

Precise Terminology and Specified Catheter Insertion Length in Ultrasound-Guided Infraclavicular Central Vein Catheterization
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Enrollment and Study Protocol
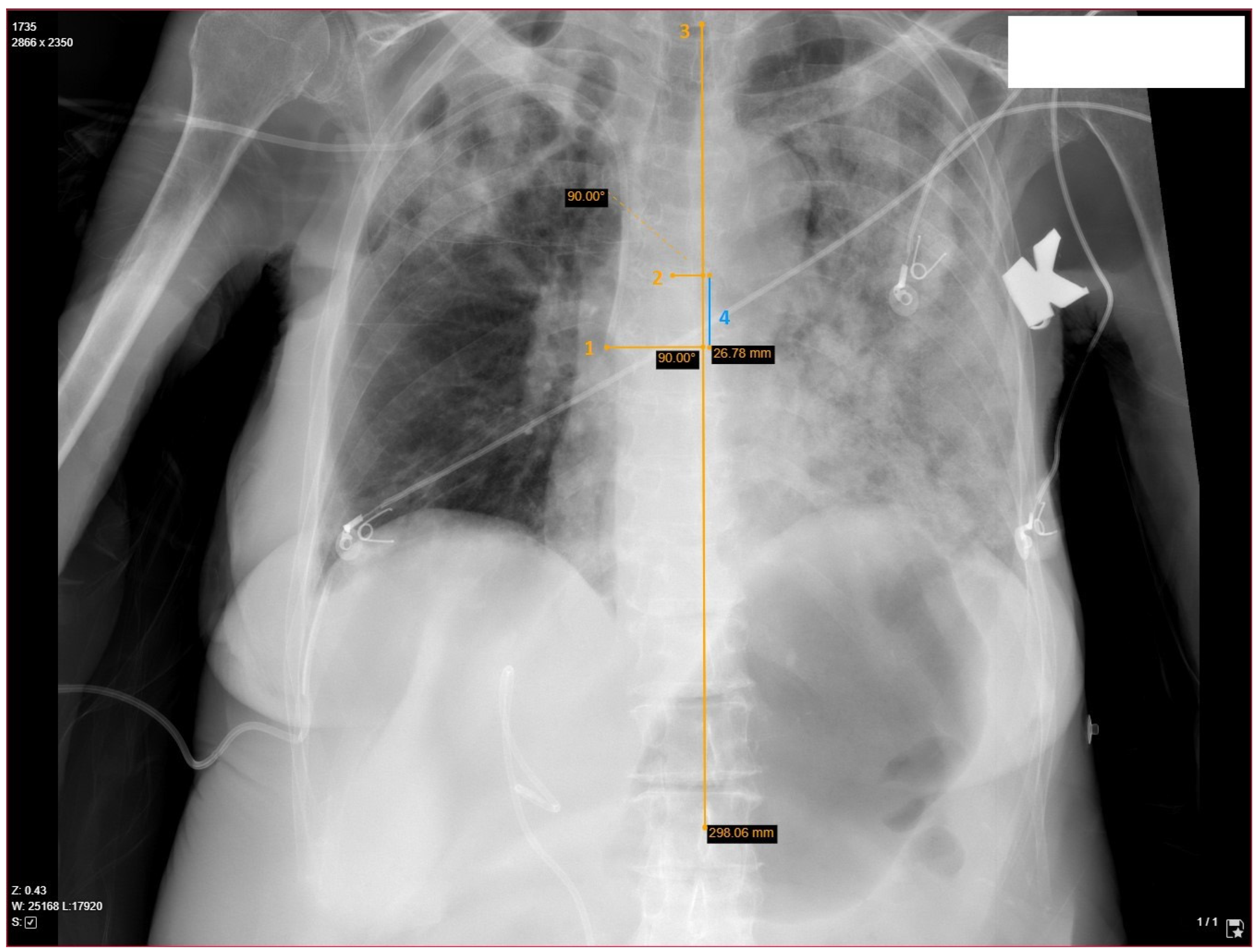
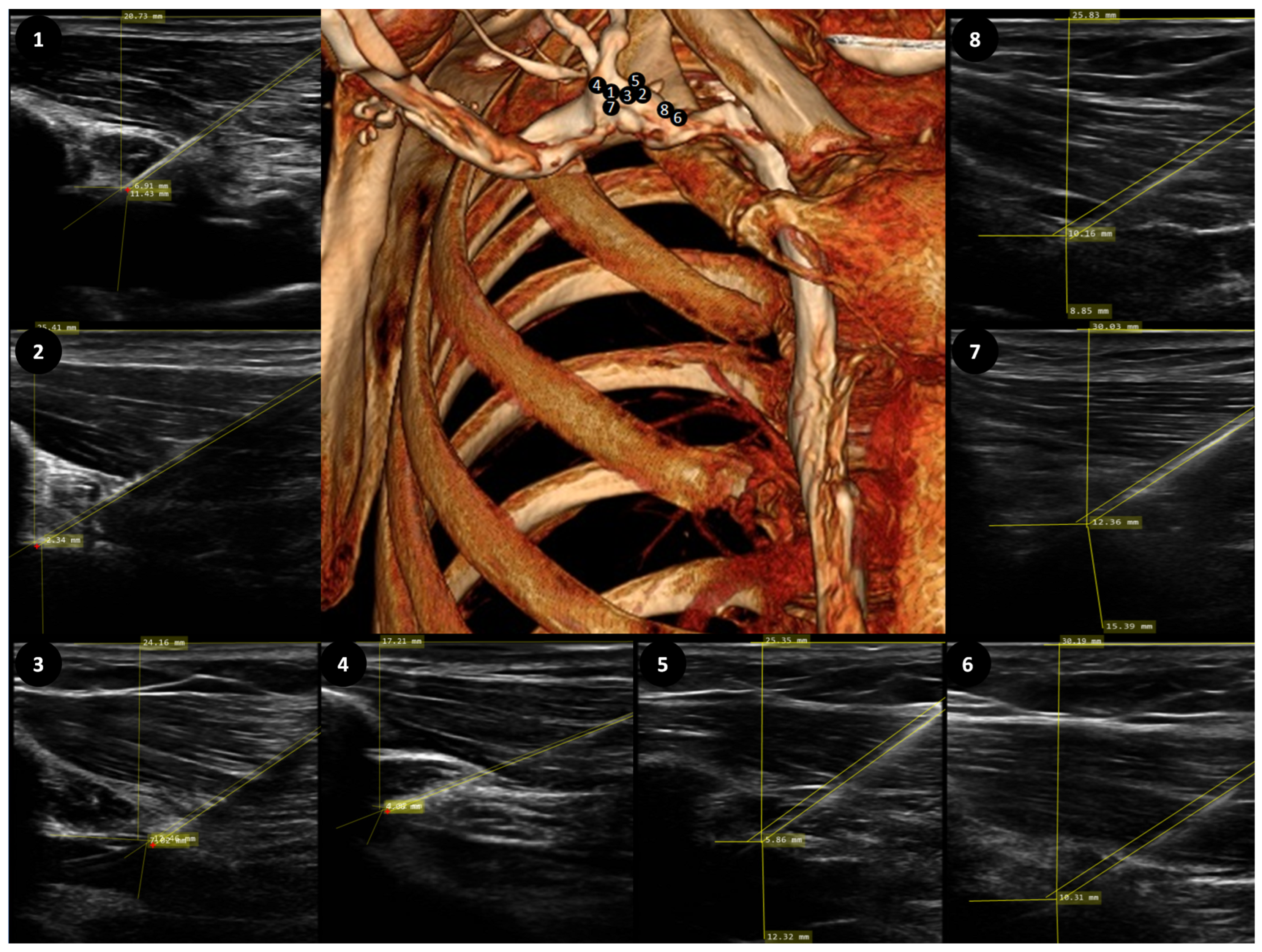
2.3. Determination of Catheter’s Length, Position and Relevant Anatomy
2.4. Statistical Analysis
3. Results
3.1. Demographic and Anatomical Parameters
