
Pituitary-Related Adverse Events and Onset Patterns Caused by Immune Checkpoint Inhibitors: Analysis Using the Japanese Adverse Drug Event Report Database

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Target Adverse Events and Target Drugs
2.3. Subsection
2.3.1. Disproportionality Analysis
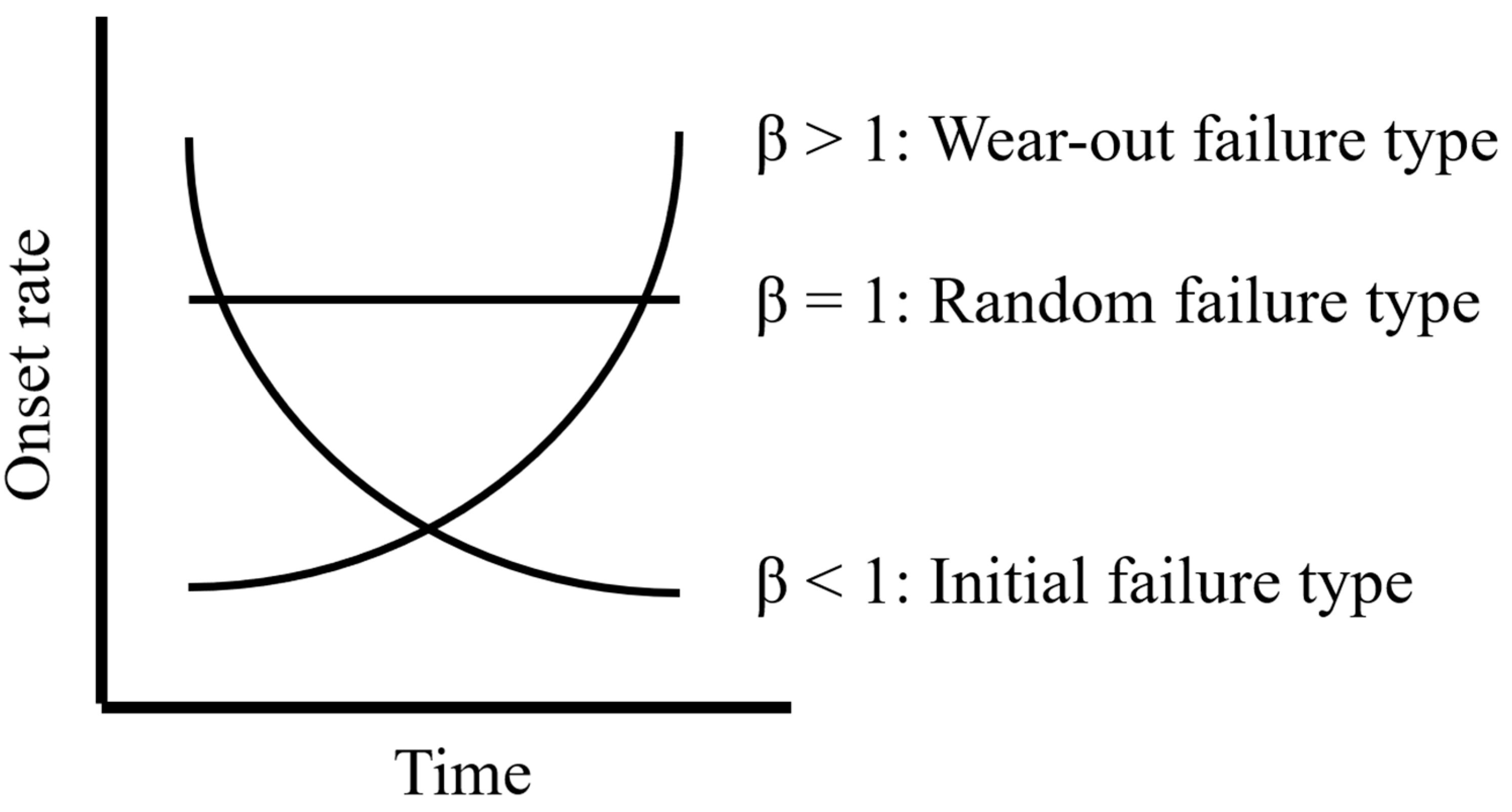
2.3.2. Weibull Analysis
3. Results
3.1. Signal Score for Pituitary-Related Adverse Events for Each ICI
3.2. Analysis of the Onset Pattern of Pituitary-Related Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gente, K.; Diekmann, L.; Daniello, L.; Will, J.; Feisst, M.; Olsavszky, V.; Günther, J.; Lorenz, H.M.; Souto-Carneiro, M.M.; Hassel, J.C.; et al. Sex and anti-inflammatory treatment affect outcome of melanoma and non-small cell lung cancer patients with rheumatic immune-related adverse events. J. Immunother. Cancer 2023, 11, e007557. [Google Scholar] [CrossRef] [PubMed]
- Haanen, J.B.; Thienen, H.; Blank, C.U. Toxicity patterns with immunomodulating antibodies and their combinations. Semin. Oncol. 2015, 42, 423–428. [Google Scholar] [CrossRef]
- Van der Kooij, M.K.; Suijkerbuijk, K.P.M.; Aarts, M.J.B.; van den Berkmortel, F.W.P.J.; Blank, C.U.; Boers-Sonderen, M.J.; van Breeschoten, J.; van den Eertwegh, A.J.M.; de Groot, J.W.B.; Haanen, J.B.A.G.; et al. Safety and Efficacy of Checkpoint Inhibition in Patients with Melanoma and Preexisting Autoimmune Disease: A Cohort Study. Ann. Intern. Med. 2021, 174, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, A.; Buti, S.; Santini, D.; Perrone, F.; Giusti, R.; Tiseo, M.; Bersanelli, M.; Michiara, M.; Grassadonia, A.; Brocco, D.; et al. Clinical Outcomes of Patients with Advanced Cancer and Pre-Existing Autoimmune Diseases Treated with Anti-Programmed Death-1 Immunotherapy: A Real-World Transverse Study. Oncologist 2019, 24, e327–e337. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Johnson, D.B. Immune-related adverse events and anti-tumor efficacy of immune checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 306. [Google Scholar] [CrossRef] [PubMed]
- Postow, M.A.; Sidlow, R.; Hellmann, M.D. Immune-related adverse events associated with immune checkpoint blockade. N. Engl. J. Med. 2018, 378, 158–168. [Google Scholar] [CrossRef]
- Mangan, B.L.; McAlister, R.K.; Balko, J.M.; Johnson, D.B.; Moslehi, J.J.; Gibson, A.; Phillips, E.J. Evolving insights into the mechanisms of toxicity associated with immune checkpoint inhibitor therapy. Br. J. Clin. Pharmacol. 2020, 86, 778–1789. [Google Scholar] [CrossRef]
