
Effectiveness of Intranasal Analgesia in the Emergency Department
 , ,
, ,  ,
,
Abstract
:1. Introduction
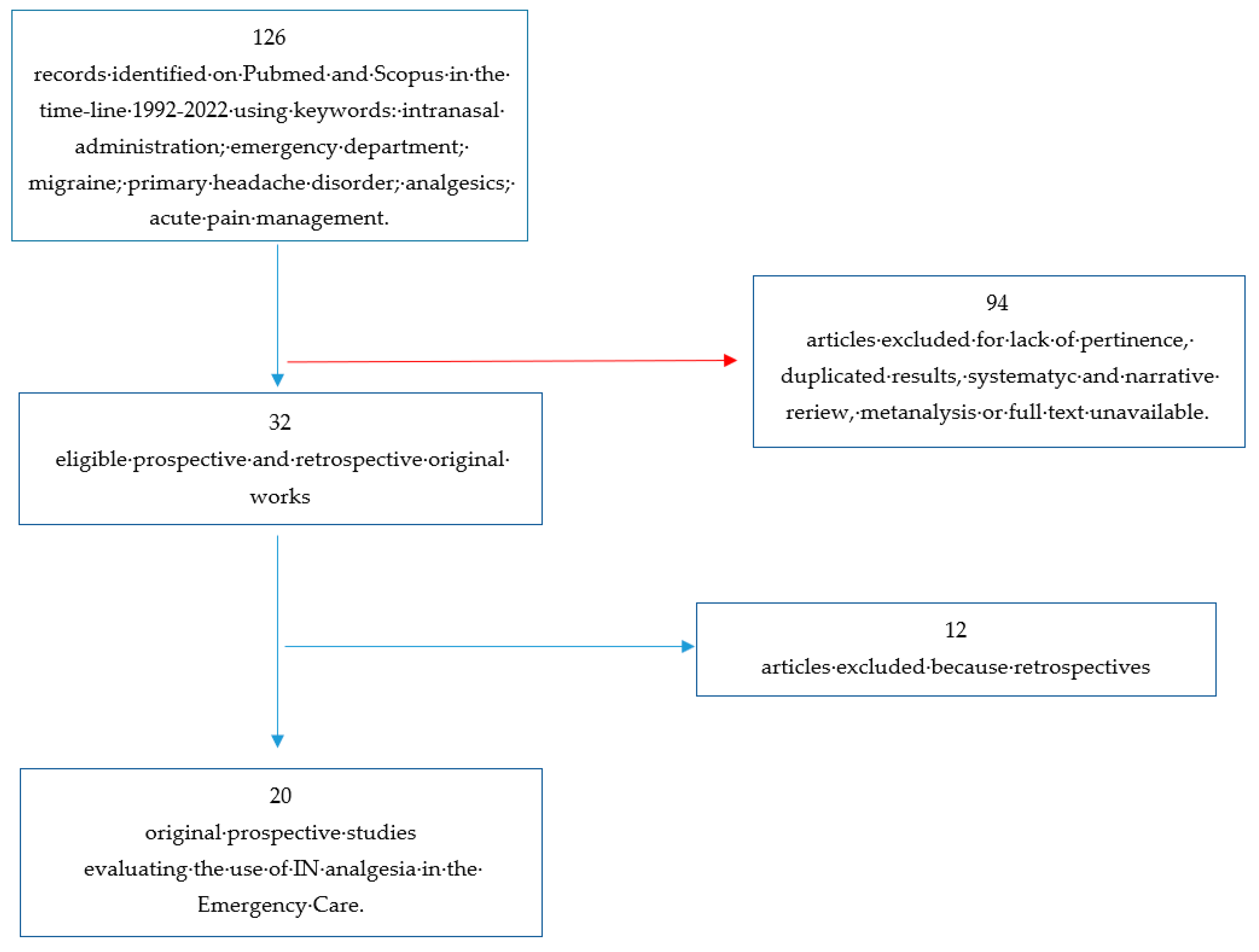
2. Materials and Methods
3. Results
3.1. Headache
3.2. Trauma and Injuries
3.3. Renal Colic
3.4. Other Situations
3.4.1. Prehospital
3.4.2. Breakthrough Cancer Pain
3.4.3. Acute Pain (Back and Abdominal Pain)
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hansen, M.S.; Mathiesen, O.; Trautner, S.; Dahl, J.B. Intranasal fentanyl in the treatment of acute pain--a systematic review. Acta Anaesthesiol. Scand. 2012, 56, 407–419. [Google Scholar] [CrossRef] [PubMed]
- Todd, K.H.; Ducharme, J.; Choiniere, M.; Crandall, C.S.; Fosnocht, D.E.; Homel, P.; Tanabe, P.; PEMI Study Group. Pain in the emergency department: Results of the pain and emergency medicine initiative (PEMI) multicenter study. J. Pain 2007, 8, 460–466. [Google Scholar] [CrossRef] [PubMed]
- Sin, B.; Wiafe, J.; Ciaramella, C.; Valdez, L.; Motov, S.M. The use of intranasal analgesia for acute pain control in the emergency department: A literature review. Am. J. Emerg. Med. 2018, 36, 310–318. [Google Scholar] [CrossRef]
- Pires, A.; Fortuna, A.; Alves, G.; Falcão, A. Intranasal drug delivery: How, why and what for? J. Pharm. Pharm. Sci. 2009, 12, 288–311. [Google Scholar] [CrossRef] [PubMed]
- Cole, J.; Shepherd, M.; Young, P. Intranasal fentanyl in 1-3-year-olds: A prospective study of the effectiveness of intranasal fentanyl as acute analgesia. Emerg. Med. Australas. 2009, 21, 395–400. [Google Scholar] [CrossRef]
- Berger, J.M.; Longhitano, Y.; Zanza, C.; Sener, S.F. Factors affecting the incidence of chronic pain following breast cancer surgery: Preoperative history, anesthetic management, and surgical technique. J. Surg. Oncol. 2020, 122, 1307–1314. [Google Scholar] [CrossRef] [PubMed]
- Dodick, D.; Brandes, J.; Elkind, A.; Mathew, N.; Rodichok, L. Speed of onset, efficacy and tolerability of zolmitriptan nasal spray in the acute treatment of migraine: A randomised, double-blind, placebo-controlled study. CNS Drugs 2005, 19, 125–136. [Google Scholar] [CrossRef]
- Meredith, J.T.; Wait, S.; Brewer, K.L. A prospective double-blind study of nasal sumatriptan versus IV ketorolac in migraine. Am. J. Emerg. Med. 2003, 21, 173–175. [Google Scholar] [CrossRef]
- Avcu, N.; Doğan, N.Ö.; Pekdemir, M.; Yaka, E.; Yılmaz, S.; Alyeşil, C.; Akalın, L.E. Intranasal Lidocaine in Acute Treatment of Migraine: A Randomized Controlled Trial. Ann. Emerg. Med. 2017, 69, 743–751. [Google Scholar] [CrossRef]
- Benish, T.; Villalobos, D.; Love, S.; Casmaer, M.; Hunter, C.J.; Summers, S.M.; April, M.D. The THINK (Treatment of Headache with Intranasal Ketamine) Trial: A Randomized Controlled Trial Comparing Intranasal Ketamine with Intravenous Metoclopramide. J. Emerg. Med. 2019, 56, 248–257.e1. [Google Scholar] [CrossRef]
