
Pitfalls of DualTracer 99m-Technetium (Tc) Pertechnetate and Sestamibi Scintigraphy before Parathyroidectomy: Between Primary-Hyperparathyroidism-Associated Parathyroid Tumour and Ectopic Thyroid Tissue
 , , and
, , and
Abstract
:1. Introduction
Aim
2. Method
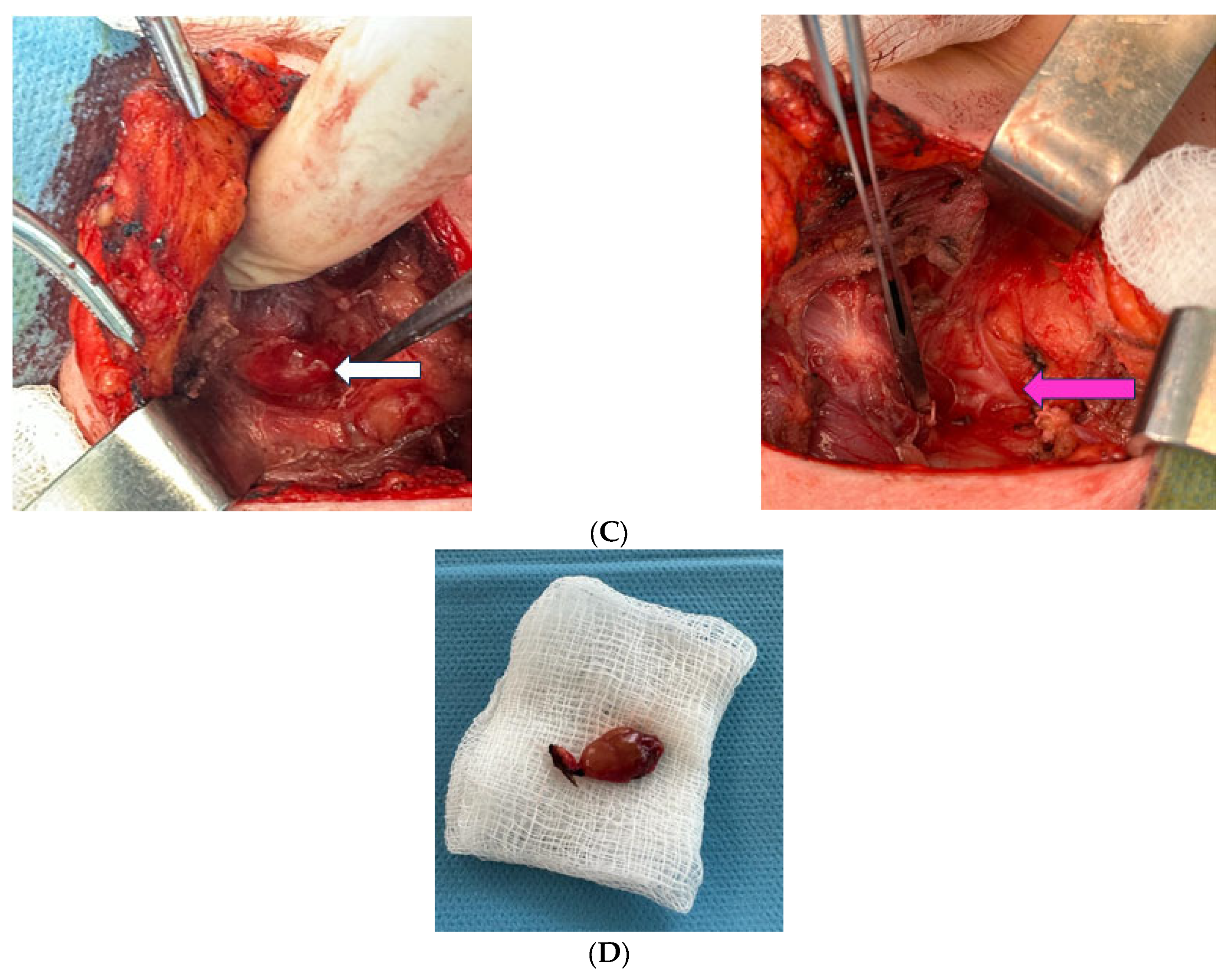
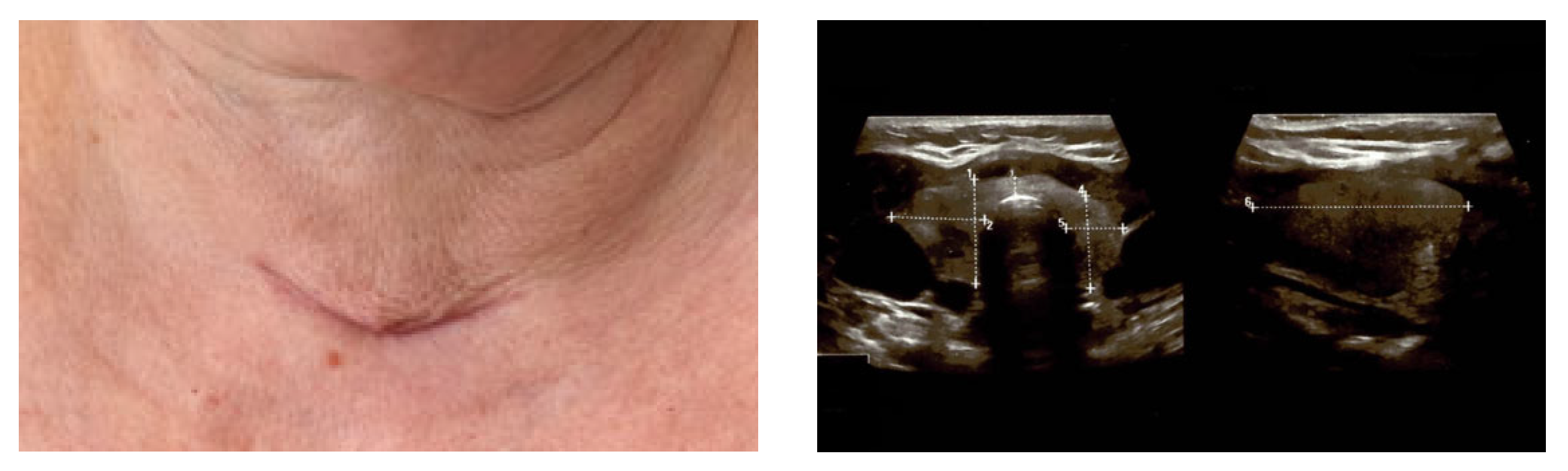
3. Clinical Vignette
4. Discussion
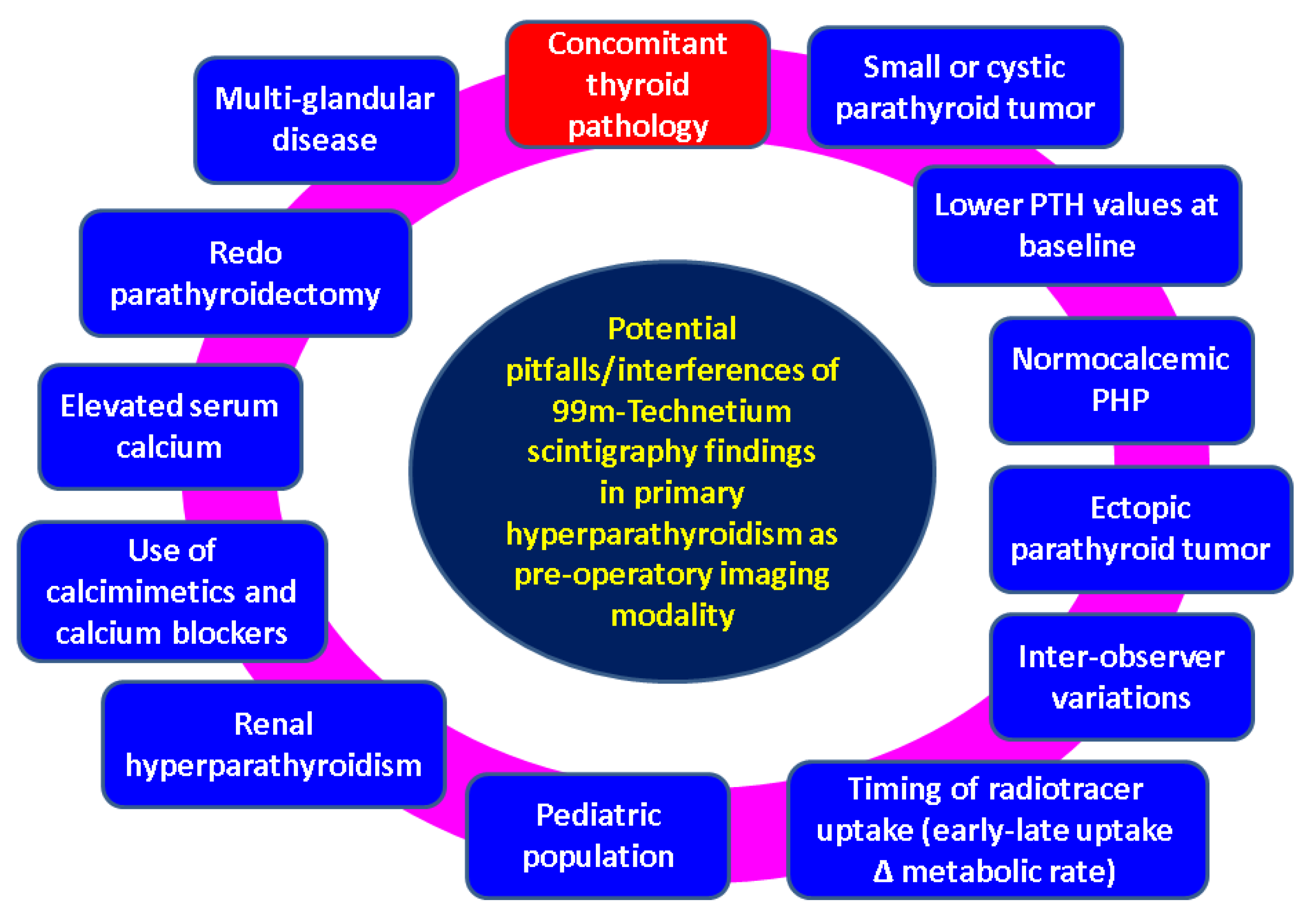
4.1. Imaging Pitfalls in PHP
4.2. Concordance of Pre-Operatory Localisation Studies in PHP
4.3. Ectopic Thyroid Tissue
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CT | computed tomography |
| 4D | four-dimensional |
| DXA | Dual-Energy X-ray Absorptiometry |
| DECT | dual-energy computed tomography |
| MIBI | methoxyisobutylisonitrile |
| 18F-FDG | 18F-fluoro-2-deoxy-d-glucose |
| MRI | magnetic resonance imaging |
| PHP | primary hyperparathyroidism |
| PET | positron emission tomography |
| PTH | parathormone |
| SPECT | single-photon-emission computed tomography |
| Tc | Technetium |
| TBS | trabecular bone score |
References
- Zielke, A.; Smaxwil, C.A. Current approach in cases of persistence and recurrence of primary hyperparathyroidism. Chirurgie 2023, 94, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Bijnens, J.; Van den Bruel, A.; Vander Poorten, V.; Goethals, I.; Van Schandevyl, S.; Dick, C.; De Geeter, F. Retrospective real-life study on preoperative imaging for minimally invasive parathyroidectomy in primary hyperparathyroidism. Sci. Rep. 2022, 12, 17427. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.A.; Saboury, B.; Ahlman, M.; Malayeri, A.A.; Jones, E.C.; Chen, C.C.; Millo, C. Parathyroid Imaging: Past, Present, and Future. Front. Endocrinol. 2022, 12, 760419. [Google Scholar] [CrossRef] [PubMed]
- Strauss, S.B.; Roytman, M.; Phillips, C.D. Parathyroid Imaging: Four-dimensional Computed Tomography, Sestamibi, and Ultrasonography. Neuroimaging Clin. N. Am. 2021, 31, 379–395. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Centeno, N.; Longoria-Dubocq, T.; Mendez-Latalladi, W. Efficacy of 4D CT Scan in Re-operative Parathyroid Surgery. Am. Surg. 2022, 88, 1549–1550. [Google Scholar] [CrossRef]
- Lalonde, M.N.; Correia, R.D.; Syktiotis, G.P.; Schaefer, N.; Matter, M.; Prior, J.O. Parathyroid Imaging. Semin. Nucl. Med. 2023, 53, 490–502. [Google Scholar] [CrossRef] [PubMed]
- Fiz, F.; Bottoni, G.; Massollo, M.; Trimboli, P.; Catrambone, U.; Bacigalupo, L.; Righi, S.; Treglia, G.; Imperiale, A.; Piccardo, A. [18F]F-Choline PET/CT and 4D-CT in the evaluation of primary hyperparathyroidism: Rivals or allies? Q. J. Nucl. Med. Mol. Imaging 2023, 67, 130–137. [Google Scholar] [CrossRef]
- Fendrich, V.; Zahn, A. Localization diagnostics and operative strategy for the first intervention in sporadic primary hyperparathyroidism. Chirurgie 2023, 94, 573–579. [Google Scholar] [CrossRef]
- Park, H.S.; Hong, N.; Jeong, J.J.; Yun, M.; Rhee, Y. Update on Preoperative Parathyroid Localization in Primary Hyperparathyroidism. Endocrinol. Metab. 2022, 37, 744–755. [Google Scholar] [CrossRef]