- Liu, M.; Christ, L.; Richters, A.; Özdemir, B.C. Toxicity, disease management and outcome of treatment with immune checkpoint inhibitors by sex in patients with cancer and preexisting autoimmune disease. Oncol. Lett. 2023, 26, 377. [Google Scholar] [CrossRef]
- Postow, M.A. Managing immune checkpoint-blocking antibody side effects. Am. Soc. Clin. Oncol. Educ. Book 2015, 76–83. [Google Scholar] [CrossRef]
- Lemery, S.; Keegan, P.; Pazdur, R. First FDA approval agnostic of cancer site-when a biomarker defines the indication. N. Engl. J. Med. 2017, 377, 1409–1412. [Google Scholar] [CrossRef]
- Wang, D.Y.; Salem, J.E.; Cohen, J.V.; Chandra, S.; Menzer, C.; Ye, F.; Zhao, S.; Das, S.; Beckermann, K.E.; Ha, L.; et al. Fatal toxic effects associated with immune checkpoint inhibitors: A systematic review and meta-analysis. JAMA Oncol. 2018, 4, 1721–1728. [Google Scholar] [CrossRef] [PubMed]
- Mizukoshi, T.; Fukuoka, H.; Takahashi, Y. Immune checkpoint inhibitor—Related hypophysitis. Best Pract. Res. Clin. Endocrinol. Metab. 2022, 36, 101668. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.J.; Powers, A.C.; Johnson, D.B. Endocrine toxicities of immune checkpoint inhibitors. Nat. Rev. Endocrinol. 2021, 17, 389–399. [Google Scholar] [CrossRef] [PubMed]
- Arlt, W.; Allolio, B. Adrenal insufficiency. Lancet 2003, 361, 1881–1893. [Google Scholar] [CrossRef]
- Bergthorsdottir, R.; Leonsson-Zachrisson, M.; Odén, A.; Johannsson, G. Premature mortality in patients with Addison’s disease: A population-based study. J. Clin. Endocrinol. Metab. 2006, 91, 4849–4853. [Google Scholar] [CrossRef]
- Caturegli, P.; Di Dalmazi, G.; Lombardi, M.; Grosso, F.; Larman, H.B.; Larman, T.; Taverna, G.; Cosottini, M.; Lupi, I. Hypophysitis Secondary to Cytotoxic T-Lymphocyte-Associated Protein 4 Blockade: Insights into Pathogenesis from an Autopsy Series. Am. J. Pathol. 2016, 186, 3225–3235. [Google Scholar] [CrossRef]
- Iwama, S.; De Remigis, A.; Callahan, M.K.; Slovin, S.F.; Wolchok, J.D.; Caturegli, P. Pituitary expression of CTLA-4 mediates hypophysitis secondary to administration of CTLA-4 blocking antibody. Sci. Transl. Med. 2014, 6, 230ra45. [Google Scholar] [CrossRef]
- Faje, A. Immunotherapy and hypophysitis: Clinical presentation, treatment, and biologic insights. Pituitary 2016, 19, 82–92. [Google Scholar] [CrossRef]
