
Association between Perceived Activity Restriction Due to People’s Perception of Aging and Unmet Medical Needs among Middle-Aged and Elderly People: A Population-Based Study


Abstract
:1. Introduction
2. Materials and Methods
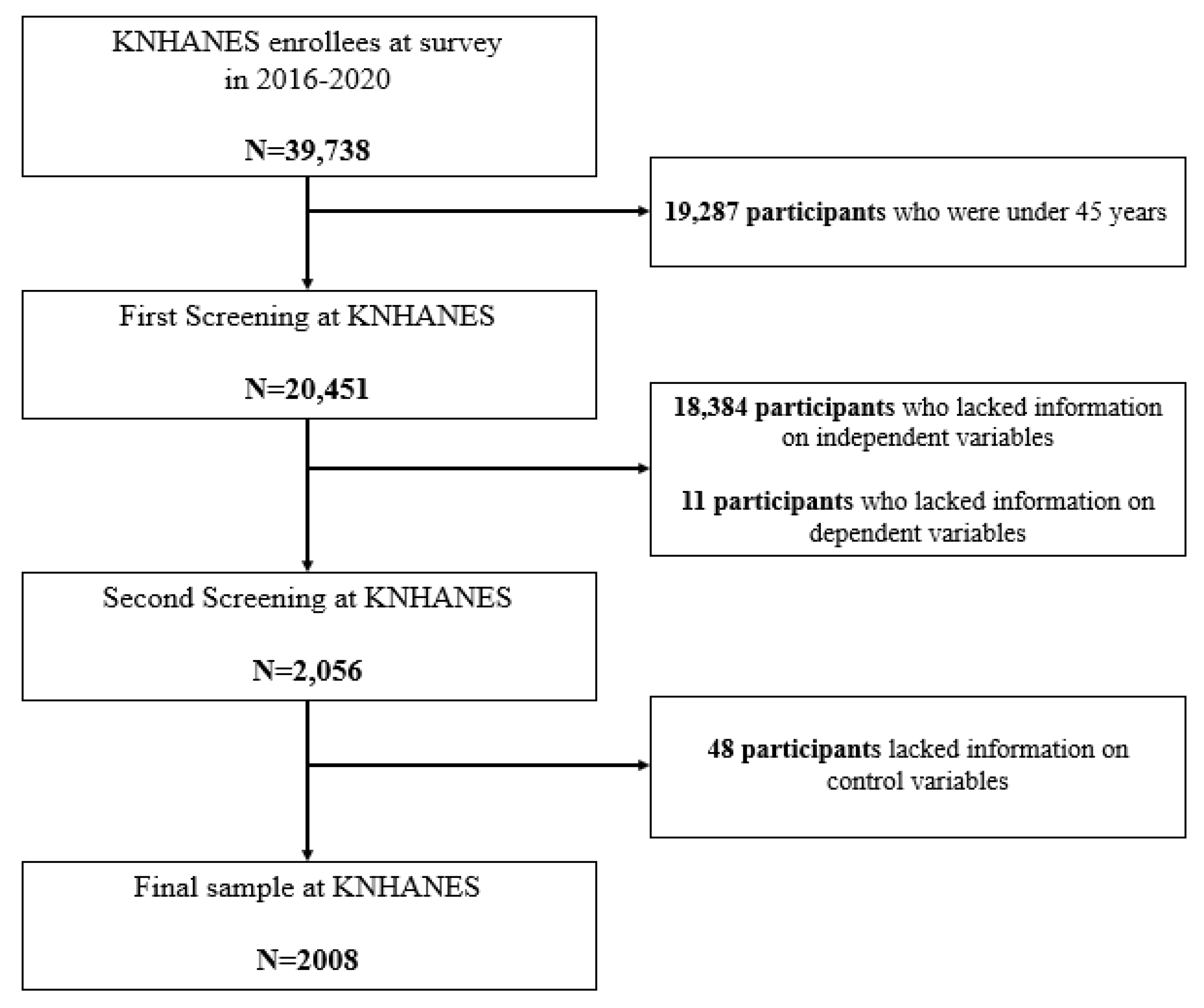
2.1. Data Source and Study Participants
2.2. Independent Variables
2.3. Dependent Variables
2.4. Control Variables
2.5. Statistical Analysis
3. Results
3.1. General Characteristics of the Study Population
3.2. Factors Associated with UMN in the Group of PAR Due to People’s Own Perception of Aging
3.3. Subgroup Analysis Stratified by Gender, Current Chronic Diseases, and Age
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shin, J.W.; Yeo, J.Y.; Song, Y.M. The elderly’s unmet need for care and their use of informal care services. Korean J. Health Econ. Policy 2011, 17, 29–146. [Google Scholar]
- Statistics Korea. Population Trends in October 2022. 2022. Available online: https://kosis.kr/statHtml/statHtml.do?orgId=101&tblId=DT_1BPB001&conn_path=I2 (accessed on 26 December 2023).