- Sarvari, H.R.; Baigrezaii, H.; Nazarianpirdosti, M.; Meysami, A.; Safari-Faramani, R. Comparison of the efficacy of intranasal ketamine versus intravenous ketorolac on acute non-traumatic headaches: A randomized double-blind clinical trial. Head Face Med. 2022, 18, 1. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, R.; Pant, S.; Shrestha, A.; Batajoo, K.H.; Thapa, R.; Vaidya, S. Intranasal ketamine for the treatment of patients with acute pain in the emergency department. World J. Emerg. Med. 2016, 7, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Shimonovich, S.; Gigi, R.; Shapira, A.; Sarig-Meth, T.; Nadav, D.; Rozenek, M.; West, D.; Halpern, P. Intranasal ketamine for acute traumatic pain in the Emergency Department: A prospective, randomized clinical trial of efficacy and safety. BMC Emerg. Med. 2016, 16, 43. [Google Scholar] [CrossRef]
- Blancher, M.; Maignan, M.; Clapé, C.; Quesada, J.-L.; Collomb-Muret, R.; Albasini, F.; Ageron, F.-X.; Fey, S.; Wuyts, A.; Banihachemi, J.-J.; et al. Intranasal sufentanil versus intravenous morphine for acute severe trauma pain: A double-blind randomized non-inferiority study. PLoS Med. 2019, 16, e1002849. [Google Scholar] [CrossRef] [PubMed]
- Chew, K.S.; Shaharudin, A.H. An open-label randomized controlled trial on the efficacy of adding intranasal fentanyl to intravenous tramadol in patients with moderate to severe pain following acute musculoskeletal injuries. Singap. Med. J. 2017, 58, 601–605. [Google Scholar] [CrossRef] [PubMed]
- Lemoel, F.; Contenti, J.; Cibiera, C.; Rapp, J.; Occelli, C.; Levraut, J. Intranasal sufentanil given in the emergency department triage zone for severe acute traumatic pain: A randomized double-blind controlled trial. Intern. Emerg. Med. 2019, 14, 571–579. [Google Scholar] [CrossRef]
- Tongbua, S.; Sri-On, J.; Thong-On, K.; Paksophis, T. Non-inferiority of intranasal ketamine compared to intravenous morphine for musculoskeletal pain relief among older adults in an emergency department: A randomised controlled trial. Age Ageing 2022, 51, afac073. [Google Scholar] [CrossRef]
- Silberstein, S.; Winner, P.K.; McAllister, P.J.; Tepper, S.J.; Halker, R.; Mahmoud, R.A.; Siffert, J. Early Onset of Efficacy and Consistency of Response Across Multiple Migraine Attacks from the Randomized COMPASS Study: AVP-825 Breath Powered® Exhalation Delivery System (Sumatriptan Nasal Powder) vs Oral Sumatriptan. Headache J. Head Face Pain 2017, 57, 862–876. [Google Scholar] [CrossRef]
- Pouraghaei, M.; Moharamzadeh, P.; Paknezhad, S.P.; Rajabpour, Z.V.; Soleimanpour, H. Intranasal ketamine versus intravenous morphine for pain management in patients with renal colic: A double-blind, randomized, controlled trial. World J. Urol. 2021, 39, 1263–1267. [Google Scholar] [CrossRef]
- Jalili, M.; Shirani, F.; Entezari, P.; Hedayatshodeh, M.; Baigi, V.; Mirfazaelian, H. Desmopressin/indomethacin combination efficacy and safety in renal colic pain management: A randomized placebo controlled trial. Am. J. Emerg. Med. 2019, 37, 1009–1012. [Google Scholar] [CrossRef]