- Kobayashi, T.; Iwama, S.; Yasuda, Y.; Okada, N.; Okuji, T.; Ito, M.; Onoue, T.; Goto, M.; Sugiyama, M.; Tsunekawa, T.; et al. Pituitary dysfunction induced by immune checkpoint inhibitors is associated with better overall survival in both malignant melanoma and non-small cell lung carcinoma: A prospective study. J. Immunother. Cancer 2020, 8, e000779. [Google Scholar] [CrossRef]
- Labadzhyan, A.; Wentzel, K.; Hamid, O.; Chow, K.; Kim, S.; Piro, L.; Melmed, S. Endocrine Autoantibodies Determine Immune Checkpoint Inhibitor-induced Endocrinopathy: A Prospective Study. J. Clin. Endocrinol. Metab. 2022, 107, 1976–1982. [Google Scholar] [CrossRef]
- Kotwal, A.; Rouleau, S.G.; Dasari, S.; Kottschade, L.; Ryder, M.; Kudva, Y.C.; Markovic, S.; Erickson, D. Immune checkpoint inhibitor-induced hypophysitis: Lessons learnt from a large cancer cohort. J. Investig. Med. 2022, 70, 939–946. [Google Scholar] [CrossRef] [PubMed]
- Yingying, H.; Jian, G.; Lifu, Z.; Xiaolin, L.; Xina, L.; Bin, Z.; Xin, H. Colitis following the use of immune checkpoint inhibitors: A real-world analysis of spontaneous reports submitted to the FDA adverse event reporting system. Int. Immunopharmacol. 2020, 84, 106601. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, K.; Kozuka, Y.; Uno, H.; Utsumi, K.; Noyori, O.; Hosoki, R. Spontaneous and immune checkpoint inhibitor-induced autoimmune diseases: Analysis of temporal information by using the Japanese adverse drug event report database. Clin. Drug Investig. 2021, 41, 615–627. [Google Scholar] [CrossRef] [PubMed]
- Noguchi, Y.; Tachi, T.; Teramachi, H. Detection algorithms and attentive points of safety signal using spontaneous reporting systems as a clinical data source. Brief. Bioinform. 2021, 22, bbab347. [Google Scholar] [CrossRef] [PubMed]
- Bate, A.; Lindquist, M.; Edwards, I.R.; Olsson, S.; Orre, R.; Lansner, A.; De Freitas, R.M. A Bayesian neural network method for adverse drug reaction signal generation. Eur. J. Clin. Pharmacol. 1998, 54, 315–321. [Google Scholar] [CrossRef]
- Norén, G.N.; Hopstadius, J.; Bate, A. Shrinkage observed-to-expected ratios for robust and transparent large-scale pattern discovery. Stat. Methods Med. Res. 2013, 22, 57–69. [Google Scholar] [CrossRef]
- Sandberg, L.; Taavola, H.; Aoki, Y.; Chandler, R.; Norén, G.N. Risk Factor Considerations in Statistical Signal Detection: Using Subgroup Disproportionality to Uncover Risk Groups for Adverse Drug Reactions in VigiBase. Drug Saf. 2020, 43, 999–1009. [Google Scholar] [CrossRef]
- Sauzet, O.; Carvajal, A.; Escudero, A.; Molokhia, M.; Cornelius, V.R. Illustration of the weibull shape parameter signal detection tool using electronic healthcare record data. Drug Saf. 2013, 36, 995–1006. [Google Scholar] [CrossRef]
