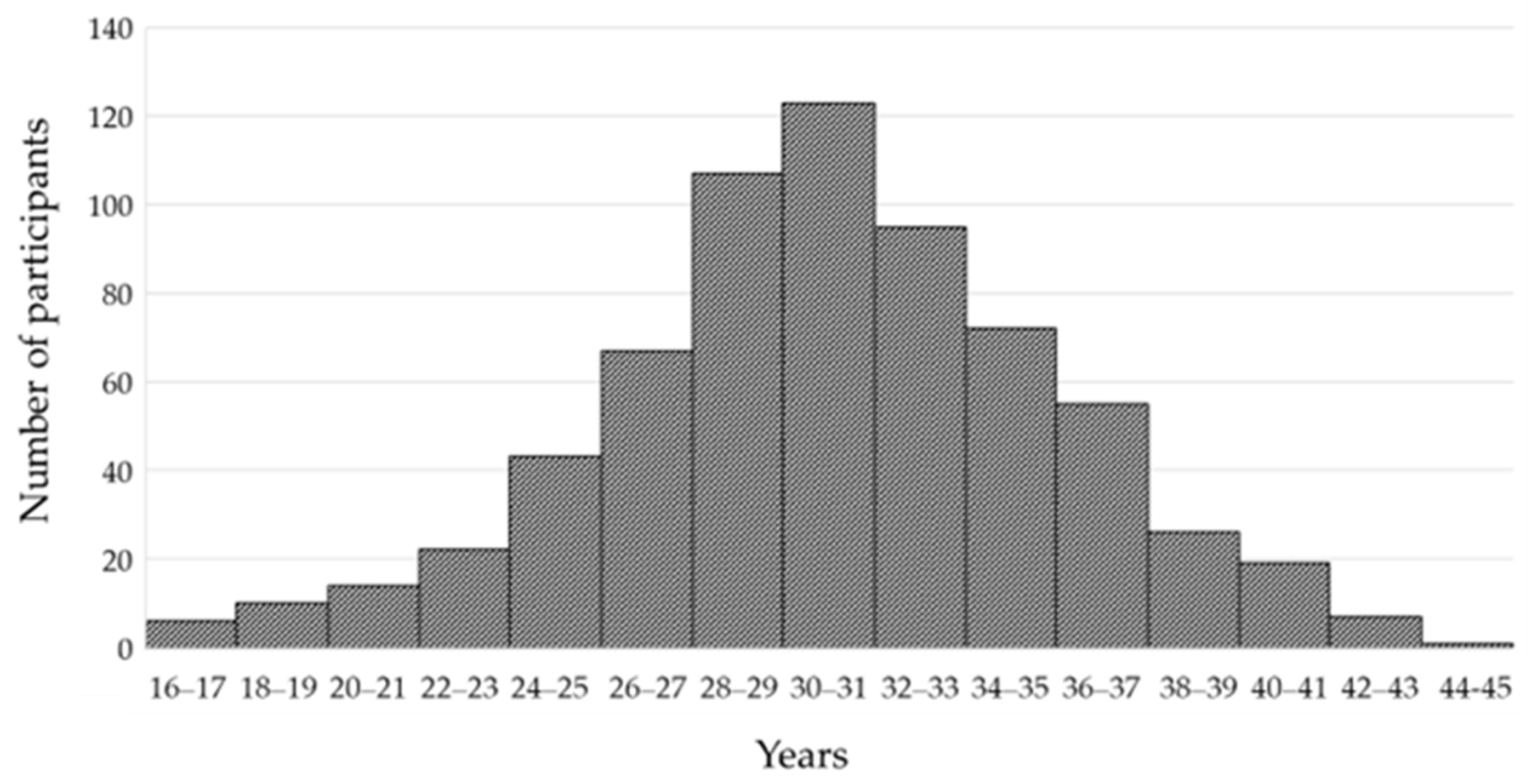
2.1. Study Participants
2.2. Methods
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Committee on Taxonomy of Viruses: ICTV. Orthoherpesviridae. Available online: https://ictv.global/report/chapter/orthoherpesviridae/orthoherpesviridae (accessed on 28 December 2023).
