
Frequency of Impulsive-Compulsive Behavior and Associated Psychological Factors in Parkinson’s Disease: Lack of Control or Too Much of It?
 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Methodology
2.1. Archival Sample
2.2. Preliminary Study’s Sample
2.3. Psychometric Tools
3. Results
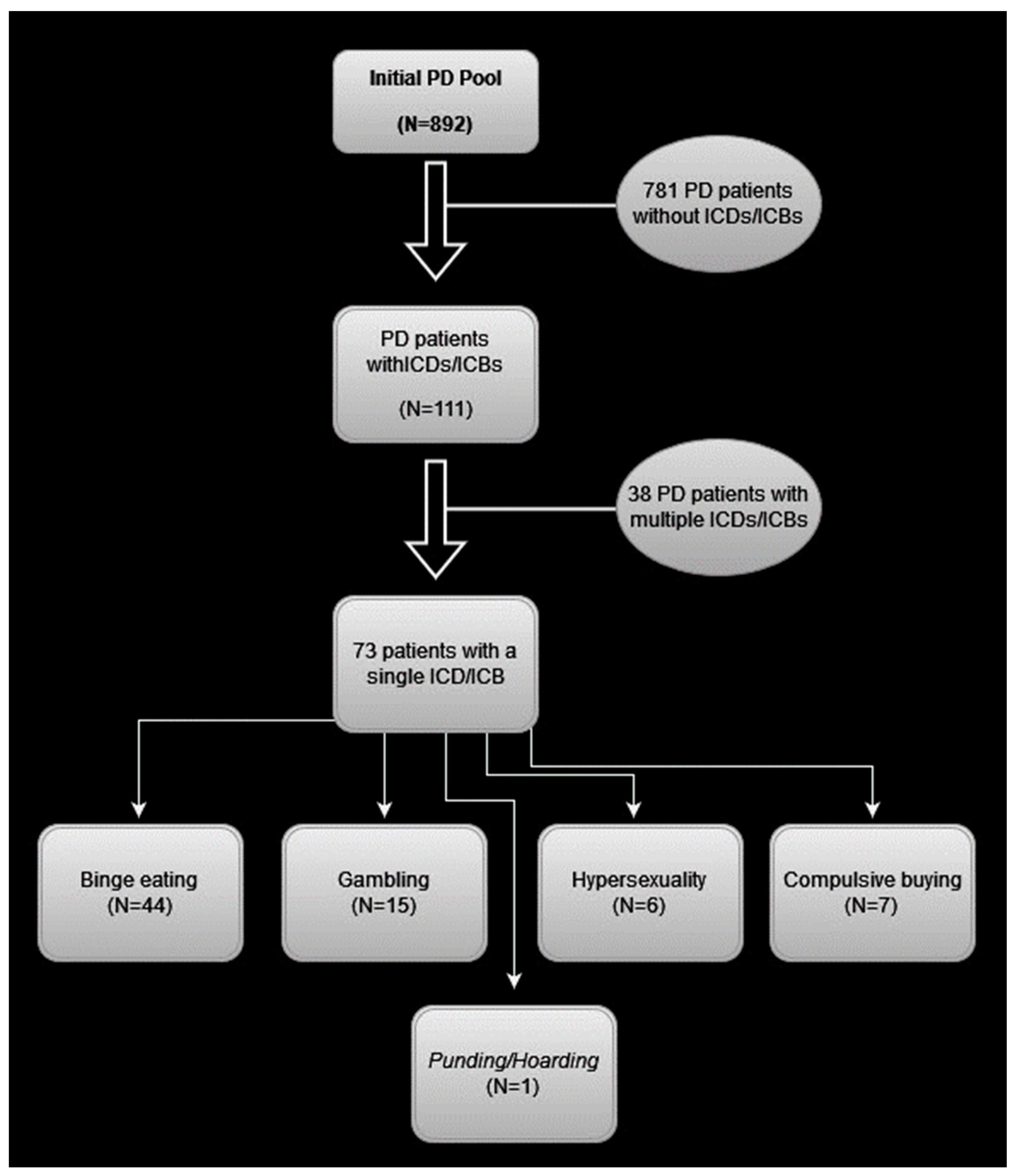
3.1. Frequency of ICDs/ICBs Based on the Archival Study
3.1.1. Frequency of ICDs/ICBs and Patients Identified with a Single ICD/ICB
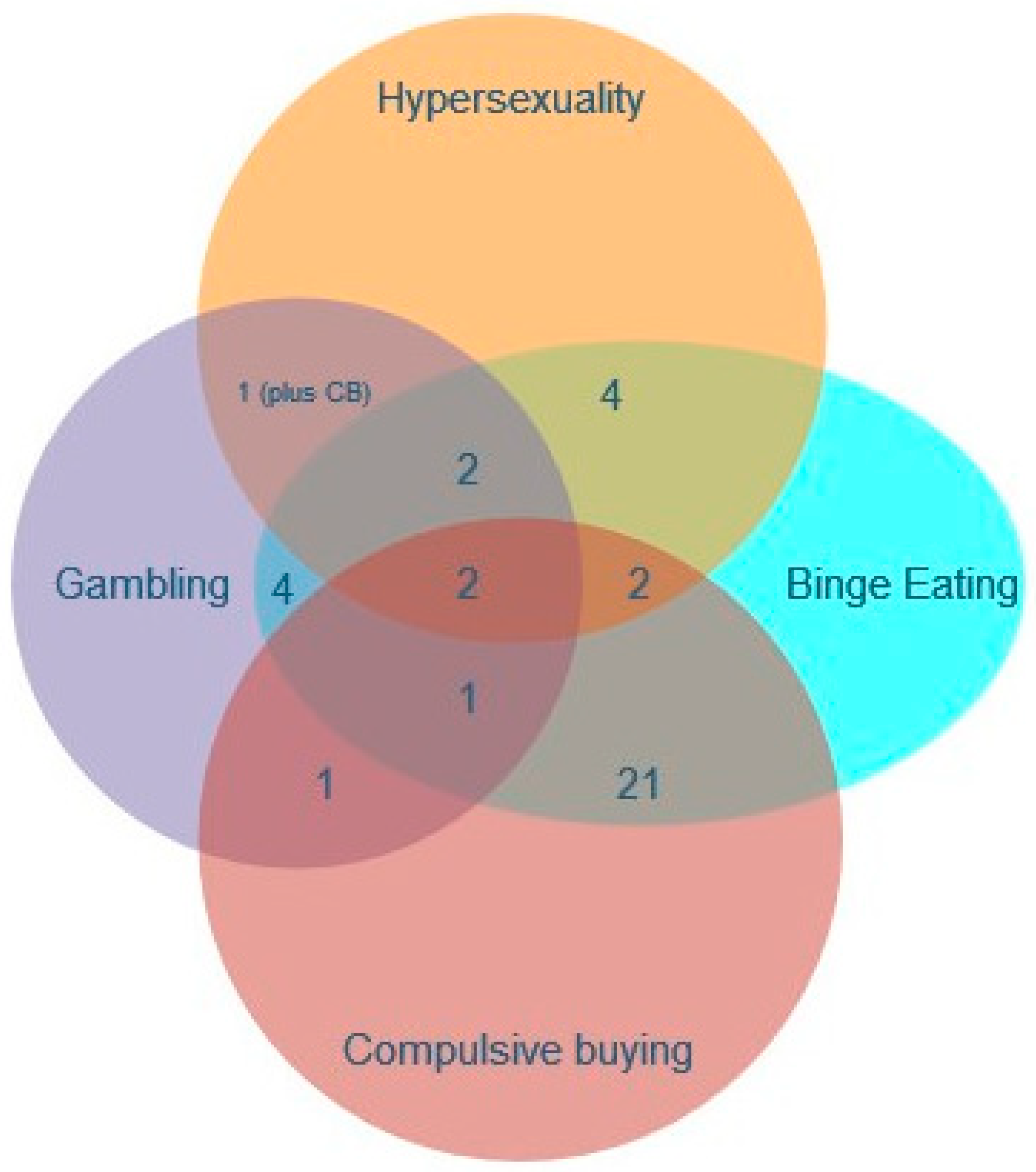
3.1.2. Patients Identified with Multiple ICDs/ICBs
3.1.3. Specifics on the ICBs and Non-Motor Symptoms in General
3.2. Preliminary Results from the 30-Patient Sample
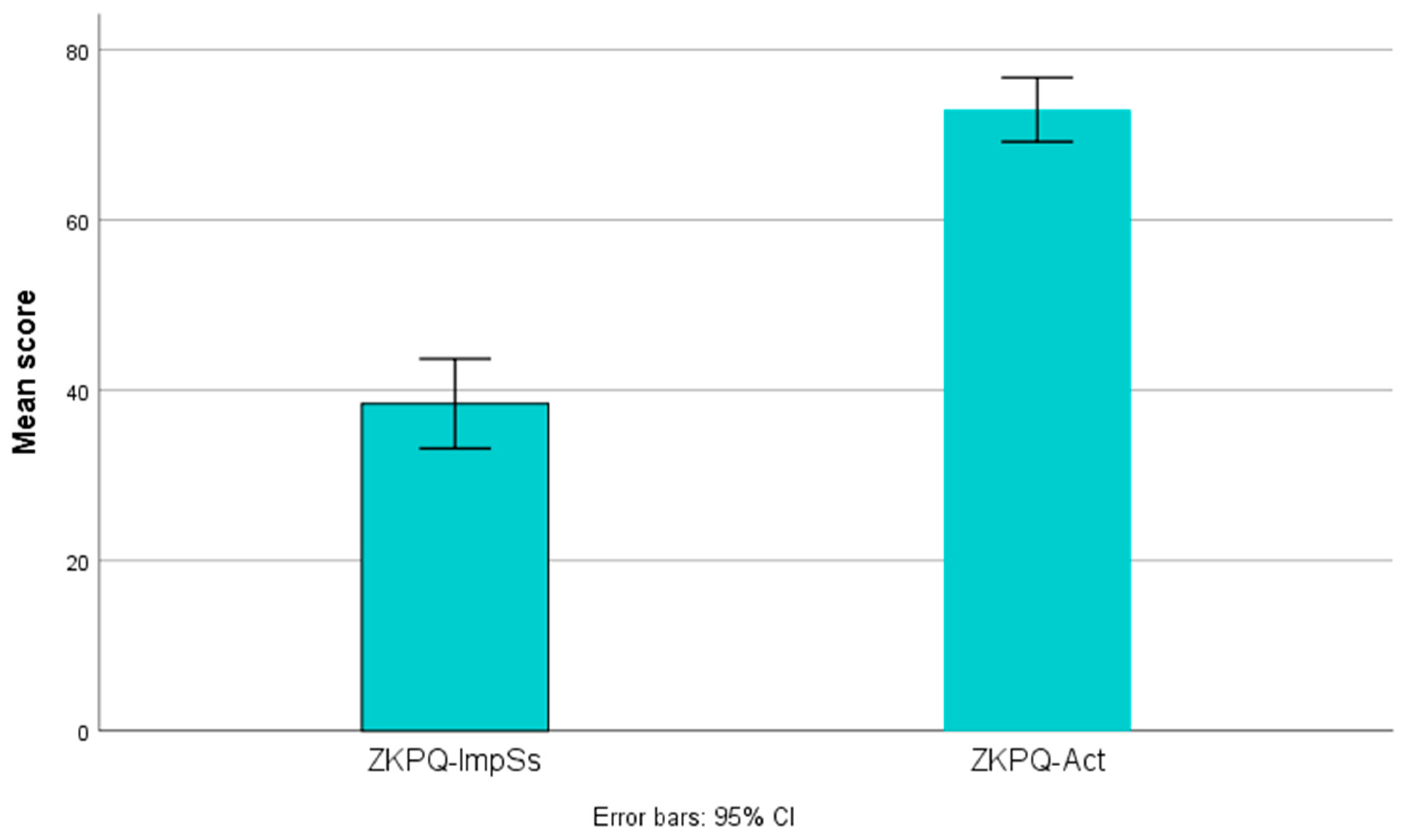
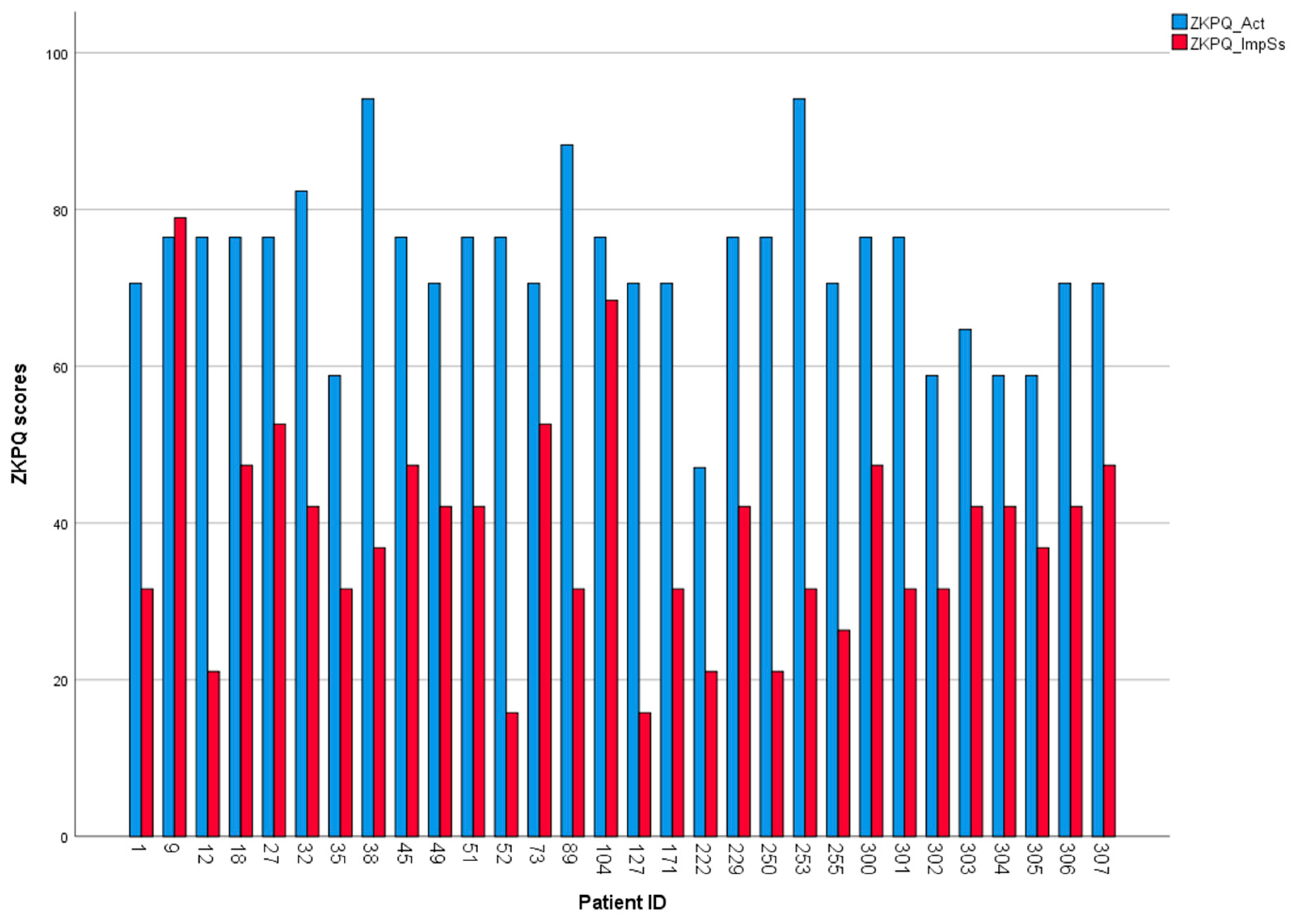
3.2.1. Impulsivity vs. Activity
3.2.2. Associations between Psychological Variables
4. Discussion
4.1. On the Frequency of ICDs/ICBs in PD
4.2. Psychological Factors Associated with ICDs/ICBs in PD
4.3. A Working Hypothesis on Addictive Behaviors of PD Patients
5. Strengths, Limitations, and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weintraub, D.; Sohr, M.; Potenza, M.N.; Siderowf, A.D.; Stacy, M.; Voon, V.; Whetteckey, J.; Wunderlich, G.R.; Lang, A.E. Amantadine Use Associated with Impulse Control Disorders in Parkinson Disease in Cross-Sectional Study. Ann. Neurol. 2010, 68, 963–968. [Google Scholar] [CrossRef] [PubMed]
- Phu, A.; Xu, Z.; Brakoulias, V.; Mahant, N.; Martin, A.J.; de Moore, G.; Starcevic, V.; Krause, M. Effect of Impulse Control Disorders on Disability and Quality of Life in Parkinson’s Disease Patients. J. Clin. Neurosci. 2014, 21, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Ryu, D.-W.; Kim, J.-S.; Yoo, S.-W.; Oh, Y.-S.; Lee, K.-S. The Impact of Impulsivity on Quality of Life in Early Drug-Naïve Parkinson’s Disease Patients. J. Mov. Disord. 2019, 12, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Leroi, I.; Harbishettar, V.; Andrews, M.; McDonald, K.; Byrne, E.J.; Burns, A. Carer Burden in Apathy and Impulse Control Disorders in Parkinson’s Disease. Int. J. Geriatr. Psychiatry 2011, 27, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-Y.; Kim, J.-M.; Kim, J.W.; Cho, J.; Lee, W.Y.; Kim, H.-J.; Jeon, B.S. Association between the Dose of Dopaminergic Medication and the Behavioral Disturbances in Parkinson Disease. Park. Relat. Disord. 2010, 16, 202–207. [Google Scholar] [CrossRef]