- Mozafari, J.; Maleki Verki, M.; Motamed, H.; Sabouhi, A.; Tirandaz, F. Comparing intranasal ketamine with intravenous fentanyl in reducing pain in patients with renal colic: A double-blind randomized clinical trial. Am. J. Emerg. Med. 2020, 38, 549–553. [Google Scholar] [CrossRef] [PubMed]
- Nazemian, N.; Torabi, M.; Mirzaee, M. Atomized intranasal vs intravenous fentanyl in severe renal colic pain management: A randomized single-blinded clinical trial. Am. J. Emerg. Med. 2020, 38, 1635–1640. [Google Scholar] [CrossRef] [PubMed]
- Rickard, C.; O’Meara, P.; McGrail, M.; Garner, D.; McLean, A.; Le Lievre, P. A randomized controlled trial of intranasal fentanyl vs intravenous morphine for analgesia in the prehospital setting. Am. J. Emerg. Med. 2007, 25, 911–917. [Google Scholar] [CrossRef]
- Andolfatto, G.; Innes, K.; Dick, W.; Jenneson, S.; Willman, E.; Stenstrom, R.; Zed, P.J.; Benoit, G. Prehospital Analgesia with Intranasal Ketamine (PAIN-K): A Randomized Double-Blind Trial in Adults. Ann. Emerg. Med. 2019, 74, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Banala, S.R.; Khattab, O.K.; Page, V.D.; Warneke, C.L.; Todd, K.H.; Yeung, S.-C.J. Intranasal fentanyl spray versus intravenous opioids for the treatment of severe pain in patients with cancer in the emergency department setting: A randomized controlled trial. PLoS ONE 2020, 15, e0235461. [Google Scholar] [CrossRef] [PubMed]
- Sin, B.; Jeffrey, I.; Halpern, Z.; Adebayo, A.; Wing, T.; Lee, A.S.; Ruiz, J.; Persaud, K.; Davenport, L.; de Souza, S.; et al. Intranasal Sufentanil Versus Intravenous Morphine for Acute Pain in the Emergency Department: A Randomized Pilot Trial. J. Emerg. Med. 2019, 56, 301–307. [Google Scholar] [CrossRef]
- Longhitano, Y.; Bottinelli, M.; Pappalardo, F.; Maj, G.; Audo, A.; Srejic, U.; Rasulo, F.A.; Zanza, C. Electrocardiogram alterations in non-traumatic brain injury: A systematic review. J. Clin. Monit. Comput. 2023. [Google Scholar] [CrossRef]
- Golzari, S.E.; Soleimanpour, H.; Rahmani, F.; Zamani Mehr, N.; Safari, S.; Heshmat, Y.; Ebrahimi Bakhtavar, H. Therapeutic approaches for renal colic in the emergency department: A review article. Anesthesiol. Pain Med. 2014, 4, e16222. [Google Scholar] [CrossRef]
- Farnia, M.R.; Jalali, A.; Vahidi, E.; Momeni, M.; Seyedhosseini, J.; Saeedi, M. Comparison of intranasal ketamine versus IV morphine in reducing pain in patients with renal colic. Am. J. Emerg. Med. 2017, 35, 434–437. [Google Scholar] [CrossRef]
- Abu-Snieneh, H.M.; Alsharari, A.F.; Abuadas, F.H.; Alqahtani, M.E. Effectiveness of pain management among trauma patients in the emergency department, a systematic review. Int. Emerg. Nurs. 2022, 62, 101158. [Google Scholar] [CrossRef]
- Nardi-Hiebl, S.; Ndieyira, J.W.; Al Enzi, Y.; Al Akkad, W.; Koch, T.; Geldner, G.; Reyher, C.; Eberhart, L.H.J. Pharmacokinetic Characterisation and Comparison of Bioavailability of Intranasal Fentanyl, Transmucosal, and Intravenous Administration through a Three-Way Crossover Study in 24 Healthy Volunteers. Pain Res. Manag. 2021, 2021, 2887773. [Google Scholar] [CrossRef] [PubMed]