- Abraham, B.M., Jr.; Sharkey, E.; Kwatampora, L.; Ranzinger, M.; von Holzen, U. Mediastinal Intrathymic Parathyroid Adenoma: A Case Report and Review of the Literature. Cureus 2023, 15, e42306. [Google Scholar] [CrossRef]
- Özçevik, H.; Öner Tamam, M.; Tatoğlu, M.T.; Mülazımoğlu, M. Comparison of Planar Imaging Using Dual-phase Tc-99m-sestamibi Scintigraphy and Single Photon Emission Computed Tomography/Computed Tomography in Hyperparathyroidism. Mol. Imaging Radionucl. Ther. 2022, 31, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Petranović Ovčariček, P.; Giovanella, L.; Hindie, E.; Huellner, M.W.; Talbot, J.N.; Verburg, F.A. An essential practice summary of the new EANM guidelines for parathyroid imaging. Q. J. Nucl. Med. Mol. Imaging 2022, 66, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Petranović Ovčariček, P.; Giovanella, L.; Carrió Gasset, I.; Hindié, E.; Huellner, M.W.; Luster, M.; Piccardo, A.; Weber, T.; Talbot, J.N.; Verburg, F.A. The EANM practice guidelines for parathyroid imaging. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2801–2822. [Google Scholar] [CrossRef] [PubMed]
- Zarei, A.; Karthik, S.; Chowdhury, F.U.; Patel, C.N.; Scarsbrook, A.F.; Vaidyanathan, S. Multimodality imaging in primary hyperparathyroidism. Clin. Radiol. 2022, 77, e401–e416. [Google Scholar] [CrossRef] [PubMed]
- Hanba, C.; Khariwala, S.S. What Is the Optimal Imaging Modality for Parathyroid Adenoma? Laryngoscope 2022, 132, 1508–1509. [Google Scholar] [CrossRef]
- Gök, İ.; Şahbaz, N.A.; Akarsu, C.; Cem Dural, A.; Mert, M.; Erbahçeci Salık, F.A.; Çil, B.E.; Güzey, D.; Alış, H. The role of selective venous sampling in patients with non-localized primary hyperparathyroidism. Turk. J. Surg. 2020, 36, 164–171. [Google Scholar] [CrossRef]
- Uludag, M. Preoperative Localization Studies in Primary Hyperparathyroidism. Med. Bull. Sisli Etfal Hosp. 2017, 53, 7–15. [Google Scholar] [CrossRef]
- Rawat, A.; Grover, M.; Kataria, T.; Samdhani, S.; Mathur, S.; Sharma, B. Minimally Invasive Parathyroidectomy as the Surgical Management of Single Parathyroid Adenomas: A Tertiary Care Experience. Indian J. Otolaryngol. Head Neck Surg. 2023, 75, 271–277. [Google Scholar] [CrossRef]
- Iwen, K.A.; Kußmann, J.; Fendrich, V.; Lindner, K.; Zahn, A. Accuracy of Parathyroid Adenoma Localization by Preoperative Ultrasound and Sestamibi in 1089 Patients with Primary Hyperparathyroidism. World J Surg. 2022, 46, 2197–2205. [Google Scholar] [CrossRef]
- Nistor, C.E.; Stanciu-Găvan, C.; Vasilescu, F.; Dumitru, A.V.; Ciuche, A. Attitude of the surgical approach in hyperparathyroidism: A retrospective study. Exp. Ther. Med. 2021, 22, 959. [Google Scholar] [CrossRef]
- Silva, B.C.; Broy, S.B.; Boutroy, S.; Schousboe, J.T.; Shepherd, J.A.; Leslie, W.D. Fracture Risk Prediction by Non-BMD DXA Measures: The 2015 ISCD Official Positions Part 2: Trabecular Bone Score. J. Clin. Densitom. 2015, 18, 309–330. [Google Scholar] [CrossRef] [PubMed]