- Joutsa, J.; Martikainen, K.; Vahlberg, T.; Voon, V.; Kaasinen, V. Impulse Control Disorders and Depression in Finnish Patients with Parkinson’s Disease. Park. Relat. Disord. 2012, 18, 155–160. [Google Scholar] [CrossRef]
- Ramírez Gómez, C.C.; Serrano Dueñas, M.; Bernal, O.; Araoz, N.; Sáenz Farret, M.; Aldinio, V.; Montilla, V.; Micheli, F. A Multicenter Comparative Study of Impulse Control Disorder in Latin American Patients with Parkinson Disease. Clin. Neuropharmacol. 2017, 40, 51–55. [Google Scholar] [CrossRef]
- Perez-Lloret, S.; Rey, M.V.; Fabre, N.; Ory, F.; Spampinato, U.; Brefel-Courbon, C.; Montastruc, J.-L.; Rascol, O. Prevalence and Pharmacological Factors Associated with Impulse-Control Disorder Symptoms in Patients with Parkinson Disease. Clin. Neuropharmacol. 2012, 35, 261–265. [Google Scholar] [CrossRef]
- Molde, H.; Moussavi, Y.; Kopperud, S.T.; Erga, A.H.; Hansen, A.L.; Pallesen, S. Impulse-Control Disorders in Parkinson’s Disease: A Meta-Analysis and Review of Case-Control Studies. Front. Neurol. 2018, 22, 330. [Google Scholar] [CrossRef]
- Rohde, K.; Riedel, O.; Lueken, U.; Rietzel, S.; Fauser, M.; Ossig, C.; Reichmann, H.; Storch, A. Impulsive-compulsive behaviours in a German Parkinson’s disease outpatient sample. Fortschr. Neurol. Psychiatr. 2013, 81, 503–510. [Google Scholar] [CrossRef]
- Liu, B.; Luo, W.; Mo, Y.; Wei, C.; Tao, R.; Han, M. Meta-Analysis of Related Factors of Impulse Control Disorders in Patients with Parkinson’s Disease. Neurosci. Lett. 2019, 707, 134313. [Google Scholar] [CrossRef]
- Maloney, E.M.; Djamshidian, A.; O’Sullivan, S.S. Phenomenology and Epidemiology of Impulsive-Compulsive Behaviours in Parkinson’s Disease, Atypical Parkinsonian Disorders and Non-Parkinsonian Populations. J. Neurol. Sci. 2017, 374, 47–52. [Google Scholar] [CrossRef]
- Zhang, J.F.; Wang, X.X.; Feng, Y.; Fekete, R.; Jankovic, J.; Wu, Y.C. Impulse control disorders in Parkinson’s disease: Epidemiology, pathogenesis and therapeutic strategies. Front. Psychiatry 2021, 12, 635494. [Google Scholar] [CrossRef] [PubMed]
- Weintraub, D.; Claassen, D.O. Impulse control and related disorders in Parkinson’s disease. Int. Rev. Neurobiol. 2017, 133, 679–717. [Google Scholar]
- MacDonald, H.J.; Stinear, C.M.; Ren, A.; Coxon, J.P.; Kao, J.; Macdonald, L.; Snow, B.; Cramer, S.C.; Byblow, W.D. Dopamine Gene Profiling to Predict Impulse Control and Effects of Dopamine Agonist Ropinirole. J. Cogn. Neurosci. 2016, 28, 909–919. [Google Scholar] [CrossRef] [PubMed]