- Nave, R.; Schmitt, H.; Popper, L. Faster absorption and higher systemic bioavailability of intranasal fentanyl spray compared to oral transmucosal fentanyl citrate in healthy subjects. Drug Deliv. 2013, 20, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, A.R.; Bourn, S.S.; Crowe, R.P.; Bronsky, E.S.; Scheppke, K.A.; Antevy, P.; Myers, J.B. Out-of-Hospital Ketamine: Indications for Use, Patient Outcomes, and Associated Mortality. Ann. Emerg. Med. 2021, 78, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Balzer, N.; McLeod, S.L.; Walsh, C.; Grewal, K. Low-dose Ketamine for Acute Pain Control in the Emergency Department: A Systematic Review and Meta-analysis. Acad. Emerg. Med. 2021, 28, 444–454. [Google Scholar] [CrossRef]
- Gao, M.; Rejaei, D.; Liu, H. Ketamine use in current clinical practice. Acta. Pharmacol. Sin. 2016, 37, 865–872. [Google Scholar] [CrossRef]
- Zanza, C.; Piccolella, F.; Racca, F.; Romenskaya, T.; Longhitano, Y.; Franceschi, F.; Savioli, G.; Bertozzi, G.; De Simone, S.; Cipolloni, L.; et al. Ketamine in Acute Brain Injury: Current Opinion Following Cerebral Circulation and Electrical Activity. Healthcare 2022, 10, 566. [Google Scholar] [CrossRef]
- Zanza, C.; Romenskaya, T.; Zuliani, M.; Piccolella, F.; Bottinelli, M.; Caputo, G.; Rocca, E.; Maconi, A.; Savioli, G.; Longhitano, Y. Acute Traumatic Pain in the Emergency Department. Diseases 2023, 11, 45. [Google Scholar] [CrossRef]
- Bouida, W.; Bel Haj Ali, K.; Ben Soltane, H.; Msolli, M.A.; Boubaker, H.; Sekma, A.; Beltaief, K.; Grissa, M.H.; Methamem, M.; Boukef, R.; et al. Effect on Opioids Requirement of Early Administration of Intranasal Ketamine for Acute Traumatic Pain. Clin. J. Pain 2020, 36, 458–462. [Google Scholar] [CrossRef]
- Green, S.M.; Roback, M.G.; Kennedy, R.M.; Krauss, B. Clinical practice guideline for emergency department ketamine dissociative sedation: 2011 update. Ann. Emerg. Med. 2011, 57, 449–461. [Google Scholar] [CrossRef]
- Grassin-Delyle, S.; Buenestado, A.; Naline, E.; Faisy, C.; Blouquit-Laye, S.; Couderc, L.-J.; Le Guen, M.; Fischler, M.; Devillier, P. Intranasal drug delivery: An efficient and non-invasive route for systemic administration: Focus on opioids. Pharmacol. Ther. 2012, 134, 366–379. [Google Scholar] [CrossRef]
- Daoust, R.; Paquet, J.; Cournoyer, A.; Piette, É.; Morris, J.; Lessard, J.; Castonguay, V.; Williamson, D.; Chauny, J.-M. Side effects from opioids used for acute pain after emergency department discharge. Am. J. Emerg. Med. 2020, 38, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Zanza, C.; Longhitano, Y.; Lin, E.; Luo, J.; Artico, M.; Savarese, B.; Bonato, V.; Piccioni, A.; Franceschi, F.; Taurone, S.; et al. Intravenous Magnesium—Lidocaine-Ketorolac Cocktail for Postoperative Opioid Resistant Pain: A Case Series of Novel Rescue Therapy. Rev. Recent Clin. Trials. 2021, 16, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Gri, N.; Longhitano, Y.; Zanza, C.; Monticone, V.; Fuschi, D.; Piccioni, A.; Bellou, A.; Esposito, C.; Ceresa, I.F.; Savioli, G. Acute Oncologic Complications: Clinical—Therapeutic Management in Critical Care and Emergency Departments. Curr. Oncol. 2023, 30, 7315–7334. [Google Scholar] [CrossRef] [PubMed]