- Iacobone, M.; Scerrino, G.; Palazzo, F.F. Parathyroid surgery: An evidence-based volume—Outcomes analysis: European Society of Endocrine Surgeons (ESES) positional statement. Langenbecks Arch. Surg. 2019, 404, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Bilen, N.; Gokalp, M.A.; Yilmaz, L.; Aytekin, A.; Baskonus, I. Analysis of intraoperative laboratory measurements and imaging techniques such as Tc-99 m-MIBI SPECT/CT, 18F-fluorocholine PET/CT and ultrasound in patients operated with prediagnosis of parathyroid adenoma. Ir. J. Med. Sci. 2023, 192, 1695–1702. [Google Scholar] [CrossRef] [PubMed]
- Maccora, D.; Fortini, D.; Moroni, R.; Sprecacenere, G.; Annunziata, S.; Bruno, I. Comparison between MIBI-based radiopharmaceuticals for parathyroid scintigraphy: Quantitative evaluation and correlation with clinical-laboratory parameters. J. Endocrinol. Investig. 2022, 45, 2139–2147. [Google Scholar] [CrossRef] [PubMed]
- Baumgarten, J.; Happel, C.; Ackermann, H.; Grünwald, F. Evaluation of intra- and interobserver agreement of Technetium-99m-sestamibi imaging in cold thyroid nodules. Nuklearmedizin 2017, 56, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Gowrishankar, S.V.; Bidaye, R.; Das, T.; Majcher, V.; Fish, B.; Casey, R.; Masterson, L. Intrathyroidal parathyroid adenomas: Scoping review on clinical presentation, preoperative localization, and surgical treatment. Head Neck 2023, 45, 706–720. [Google Scholar] [CrossRef]
- Neuberger, M.; Dropmann, J.A.; Kleespies, A.; Fuerst, H. Determinants and clinical significance of negative scintigraphic findings in primary hyperparathyroidism: A retrospective observational study. Nuklearmedizin 2022, 61, 440–448. [Google Scholar] [CrossRef]
- Kowalski, G.; Buła, G.; Bednarczyk, A.; Gawrychowska, A.; Gawrychowski, J. Multiglandular Parathyroid Disease. Life 2022, 12, 1286. [Google Scholar] [CrossRef]
- Aktaş, A.; Baskin, E.; Gençoğlu, E.A.; Çolak, T. Comparison of parathyroid scintigraphy findings in pediatric and adult patients with secondary hyperparathyroidism. Nucl. Med. Commun. 2023, 44, 860–863. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, Y.; Li, N.; Zhang, W. Comparison of biochemical markers and technetium 99mmethoxyisobutylisonitrile imaging in primary and secondary hyperparathyroidism. Front. Endocrinol. 2023, 14, 1094689. [Google Scholar] [CrossRef]
- Tlili, G.; Mesguich, C.; Gaye, D.; Tabarin, A.; Haissaguerre, M.; Hindié, E. Dual-tracer 99mTc-sestamibi/123I imaging in primary hyperparathyroidism. Q. J. Nucl. Med. Mol. Imaging 2023, 67, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Benderradji, H.; Beron, A.; Wémeau, J.L.; Carnaille, B.; Delcroix, L.; Do Cao, C.; Baillet, C.; Huglo, D.; Lion, G.; Boury, S.; et al. Quantitative dual isotope 123iodine/99mTc-MIBI scintigraphy: A new approach to rule out malignancy in thyroid nodules. Ann. Endocrinol. 2021, 82, 83–91. [Google Scholar] [CrossRef]
- Thuillier, P.; Benisvy, D.; Ansquer, C.; Corvilain, B.; Mirallié, E.; Taïeb, D.; Borson-Chazot, F.; Lussey-Lepoutre, C. SFE-AFCE-SFMN 2022 Consensus on the management of thyroid nodules: What is the role of functional imaging and isotopic treatment? Ann. Endocrinol. 2022, 83, 401–406. [Google Scholar] [CrossRef]
