
Analysis of Genetic and MRI Changes, Blood Markers, and Risk Factors in a Twin Pair Discordant of Progressive Supranuclear Palsy


 ,
,  , ,
, ,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Questionnaires
2.3. Sample Collection
2.4. Routine Laboratory Testing
2.5. Bead-Based Multiplex Immunoassay
2.6. Genotyping Apolipoprotein E Gene
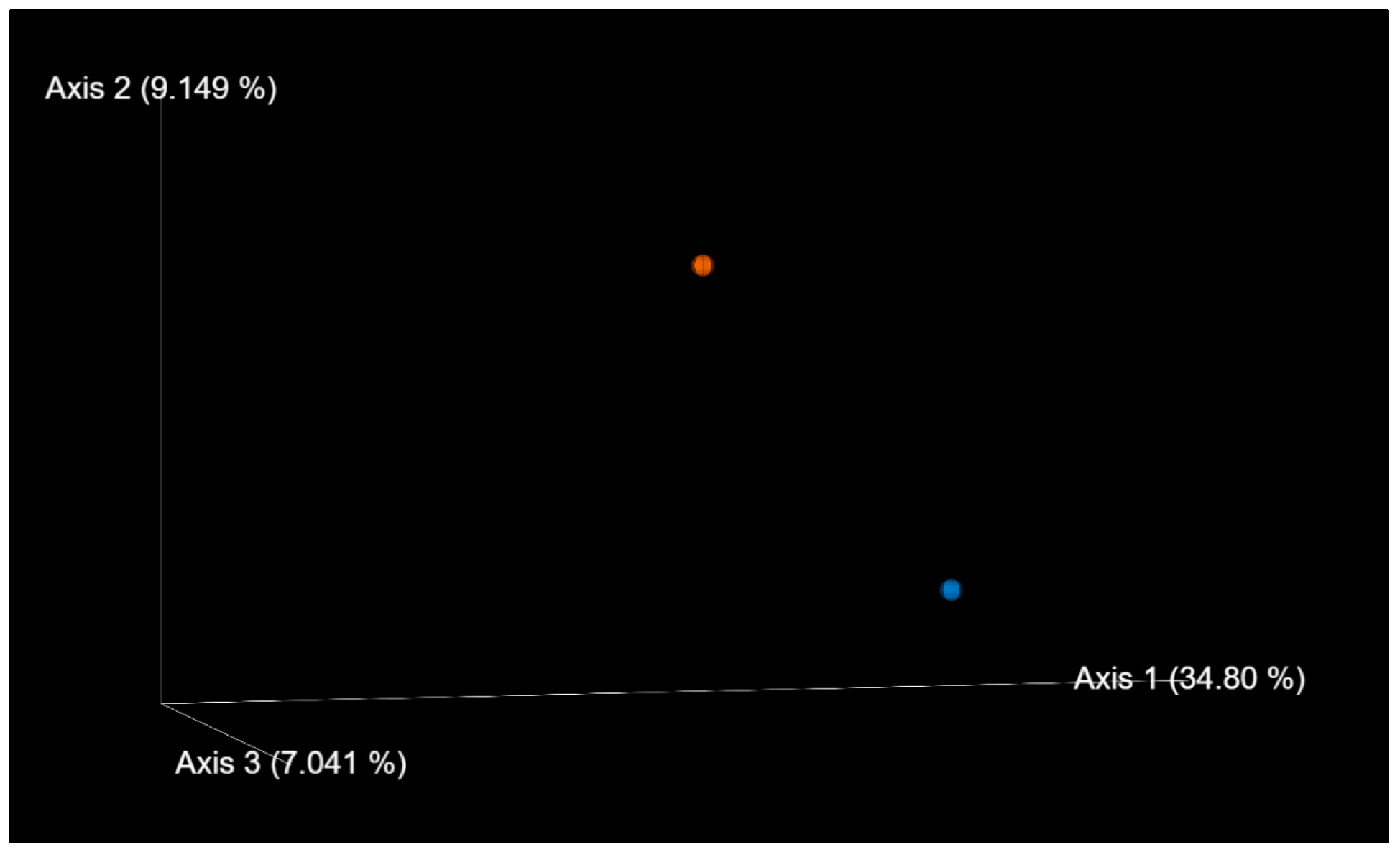
2.7. Stool Sample Collection and Processing, Bioinformatics, and Statistical Analysis
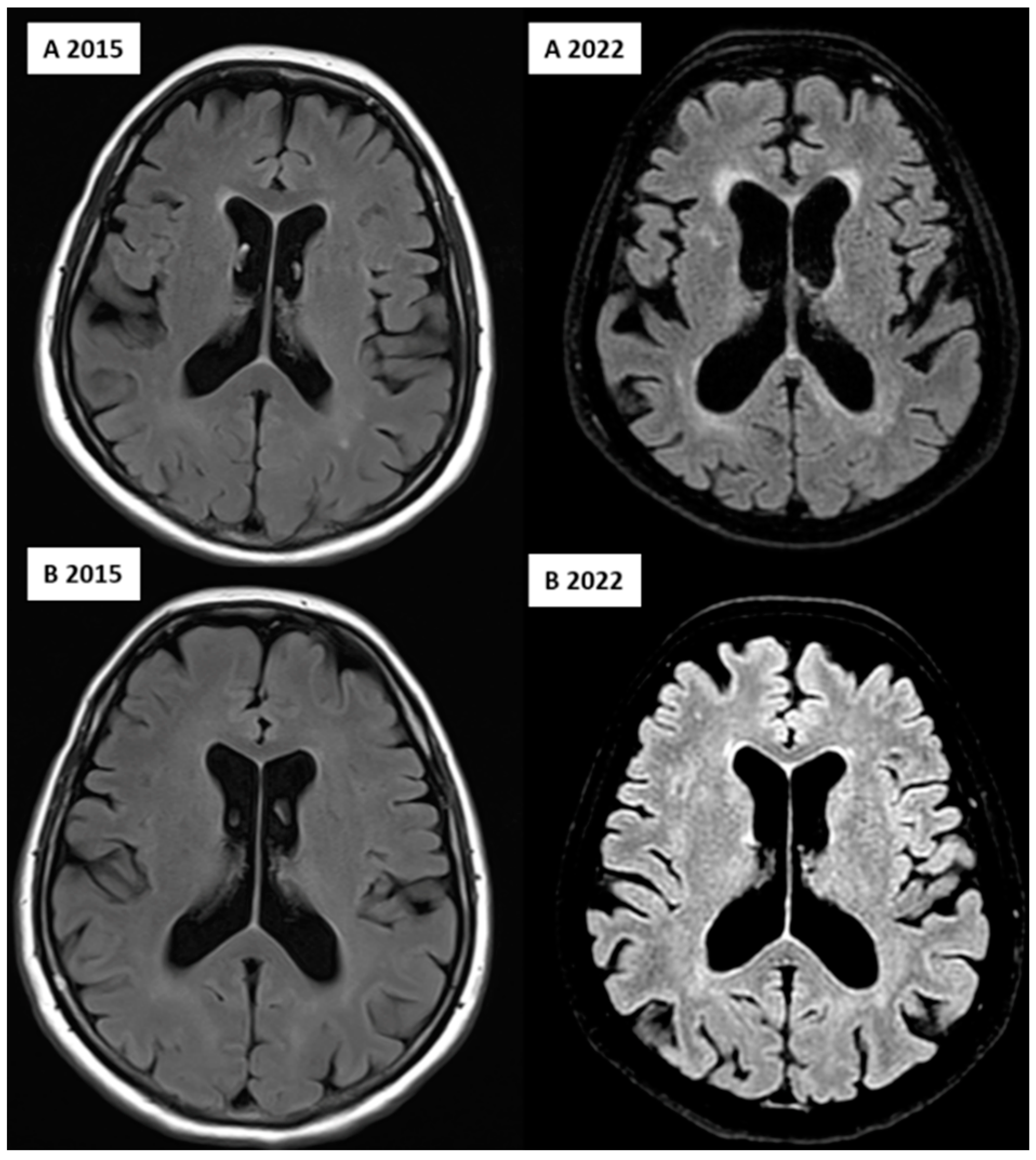
2.8. MRI Acquisition
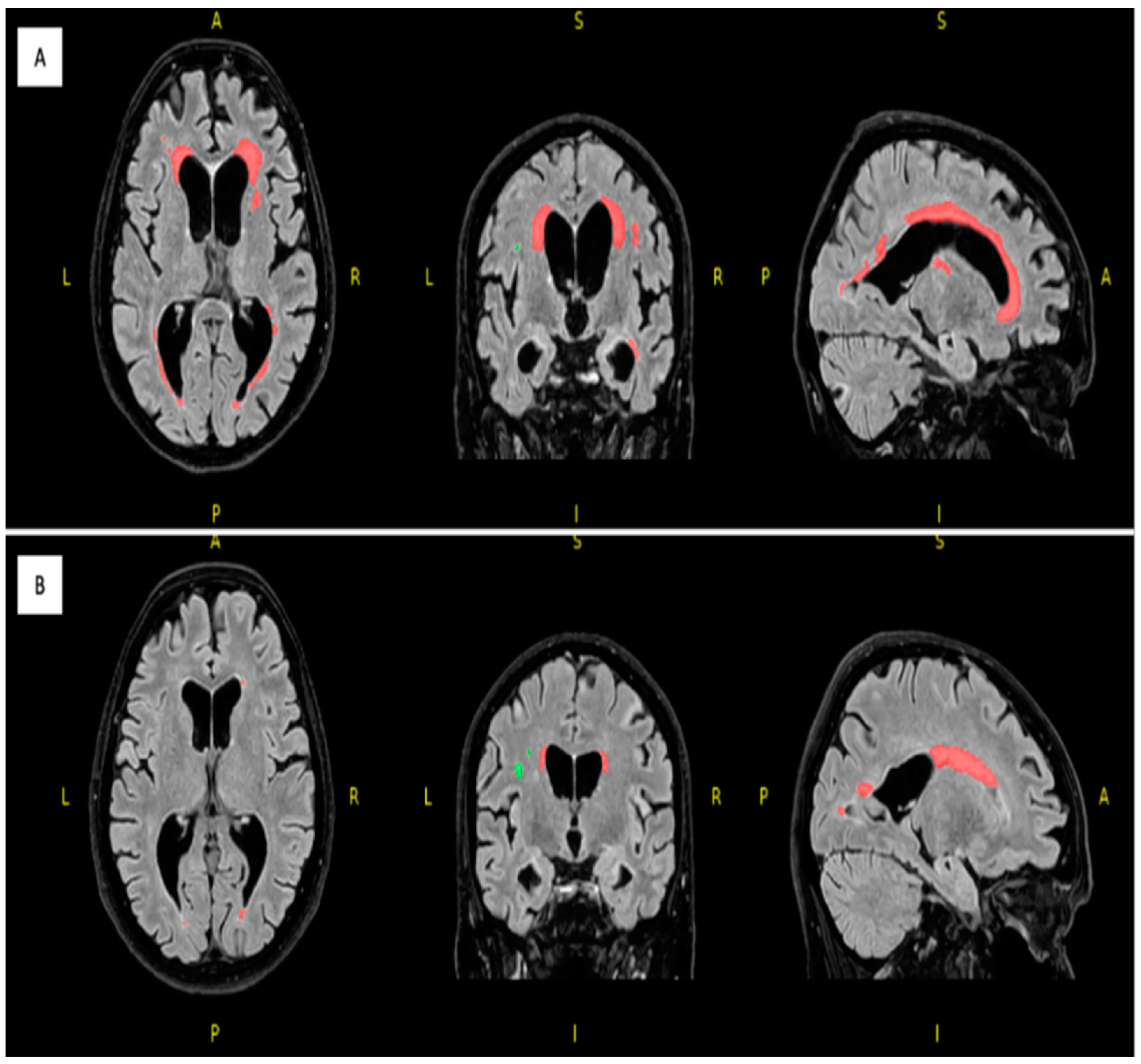
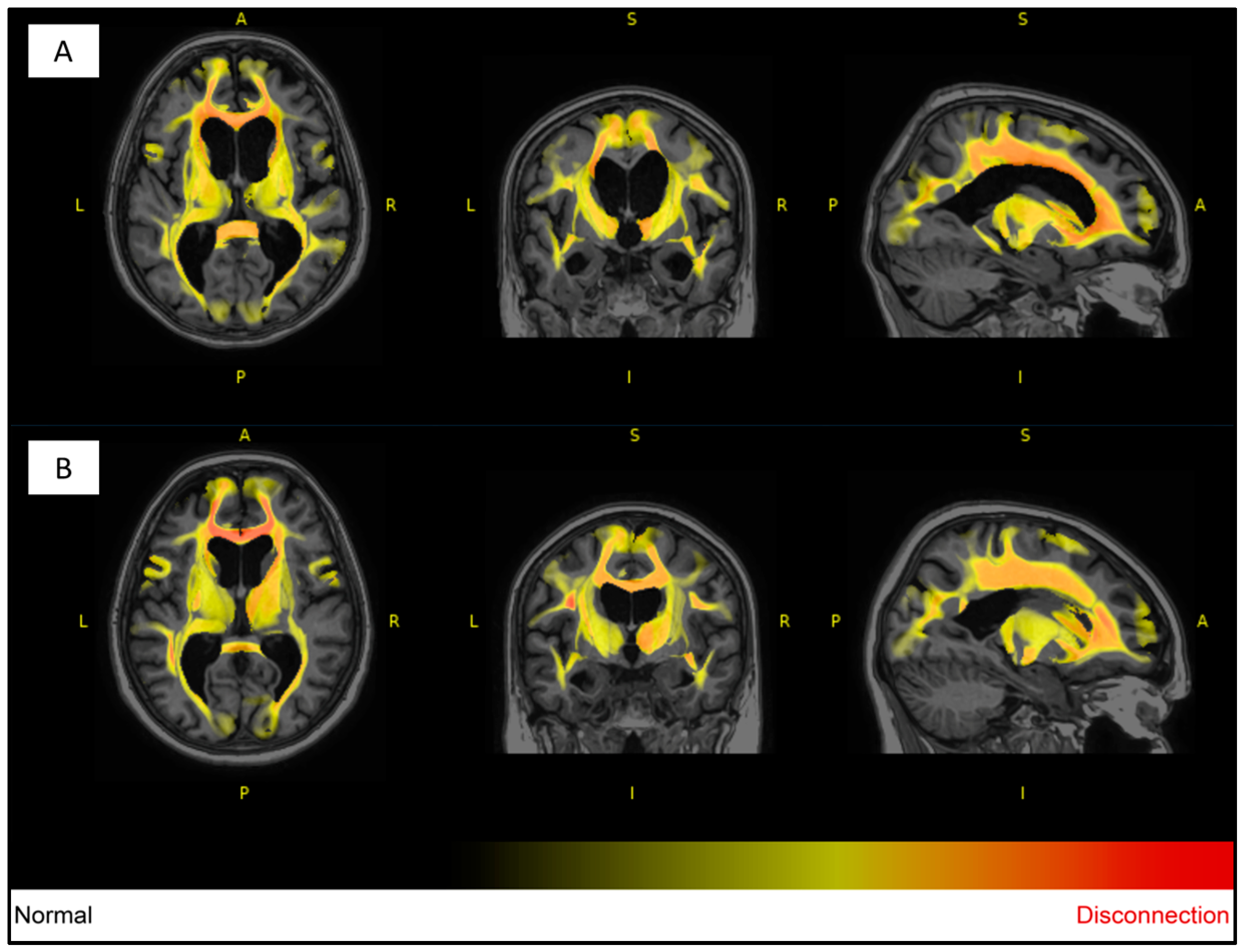
2.9. Image Processing
3. Results
4. Discussion
5. Summary and Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACD-A | Acid citrate dextrose A |
| ACE | Addenbrooke Cognitive Examination |
| APO | Apolipoprotein |
| ApoA1 | Apolipoprotein AI |
| Apo-AII | Apolipoprotein AII |
| ApoB | Apolipoprotein B |
| Apo-CII | Apolipoprotein CII |
| Apo-CIII | Apolipoprotein CIII |
| Apo-D | Apolipoprotein D |
| ApoE | Apolipoprotein E |
| Apo-H | Apolipoprotein H |
| Apo-J | Apolipoprotein J |
| Apo-M | Apolipoprotein M |
| Aβ40 | β-amyloid-40 |
| Aβ42 | β-amyloid-42 |
| BDI | Beck Depression Inventory |
| BIA | Body impedance analysis |
| BMI | Body mass index |
| CBD | Corticobasal degeneration |
| CSF | Cerebrospinal fluid |
| CysC | Cystatin C |
| DBP | Diastolic blood pressure |
| DICOM | Digital Imaging and Communications in Medicine |
| DLB | DeepLesionBrain |
| DNA | Deoxyribonucleic acid |
| EDTA | Ethylenediaminetetraacetic acid |
| FLAIR | Fluid-attenuated inversion recovery |