- Statistics Korea. Statistics of The Elderly in 2022. 2022. Available online: https://kostat.go.kr/board.es?mid=a10301060100&bid=10820&act=view&list_no=420896&tag=&nPage=1&ref_bid=218,219,220,10820,11815,11895,11816,208&keyField=T&keyWord=%EA%B3%A0%EB%A0%B9%EC%9E%90 (accessed on 26 December 2023).
- Lee, H.J.; Huh, S.I. Unmet Health Care Needs and Impact of Type of Household among the Elderly in Korea. Korean J. Health Econ. Policy 2017, 23, 85–108. [Google Scholar]
- Herr, M.; Arvieu, J.-J.; Aegerter, P.; Robine, J.-M.; Ankri, J. Unmet health care needs of older people: Prevalence and predictors in a French cross-sectional survey. Eur. J. Public Health 2014, 24, 808–813. [Google Scholar] [CrossRef] [PubMed]
- Alonso, F.O.A.J.; Orfila, F.; Ruigómez, A.; Ferrer, M.; Antó, J.M. Unmet health care needs and mortality among Spanish elderly. Am. J. Public Health 1997, 87, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Bennett, A.C.; Rankin, K.M.; Rosenberg, D. Does a medical home mediate racial disparities in unmet healthcare needs among children with special healthcare needs? Matern. Child Health J. 2012, 16 (Suppl. S2), 330–338. [Google Scholar] [CrossRef] [PubMed]
- Choi, R.; Hwang, B.-D. Health care utilization of age group in the elderly on the Korean health panel. Korean J. Health Serv. Manag. 2014, 8, 49–61. [Google Scholar] [CrossRef]
- Ahn, Y.H.; Kim, N.H.; Kim, C.B.; Ham, O.K. Factors affecting unmet healthcare needs of older people in Korea. Int. Nurs. Rev. 2013, 60, 510–519. [Google Scholar] [CrossRef]
- Kim, Y.-S.; Lee, J.; Moon, Y.; Kim, K.J.; Lee, K.; Choi, J.; Han, S.-H. Unmet healthcare needs of elderly people in Korea. BMC Geriatr. 2018, 18, 98. [Google Scholar] [CrossRef]
- Korea Institute For Health And Social Affairs. Long-Term Development of Social Policy in the Age of Aging. 2002. Available online: https://repository.kihasa.re.kr/handle/201002/366 (accessed on 26 December 2023).