- Hammad, W.A.B.; Konje, J.C. Herpes simplex virus infection in pregnancy—An update. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 259, 38–45. [Google Scholar] [CrossRef]
- Tunbäck, P.; Liljeqvist, J.A.; Löwhagen, G.B.; Bergström, T. Glycoprotein G of herpes simplex virus type 1: Identification of type-specific epitopes by human antibodies. J. Gen. Virol. 2000, 81 Pt 4, 1033–1040. [Google Scholar] [CrossRef] [PubMed]
- James, C.; Harfouche, M.; Welton, N.J.; Turner, K.M.E.; Abu-Raddad, L.J.; Gottlieb, S.L.; Looker, K.J. Herpes simplex virus: Global infection prevalence and incidence estimates, 2016. Bull. World Health Organ. 2020, 98, 315–329. [Google Scholar] [CrossRef]
- World Health Organization. Herpes Simplex Virus. Available online: https://www.who.int/news-room/fact-sheets/detail/herpes-simplex-virus (accessed on 30 December 2023).
- Mark, K.E.; Wald, A.; Magaret, A.S.; Selke, S.; Olin, L.; Huang, M.L.; Corey, L. Rapidly cleared episodes of herpes simplex virus reactivation in immunocompetent adults. J. Infect. Dis. 2008, 198, 1141–1149. [Google Scholar] [CrossRef]
- Anzivino, E.; Fioriti, D.; Mischitelli, M.; Bellizzi, A.; Barucca, V.; Chiarini, F.; Pietropaolo, V. Herpes simplex virus infection in pregnancy and in neonate: Status of art of epidemiology, diagnosis, therapy and prevention. Virol. J. 2009, 6, 40. [Google Scholar] [CrossRef] [PubMed]
- Straface, G.; Selmin, A.; Zanardo, V.; De Santis, M.; Ercoli, A.; Scambia, G. Herpes simplex virus infection in pregnancy. Infect. Dis. Obstet. Gynecol. 2012, 2012, 385697. [Google Scholar] [CrossRef]
- Marchi, S.; Trombetta, C.M.; Gasparini, R.; Temperton, N.; Montomoli, E. Epidemiology of herpes simplex virus type 1 and 2 in Italy: A seroprevalence study from 2000 to 2014. J. Prev. Med. Hyg. 2017, 58, E27–E33. [Google Scholar] [PubMed]
- Alanen, A.; Kahala, K.; Vahlberg, T.; Koskela, P.; Vainionpää, R. Seroprevalence, incidence of prenatal infections and reliability of maternal history of varicella zoster virus, cytomegalovirus, herpes simplex virus and parvovirus B19 infection in South-Western Finland. BJOG 2005, 112, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Gaytant, M.A.; Steegers, E.A.; van Laere, M.; Semmekrot, B.A.; Groen, J.; Weel, J.F.; van der Meijden, W.I.; Boer, K.; Galama, J.M. Seroprevalences of herpes simplex virus type 1 and type 2 among pregnant women in the Netherlands. Sex. Transm. Dis. 2002, 29, 710–714. [Google Scholar] [CrossRef]
- Nath, P.; Kabir, M.A.; Doust, S.K.; Ray, A. Diagnosis of Herpes Simplex Virus: Laboratory and Point-of-Care Techniques. Infect. Dis. Rep. 2021, 13, 49. [Google Scholar] [CrossRef]
- Vilibic-Cavlek, T.; Ljubin-Sternak, S.; Ban, M.; Kolaric, B.; Sviben, M.; Mlinaric-Galinovic, G. Seroprevalence of TORCH infections in women of childbearing age in Croatia. J. Matern. Fetal Neonatal Med. 2011, 24, 280–283. [Google Scholar] [CrossRef] [PubMed]
- Vilibic-Cavlek, T.; Kolaric, B.; Ljubin-Sternak, S.; Mlinaric-Galinovic, G. Herpes simplex virus infection in the Croatian population. Scand. J. Infect. Dis. 2011, 43, 918–922. [Google Scholar] [CrossRef] [PubMed]