- Savioli, G.; Ceresa, I.F.; Gri, N.; Bavestrello Piccini, G.; Longhitano, Y.; Zanza, C.; Piccioni, A.; Esposito, C.; Ricevuti, G.; Bressan, M.A. Emergency Department Overcrowding: Understanding the Factors to Find Corresponding Solutions. J. Pers. Med. 2022, 12, 279. [Google Scholar] [CrossRef]
- Zanza, C.; Tornatore, G.; Naturale, C.; Longhitano, Y.; Saviano, A.; Piccioni, A.; Maiese, A.; Ferrara, M.; Volonnino, G.; Bertozzi, G.; et al. Cervical spine injury: Clinical and medico-legal overview. Radiol. Med. 2023, 128, 103–112. [Google Scholar] [CrossRef]


{kind=link}
| First Author | Randomization Process | Deviation from Intended Intervention | Missing Outcome Data | Measurement of the Outcome | Selection of the Reported Results | Overall |
|---|---|---|---|---|---|---|
| Dodick et al. [7] |  | | | | | |
| Meredith et al. [8] |  | | | | |  |
| Avcu et al. [9] | | | | | | |
| Benish et al. [10] | | | | | | |
| Sarvari et al. [11] | | | | | | |
| Shrestha et al. [12] | | | | | | |
| Shimonovic et al. [13] | | | | | | |
| Blancher et al. [14] | | | | | | |
| Chew et al. [15] | | | | | | |
| Leomoel et al. [16] | | | | | | |
| Tongbual et al. [17] | | | | | | |
| Silberstein et al. [18] | | | | | | |
| Pouraghaei et al. [19] | | | | | | |
| Jalili et al. [20] | | | | | | |
| Mozafari et al. [21] | | | | | | |
| Nazemian et al. [22] | | | | | | |
| Rickard et al. [23] | | | | | | |
| Andolfatto et al. [24] | | | | | | |
| Banala et al. [25] | | | | | | |
| Sin et al. [26] | | | | | | |
| Author | Intervention | Population | Objective | Findings | Adverse Events |
|---|---|---|---|---|---|
| Dodick et al. 2005 [7] | IN zolmitriptan for headache | 886 zolmitriptan, 854 placebo | Headache reduction at 15 min, 30 min, 1 h, 2 h | Response rate superior in zolmitriptan (66,2%) vs. placebo (35,0%) p < 0.001 | Adverse events (dysgeusia and nasal irritation overall) more frequent in the Zolmitriptan group |
| Meredith et al. 2003 [8] | IN zolmitriptan vs. IV ketorolac for headache | 16 sumatriptan, 13 ketorolac | Headache reduction at 1 h | Both achieved significant pain reduction; however, ketorolac was superior in reducing VAS | Not reported |
| Avcu et al. 2017 [9] | IN lidocaine for headache | 81 lidocaine, 81 placebo | Headache reduction at 15 and 30 min | No difference in pain reduction | Local irritation in the lidocaine group; no serious adverse reactions |
| Benish et al. 2019 [10] | IN ketamine vs. IV metoclopramide for headache | 27 ketamine, 26 placebo | Headache reduction at 30 min and requirement for rescue at 60 min | No difference in pain reduction | No difference in the occurrence of side effects |