- Antonini, A.; Siri, C.; Santangelo, G.; Cilia, R.; Poletti, M.; Canesi, M.; Caporali, A.; Mancini, F.; Pezzoli, G.; Ceravolo, R.; et al. Impulsivity and Compulsivity in Drug-Naïve Patients with Parkinson’s Disease. Mov. Disord. 2011, 26, 464–468. [Google Scholar] [CrossRef]
- Voon, V.; Fox, S.H. Medication-Related Impulse Control and Repetitive Behaviors in Parkinson Disease. Arch. Neurol. 2007, 64, 1089. [Google Scholar] [CrossRef] [PubMed]
- Brewer, J.A.; Potenza, M.N. The Neurobiology and Genetics of Impulse Control Disorders: Relationships to Drug Addictions. Biochem. Pharmacol. 2008, 75, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Evans, A.H.; Pavese, N.; Lawrence, A.D.; Tai, Y.F.; Appel, S.; Doder, M.; Brooks, D.J.; Lees, A.J.; Piccini, P. Compulsive Drug Use Linked to Sensitized Ventral Striatal Dopamine Transmission. Ann. Neurol. 2006, 59, 852–858. [Google Scholar] [CrossRef]
- Mallahzadeh, A.; Shafie, M.; Tahvilian, M.; Sadeghi, M.; Moslemian, G.; Barzin, P.; Bemanalizadeh, M.; Mayeli, M.; Aarabi, M.H. White matter tracts alterations underpinning reward and conflict processing. J. Affect. Disord. 2023, 331, 251–258. [Google Scholar] [CrossRef]
- Erga, A.H.; Dalen, I.; Ushakova, A.; Chung, J.; Tzoulis, C.; Tysnes, O.B.; Alves, G.; Pedersen, K.F.; Maple-Grødem, J. Dopaminergic and Opioid Pathways Associated with Impulse Control Disorders in Parkinson’s Disease. Front. Neurol. 2018, 9, 109. [Google Scholar] [CrossRef] [PubMed]
- Kraemmer, J.; Smith, K.; Weintraub, D.; Guillemot, V.; Nalls, M.A.; Cormier-Dequaire, F.; Moszer, I.; Brice, A.; Singleton, A.B.; Corvol, J.-C. Clinical-Genetic Model Predicts Incident Impulse Control Disorders in Parkinson’s Disease. J. Neurol. Neurosurg. Psychiatry 2016, 87, 1106–1111. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-Y.; Jeon, B.S.; Kim, H.-J.; Park, S.-S. Genetic Variant of HTR2A Associates with Risk of Impulse Control and Repetitive Behaviors in Parkinson’s Disease. Park. Relat. Disord. 2012, 18, 76–78. [Google Scholar] [CrossRef] [PubMed]
- Vallelunga, A.; Flaibani, R.; Formento-Dojot, P.; Biundo, R.; Facchini, S.; Antonini, A. Role of Genetic Polymorphisms of the Dopaminergic System in Parkinson’s Disease Patients with Impulse Control Disorders. Park. Relat. Disord. 2012, 18, 397–399. [Google Scholar] [CrossRef] [PubMed]
- Isaias, I.U.; Siri, C.; Cilia, R.; De Gaspari, D.; Pezzoli, G.; Antonini, A. The Relationship between Impulsivity and Impulse Control Disorders in Parkinson’s Disease. Mov. Disord. 2008, 23, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Riley, M.; Bakeberg, M.; Byrnes, M.; Jefferson, A.; Ghosh, S.; Stell, R.; Mastaglia, F.L.; Hince, D.; Anderton, R.S. Demographic and Clinical Predictors of Trait Impulsivity in Parkinson’s Disease Patients. Park. Dis. 2018, 2018, 9472120. [Google Scholar] [CrossRef]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef]