- Alareeki, A.; Osman, A.M.M.; Khandakji, M.N.; Looker, K.J.; Harfouche, M.; Abu-Raddad, L.J. Epidemiology of herpes simplex virus type 2 in Europe: Systematic review, meta-analyses, and meta-regressions. Lancet Reg. Health Eur. 2022, 25, 100558. [Google Scholar] [CrossRef]
- Patton, M.E.; Bernstein, K.; Liu, G.; Zaidi, A.; Markowitz, L.E. Seroprevalence of Herpes Simplex Virus Types 1 and 2 Among Pregnant Women and Sexually Active, Nonpregnant Women in the United States. Clin. Infect. Dis. 2018, 67, 1535–1542. [Google Scholar] [CrossRef]
- Enders, G.; Risse, B.; Zauke, M.; Bolley, I.; Knotek, F. Seroprevalence study of herpes simplex virus type 2 among pregnant women in Germany using a type-specific enzyme immunoassay. Eur. J. Clin. Microbiol. Infect. Dis. 1998, 17, 870–872. [Google Scholar] [CrossRef] [PubMed]
- Uusküla, A.; Nygard-Kibur, M.; Cowan, F.M.; Mayaud, P.; French, R.S.; Robinson, J.N.; Brown, D.W. The burden of infection with herpes simplex virus type 1 and type 2: Seroprevalence study in Estonia. Scand. J. Infect. Dis. 2004, 36, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Kucera, P.; Gerber, S.; Marques-Vidal, P.; Meylan, P.R. Seroepidemiology of herpes simplex virus type 1 and 2 in pregnant women in Switzerland: An obstetric clinic based study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 160, 13–17. [Google Scholar] [CrossRef]
- LeGoff, J.; Saussereau, E.; Boulanger, M.C.; Chemin, C.; Si-Mohamed, A.; Bélec, L.; Maisonneuve, L. Unexpected high prevalence of herpes simplex virus (HSV) type 2 seropositivity and HSV genital shedding in pregnant women living in an East Paris suburban area. Int. J. STD AIDS 2007, 18, 593–595. [Google Scholar] [CrossRef]
- Ozdemir, R.; Er, H.; Baran, N.; Vural, A.; Demirci, M. HSV-1 and HSV-2 seropositivity rates in pregnant women admitted to Izmir Ataturk Research and Training Hospital, Turkey. Mikrobiyol. Bul. 2009, 43, 709–711. [Google Scholar]
- Arama, V.; Vladareanu, R.; Mihailescu, R.; Streinu Cercel, A.; Mihai, C.; Hristea, A.; Iosipenco, M.; Stefan Arama, S.; Rabilloud, M. Seroprevalence and Risk Factors Associated with Herpes Simplex Virus Infection among Pregnant Women. J. Perinat. Med. 2008, 36, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Puhakka, L.; Sarvikivi, E.; Lappalainen, M.; Surcel, H.M.; Saxen, H. Decrease in seroprevalence for herpesviruses among pregnant women in Finland: Cross-sectional study of three time points 1992, 2002 and 2012. Infect. Dis. 2016, 48, 406–410. [Google Scholar] [CrossRef] [PubMed]
- Lima, L.R.P.; Dos Santos Pereira, J.S.; de Almeida, N.A.A.; de Meneses, M.D.F.; Aguiar, S.F.; Fernandes, C.A.S.; Azevedo, R.C.; de Paula, V.S. Seroprevalence of human alphaherpesvirus 1 and 2 among pregnant women infected or uninfected with Zika virus from Rio de Janeiro, Brazil. J. Med. Virol. 2021, 93, 3383–3388. [Google Scholar] [CrossRef] [PubMed]