| FTM | Fecal microbiome transplantation |
| GDS | Geriatric Depression Scale |
| GFAP | Glial fibrillar acidic protein |
| GM | Gray matter |
| HDL-C | High-density lipoprotein cholesterol |
| ICAM1 | Intercellular adhesion molecule 1 |
| IGFBP-4 | Insulin-like growth factor-binding protein-4 |
| LDL-C | Low-density lipoprotein cholesterol |
| Lp(a) | Lipoprotein (a) |
| MAPT | Microtubule-associated protein tau |
| MB | Myoglobin |
| MMP-2 | Matrix metalloproteinase-2 |
| MMP-9 | Matrix metalloproteinase-9 |
| MMSE | Mini-Mental State Examination |
| MNI | Montreal Neurologic Institute |
| MoCA | Montreal Cognitive Assessment (MoCA) |
| MPO | Myeloperoxidase |
| MRI | Magnetic resonance imaging |
| MRP 8/14 | Calprotectin |
| NFL | Neurofilament light chain |
| NGAL | Lipocalin A |
| NGS | Next-generation sequencing |
| NIfTI | Neuroimaging Informatics Technology Initiative |
| NPH | Normal pressure hydrocephalus |
| OPN | Osteopontin |
| PCoA | Principal coordinate analysis |
| PCR | Polymerase chain reaction |
| PSP | Progressive supranuclear palsy |
| RNA | Ribonucleic acid |
| SAA | Serum amyloid A |
| SBP | Systolic blood pressure |
| SCFA | Short-chain fatty acid |
| T1W | T1-weighted |
| T2W | T2-weighted |
| TAU | Tau protein |
| VCAM1 | Vascular cell adhesion molecule-1 |
| WM | White matter |
| WMH | White matter hyperintensity |
| ZDS | Zung Depression Scale |
| αSyn | α-Synuclein |
References