- Peng, Y.; Pan, G.; Zhao, B.; Zuo, C.; Wang, Y.; Chen, R. Incremental value of 99mTc-MIBI single-photon emission computed tomography/computed tomography fusion imaging for the diagnosis of secondary hyperparathyroidism. Nucl. Med. Commun. 2023, 44, 767–771. [Google Scholar] [CrossRef] [PubMed]
- Sankaran, S.J.; Davidson, J. Diagnosis and localization of parathyroid adenomas using 16-slice SPECT/CT: A clinicopathological correlation. J. Med. Imaging Radiat. Oncol. 2022, 66, 618–622. [Google Scholar] [CrossRef]
- Guo, Y.H.; Huang, J.W.; Wang, Y.; Lu, R.; Yang, M.F. Value of 99mTc-MIBI SPECT/CT in the localization of recurrent lesions in patients with suspected recurrent parathyroid carcinoma. Nucl. Med. Commun. 2023, 44, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Saiz, I.; Goñi-Gironés, E.; Ribelles-Segura, M.J.; Salvador-Egea, P.; Díaz-Tobarra, M.; Camarero-Salazar, A.; Rudic-Chipe, N.; Saura-López, I.; Alomar-Casanovas, A.; Rabines-Juárez, A.; et al. Preoperative parathyroid localization. Relevance of MIBI SPECT-CT in adverse scenarios. Endocrinol. Diabetes Nutr. 2023, 70 (Suppl. S2), 35–44. [Google Scholar] [CrossRef]
- Musumeci, M.; Pereira, L.V.; San Miguel, L.; Cianciarelli, C.; Vazquez, E.C.; Mollerach, A.M.; Arma, I.J.; Hume, I.; Galich, A.M.; Collaud, C. Normocalcemic primary hyperparathyroidism: 99mTc SestaMibi SPECT/CT results compare with hypercalcemic hyperparathyroidism. Clin. Endocrinol. 2022, 96, 831–836. [Google Scholar] [CrossRef]
- Guenette, J.P. Opportunistic CT Screening for Parathyroid Adenoma. Acad. Radiol. 2023, 30, 891–892. [Google Scholar] [CrossRef]
- Lincoln, C.M.M. Editorial Comment: Value-Added Assessment for Parathyroid Adenomas on Routine CT Examinations. AJR Am. J. Roentgenol. 2023, 221, 226. [Google Scholar] [CrossRef]
- Sharma, A.; Patil, V.; Sarathi, V.; Purandare, N.; Hira, P.; Memon, S.; Jadhav, S.S.; Karlekar, M.; Lila, A.R.; Bandgar, T. Dual-phase computed tomography for localization of parathyroid lesions in children and adolescents with primary hyperparathyroidism. Ann. Endocrinol. 2023, 84, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Guo, M.; Lustig, D.B.; Lee, D.; Manhas, N.; Wiseman, S.M. Use of dual energy computed tomography versus conventional techniques for preoperative localization in primary hyperparathyroidism: Effect of preoperative calcium and parathyroid hormone levels. Am. J. Surg. 2023, 225, 852–856. [Google Scholar] [CrossRef] [PubMed]
- Dugonjić, S.; Šišić, M.; Radulović, M.; Ajdinović, B. Positive 99mTc-MIBI and the subtraction parathyroid scan are related to intact parathyroid hormone but not to total plasma calcium in primary hyperparathyroidism. Hell. J. Nucl. Med. 2017, 20, 46–50. [Google Scholar]
- Huynh, K.A.; MacFarlane, J.; Newman, C.; Gillett, D.; Das, T.; Scoffings, D.; Cheow, H.K.; Moyle, P.; Koulouri, O.; Harper, I.; et al. Diagnostic utility of 11C-methionine PET/CT in primary hyperparathyroidism in a UK cohort: A single-centre experience and literature review. Clin. Endocrinol. 2023, 99, 233–245. [Google Scholar] [CrossRef] [PubMed]