- Postuma, R.B.; Poewe, W.; Litvan, I.; Lewis, S.; Lang, A.E.; Halliday, G.; Goetz, C.G.; Chan, P.; Slow, E.; Seppi, K.; et al. Validation of the MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 2018, 33, 1601–1608. [Google Scholar] [CrossRef]
- Schreiber, L.; Odlaug, B.L.; Grant, J.E. Impulse control disorders: Updated review of clinical characteristics and pharmacological management. Front. Psychiatry 2011, 2, 1. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bedirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Poptsi, E.; Moraitou, D.; Eleftheriou, M.; Kounti-Zafeiropoulou, F.; Papasozomenou, C.; Agogiatou, C.; Bakoglidou, E.; Batsila, G.; Liapi, D.; Markou, N.; et al. Normative Data for the Montreal Cognitive Assessment in Greek Older Adults with Subjective Cognitive Decline, Mild Cognitive Impairment and Dementia. J. Geriatr. Psychiatry Neurol. 2019, 32, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Kaminska, M.; Mery, V.P.; Lafontaine, A.-L.; Robinson, A.; Benedetti, A.; Gros, P.; Kimoff, R.J. Change in Cognition and Other Non-Motor Symptoms with Obstructive Sleep Apnea Treatment in Parkinson Disease. J. Clin. Sleep. Med. 2018, 14, 819–828. [Google Scholar] [CrossRef]
- Kosmidis, M.H.; Vlahou, C.H.; Panagiotaki, P.; Kiosseoglou, G. The Verbal Fluency Task in the Greek Population: Normative Data, and Clustering and Switching Strategies. J. Int. Neuropsychol. Soc. 2004, 10, 164–172. [Google Scholar] [CrossRef]
- Hyphantis, T.; Antoniou, K.; Floros, D.G.; Valma, V.; Pappas, A.I.; Douzenis, A.; Assimakopoulos, K.; Iconomou, G.; Kafetzopoulos, E.; Garyfallos, G.; et al. Assessing Personality Traits by Questionnaire: Psychometric Properties of the Greek Version of the Zuckerman-Kuhlman Personality Questionnaire and Correlations with Psychopathology and Hostility. Hippokratia 2013, 17, 342. [Google Scholar] [PubMed]
- Zuckerman, M. Zuckerman-Kuhlman Personality Questionnaire (ZKPQ). An alternative five-factorial model. In Big Five Assessment; Hogrefe & Huber: Boston, MA, USA, 2002; pp. 377–396. [Google Scholar]
- Sáez-Francàs, N.; Martí Andrés, G.; Ramírez, N.; de Fàbregues, O.; Álvarez-Sabín, J.; Casas, M.; Hernández-Vara, J. Clinical and Psychopathological Factors Associated with Impulse Control Disorders in Parkinson’s Disease. Neurología 2016, 31, 231–238. [Google Scholar] [CrossRef]