- Rostamzadeh Khameneh, Z.; Sepehrvand, N.; Mohammadian, M. Herpes Simplex Virus Type 2 Seroprevalence in Pregnant Women in Urmia, Northwest of Iran, during 2014–2015. Iran. Biomed. J. 2020, 24, 136–139. [Google Scholar] [CrossRef] [PubMed]
- Biswas, D.; Borkakoty, B.; Mahanta, J.; Walia, K.; Saikia, L.; Akoijam, B.S.; Jampa, L.; Kharkongar, A.; Zomawia, E. Seroprevalence and risk factors of herpes simplex virus type-2 infection among pregnant women in Northeast India. BMC Infect. Dis. 2011, 11, 325. [Google Scholar] [CrossRef] [PubMed]
- Patrick, D.M.; Dawar, M.; Cook, D.A.; Krajden, M.; Ng, H.C.; Rekart, M.L. Antenatal seroprevalence of herpes simplex virus type 2 (HSV-2) in Canadian women: HSV-2 prevalence increases throughout the reproductive years. Sex. Transm. Dis. 2001, 28, 424–428. [Google Scholar] [CrossRef] [PubMed]
- Li, J.M.; Chen, Y.R.; Li, X.T.; Xu, W.C. Screening of Herpes simplex virus 2 infection among pregnant women in southern China. J. Dermatol. 2011, 38, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Anjulo, A.A.; Abebe, T.; Hailemichael, F.; Mihret, A. Seroprevalence and risk factors of herpes simplex virus-2 among pregnant women attending antenatal care at health facilities in Wolaita zone, Ethiopia. Virol. J. 2016, 13, 43. [Google Scholar] [CrossRef] [PubMed]
- Duran, N.; Yarkin, F.; Evruke, C.; Koksal, F. Asymptomatic herpes simplex virus type 2 (HSV-2) infection among pregnant women in Turkey. Indian J. Med. Res. 2004, 120, 106–110. [Google Scholar]
- Bünzli, D.; Wietlisbach, V.; Barazzoni, F.; Sahli, R.; Meylan, P.R. Seroepidemiology of herpes simplex virus type 1 and 2 in western and southern Switzerland in adults aged 25–74 in 1992–93: A population-based study. BMC Infect. Dis. 2004, 4, 10. [Google Scholar] [CrossRef]
- Korr, G.; Thamm, M.; Czogiel, I.; Poethko-Mueller, C.; Bremer, V.; Jansen, K. Decreasing seroprevalence of herpes simplex virus type 1 and type 2 in Germany leaves many people susceptible to genital infection: Time to raise awareness and enhance control. BMC Infect. Dis. 2017, 17, 471. [Google Scholar] [CrossRef]
- Hettmann, A.; Gerle, B.; Barcsay, E.; Csiszár, C.; Takács, M. Seroprevalence of HSV-2 in Hungary and comparison of the HSV-2 prevalence of pregnant and infertile women. Acta Microbiol. Immunol. Hung. 2008, 55, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Berntsson, M.; Tunbäck, P.; Ellström, A.; Krantz, I.; Löwhagen, G.B. Decreasing prevalence of herpes simplex virus-2 antibodies in selected groups of women in Sweden. Acta Derm. Venereol. 2009, 89, 623–626. [Google Scholar] [CrossRef] [PubMed]
- Sert, U.Y.; Ozgu-Erdinc, A.S.; Saygan, S.; Engin-Ustun, Y. Herpes Simplex Infection During Pregnancy, Results of a Tertiary Referral Center in Turkey. Z. Geburtshilfe Neonatol. 2020, 224, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Riley, L.E.; Wald, A. Genital Herpes Simplex Virus Infection and Pregnancy. Available online: https://uptodatefree.ir/topic.htm?path=genital-herpes-simplex-virus-infection-and-pregnancy (accessed on 4 January 2024).