- Koumakis, E.; Gauthé, M.; Martinino, A.; Sindayigaya, R.; Delbot, T.; Wartski, M.; Clerc, J.; Roux, C.; Borderie, D.; Cochand-Priollet, B.; et al. FCH-PET/CT in Primary Hyperparathyroidism with Discordant/Negative MIBI Scintigraphy and Ultrasonography. J. Clin. Endocrinol. Metab. 2023, 108, 1958–1967. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.; Vierkant, R.A.; Johnson, G.B.; Parvinian, A.; Wermers, R.A.; Foster, T.; McKenzie, T.; Dy, B.; Lyden, M. C11 choline PET/CT succeeds when conventional imaging for primary hyperparathyroidism fails. Surgery 2023, 173, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Stanciu, M.; Boicean, L.C.; Popa, F.L. The role of combined techniques of scintigraphy and SPECT/CT in the diagnosis of primary hyperparathyroidism: A case report. Medicine 2019, 98, e14154. [Google Scholar] [CrossRef] [PubMed]
- Vestergaard, S.; Gerke, O.; Bay, M.; Madsen, A.R.; Stilgren, L.; Ejersted, C.; Rewers, K.I.; Jakobsen, N.; Asmussen, J.T.; Braad, P.E.; et al. Head-to-Head Comparison of Tc-99m-sestamibi SPECT/CT and C-11-L-Methionin PET/CT in Parathyroid Scanning Before Operation for Primary Hyperparathyroidism. Mol. Imaging Biol. 2023, 25, 720–726. [Google Scholar] [CrossRef]
- Aphale, R.; Damle, N.; Chumber, S.; Khan, M.; Khadgawat, R.; Dharmashaktu, Y.; Agarwal, S.; Bal, C. Impact of Fluoro-Choline PET/CT in Reduction in Failed Parathyroid Localization in Primary Hyperparathyroidism. World J. Surg. 2023, 47, 1231–1237. [Google Scholar] [CrossRef]
- Boudousq, V.; Guignard, N.; Gilly, O.; Chambert, B.; Mamou, A.; Moranne, O.; Zemmour, M.; Sharara, H.; Lallemant, B. Diagnostic Performance of Cervical Ultrasound, 99mTc-Sestamibi Scintigraphy, and Contrast-Enhanced 18F-Fluorocholine PET in Primary Hyperparathyroidism. J. Nucl. Med. 2022, 63, 1081–1086. [Google Scholar] [CrossRef]
- Freesmeyer, M.; Müller, U.A.; Männel, M.; Mtuka-Pardon, G.; Seifert, P. Synchronous Metastatic Medullary Thyroid Carcinoma and Paraesophageal Parathyroid Adenoma Detected on 18F-Ethylcholine PET/US Fusion Imaging. Clin. Nucl. Med. 2022, 47, 977–979. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Dang, Y.; Huo, L.; Hu, Y.; Wang, O.; Liu, H.; Chang, X.; Liu, Y.; Xing, X.; Li, F.; et al. Preoperative Localization of Adenomas in Primary Hyperparathyroidism: The Value of 11C-Choline PET/CT in Patients with Negative or Discordant Findings on Ultrasonography and 99mTc-Sestamibi SPECT/CT. J. Nucl. Med. 2020, 61, 584–589. [Google Scholar] [CrossRef] [PubMed]
- Noltes, M.E.; Rotstein, L.; Eskander, A.; Kluijfhout, W.P.; Bongers, P.; Brouwers, A.H.; Kruijff, S.; Metser, U.; Pasternak, J.D.; Veit-Haibach, P. 18F-fluorocholine PET/MRI versus ultrasound and sestamibi for the localization of parathyroid adenomas. Langenbecks Arch. Surg. 2023, 408, 155. [Google Scholar] [CrossRef] [PubMed]
- Talbot, J.N.; Périé, S.; Tassart, M.; Delbot, T.; Aveline, C.; Zhang-Yin, J.; Kerrou, K.; Gaujoux, S.; Wagner, I.; Bennis, M.; et al. 18F-fluorocholine PET/CT detects parathyroid gland hyperplasia as well as adenoma: 401 PET/CTs in one center. Q. J. Nucl. Med. Mol. Imaging 2023, 67, 96–113. [Google Scholar] [CrossRef] [PubMed]