- Jae, H.H.; Yonhtae, C. Activity Limitations and Health Behaviors by Socioeconomic Status among the Elderly Seoul Population. J. Korean Gerontol. Soc. 2008, 28, 87–104. [Google Scholar]
- Kang, S.R.; Moon, J.H. Comparison of sociodemographic characteristics, depression, quality of life, and unmet medical need between elders with and without limitation of activity by aging or dementia: Using seventh Korea national health and nutrition examination survey. J. Occup. Ther. Aged Dement. 2018, 12, 1–11. [Google Scholar] [CrossRef]
- Hwang, H.S.; Choi, J.H.; Kim, S.K. Factors Affecting Activity Restriction in the Elderly with Chronic Disease: Using data from the 8th period of the National Health and Nutrition Examination Survey. J. Korea Converg. Soc. 2021, 12, 359–369. [Google Scholar]
- Korea National Health and Nutrition Examination Survey. National Health Statistics 2017. Available online: https://dataon.kisti.re.kr/search/view.do?svcId=c3aaeefa557772ed8c57515a0793ffab&mode=02 (accessed on 26 December 2023).
- Monma, T.; Takeda, F.; Noguchi, H.; Tamiya, N. Age and sex differences of risk factors of activity limitations in Japanese older adults. Geriatr. Gerontol. Int. 2016, 16, 670–678. [Google Scholar] [CrossRef] [PubMed]
- van Gool, C.H.; Picavet, H.S.J.; Deeg, D.J.H.; de Klerk, M.M.Y.; Nusselder, W.J.; van Boxtel, M.P.J.; Wong, A.; Hoeymans, N. Trends in activity limitations: The Dutch older population between 1990 and 2007. Int. J. Epidemiol. 2011, 40, 1056–1067. [Google Scholar] [CrossRef] [PubMed]
- Hootman, J.M.; Helmick, C.G. Projections of US prevalence of arthritis and associated activity limitations. Arthritis Rheum. 2006, 54, 226–229. [Google Scholar] [CrossRef] [PubMed]
- Hill, E.J.; Erickson, J.J.; Fellows, K.J.; Martinengo, G.; Allen, S.M. Work and family over the life course: Do older workers differ? J. Fam. Econ. Issues 2014, 35, 1–13. [Google Scholar] [CrossRef]
- Mor-Barak, M.E. The meaning of work for older adults seeking employment: The generativity factor. Int. J. Aging Hum. Dev. 1995, 41, 325–344. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, T.E.; Choi, J.; Lee, S.; Gurland, B.; Devanand, D.P. Effects of restriction of activities and social isolation on risk of dementia in the community. Int. Psychogeriatr. 2021, 33, 1207–1215. [Google Scholar] [CrossRef]
- Yang, J.M.; Kim, J.H. The relationship between unmet medical needs awareness and health care utilization in Korean adults with social activity restriction: A secondary analysis study using propensity score matching. J. Health Res. 2024, 38, 2. [Google Scholar] [CrossRef]
- Song, K.S.; Lee, J.H.; Rhim, K.H. Factors Associated with Unmet Needs for Health Care. Korean Public Health Res. 2011, 37, 131–140. [Google Scholar]
- Hwang, B.-D.; Choi, R. The prevalence and association factors of unmet medical needs by age group in the elderly. Korean J. Health Serv. Manag. 2015, 9, 81–93. [Google Scholar] [CrossRef]
- Moon, J.H.; Kang, M.A. The Prevalence and Predictors of Unmet Medical Needs among the Elderly Living Alone in Korea: An Application of the Behavioral Model for Vulnerable Populations. Health Soc. Welf. Rev. 2016, 36, 480–510. [Google Scholar]
- Berger, N.; Van Oyen, H.; Cambois, E.; Fouweather, T.; Jagger, C.; Nusselder, W.; Robine, J.-M. Assessing the validity of the global activity limitation indicator in fourteen European countries. BMC Med. Res. Methodol. 2015, 15, 1. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J. Understanding reasons for unmet health care needs in Korea: What are health policy implications? BMC Health Serv. Res. 2018, 18, 557. [Google Scholar] [CrossRef] [PubMed]
- Gulley, S.P.; Altman, B.M. Disability in two health care systems: Access, quality, satisfaction, and physician contacts among working-age Canadians and Americans with disabilities. Disabil. Health J. 2008, 1, 196–208. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.-Y.; Ryu, S.-Y. Factors associated with the types of unmet health care needs among the elderly in Korea. Korean J. Health Serv. Manag. 2017, 11, 65–79. [Google Scholar] [CrossRef]
- Lemon, B.W.; Bengtson, V.L.; Peterson, J.A. An exploration of the activity theory of aging: Activity types and life satisfaction among in-movers to a retirement community. J. Gerontol. 1972, 27, 511–523. [Google Scholar] [CrossRef] [PubMed]
- Keum, J.L.; Hye, S.P. A Study on the Perceived Health Status, Depression, and Activities of Daily Living for the Elderly in Urban Areas. Korean J. Women Health Nurs. 2006, 12, 221–230. [Google Scholar]
- Park, G.R.; Choi, B.H. Association between Unmet Healthcare Needs and Unmet Long-term Care Needs among the Korean Elderly. Health Soc. Welf. Rev. 2018, 38, 40–56. [Google Scholar] [CrossRef]
- Statistics Korea. National Health Statistics 2021. Available online: https://www.hira.or.kr/bbsDummy.do?pgmid=HIRAJ030000007001&brdScnBltNo=4&brdBltNo=6&pageIndex=1&pageIndex2=1 (accessed on 26 December 2023).