{kind=link}
{kind=link}
{kind=link}
| Characteristic | N (%) Tested | HSV-1 IgM | HSV-1 IgG | ||||
|---|---|---|---|---|---|---|---|
| N (%) | 95%CI | p | N (%) | 95%CI | p | ||
| Age group | 0.239 | 0.083 | |||||
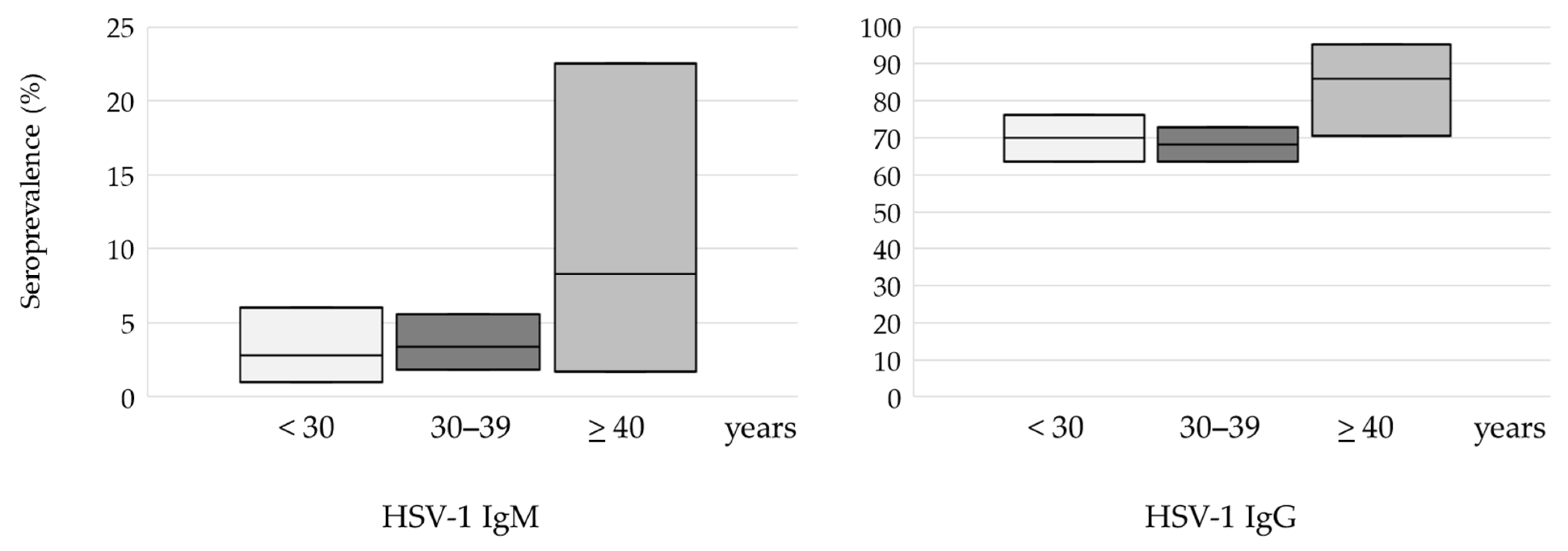
| <30 years | 214 (32.1) | 6 (2.8) | 1.0–6.0 | 150 (70.0) | 63.5–76.1 | ||
| 30–39 years | 417 (62.5) | 14 (3.4) | 1.8–5.6 | 285 (68.3) | 63.6–72.8 | ||
| ≥40 years | 36 (5.4) | 3 (8.3) | 1.7–22.5 | 31 (86.1) | 70.5–95.3 | ||
| Area or residence | 0.348 | 0.208 | |||||
| Urban | 614 (92.1) | 19 (3.1) | 1.9–4.8 | 433 (70.5) | 66.7–74.1 | ||
| Suburban/rural | 53 (7.9) | 4 (7.5) | 2.1–18.2 | 33 (62.3) | 47.9–75.2 | ||
| Geographic region | 0.973 | 0.390 | |||||
| Continental | 483 (72.4) | 16 (3.3) | 1.9–5.3 | 342 (70.8) | 66.5–74.8 | ||
| Coastal | 184 (27.6) | 6 (3.2) | 1.2–6.9 | 124 (67.3) | 60.1–74.1 | ||
| Obstetric history | 0.461 | 0.883 | |||||
| Normal pregnancy | 453 (67.9) | 14 (3.1) | 1.7–5.1 | 315 (69.5) | 65.1–73.7 | ||
| Unfavorable obstetric history | 214 (32.1) | 9 (4.2) | 1.9–7.8 | 150 (70.1) | 63.5–76.1 | ||
| Characteristic | N (%) Tested | HSV-2 IgM | HSV-2 IgG | ||||
|---|---|---|---|---|---|---|---|
| N (%) | 95%CI | p | N (%) | 95%CI | p | ||
| Age group | 0.219 | 0.005 | |||||
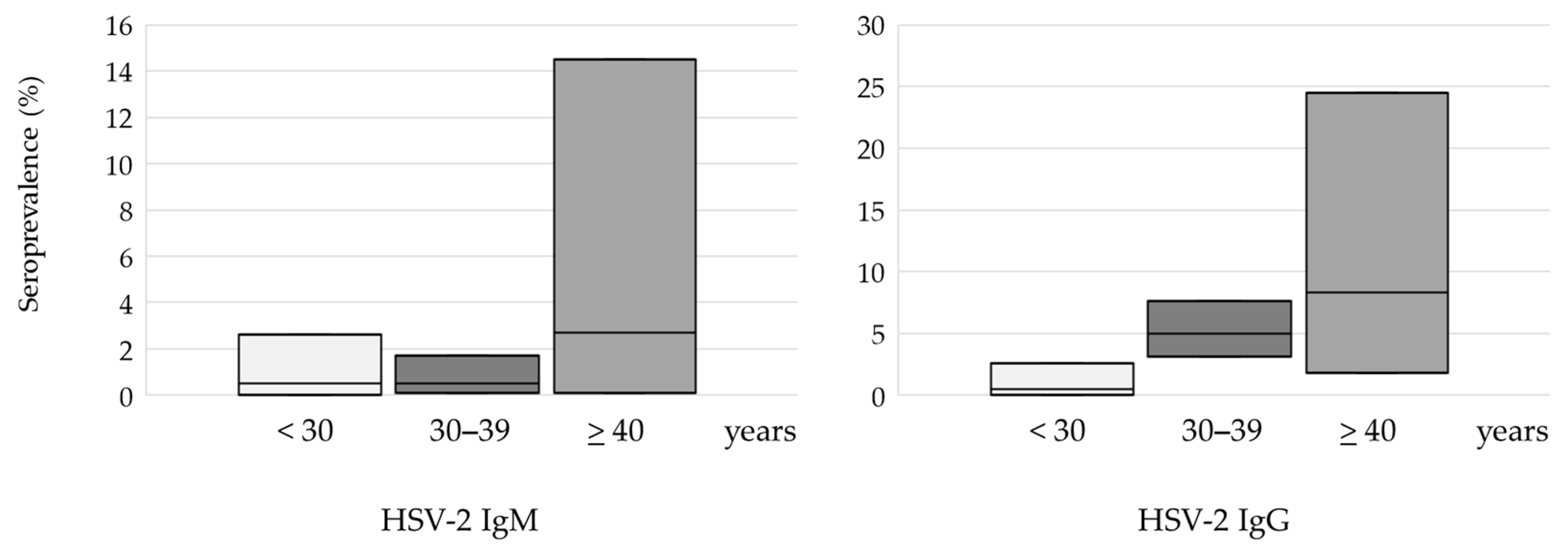
| <30 years | 214 (32.1) | 1 (0.5) | 0.0–2.6 | 1 (0.5) | 0.01–2.6 | ||
| 30–39 years | 417 (62.5) | 2 (0.5) | 0.1–1.7 | 21 (5.0) | 3.1–7.6 | ||
| ≥40 years | 36 (5.4) | 1 (2.7) | 0.1–14.5 | 3 (8.3) | 1.8–24.5 | ||