- Donias, S.; Karastergiou, A.; Manos, N. Standardization of the Symptom Checklist-90-R Rating Scale in a Greek Population. Psychiatriki 1991, 2, 42–48. [Google Scholar]
- Derogatis, L.R.; Lipman, R.S.; Covi, L. SCL-90: An Outpatient Psychiatric Rating Scale—Preliminary Report. Psychopharmacol. Bull. 1973, 9, 13–28. [Google Scholar]
- Derogatis, L.R.; Rickels, K.; Rock, A.F. The SCL-90 and the MMPI: A Step in the Validation of a New Self-Report Scale. Br. J. Psychiatry 1976, 128, 280–289. [Google Scholar] [CrossRef] [PubMed]
- Derogatis, L.R. Symptom Checklist-90-R: Administration, Scoring, and Procedures Manual; Pearson: San Antonio, TX, USA, 1994. [Google Scholar]
- Hyphantis, T. The Greek Version of the Defense Style Questionnaire: Psychometric Properties in Three Different Samples. Compr. Psychiatry 2010, 51, 618–629. [Google Scholar] [CrossRef] [PubMed]
- Connor, K.M.; Davidson, J.R.T. Development of a New Resilience Scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Tsigkaropoulou, E.; Douzenis, A.; Tsitas, N.; Ferentinos, P.; Liappas, I.; Michopoulos, I. Greek Version of the Connor-Davidson Resilience Scale: Psychometric Properties in a Sample of 546 Subjects. In Vivo 2018, 32, 1629–1634. [Google Scholar] [CrossRef] [PubMed]
- Antonovsky, A. The Structure and Properties of the Sense of Coherence Scale. Soc. Sci. Med. 1993, 36, 725–733. [Google Scholar] [CrossRef] [PubMed]
- Karalis, I.; Langius, A.; Tsirogianni, M.; Faresjö, T.; Nettelbladt, P.; Lionis, C. The Translation-Validation of the Sense of Coherence Scale into Greek and Its Use in Primary Health Care. Arch. Hell. Med. 2004, 21, 195–203. [Google Scholar]
- Paika, V.; Ntountoulaki, E.; Papaioannou, D.; Hyphantis, T. The Greek Version of the Sense of Coherence Scale (SOC-29): Psychometric Properties and Associations with Mental Illness, Suicidal Risk and Quality of Life. J. Psychol. Clin. Psychiatry 2017, 7, 00449. [Google Scholar] [CrossRef]
- Ginieri-Coccossis, M.; Triantafillou, E.; Tomaras, V.; Soldatos, C.R.; Mavreas, V.; Christodoulou, G.N. Psychometric Properties of WHOQOL-BREF in Clinical and Health Greek Populations: Incorporating New Culture-Relevant Items. Psychiatriki 2012, 23, 130–142. [Google Scholar]
- Wu, K.; Politis, M.; Piccini, P. Parkinson Disease and Impulse Control Disorders: A Review of Clinical Features, Pathophysiology and Management. Postgrad. Med. J. 2009, 85, 590–596. [Google Scholar] [CrossRef]