- Ojeda, V.D.; Bergstresser, S.M. Gender, race-ethnicity, and psychosocial barriers to mental health care: An examination of perceptions and attitudes among adults reporting unmet need. J. Health Soc. Behav. 2008, 49, 317–334. [Google Scholar] [CrossRef]
- Jung, B.; Ha, I.H. Determining the reasons for unmet healthcare needs in South Korea: A secondary data analysis. Health Qual Life Outcomes 2021, 19, 99. [Google Scholar] [CrossRef]
- Han, J.Y.; Park, H.S. Factors Affecting Unmet Healthcare Needs among Adults with Chronic Diseases. J. Korean Acad. Community Health Nurs. 2021, 32, 131–139. [Google Scholar] [CrossRef]
- Gill, T.M.; Desai, M.M.; Gahbauer, E.A.; Holford, T.R.; Williams, C.S. Restricted Activity among Community-Living Older Persons: Incidence, Precipitants, and Health Care Utilization. Ann. Intern. Med. 2001, 135, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Park, E.H.; Oh, D.H.; Cho, E. The effect of stress and depression on unmet medical needs. Korean J. Clin. Pharm. 2017, 27, 44–54. [Google Scholar] [CrossRef]
- Korea Institute For Health And Social Affairs. Policy Options to Tackle Unmet Health Needs; Korea Institute For Health And Social Affairs: Sejong, Republic of Korea, 2009. [Google Scholar]
- Condelius, A.; Edberg, A.-K.; Hallberg, I.R.; Jakobsson, U. Utilization of medical healthcare among people receiving long-term care at home or in special accommodation. Scand. J. Caring Sci. 2010, 24, 404–413. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total | UMN | p-Value | ||||
|---|---|---|---|---|---|---|---|
| No | Yes | ||||||
| N | % * | N | % * | N | % * | ||
| Total | 2008 | 100.0 | 1619 | 80.6 | 389 | 19.4 | |
| PAR due to people’s own perception of aging | 0.0071 | ||||||
| No | 1923 | 96.2 | 1557 | 81.1 | 366 | 18.9 | |
| Yes | 85 | 3.8 | 62 | 67.6 | 23 | 32.4 | |
| Age | 0.5425 | ||||||
| 45–54 | 237 | 19.9 | 190 | 79.9 | 47 | 20.1 | |
| 55–64 | 476 | 26.5 | 374 | 78.4 | 102 | 21.6 | |
| 65–75 | 667 | 26.0 | 542 | 82.5 | 125 | 17.5 | |
| Over 75 | 628 | 27.6 | 513 | 81.5 | 115 | 18.5 | |
| Gender | 0.0133 | ||||||
| Male | 770 | 41.4 | 655 | 83.8 | 115 | 16.2 | |
| Female | 1238 | 58.6 | 964 | 78.4 | 274 | 21.6 | |
| Marital Status | <0.0001 | ||||||
| Single (including separated and divorced) | 789 | 37.4 | 590 | 75.1 | 199 | 24.9 | |
| Married | 1219 | 62.6 | 1029 | 83.9 | 190 | 16.1 | |
| Education | 0.4443 | ||||||
| ≤Elementary school | 1098 | 47.4 | 872 | 78.9 | 226 | 21.1 | |