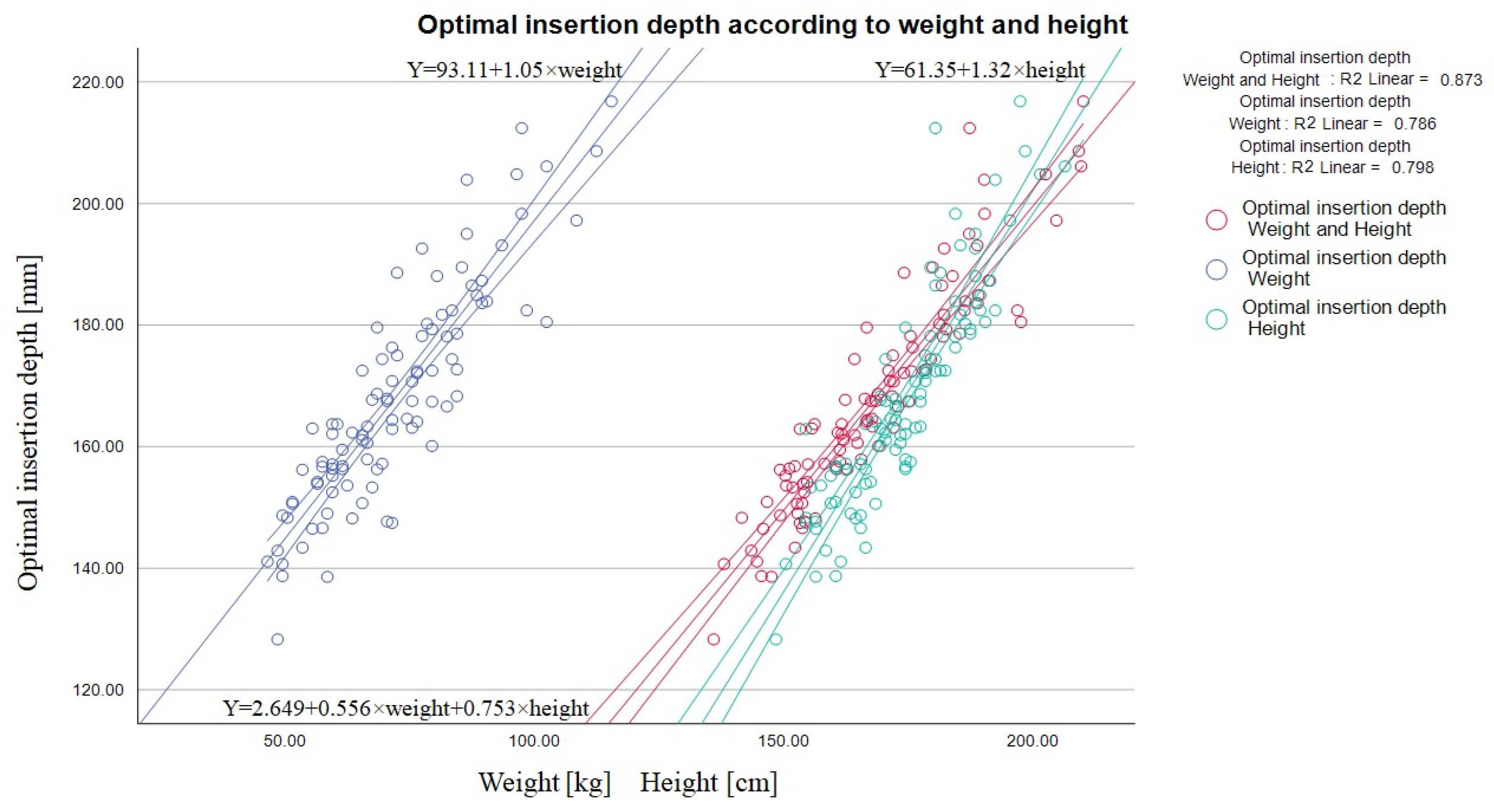
3.2. Predictors of Optimal Catheter Insertion Length
3.3. Precise Terminology
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Žarskus, A.; Zykutė, D.; Trepenaitis, D.; Macas, A. Implementation of Ultrasound-Guided Infraclavicular Subclavian Venous Catheterization During Anesthesia and Elective Surgery: A Prospective Observational Study at a Single Center in Lithuania. Med. Sci. Monit. 2023, 29, e938851. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Bodenham, A.R.; Mallick, A. Ultrasound-guided infraclavicular axillary vein cannulation for central venous access. Br. J. Anaesth. 2004, 93, 188–192, Correction in Br. J. Anaesth. 2004, 93, 752. [Google Scholar] [CrossRef] [PubMed]
- Heffner, A.C.; Andro, M. Placement of Subclavian Venous Catheters; Post, T.W., Ed.; UpToDate Inc.: Waltham, MA, USA, 2022. Available online: www.uptodate.com (accessed on 15 September 2023).