- Golbe, L.I. Progressive Supranuclear Palsy. Semin. Neurol. 2014, 34, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Dickson, D.W.; Kouri, N.; Murray, M.E.; Josephs, K.A. Neuropathology of Frontotemporal Lobar Degeneration-Tau (FTLD-Tau). J. Mol. Neurosci. 2011, 45, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Pastor, P.; Tolosa, E. Progressive supranuclear palsy: Clinical and genetic aspects. Curr. Opin. Neurol. 2002, 15, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Ling, H.; de Silva, R.; Massey, L.A.; Courtney, R.; Hondhamuni, G.; Bajaj, N.; Lowe, J.; Holton, J.L.; Lees, A.; Revesz, T. Characteristics of progressive supranuclear palsy presenting with corticobasal syndrome: A cortical variant. Neuropathol. Appl. Neurobiol. 2014, 40, 149–163. [Google Scholar] [CrossRef]
- Quattron, A.; Nicoletti, G.; Messina, D.; Fera, F.; Condino, F.; Pugliese, P.; Lanza, P.; Barone, P.; Morgante, L.; Zappia, M.; et al. MR imaging index for Differentiation of Progressive Supranuclear Palsy from Parkinson disease and the Parkinson variant of Multiple System Atrophy. Radiology 2008, 246, 214–221. [Google Scholar] [CrossRef]
- Massey, L.A.; Micallef, C.; Paviour, D.C.; O’Sullivan, S.S.; Ling, H.; Williams, D.R.; Kallis, C.; Holton, J.L.; Revesz, T.; Burn, D.J.; et al. Conventional magnetic resonance imaging in confirmed progressive supranuclear palsy and multiple system atrophy. Mov. Disord. 2012, 27, 1754–1762. [Google Scholar] [CrossRef]
- Rojo, A.; Pernaute, R.S.; Fontán, A.; Ruíz, P.G.; Honnorat, J.; Lynch, T.; Chin, S.; Gonzalo, I.; Rábano, A.; Martínez, A.; et al. Clinical genetics of familial progressive supranuclear palsy. Brain 1999, 122, 1233–1245. [Google Scholar] [CrossRef]