| Middle school | 316 | 16.9 | 254 | 83.0 | 62 | 17.0 | |
| High school | 400 | 23.3 | 331 | 82.4 | 69 | 17.6 | |
| ≥College | 194 | 12.4 | 162 | 80.7 | 32 | 19.3 | |
| Family Income | 0.0009 | ||||||
| Poor | 1022 | 47.8 | 775 | 76.3 | 247 | 23.7 | |
| Fair | 757 | 38.8 | 651 | 85.4 | 106 | 14.6 | |
| Good | 229 | 13.4 | 193 | 82.4 | 36 | 17.6 | |
| Residency Region | 0.4761 | ||||||
| Capital area | 434 | 24.6 | 339 | 78.4 | 95 | 21.6 | |
| Metropolitan city | 614 | 31.1 | 500 | 80.9 | 114 | 19.1 | |
| Rural area | 960 | 44.3 | 780 | 81.7 | 180 | 18.3 | |
| Occupation | 0.4923 | ||||||
| White-collar | 305 | 16.9 | 256 | 82.3 | 49 | 17.7 | |
| Blue-collar | 1584 | 77.9 | 1261 | 80.0 | 323 | 20.0 | |
| Unemployment | 119 | 5.2 | 102 | 84.9 | 17 | 15.1 | |
| Health Insurance Type | 0.0190 | ||||||
| National health insurance (regional) | 644 | 31.8 | 513 | 79.7 | 131 | 20.3 | |
| National health insurance (work) | 1064 | 53.3 | 884 | 82.9 | 180 | 17.1 | |
| Medical benefits | 300 | 14.9 | 222 | 74.5 | 78 | 25.5 | |
| Self-Rated Health | <0.0001 | ||||||
| Poor | 1261 | 61.0 | 975 | 77.1 | 286 | 22.9 | |
| Fair | 637 | 33.0 | 545 | 85.1 | 92 | 14.9 | |
| Good | 110 | 6.0 | 99 | 91.5 | 11 | 8.5 | |
| Current Chronic Disease † | 0.0220 | ||||||
| No | 250 | 14.7 | 218 | 86.9 | 32 | 13.1 | |
| Yes | 1758 | 85.3 | 1401 | 79.5 | 357 | 20.5 | |
| Smoking Status | 0.6474 | ||||||
| Ever | 1254 | 59.6 | 1002 | 80.2 | 252 | 19.8 | |
| Never | 754 | 40.4 | 617 | 81.2 | 137 | 18.8 | |
| Alcohol Status | 0.6135 | ||||||
| Ever | 489 | 22.2 | 396 | 81.5 | 93 | 18.5 | |
| Never | 1519 | 77.8 | 1223 | 80.4 | 296 | 19.6 | |
| Variables | UMN | ||
|---|---|---|---|
| Adjusted OR | 95% CI | p-Value | |
| PAR due to people’s own perception of aging | |||
| No | 1.00 | ||
| Yes | 2.13 | (1.27–3.56) | 0.004 |
| Age | |||
| 45–54 | 1.00 | ||
| 55–64 | 1.00 | (0.61–1.62) | 0.984 |
| 65–75 | 0.65 | (0.39–1.10) | 0.107 |
| Over 75 | 0.56 | (0.32–0.96) | 0.034 |
| Gender | |||
| Male | 1.00 | ||
| Female | 1.65 | (1.07–2.54) | 0.022 |
| Marital Status | |||
| Single (including separated and divorced) | 1.00 | - | |
| Married | 1.42 | (1.06–1.90) | 0.018 |
| Education | |||
| ≤Elementary school | 0.93 | (0.46–1.87) | 0.828 |
| Middle school | 0.76 | (0.37–1.55) | 0.450 |
| High school | 0.79 | (0.43–1.45) | 0.443 |
| ≥College | 1.00 | - | |
| Family Income | |||
| Poor | 1.31 | (0.80–2.16) | 0.288 |
| Fair | 0.76 | (0.45–1.27) | 0.293 |
| Good | 1.00 | - | |
| Residency Region | |||
| Capital area | 1.00 | - | |