- Klein, P.; Alsleibi, S.; Cohen, O.; Ilany, J.; Hemi, R.; Barhod, E.; Vered, I.; Winder, O.; Avior, G.; Tripto-Shklonik, L. Parathyroid fine-needle aspiration with parathyroid hormone washout as a preoperative localisation of parathyroid adenoma—A retrospective study. Clin. Endocrinol. 2023, 99, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Prades, J.M.; Lelonge, Y.; Farizon, B.; Chatard, S.; Prevot-Bitot, N.; Gavid, M. Positive predictive values of ultrasound-guided fine-needle aspiration with parathyroid hormone assay and Tc-99m sestamibi scintigraphy in sporadic primary hyperparathyroidism. Eur. Ann. Otorhinolaryngol. Head. Neck Dis. 2023, 140, 3–7. [Google Scholar] [CrossRef]
- Amjad, W.; Trerotola, S.O.; Fraker, D.L.; Wachtel, H. Tricks of the trade: Techniques for preoperative localization in reoperative parathyroidectomy. Am. J. Surg. 2023, 226, 207–212. [Google Scholar] [CrossRef]
- Hiramitsu, T.; Hasegawa, Y.; Futamura, K.; Okada, M.; Goto, N.; Narumi, S.; Watarai, Y.; Tominaga, Y.; Ichimori, T. Intraoperative intact parathyroid hormone monitoring and frozen section diagnosis are essential for successful parathyroidectomy in secondary hyperparathyroidism. Front. Med. 2022, 9, 1007887. [Google Scholar] [CrossRef]
- Akgün, I.E.; Ünlü, M.T.; Aygun, N.; Kostek, M.; Uludag, M. Contribution of intraoperative parathyroid hormone monitoring to the surgical success in minimal invasive parathyroidectomy. Front. Surg. 2022, 9, 1024350. [Google Scholar] [CrossRef]
- Habib, A.; Molena, E.; Snowden, C.; England, J. Efficacy of surgeon-performed, intra-operative ultrasound scan for localisation of parathyroid adenomas in patients with primary hyperparathyroidism. J. Laryngol. Otol. 2023, 137, 910–913. [Google Scholar] [CrossRef]
- Girotti, P.N.C.; Gassner, J.; Hodja, V.; Tschann, P.; Königsrainer, I. “Before skin incision” high-resolution ultrasound in primary hyperparathyroidism: A new imaging tool for surgeons? Langenbecks Arch. Surg. 2022, 407, 3643–3649. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Jayaram, A.; Bresnahan, E.; Pletcher, E.; Steinmetz, D.; Owen, R.; Inabnet, W., III; Fernandez-Ranvier, G.; Taye, A. The Role of Surgeon-Performed Office and Preincision Ultrasounds in Localization of Parathyroid Adenomas in Primary Hyperparathyroidism. Endocr. Pract. 2022, 28, 660–666. [Google Scholar] [CrossRef] [PubMed]
- Ishii, S.; Sugawara, S.; Yaginuma, Y.; Kobiyama, H.; Hiruta, M.; Watanabe, H.; Yamakuni, R.; Hakozaki, M.; Fujimaki, H.; Ito, H. Causes of false negatives in technetium-99mmethoxyisobutylisonitrile scintigraphy for hyperparathyroidism: Influence of size and cysts in parathyroid lesions. Ann. Nucl. Med. 2020, 34, 892–898. [Google Scholar] [CrossRef] [PubMed]
- Stanciu, M.; Ristea, R.P.; Popescu, M.; Vasile, C.M.; Popa, F.L. Thyroid Carcinoma Showing Thymus-like Differentiation (CASTLE): A Case Report. Life 2022, 12, 1314. [Google Scholar] [CrossRef] [PubMed]
- Saowapa, S.; Chamroonrat, W.; Suvikapakornkul, R.; Sriphrapradang, C. Incidental breast lesion detected by technetium-99m sestamibi scintigraphy in a patient with primary hyperparathyroidism. World J. Nucl. Med. 2019, 19, 69–71. [Google Scholar] [CrossRef]