- Kelley, K.D.; Checkoway, H.; Hall, D.A.; Reich, S.G.; Cunningham, C.; Litvan, I. Traumatic brain injury and firearm use and risk of progressive supranuclear palsy among veterans. Front. Neurol. 2018, 9, 474. [Google Scholar] [CrossRef]
- Ogaki, K.; Li, Y.; Takanashi, M.; Ishikawa, K.; Kobayashi, T.; Nonaka, T.; Hasegawa, M.; Kishi, M.; Yoshino, H.; Funayama, M.; et al. Analyses of the MAPT, PGRN, and C9orf72 mutations in Japanese patients with FTLD, PSP, and CBS. Park. Relat. Disord. 2013, 19, 15–20. [Google Scholar] [CrossRef]
- Cryan, J.F.; O’Riordan, K.J.; Sandhu, K.; Peterson, V.; Dinan, T.G. The gut microbiome in neurological disorders. Lancet Neurol. 2020, 19, 179–194. [Google Scholar] [CrossRef]
- Liang, X.X.; Fu, Y.; Cao, W.T.; Wang, Z.; Zhang, K.; Jiang, Z.; Jia, X.; Liu, C.Y.; Lin, H.R.; Zhong, H.; et al. Gut microbiome, cognitive function and brain structure: A multi-omics integration analysis. Transl. Neurodegener. 2022, 11, 49. [Google Scholar] [CrossRef] [PubMed]
- Tarnoki, A.D.; Tarnoki, D.L.; Forgo, B.; Szabo, H.; Melicher, D.; Metneki, J.; Littvay, L. The Hungarian Twin Registry Update: Turning From a Voluntary to a Population-Based Registry. Twin Res. Hum. Genet. 2019, 22, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Heath, A.C.; Nyholt, D.R.; Neuman, R.; Madden, P.A.; Bucholz, K.K.; Todd, R.D.; Nelson, E.C.; Montgomery, G.W.; Martin, N.G. Zygosity diagnosis in the absence of genotypic data: An approach using latent class analysis. Twin Res. 2003, 6, 22–26. [Google Scholar] [CrossRef]
- Fiorenzato, E.; Weis, L.; Falup-Pecurariu, C.; Diaconu, S.; Siri, C.; Reali, E.; Pezzoli, G.; Bisiacchi, P.; Antonini, A.; Biundo, R. Montreal Cognitive Assessment (MoCA) and Mini-Mental State Examination (MMSE) performance in progressive supranuclear palsy and multiple system atrophy. J. Neural Transm. 2016, 123, 1435–1442. [Google Scholar] [CrossRef]