| Metropolitan city | 0.89 | (0.61–1.30) | 0.546 |
| Rural area | 0.83 | (0.60–1.15) | 0.260 |
| Occupation | |||
| White-collar | 1.00 | - | |
| Blue-collar | 1.02 | (0.59–1.77) | 0.947 |
| Unemployment | 0.67 | (0.26–1.72) | 0.406 |
| Health Insurance Type | |||
| National health insurance (regional) | 1.00 | - | |
| National health insurance (work) | 0.89 | (0.67–1.18) | 0.406 |
| Medical benefits | 0.86 | (0.55–1.34) | 0.498 |
| Self-Rated Health | |||
| Poor | 2.90 | (1.42–5.95) | 0.004 |
| Fair | 1.91 | (0.90–4.04) | 0.089 |
| Good | 1.00 | - | |
| Current Chronic Disease † | |||
| No | 1.00 | - | |
| Yes | 1.45 | (0.90–2.35) | 0.130 |
| Smoking Status | |||
| Ever | 1.00 | - | |
| Never | 1.29 | (0.84–1.99) | 0.244 |
| Alcohol Status | |||
| Ever | 1.00 | - | |
| Never | 1.13 | (0.82–1.57) | 0.449 |
| Variables | UMN | |||
|---|---|---|---|---|
| Male | Female | |||
| Adjusted OR | 95% CI | Adjusted OR | 95% CI | |
| PAR due to people’s own perception of aging | ||||
| No | 1.00 | 1.00 | ||
| Yes | 1.48 | (0.41–5.39) | 2.21 | (1.23–4.00) *** |
| Variables | UMN | |||
| No Current Chronic Disease | Current Chronic Disease | |||
| Adjusted OR | 95% CI | Adjusted OR | 95% CI | |
| PAR due to aging perception | ||||
| No | 1.00 | 1.00 | ||
| Yes | 0.60 | (0.60–5.82) | 2.25 | (1.30–3.89) *** |
| Variables | UMN | |||
| Middle-aged group | Elderly group | |||
| Adjusted OR | 95% CI | Adjusted OR | 95% CI | |
| PAR due to aging perception | ||||
| No | 1.00 | 1.00 | ||
| Yes | 2.14 | (0.89–5.11) | 2.20 | (1.31–3.69) ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, J.-M.; Kim, M.-S.; Hong, J.-S.; Kim, J.-H. Association between Perceived Activity Restriction Due to People’s Perception of Aging and Unmet Medical Needs among Middle-Aged and Elderly People: A Population-Based Study. Medicina 2024, 60, 87. https://doi.org/10.3390/medicina60010087
Yang J-M, Kim M-S, Hong J-S, Kim J-H. Association between Perceived Activity Restriction Due to People’s Perception of Aging and Unmet Medical Needs among Middle-Aged and Elderly People: A Population-Based Study. Medicina. 2024; 60(1):87. https://doi.org/10.3390/medicina60010087
Chicago/Turabian StyleYang, Jeong-Min, Min-Soo Kim, Ji-Sung Hong, and Jae-Hyun Kim. 2024. "Association between Perceived Activity Restriction Due to People’s Perception of Aging and Unmet Medical Needs among Middle-Aged and Elderly People: A Population-Based Study" Medicina 60, no. 1: 87. https://doi.org/10.3390/medicina60010087