- Ambermoon, P.; Carter, A.; Hall, W.D.; Dissanayaka, N.N.; O’Sullivan, J.D. Impulse control disorders in patients with Parkinson’s disease receiving dopamine replacement therapy: Evidence and implications for the addictions field. Addiction 2011, 106, 283–293. [Google Scholar] [CrossRef]
- Smith, K.M.; Xie, S.X.; Weintraub, D. Incident Impulse Control Disorder Symptoms and Dopamine Transporter Imaging in Parkinson Disease. J. Neurol. Neurosurg. Psychiatry 2016, 87, 864–870. [Google Scholar] [CrossRef]
- Callesen, M.B.; Scheel-Krüger, J.; Kringelbach, M.L.; Møller, A. A Systematic Review of Impulse Control Disorders in Parkinson’s Disease. J. Park. Dis. 2013, 3, 105–138. [Google Scholar] [CrossRef]
- Maraz, A.; Griffiths, M.D.; Demetrovics, Z. The Prevalence of Compulsive Buying: A Meta-Analysis. Addiction 2016, 111, 408–419. [Google Scholar] [CrossRef]
- Koran, L.M.; Faber, R.J.; Aboujaoude, E.; Large, M.D.; Serpe, R.T. Estimated Prevalence of Compulsive Buying Behavior in the United States. Am. J. Psychiatry 2006, 163, 1806–1812. [Google Scholar] [CrossRef] [PubMed]
- Hassay, D.N.; Smith, M.C. Compulsive Buying: An Examination of the Consumption Motive. Psychol. Mark. 1996, 13, 741–752. [Google Scholar] [CrossRef]
- Erskine, H.E.; Whiteford, H.A. Epidemiology of Binge Eating Disorder. Curr. Opin. Psychiatry 2018, 31, 462–470. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Hodgins, D.C.; Stea, J.N.; Grant, J.E. Gambling Disorders. Lancet 2011, 378, 1874–1884. [Google Scholar] [CrossRef]
- Garcia, F.D.; Thibaut, F. Sexual addictions. Am. J. Drug Alcohol. Abus. 2010, 36, 254–260. [Google Scholar] [CrossRef]
- Kuopio, A.M.; Marttila, R.J.; Helenius, H.; Toivonen, M.; Rinne, U.K. The quality of life in Parkinson’s disease. Mov. Disord. 2000, 15, 216–223. [Google Scholar] [CrossRef]
- Leroi, I.; Ahearn, D.J.; Andrews, M.; McDonald, K.R.; Byrne, E.J.; Burns, A. Behavioural Disorders, Disability and Quality of Life in Parkinson’s Disease. Age Ageing 2011, 40, 614–621. [Google Scholar] [CrossRef]
- Pusswald, G.; Fleck, M.; Lehrner, J.; Haubenberger, D.; Weber, G.; Auff, E. The “Sense of Coherence” and the Coping Capacity of Patients with Parkinson Disease. Int. Psychogeriatr. 2012, 24, 1972–1979. [Google Scholar] [CrossRef] [PubMed]
- Hyphantis, T.; Goulia, P.; Carvalho, A.F. Personality Traits, Defense Mechanisms and Hostility Features Associated with Somatic Symptom Severity in Both Health and Disease. J. Psychosom. Res. 2013, 75, 362–369. [Google Scholar] [CrossRef]