- Rittman, T.; Ghosh, B.C.; McColgan, P.; Breen, D.P.; Evans, J.; Williams-Gray, C.H.; Barker, R.A.; Rowe, J.B. The Addenbrooke’s Cognitive Examination for the differential diagnosis and longitudinal assessment of patients with parkinsonian disorders. J. Neurol. Neurosurg. Psychiatry 2013, 84, 544–551. [Google Scholar] [CrossRef]
- Schmotz, C.; Richinger, C.; Lorenzl, S. High Burden and Depression among Late-Stage Idiopathic Parkinson Disease and Progressive Supranuclear Palsy Caregivers. J. Geriatr. Psychiatry Neurol. 2017, 30, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Cuoco, S.; Cappiello, A.; Abate, F.; Tepedino, M.F.; Erro, R.; Volpe, G.; Pellecchia, M.T.; Barone, P.; Picillo, M. Psychometric properties of the Beck Depression Inventory-II in progressive supranuclear palsy. Brain Behav. 2021, 11, e2344. [Google Scholar] [CrossRef]
- Bosy-Westphal, A.; Later, W.; Hitze, B.; Sato, T.; Kossel, E.; Gluer, C.C.; Heller, M.; Muller, M.J. Accuracy of bioelectrical impedance consumer devices for measurement of body composition in comparison to whole body magnetic resonance imaging and dual X-ray absorptiometry. Obes. Facts 2008, 1, 319–324. [Google Scholar] [CrossRef]
- Zhong, L.; Xie, Y.Z.; Cao, T.T.; Wang, Z.; Wang, T.; Li, X.; Shen, R.C.; Xu, H.; Bu, G.; Chen, X.F. A rapid and cost-effective method for genotyping apolipoprotein e gene polymorphism. Mol. Neurodegener. 2016, 11, 2. [Google Scholar] [CrossRef]