- Arima, H.; Iwama, S.; Inaba, H.; Ariyasu, H.; Makita, N.; Otsuki, M.; Kageyama, K.; Imagawa, A.; Akamizu, T. Management of immune-related adverse events in endocrine organs induced by immune checkpoint inhibitors: Clinical guidelines of the Japan Endocrine Society. Endocr. J. 2019, 66, 581–586. [Google Scholar] [CrossRef]
- Available online: https://www.opdivo.jp/system/files/2023-03/OPD_guide.pdf (accessed on 26 September 2023).
- Hasegawa, S.; Ikesue, H.; Nakao, S.; Shimada, K.; Mukai, R.; Tanaka, M.; Matsumoto, K.; Inoue, M.; Satake, R.; Yoshida, Y.; et al. Analysis of immune-related adverse events caused by immune checkpoint inhibitors using the Japanese Adverse Drug Event Report database. Pharmacoepidemiol. Drug Saf. 2020, 29, 1279–1294. [Google Scholar] [CrossRef]
- Santini, F.C.; Rizvi, H.; Plodkowski, A.J.; Ni, A.; Lacouture, M.E.; Gambarin-Gelwan, M.; Wilkins, O.; Panora, E.; Halpenny, D.F.; Long, N.M.; et al. Safety and Efficacy of Re-Treating with Immunotherapy after Immune-Related Adverse Events in Patients with NSCLC. Cancer Immunol. Res. 2018, 6, 1093–1099. [Google Scholar] [CrossRef] [PubMed]
- Jing, Y.; Zhang, Y.; Wang, J.; Li, K.; Chen, X.; Heng, J.; Gao, Q.; Ye, Y.; Zhang, Z.; Liu, Y.; et al. Association Between Sex and Immune-Related Adverse Events During Immune Checkpoint Inhibitor Therapy. J. Natl. Cancer Inst. 2021, 113, 1396–1404. [Google Scholar] [CrossRef]
- Ishikawa, Y.; Yoneyama, E.; Takaki, A.; Takahashi, N.; Ono, A.; Kato, A.; Adachi, I. Safety Evaluation of Retreatment with Immune Checkpoint Inhibitors. Jpn. J. Pharm. Health Care Sci. 2019, 45, 659–666. [Google Scholar] [CrossRef]
- Yang, F.; Shay, C.; Abousaud, M.; Tang, C.; Li, Y.; Qin, Z.; Saba, N.F.; Teng, Y. Patterns of toxicity burden for FDA-approved immune checkpoint inhibitors in the United States. J. Exp. Clin. Cancer Res. 2023, 42, 4. [Google Scholar] [CrossRef] [PubMed]
- Unger, J.M.; Vaidya, R.; Albain, K.S.; LeBlanc, M.; Minasian, L.M.; Gotay, C.C.; Henry, N.L.; Fisch, M.J.; Lee, S.M.; Blanke, C.D.; et al. Sex Differences in Risk of Severe Adverse Events in Patients Receiving Immunotherapy, Targeted Therapy, or Chemotherapy in Cancer Clinical Trials. J. Clin. Oncol. 2022, 40, 1474–1486. [Google Scholar] [CrossRef] [PubMed]
- Di Dalmazi, G.; Ippolito, S.; Lupi, I.; Caturegli, P. Hypophysitis induced by immune checkpoint inhibitors: A 10-year assessment. Expert. Rev. Endocrinol. Metab. 2019, 14, 381–398. [Google Scholar] [CrossRef] [PubMed]