| Sarvari et al. 2022 [11] | IN ketamine vs. IV ketorolac for headache | 70 ketamine, 70 ketorolac | Headache reduction at 30, 60, 120 min | Ketamine had more analgesic effect than intravenous ketorolac in a shorter time | Ketamine group reported increased incidence of dizziness, HR increase, and BP increase |
| Shrestha et al. 2016 [12] | Effectiveness of IN ketamine in pain reduction (various acute injuries) | 39 patients | Pain reduction at 15, 30, 60 min | IN ketamine reduced VAS pain scores to a clinically significant degree in 80% of patients | Most common side effects were dizziness, nausea, and sedation |
| Shimonovic et al. 2016 [13] | IN ketamine vs. IV morphine vs. IM morphine in acute traumatic pain | 34 IN ketamine, 26 IV morphine, 30 IM morphine | Pain at 5 min interval from 0 to 60 min | IN ketamine may provide analgesia clinically equal to IV or IM morphine | Ketamine group reported increased incidence of difficulty in concentrating, dizziness, confusion |
| Blancher et al. 2019 [14] | IN sufentanil vs. IV morphine in acute pain | 77 IN sufentanil, 80 IV morphine | Non-inferiority study | IN sufentanil was non-inferior to IV morphine | Incidence of adverse events was higher in the IN group |
| Chew et al. 2017 [15] | IN fentanil plus IV tramadol vs. IV tramadol in acute pain | 10 IN fent. + IV tramad., 10 IV tramadol | Pain reduction at 10 min | Greater reduction in the mean VAS score among the patients in the fentanyl + tramadol arm | Fentanyl + tramadol group had an increased incidence of sleepiness |
| Lemoel et al. 2019 [16] | IN sufentanil vs. IN placebo in acute pain (all plus IV multimodal analgesia) | 72 IN sufentanil, 72 IN placebo | Proportion of VAS < 3 at 30 min | IN sufentanil determines a 20% absolute increase in proportion of patients reaching pain relief | IN sufentanil group showed an increased incidence of opioid-related adverse events |
| Tongbual et al. 2022 [17] | IN ketamine vs. IV morphine in musculoskeletal pain in ED | 37 IN ketamine, 37 IN morphine | Pain reduction at 30 min | IN ketamine provides analgesic efficacy comparable (non-inferior) to IV morphine | No substantial differences in adverse effects. |
| Silberstein et al. 2017 [18] | Sumatriptan nasal powder (with IN delivery system) vs. oral sumatriptan in migraine | 765 nasal powder, 766 oral sumatriptan | Headache reduction at 30 min | Sumatriptan powder provided greater reduction in migraine pain intensity | IN group showed an increased incidence of local adverse effects (irritation, bad taste) |
| Pouraghaei et al. 2021 [19] | IN ketamine vs. IV morphine in renal colic | 100 IN ketamine, 100 IV morphine | Pain reduction at 15, 30, 60 min | IN ketamine has the same efficacy as IV morphine in renal colic pain control | No remarkable side effects occurred after IN ketamine |
| Jalili et al. 2019 [20] | Indomethacin plus IN desmopressin vs. Indomethacin plus IN placebo in renal colic | 62 IN desmopressin, 62 IN placebo | Pain reduction | Desmopressin, as an adjunct to NSAIDs in the management of renal colic, does not significantly improve pain relief | No severe adverse event (e.g., chest pain, anaphylaxis, and dyspnea) occurred for any of the patients |