- Santangelo, G.; Garramone, F.; Baiano, C.; D’Iorio, A.; Piscopo, F.; Raimo, S.; Vitale, C. Personality and Parkinson’s disease: A meta-analysis. Park. Relat. Disord. 2018, 49, 67–74. [Google Scholar] [CrossRef]
- Luca, A.; Nicoletti, A.; Mostile, G.; Zappia, M. The Parkinsonian Personality: More than Just a “Trait”. Front. Neurol. 2019, 9, 1191. [Google Scholar] [CrossRef] [PubMed]
- Menza, M. The personality associated with Parkinson’s disease. Curr. Psychiatry Rep. 2000, 2, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Todes, C.J.; Lees, A.J. The Pre-Morbid Personality of Patients with Parkinson’s Disease. J. Neurol. Neurosurg. Psychiatry 1985, 48, 97–100. [Google Scholar] [CrossRef]
- Allcock, C.C.; Grace, D.M. Pathological Gamblers Are Neither Impulsive nor Sensation—Seekers. Aust. N. Z. J. Psychiatry 1988, 22, 307–311. [Google Scholar] [CrossRef]
- Robbins, T.W.; Gillan, C.M.; Smith, D.G.; de Wit, S.; Ersche, K.D. Neurocognitive Endophenotypes of Impulsivity and Compulsivity: Towards Dimensional Psychiatry. Trends Cogn. Sci. 2012, 16, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.E.; Kim, S.W. Brain Circuitry of Compulsivity and Impulsivity. CNS Spectr. 2014, 19, 21–27. [Google Scholar] [CrossRef]
- Marin-Lahoz, J.; Pagonabarraga, J.; Martinez-Horta, S.; Fernandez de Bobadilla, R.; Pascual-Sedano, B.; Pérez-Pérez, J.; Gironell, A.; Kulisevsky, J. Parkinson’s disease: Impulsivity does not cause impulse control disorders but boosts their severity. Front. Psychiatry 2018, 9, 465. [Google Scholar] [CrossRef]
- Weatherly, J.N.; Miller, K.B. Exploring the Factors Related to Endorsing Gambling as an Escape. Int. Gambl. Stud. 2013, 13, 52–64. [Google Scholar] [CrossRef]
- Heatherton, T.F.; Baumeister, R.F. Binge Eating as Escape from Self-Awareness. Psychol. Bull. 1991, 110, 86–108. [Google Scholar] [CrossRef]
- Rosenbaum, D.L.; White, K.S. The Role of Anxiety in Binge Eating Behavior: A Critical Examination of Theory and Empirical Literature. Health Psychol. Res. 2013, 1, e19. [Google Scholar] [CrossRef]
- Rosenbaum, D.L.; White, K.S. The relation of anxiety, depression, and stress to binge eating behavior. J. Health Psychol. 2015, 20, 887–898. [Google Scholar] [CrossRef] [PubMed]
- Black, D.W. Compulsive Buying Disorder: A Review of the Evidence. CNS Spectr. 2007, 12, 124–132. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | 69M/42F |
| Marital status | Married: 86; Single: 12; Divorced: 4; Widowed: 9 |
| Parenthood | 81 individuals with children |