- Dumitru, N.; Ghemigian, A.; Carsote, M.; Albu, S.E.; Terzea, D.; Valea, A. Thyroid nodules after initial evaluation by primary health care practitioners: An ultrasound pictorial essay. Arch. Balk. Med. Union 2016, 51, 434–438. [Google Scholar]
- Stanciu, M.; Zaharie, I.S.; Bera, L.G.; Cioca, G. Correlations between the presence of Hürthle cells and cytomorphological features of fine-needle aspiration biopsy in thyroid nodules. Acta Endocrinol. 2016, 12, 485–490. [Google Scholar] [CrossRef]
- Lee, J.Y.; Song, H.S.; Choi, J.H.; Hyun, C.L.; Lee, S.A.; Choi, J.H.; Lee, S. Detecting Synchronous Thyroid Adenoma and False-Positive Findings on Technetium-99m MIBI Single Photon-Emission Computed Tomography/Computed Tomography. Diagnostics 2019, 9, 57. [Google Scholar] [CrossRef]
- Paillahueque, G.; Massardo, T.; Barberán, M.; Ocares, G.; Gallegos, I.; Toro, L.; Araya, A.V. False negative spect parathyroid scintigraphy with sestamibi in patients with primary hyperparathyroidism. Rev. Med. Chil. 2017, 145, 1021–1027. [Google Scholar] [CrossRef]
- Carral, F.; Jiménez, A.I.; Tomé, M.; Álvarez, J.; Díez, A.; Partida, F.; Ayala, C. Factors associated with negative 99mTc-MIBI scanning in patients with primary hyperparathyroidism. Rev. Esp. Med. Nucl. Imagen Mol. 2021, 40, 222–228. [Google Scholar] [CrossRef]
- Filser, B.; Uslar, V.; Weyhe, D.; Tabriz, N. Predictors of adenoma size and location in primary hyperparathyroidism. Langenbecks Arch. Surg. 2021, 406, 1607–1614. [Google Scholar] [CrossRef] [PubMed]
- Buicko, J.L.; Kichler, K.M.; Amundson, J.R.; Scurci, S.; Kozol, R.A. The Sestamibi Paradox: Improving Intraoperative Localization of Parathyroid Adenomas. Am. Surg. 2017, 83, 832–835. [Google Scholar] [CrossRef] [PubMed]
- Palot Manzil, F.F.; Eichhorn, J.; Vattoth, S. Synchronous Ectopic Thyroid Gland and Ectopic Parathyroid Adenoma on 99mTc-Sestamibi Scintigraphy and Correlative Imaging. J. Nucl. Med. Technol. 2023, 51, 263–264. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Liu, F.; Chen, K.; Wang, Y.; Dou, J.; Mu, Y.; Lyu, Z.; Zang, L. Case report: Coexistence of primary hyperparathyroidism with giant toxic nodular goiter. BMC Endocr. Disord. 2022, 22, 200. [Google Scholar] [CrossRef]
- Cansu, G.B.; Taşkıran, B.; Bahçeci, T. Thyroid Hemiagenesis Associated with Graves’ Disease: A Case Report and Review of the Literature. Acta Endocrinol. 2017, 13, 342–348. [Google Scholar] [CrossRef]
- Lesi, O.K.; Thapar, A.; Appaiah, N.N.B.; Iqbal, M.R.; Kumar, S.; Maharaj, D.; Saad Abdalla Al-Zawi, A.; Dindyal, S. Thyroid Hemiagenesis: Narrative Review and Clinical Implications. Cureus 2022, 14, e22401. [Google Scholar] [CrossRef]
- Ren, Y.; Jiang, G.; Meng, Y.; Chen, J.; Liu, J. 99mTc-pertechnetate thyroid static scintigraphy unexpectedly revealed ectopic gastric mucosa of upper esophagus. Hell. J. Nucl. Med. 2023, 26, 157–159. [Google Scholar]
- Giovanella, L.; Petranović Ovčariček, P. Functional and molecular thyroid imaging. Q. J. Nucl. Med. Mol. Imaging 2022, 66, 86–92. [Google Scholar] [CrossRef]