| Mozafari et al. 2020 [21] | IN ketamine vs. IV fentanil in renal colic | 65 IN ketamine, 65 IV fentanil | Pain reduction at 5, 15, 30 min | The effect of IN ketamine was less significant than of IV fentanil | No difference in the occurrence of side effects (more common nausea, vomiting, dizziness) |
| Nazemian et al. 2020 [22] | IN fentanil plus IV ketorolac vs. IV fentanil plus IV ketorolac in renal colic | 110 IN fentanil, 110 IV fentanil | Pain reduction at 60 min | The mean pain score was higher in the IN group. Nevertheless, the pain intensity significantly and consecutively reduced in both groups during the study | IV fentanil: nausea and pruritus; IN fentanil: bad taste and pharyngeal irritation |
| Rickard et al. 2007 [23] | IV morphine vs. IN fentanil in prehospital analgesia | 122 IV morphine, 136 IN fentanil | Difference between baseline and destination pain score | No difference in pain reduction | IN fentanyl group showed an increased incidence of opioid-related events |
| Andolfatto et al. 2019 [24] | Effectiveness of IN ketamine in pain reduction in prehospital setting | 60 IN ketamine, 60 IN placebo | Pain reduction at 2 and 30 min | Intranasal ketamine provides clinically significant pain reduction and improved comfort compared with intranasal placebo | Adverse events were more frequent in ketamine group: unreality, dizziness, nausea, fatigue |
| Banala et al. 2020 [25] | IN fentanil vs. IV hydromorphone in cancer pain in ED setting | 42 IN fentanil, 42 IV hydromorphone | Pain reduction at 60 min | Two of three analyses supported non-inferiority of INF versus IVH, while one analysis was inconclusive | Not reported |
| Sin et al. 2019 [26] | IN sufentanil vs. IV morphine in acute pain in ED | 30 IN sufentanil, 30 IV morphine | Efficacy and safety of IN sufentanil in ED | IN resulted in safe analgesia, comparable with IV morphine | There were no significant differences in the incidence of adverse events between the groups |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zanza, C.; Saglietti, F.; Giamello, J.D.; Savioli, G.; Biancone, D.M.; Balzanelli, M.G.; Giordano, B.; Trompeo, A.C.; Longhitano, Y. Effectiveness of Intranasal Analgesia in the Emergency Department. Medicina 2023, 59, 1746. https://doi.org/10.3390/medicina59101746
Zanza C, Saglietti F, Giamello JD, Savioli G, Biancone DM, Balzanelli MG, Giordano B, Trompeo AC, Longhitano Y. Effectiveness of Intranasal Analgesia in the Emergency Department. Medicina. 2023; 59(10):1746. https://doi.org/10.3390/medicina59101746
Chicago/Turabian StyleZanza, Christian, Francesco Saglietti, Jacopo Davide Giamello, Gabriele Savioli, Davide Maria Biancone, Mario Giosuè Balzanelli, Benedetta Giordano, Anna Chiara Trompeo, and Yaroslava Longhitano. 2023. "Effectiveness of Intranasal Analgesia in the Emergency Department" Medicina 59, no. 10: 1746. https://doi.org/10.3390/medicina59101746