- 16S Sample Preparation Guide. Available online: https://emea.support.illumina.com/content/dam/illumina-support/documents/documentation/chemistry_documentation/16s/16s-metagenomic-library-prep-guide-15044223-b.pdf (accessed on 23 August 2023).
- Weber, N.; Liou, D.; Dommer, J.; MacMenamin, P.; Quiñones, M.; Misner, I.; Oler, A.J.; Wan, J.; Kim, L.; Coakley McCarthy, M.; et al. Nephele: A cloud platform for simplified, standardized and reproducible microbiome data analysis. Bioinformatics 2018, 34, 1411–1413. [Google Scholar] [CrossRef]
- Bolyen, E.; Rideout, J.R.; Dillon, M.R.; Bokulich, N.A.; Abnet, C.C.; Al-Ghalith, G.A.; Alexander, H.; Alm, E.J.; Arumugam, M.; Asnicar, F.; et al. Reproducible, interactive, scalable and extensible microbiome data science using QIIME 2. Nat. Biotechnol. 2019, 37, 852–857. [Google Scholar] [CrossRef] [PubMed]
- Quast, C.; Pruesse, E.; Yilmaz, P.; Gerken, J.; Schweer, T.; Yarza, P.; Peplies, J.; Glöckner, F.O. The SILVA ribosomal RNA gene database project: Improved data processing and web-based tools. Nucleic Acids Res. 2012, 41, D590–D596. [Google Scholar] [CrossRef] [PubMed]
- Rorden, C.; Karnath, H.O.; Bonilha, L. Improving lesion-symptom mapping. J. Cogn. Neurosci. 2007, 19, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Kamraoui, R.A.; Ta, V.T.; Tourdias, T.; Mansencal, B.; Manjon, J.V.; Coup, P. DeepLesionBrain: Towards a broader deep-learning generalization for multiple sclerosis lesion segmentation. Med. Image Anal. 2022, 76, 102312. [Google Scholar] [CrossRef] [PubMed]