- Shiloh, A.L.; Eisen, L.A.; Yee, M.; Langner, J.B.; LeDonne, J.; Karakitsos, D. Ultrasound-guided subclavian and axillary vein cannulation via an infraclavicular approach: In the tradition of Robert Aubaniac. Crit Care Med. 2012, 40, 2922–2923. [Google Scholar] [CrossRef] [PubMed]
- Biasucci, D.G.; La Greca, A.; Scoppettuolo, G.; Pittiruti, M. Ultrasound-Guided Central Venous Catheterization: It Is High Time to Use a Correct Terminology. Crit. Care Med. 2015, 43, e394-6. [Google Scholar] [CrossRef] [PubMed]
- Peres, P.W. Positioning central venous catheters—A prospective survey. Anaesth Intensive Care 1990, 18, 536–539. [Google Scholar] [CrossRef] [PubMed]
- Stonelake, P.A.; Bodenham, A.R. The carina as a radiological landmark for central venous catheter tip position. Br. J. Anaesth. 2006, 96, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Kujur, R.; Rao, M.S.; Mrinal, M. How correct is the correct length for central venous catheter insertion. Indian J. Crit. Care Med. 2009, 13, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Sivasubramaniam, S.; Hiremath, M. Central Venous Catheters: Do we need to Review Practice on Positioning? J. Intensive Care Soc. 2008, 9, 228–231. [Google Scholar] [CrossRef]
- Cadman, A.; Lawrance, J.A.; Fitzsimmons, L.; Spencer-Shaw, A.; Swindell, R. To clot or not to clot? That is the question in central venous catheters. Clin. Radiol. 2004, 59, 349–355. [Google Scholar] [CrossRef]
- Raad, I.I.; Luna, M.; Khalil, S.A.; Costerton, J.W.; Lam, C.; Bodey, G.P. The relationship between the thrombotic and infectious complications of central venous catheters. JAMA 1994, 271, 1014–1016. [Google Scholar] [CrossRef]
- Timsit, J.F.; Farkas, J.C.; Boyer, J.M.; Martin, J.B.; Misset, B.; Renaud, B.; Carlet, J. Central vein catheter-related thrombosis in intensive care patients: Incidence, risks factors, and relationship with catheter-related sepsis. Chest 1998, 114, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Chabanier, A.; Dany, F.; Brutus, P.; Vergnoux, H. Iatrogenic cardiac tamponade after central venous catheter. Clin. Cardiol. 1988, 11, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Collier, P.E.; Ryan, J.J.; Diamond, D.L. Cardiac tamponade from central venous catheters. Report of a case and review of the English literature. Angiology 1984, 35, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Dane, T.E.B.; King, E.G. Fatal cardiac tamponade and other mechanical complications of central venous catheters. Br. J. Surg. 1975, 62, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Kwon, M.Y.; Lee, E.K.; Kang, H.J.; Kil, H.Y.; Jang, K.H.; Koo, M.S.; Lee, G.H.; Lee, M.A.; Kim, T.Y. The effects of the Trendelenburg position and intrathoracic pressure on the subclavian cross-sectional area and distance from the subclavian vein to pleura in anesthetized patients. Anesth. Analg. 2013, 117, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Ely, E.W.; Hite, R.D.; Baker, A.M.; Johnson, M.M.; Bowton, D.L.; Haponik, E.F. Venous air embolism from central venous catheterization: A need for increased physician awareness. Crit. Care Med. 1999, 27, 2113–2117. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, K.; Nave, H.; Breitmeier, D.; Panning, B.; Tröger, H.D. Applied anatomy of the superior vena cava-the carina as a landmark to guide central venous catheter placement. Br. J. Anaesth. 2004, 92, 75–77. [Google Scholar] [CrossRef] [PubMed]