- Campennì, A.; Giovanella, L.; Siracusa, M.; Alibrandi, A.; Pignata, S.A.; Giovinazzo, S.; Trimarchi, F.; Ruggeri, R.M.; Baldari, S.; Trimboli, P.; et al. (99m)Tc-Methoxy-Isobutyl-Isonitrile Scintigraphy Is a Useful Tool for Assessing the Risk of Malignancy in Thyroid Nodules with Indeterminate Fine-Needle Cytology. Thyroid 2016, 26, 1101–1109. [Google Scholar] [CrossRef]
- Campennì, A.; Siracusa, M.; Ruggeri, R.M.; Laudicella, R.; Pignata, S.A.; Baldari, S.; Giovanella, L. Differentiating malignant from benign thyroid nodules with indeterminate cytology by 99mTc-MIBI scan: A new quantitative method for improving diagnostic accuracy. Sci. Rep. 2017, 7, 6147. [Google Scholar] [CrossRef]
- Arabi, M.; Zamani, H.; Soltanabadi, M.; Kalhor, L. [99mTc]MIBI scintigraphy in a patient with thyroid follicular neoplasm: A case report and review of literature. Nucl. Med. Rev. Cent. East. Eur. 2021, 24, 118–119. [Google Scholar] [CrossRef] [PubMed]
- Schenke, S.A.; Görges, R.; Seifert, P.; Zimny, M.; Kreissl, M.C. Update on diagnosis and treatment of hyperthyroidism: Ultrasonography and functional imaging. Q. J. Nucl. Med. Mol. Imaging 2021, 65, 102–112. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Patient’s Value | Normal Range |
|---|---|---|
| Total serum calcium (mg/dL) | 11.3 | 8.5–10.2 |
| Ionised calcium (mg/dL) | 5.07 | 3.9–4.9 |
| Total proteins(g/dL) | 6.8 | 6.5–8.7 |
| Phosphorus (mg/dL) | 2.8 | 2.5–4.5 |
| Creatinine (mg/dL) | 0.77 | 0.5–1.1 |
| Urea (mg/dL) | 35 | 15–50 |
| Hormones of mineral metabolism | ||
| 25-hydroxyvitamin D (ng/mL) | 34 | 20–100 |
| PTH (pg/mL) | 103.1 | 15–65 |
| Bone turnover markers | ||
| Osteocalcin (ng/mL) * | 48.2 | 15–46 |
| Alkaline phosphatase(U/L) * | 117 | 38–105 |
| P1NP (ng/mL) * | 103.1 | 14.28–58.92 |
| CrossLaps (ng/mL) ** | 1.05 | 0.33–0.782 |
| Region | Bone Mineral Density (g/cm2) | T-Score (SD) | Z-Score (SD) |
|---|---|---|---|
| Lumbar spine L1–4 | 0.764 | −3.5 | −2.5 |
| Femoral neck | 0.640 | −2.8 | −1.9 |
| Total hip | 0.606 | −3.3 | −2.6 |
| 1/3 distal radius | 0.592 | −3.2 | −2.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carsote, M.; Stanciu, M.; Popa, F.L.; Sima, O.-C.; Petrova, E.; Cucu, A.-P.; Nistor, C. Pitfalls of DualTracer 99m-Technetium (Tc) Pertechnetate and Sestamibi Scintigraphy before Parathyroidectomy: Between Primary-Hyperparathyroidism-Associated Parathyroid Tumour and Ectopic Thyroid Tissue. Medicina 2024, 60, 15. https://doi.org/10.3390/medicina60010015
Carsote M, Stanciu M, Popa FL, Sima O-C, Petrova E, Cucu A-P, Nistor C. Pitfalls of DualTracer 99m-Technetium (Tc) Pertechnetate and Sestamibi Scintigraphy before Parathyroidectomy: Between Primary-Hyperparathyroidism-Associated Parathyroid Tumour and Ectopic Thyroid Tissue. Medicina. 2024; 60(1):15. https://doi.org/10.3390/medicina60010015
Chicago/Turabian StyleCarsote, Mara, Mihaela Stanciu, Florina Ligia Popa, Oana-Claudia Sima, Eugenia Petrova, Anca-Pati Cucu, and Claudiu Nistor. 2024. "Pitfalls of DualTracer 99m-Technetium (Tc) Pertechnetate and Sestamibi Scintigraphy before Parathyroidectomy: Between Primary-Hyperparathyroidism-Associated Parathyroid Tumour and Ectopic Thyroid Tissue" Medicina 60, no. 1: 15. https://doi.org/10.3390/medicina60010015