- Ko, M.; Oh, J.M.; Kim, I.W. Drug repositioning prediction for psoriasis using the adverse event reporting database. Front. Med. 2023, 10, 1159453. [Google Scholar] [CrossRef]
- Barnabei, A.; Corsello, A.; Paragliola, R.M.; Iannantuono, G.M.; Falzone, L.; Corsello, S.M.; Torino, F. Immune Checkpoint Inhibitors as a Threat to the Hypothalamus-Pituitary Axis: A Completed Puzzle. Cancers 2022, 14, 1057. [Google Scholar] [CrossRef]
- Jo, K., III. Hypothalamic Syndrome: Key Points and Precautions for Diagnosis and Treatment. Nihon Naika Gakkai Zasshi 1994, 83, 2052–2507. [Google Scholar] [CrossRef]
- Tshuma, N.; Glynn, N.; Evanson, J.; Powles, T.; Drake, W.M. Hypothalamitis and severe hypothalamic dysfunction associated with anti-programmed cell death ligand 1 antibody treatment. Eur. J. Cancer 2018, 104, 247–249. [Google Scholar] [CrossRef]
- Available online: https://www.opdivo.jp/system/files/2023-06/side_effect.pdf (accessed on 30 September 2023).
- Weber, J. Epidemiology of adverse reactions to nonsteroidal anti-inflammatory drugs. Adv. Inflamm. Res. 1984, 6, 1–7. [Google Scholar]
- McAdams, M.A.; Governale, L.A.; Swartz, L.; Hammad, T.A.; Dal Pan, G.J. Identifying patterns of adverse event reporting for four members of the angiotensin II receptor blockers class of drugs: Revisiting the Weber effect. Pharmacoepidemiol. Drug Saf. 2008, 17, 882–889. [Google Scholar] [CrossRef] [PubMed]
- Neha, R.; Subeesh, V.; Beulah, E.; Gouri, N.; Maheswari, E. Existence of Notoriety Bias in FDA Adverse Event Reporting System Database and Its Impact on Signal Strength. Hosp. Pharm. 2021, 56, 152–158. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Target Adverse Event | Other Adverse Events | Total | ||
|---|---|---|---|---|
| Target drug | N11 | N10 | N1+ | |
| Other drugs | N01 | N00 | N0+ | |
| Total | N+1 | N+0 | N++ | |
| Target Adverse Event | Other Adverse Events | Total | ||
|---|---|---|---|---|
| Women | Target drug | Nwomen11 | Nwomen10 | Nwomen1+ |
| Other drugs | Nwomen01 | Nwomen00 | Nwomen0+ | |
| Men | Target drug | Nmen11 | Nmen10 | Nmen1+ |
| Other drugs | Nmen 01 | Nmen00 | Nmen0+ |
| Class | Drug | Anterior Pituitary Hypofunction | Anterior Pituitary Hyperfunction | Posterior Pituitary Disorder | Pituitary Neoplasm | ||||
|---|---|---|---|---|---|---|---|---|---|
| N11 | IC (95%CrI) | N11 | IC (95%CrI) | N11 | IC (95%CrI) | N11 | IC (95%CrI) | ||