| Age of onset—Mean (SD) | 56.23 (8.70) |
| Age at manifestation of ICDs—Mean (SD) | 62.29 (7.17) |
| Psychiatric manifestations | 29 patients diagnosed with depression 39 patients with psychotic manifestations |
| Sleep disturbances | 65 patients with RBD/parasomnias |
| Family neurological history | n = 26 |
| Comorbidities with systemic diseases | Thyroid (n = 26); Heart disease (n = 19); Diabetes (n = 8) |
| Psychometric Tool | Min | Max | Mean | SD |
|---|---|---|---|---|
| ZKPQ-ImpSs | 15.79 | 78.95 | 38.42 | 14.11 |
| ZKPQ-NAnx | 5.26 | 89.47 | 48.07 | 27.32 |
| ZKPQ-AggHost | 5.88 | 70.59 | 30.59 | 18.76 |
| ZKPQ-Act | 47.06 | 94.12 | 72.94 | 10.08 |
| ZKPQ-Sy | 5.88 | 76.47 | 44.12 | 16.76 |
| DSQ-As | 2.61 | 7.84 | 5.79 | 1.41 |
| DSQ-MAs | 2.33 | 5.45 | 3.64 | 0.90 |
| DSQ-SSs | 2.61 | 6.31 | 4.38 | 1.05 |
| DSQ-IDs | 1.38 | 5.41 | 3.57 | 1.13 |
| SCL-GSI | 0.22 | 1.88 | 0.89 | 0.48 |
| CD-RISK | 53.00 | 96.00 | 76.25 | 13.39 |
| SOC | 104.00 | 177.00 | 143.13 | 20.30 |
| MoCA | 19.00 | 29.00 | 24.71 | 2.54 |
| COWF-S | 25.00 | 63.00 | 44.59 | 10.56 |
| COWF-Ph | 16.00 | 42.00 | 29.82 | 8.45 |
| WHO-QOL—Physical | 25.00 | 85.71 | 56.5124 | 18.09 |
| WHO-QOL—Psychological | 41.67 | 95.83 | 64.22 | 15.80 |
| WHO-QOL—Social | 33.00 | 83.33 | 57.8229 | 14.31 |
| WHO-QOL—Environmental | 50.00 | 90.63 | 70.96 | 11.89 |
| WHO-QOL—SubjQOL | 25.00 | 100.00 | 60.29 | 19.88 |
| WHO-QOL—SubjH | 25.00 | 100.00 | 51.47 | 25.72 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kapsomenakis, A.; Kasselimis, D.; Vaniotis, E.; Bougea, A.; Koros, C.; Simitsi, A.M.; Stefanis, L.; Potagas, C. Frequency of Impulsive-Compulsive Behavior and Associated Psychological Factors in Parkinson’s Disease: Lack of Control or Too Much of It? Medicina 2023, 59, 1942. https://doi.org/10.3390/medicina59111942
Kapsomenakis A, Kasselimis D, Vaniotis E, Bougea A, Koros C, Simitsi AM, Stefanis L, Potagas C. Frequency of Impulsive-Compulsive Behavior and Associated Psychological Factors in Parkinson’s Disease: Lack of Control or Too Much of It? Medicina. 2023; 59(11):1942. https://doi.org/10.3390/medicina59111942
Chicago/Turabian StyleKapsomenakis, Alexandros, Dimitrios Kasselimis, Emily Vaniotis, Anastasia Bougea, Christos Koros, Athina Maria Simitsi, Leonidas Stefanis, and Constantin Potagas. 2023. "Frequency of Impulsive-Compulsive Behavior and Associated Psychological Factors in Parkinson’s Disease: Lack of Control or Too Much of It?" Medicina 59, no. 11: 1942. https://doi.org/10.3390/medicina59111942