- Kasten, G.W.; Owens, E.; Kennedy, D. Ventricular Tachycardia Resulting from Central Venous Catheter Tip Migration Due to Arm Position Changes: Report of Two Cases. Anesthesiology 1985, 62, 185–187. [Google Scholar] [CrossRef]
- Food and Drug Administration. Precautions necessary with central venous catheters. FDA Task Force. FDA Drug Bull. 1989, 19, 5. [Google Scholar]
- Pittiruti, M.; Hamilton, H.; Biffi, R.; MacFie, J.; Pertkiewicz, M.; ESPEN. ESPEN Guidelines on Parenteral Nutrition: Central venous catheters (access, care, diagnosis and therapy of complications). Clin. Nutr. 2009, 28, 365–377. [Google Scholar] [CrossRef]
- Morgan, D.; Ho, K.; Murray, C.; Davies, H.; Louw, J. A randomized trial of catheters of different lengths to achieve right atrium versus superior vena cava placement for continuous renal replacement therapy. Am. J. Kidney Dis. 2012, 60, 272–279. [Google Scholar] [CrossRef] [PubMed]
- Joshi, A.M.; Bhosale, G.P.; Parikh, G.P.; Shah, V.R. Optimal positioning of right-sided internal jugular venous catheters: Comparison of intra-atrial electrocardiography versus Peres’ formula. Indian J. Crit. Care Med. 2008, 12, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Gebhard, R.E.; Szmuk, P.; Pivalizza, E.G.; Melnikov, V.; Vogt, C.; Warters, R.D. The accuracy of electrocardiogram-controlled central line placement. Anesth. Analg. 2007, 104, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Jeon, Y.; Ryu, H.G.; Yoon, S.Z.; Kim, J.H.; Bahk, J.H. Transesophageal echocardiographic evaluation of ECG-guided central venous catheter placement. Can. J. Anaesth. 2006, 53, 978–983. [Google Scholar] [CrossRef] [PubMed]
- Caruso, L.J.; Gravenstein, N.; Layon, A.J.; Peters, K.; Gabrielli, A. A better landmark for positioning a central venous catheter. J. Clin. Monit. Comput. 2002, 17, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Schuster, M.; Nave, H.; Piepenbrock, S.; Pabst, R.; Panning, B. The carina as a landmark in central venous catheter placement. Br. J. Anaesth. 2000, 85, 192–194. [Google Scholar] [CrossRef] [PubMed]
- Chin, J.H.; Lee, E.H.; Kim, J.I.; Choi, I.C. Prediction of the optimal depth for superior vena cava cannulae with cardiac computed tomography during minimally invasive cardiac surgery: A prospective observational cohort study. BMC Anesthesiol. 2017, 17, 56. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.Y.; Lee, C.W.; Sohn, C.H.; Seo, D.W.; Yoon, J.C.; Koh, J.W.; Kim, W.; Lim, K.S.; Hong, S.-B.; Lim, C.-M.; et al. Optimal insertion depth of central venous catheters—Is a formula required? A prospective cohort study. Injury 2012, 43, 38–41. [Google Scholar] [CrossRef]