| anti-CTLA-4 antibody | ipilimumab | 213 | 5.53 (5.30 *–5.69) | 0 | NA | 5 | −1.24 (−2.80–−0.26 †) | 1 | 0.62 (−3.17–2.30) |
| anti-PD-1 antibody | nivolumab | 400 | 4.96 (4.79 *–5.08) | 1 | −0.94 (−4.72–0.75) | 20 | −0.89 (−1.64–−0.37 †) | 1 | −0.37 (−4.15–1.32) |
| pembrolizumab | 134 | 4.04 (3.76 *–4.25) | 0 | NA | 26 | 0.16 (−0.49–0.63) | 0 | NA | |
| anti-PD-L1 antibody | atezolizumab | 15 | 2.40 (1.53 *–3.00) | 0 | NA | 11 | 0.55 (−0.48–1.24) | 0 | NA |
| avelumab | 0 | NA | 0 | NA | 0 | NA | 0 | NA | |
| durvalumab | 3 | 0.69 (−1.38–1.90) | 0 | NA | 0 | NA | 0 | NA | |
| Class | Drug | Women | Men | Women Versus Men | ||
|---|---|---|---|---|---|---|
| Nwomen11 | IC (95%CrI) | Nmen11 | IC (95%CrI) | ICΔ (95%CrI) | ||
| anti-CTLA-4 antibody | ipilimumab | 73 | 5.77 (5.39 *–6.05) | 137 | 5.01 (4.73 *–5.21) | 1.24 (0.85 **–1.52) |
| anti-PD−1 antibody | nivolumab | 105 | 5.35 (5.03 *–5.59) | 292 | 4.50 (4.31 *–4.64) | 1.09 (0.77 **–1.33) |
| pembrolizumab | 28 | 4.14 (3.51 *–4.58) | 104 | 3.65 (3.32 *–3.88) | 0.89 (0.26 **–1.34) | |
| anti-PD-L1 antibody | atezolizumab | 5 | 2.60 (1.04 *–3.58) | 9 | 1.86 (0.72 *–2.62) | 1.30 (−0.26–2.28) |
| Class | Drug | N11 | α (95%CI) | β (95%CI) |
|---|---|---|---|---|
| anti-CTLA-4 antibody | ipilimumab | 131 | 97.3 (86.3–109.4) | 1.54 (1.36–1.73) |
| anti-PD-1 antibody | nivolumab | 164 | 158.5 (141.9–176.6) | 1.50 (1.34–1.67) |
| pembrolizumab | 63 | 201.6 (174.6–231.7) | 1.87 (1.54–2.22) | |
| anti-PD-L1 antibody | atezolizumab | 5 | 115.7 (67.6–194.7) | 2.29 (0.92–4.49) |
| avelumab | 0 | NA | NA | |
| durvalumab | 0 | NA | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asano, H.; Noguchi, Y.; Kimura, M.; Usami, E.; Yoshimura, T. Pituitary-Related Adverse Events and Onset Patterns Caused by Immune Checkpoint Inhibitors: Analysis Using the Japanese Adverse Drug Event Report Database. Medicina 2023, 59, 1963. https://doi.org/10.3390/medicina59111963
Asano H, Noguchi Y, Kimura M, Usami E, Yoshimura T. Pituitary-Related Adverse Events and Onset Patterns Caused by Immune Checkpoint Inhibitors: Analysis Using the Japanese Adverse Drug Event Report Database. Medicina. 2023; 59(11):1963. https://doi.org/10.3390/medicina59111963
Chicago/Turabian StyleAsano, Hiroki, Yoshihiro Noguchi, Michio Kimura, Eiseki Usami, and Tomoaki Yoshimura. 2023. "Pituitary-Related Adverse Events and Onset Patterns Caused by Immune Checkpoint Inhibitors: Analysis Using the Japanese Adverse Drug Event Report Database" Medicina 59, no. 11: 1963. https://doi.org/10.3390/medicina59111963