| Area or residence | 0.555 | 0.134 | |||||
| Urban Suburban/rural | 614 (92.1) 53 (7.9) | 4 (0.6) 0 (0) | 0.2–1.6 0.0–6.7 * | 25 (4.1) 0 (0) | 2.5–5.8 0.0–6.7 * | ||
| Geographic region | 0.230 | 0.387 | |||||
| Continental | 483 (72.4) | 4 (0.8) | 0.2–2.1 | 20 (4.1) | 2.5–6.3 | ||
| Coastal | 184 (27.6) | 0 (0) | 0.0–1.9 * | 5 (2.7) | 0.9–6.2 | ||
| Obstetric history | 0.440 | 0.193 | |||||
| Normal pregnancy | 453 (67.9) | 2 (0.5) | 0.1–1.6 | 14 (3.5) | 1.7–5.1 | ||
| Unfavorable obstetric history | 214 (32.1) | 2 (1.1) | 0.2–1.5 | 11 (5.1) | 2.6–9.0 | ||
| Characteristic | HSV-1 IgM | HSV-1 IgG | ||||
|---|---|---|---|---|---|---|
| OR | 95%CI | p | OR | 95%CI | p | |
| Age (one-year increase) | 1.02 | 0.94–1.10 | 0.600 | 1.03 | 0.99–1.06 | 0.052 |
| Urban (Ref.) vs. suburban/rural area of residence | 1.69 | 0.48–5.87 | 0.406 | 0.75 | 0.42–1.35 | 0.346 |
| Continental (Ref.) vs. coastal geographic region | 0.98 | 0.37–2.55 | 0.973 | 0.852 | 0.59–1.22 | 0.390 |
| Normal pregnancy (Ref.) vs. unfavorable obstetric history | 1.06 | 0.44–2.51 | 0.894 | 1.11 | 0.78–1.58 | 0.553 |
| Characteristic | HSV-2 IgM | HSV-2 IgG | ||||
|---|---|---|---|---|---|---|
| OR | 95%CI | p | OR | 95%CI | p | |
| Age (one-year increase) | 1.09 | 0.89–1.34 | 0.380 | 1.19 | 1.09–1.30 | <0.001 |
| Urban (Ref.) vs. suburban/rural area of residence | 1.00 | NA | NA | 1.00 | NA | NA |
| Continental (Ref.) vs. coastal geographic region | 0.22 | 0.01–4.26 | 0.323 | 0.64 | 0.24–1.75 | 0.390 |