- Coupé, P.; Mansencal, B.; Clément, M.; Giraud, R.; Denis de Senneville, B.; Ta, V.T.; Lepetit, V.; Manjon, J.V. AssemblyNet: A large ensemble of CNNs for 3D whole brain MRI segmentation. NeuroImage 2020, 219, 117026. [Google Scholar] [CrossRef]
- Park, H.K.; Ilango, S.D.; Litvan, I. Environmental risk factors for progressive supranuclear palsy. J. Mov. Disord. 2021, 14, 103–113. [Google Scholar] [CrossRef]
- Vidal, J.S.; Vidailhet, M.; Derkinderen, P.; de Gaillarbois, T.D.; Tzourio, C.; Alpérovitch, A. Risk factors for progressive supranuclear palsy: A case-control study in France. J. Neurol. Neurosurg. Psychiatry 2009, 80, 1271–1274. [Google Scholar] [CrossRef]
- Vanacore, N.; Bonifati, V.; Fabbrini, G.; Colosimo, C.; Marconi, R.; Nicholl, D.; Bonuccelli, U.; Stocchi, F.; Lamberti, P.; Volpe, G.; et al. Smoking habits in multiple system atrophy and progressive supranuclear palsy. Neurology 2000, 54, 114–119. [Google Scholar] [CrossRef]
- Litvan, I.; Lees, P.S.; Cunningham, C.R.; Rai, S.N.; Cambon, A.C.; Standaert, D.G.; Marras, C.; Juncos, J.; Riley, D.; Reich, S.; et al. Environmental and occupational risk factors for progressive supranuclear palsy: Case-control study. Mov. Disord. 2016, 31, 644–652. [Google Scholar] [CrossRef]
- Rabadia, S.V.; Litvan, I.; Juncos, J.; Bordelon, Y.; Riley, D.E.; Standaert, D.; Reich, S.G.; Hall, D.A.; Kluger, B.; Shprecher, D.; et al. Hypertension and progressive supranuclear palsy. Park. Relat Disord. 2019, 66, 166–170. [Google Scholar] [CrossRef]
- Boxer, A.L.; Yu, J.T.; Golbe, L.I.; Litvan, I.; Lang, A.E.; Höglinger, G.U. Advances in progressive supranuclear palsy: New diagnostic criteria, biomarkers, and therapeutic approaches. Lancet Neurol. 2017, 16, 552–563. [Google Scholar] [CrossRef] [PubMed]