- Choi, Y.J.; Hahm, K.D.; Kwon, K.; Lee, E.H.; Ro, Y.J.; Yang, H.S. Previsão do comprimento de inserção de cateteremveiasubcláviadireita à beira do leito [Bedside prediction of right subclavian venous catheter insertion length]. Rev. Bras. Anestesiol. 2014, 64, 419–424. [Google Scholar] [CrossRef]
- Shin, H.J.; Kim, B.G.; Na, H.S.; Oh, A.Y.; Park, H.P.; Jeon, Y.T. Estimation of catheter insertion depth during ultrasound-guided subclavian venous catheterization. J. Anesth. 2015, 29, 724–727. [Google Scholar] [CrossRef]
- Ryu, H.G.; Bahk, J.H.; Kim, J.T.; Lee, J.H. Bedside prediction of the central venous catheter insertion depth. Br. J. Anaesth. 2007, 98, 225–227. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Kolmogorov–Smirnov Test of Normality | Mean | Std. Error | Std. Dev | |
|---|---|---|---|---|
| Age | 0.200 | 61.33 years | 1.76 | 17.46 |
| Weight | 0.153 | 71.65 kg | 1.54 | 15.29 |
| Height | 0.200 | 173.71 cm | 1.23 | 12.20 |
| Ideal catheter insertion length | 0.73 | 168.03 mm | 1.82 | 18.03 |
| Pere’s predicted insertion length for the right subclavian vein | 0.200 | 153.7 mm | 1.23 | 12.20 |
| Optimal Insertion Length | R | Unstandardized B | Coefficient Std. Error | Standardized Coefficients Beta | Sig. |
|---|---|---|---|---|---|
| Constant | 0.580 | 209.822 | 35.383 | - | <0.001 |
| Vein diameter | 1.646 | 0.562 | 0.272 | 0.004 | |
| Vein depth | 5.571 | 1.822 | 1.687 | 0.003 | |
| Punction path | 2.056 | 0.930 | −0.892 | 0.029 | |
| Punction angle | 2.925 | 1.117 | −0.997 | 0.010 | |
| Constant | 0.934 | −2.649 | 12.247 | - | 0.829 |
| Weight | 0.556 | 0.074 | 0.471 | <0.001 | |
| Height | 0.753 | 0.093 | 0.510 | <0.001 |
| Distance from Vein Entry Point to Clavicle Shadow | Mean (mm) | Std. Error (mm) | Std. Dev (mm) | Median (mm) | Interquartile Range |
|---|---|---|---|---|---|
| Axillary vein | 6.86 | 3.18 | 5.52 | 6.91 | 0.0 |
| Subclavian vein | 8.54 | 1.57 | 3.51 | 10.16 | 15.29 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Žarskus, A.; Zykutė, D.; Lukoševičius, S.; Jankauskas, A.; Trepenaitis, D.; Macas, A. Precise Terminology and Specified Catheter Insertion Length in Ultrasound-Guided Infraclavicular Central Vein Catheterization. Medicina 2024, 60, 28. https://doi.org/10.3390/medicina60010028
Žarskus A, Zykutė D, Lukoševičius S, Jankauskas A, Trepenaitis D, Macas A. Precise Terminology and Specified Catheter Insertion Length in Ultrasound-Guided Infraclavicular Central Vein Catheterization. Medicina. 2024; 60(1):28. https://doi.org/10.3390/medicina60010028
Chicago/Turabian StyleŽarskus, Ainius, Dalia Zykutė, Saulius Lukoševičius, Antanas Jankauskas, Darius Trepenaitis, and Andrius Macas. 2024. "Precise Terminology and Specified Catheter Insertion Length in Ultrasound-Guided Infraclavicular Central Vein Catheterization" Medicina 60, no. 1: 28. https://doi.org/10.3390/medicina60010028