| Normal pregnancy (Ref.) vs. unfavorable obstetric history | 2.12 | 0.29–15.20 | 0.451 | 1.33 | 0.59–3.00 | 0.479 |
| Characteristic | HSV-1 IgG | HSV-2 IgG | ||||
|---|---|---|---|---|---|---|
| OR | 95%CI | p | OR | 95%CI | p | |
| Age (one-year increase) | 1.03 | 0.99–1.06 | 0.063 | 1.19 | 1.09–1.30 | <0.001 |
| Urban vs. suburban/rural area of residence | 0.77 | 0.43–1.39 | 0.396 | 1 | NA | NA |
| Normal pregnancy vs. unfavorable obstetric history | 1.11 | 0.78–1.58 | 0.553 | 1.35 | 0.59–3.09 | 0.469 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vilibic-Cavlek, T.; Belamaric, M.; Ferenc, T.; Navolan, D.; Kolaric, B.; Milasincic, L.; Antolasic, L.; Vujica Ferenc, M.; Vilibic, M.; Lukunic, A.; et al. Seroepidemiology of Herpes Simplex Viruses Type 1 and 2 in Pregnant Women in Croatia. Medicina 2024, 60, 284. https://doi.org/10.3390/medicina60020284
Vilibic-Cavlek T, Belamaric M, Ferenc T, Navolan D, Kolaric B, Milasincic L, Antolasic L, Vujica Ferenc M, Vilibic M, Lukunic A, et al. Seroepidemiology of Herpes Simplex Viruses Type 1 and 2 in Pregnant Women in Croatia. Medicina. 2024; 60(2):284. https://doi.org/10.3390/medicina60020284
Chicago/Turabian StyleVilibic-Cavlek, Tatjana, Marko Belamaric, Thomas Ferenc, Dan Navolan, Branko Kolaric, Ljiljana Milasincic, Ljiljana Antolasic, Mateja Vujica Ferenc, Maja Vilibic, Adriana Lukunic, and et al. 2024. "Seroepidemiology of Herpes Simplex Viruses Type 1 and 2 in Pregnant Women in Croatia" Medicina 60, no. 2: 284. https://doi.org/10.3390/medicina60020284