- Chouliaras, L.; Thomas, A.; Malpetti, M.; Donaghy, P.; Kane, J.; Mak, E.; Savulich, G.; Prats-Sedano, M.A.; Heslegrave, A.J.; Zetterberg, H.; et al. Differential levels of plasma biomarkers of neurodegeneration in Lewy body dementia, Alzheimer’s disease, frontotemporal dementia and progressive supranuclear palsy. J. Neurol. Neurosurg. Psychiatry 2022, 93, 651–658. [Google Scholar] [CrossRef]
- Jabbari, E.; Zetterberg, H.; Morris, H.R. Tracking and predicting disease progression in progressive supranuclear palsy: CSF and blood biomarkers. J. Neurol. Neurosurg. Psychiatry 2017, 88, 883–888. [Google Scholar] [CrossRef] [PubMed]
- Morris, H.R. Blood based biomarkers for movement disorders. Acta Neurol. Scand. 2022, 146, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, K.; Tokumaru, A.M.; Shimoji, K.; Murayama, S.; Kanemaru, K.; Morimoto, S.; Aiba, I.; Nakagawa, M.; Ozawa, Y.; Shimohira, M.; et al. Beyond the midbrain atrophy: Wide spectrum of structural MRI finding in cases of pathologically proven progressive supranuclear palsy. Neuroradiology 2017, 59, 431–443. [Google Scholar] [CrossRef]
- Litvan, I. Update on progressive supranuclear palsy. Curr. Neurol. Neurosci. Rep. 2004, 4, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Schrag, A.; Sheikh, S.; Quinn, N.P.; Lees, A.J.; Selai, C.; Mathias, C.; Litvan, I.; Lang, A.E.; Bower, J.H.; Burn, D.J.; et al. A comparison of depression, anxiety, and health status in patients with progressive supranuclear palsy and multiple system atrophy. Mov. Disord. 2010, 25, 1077–1081. [Google Scholar] [CrossRef] [PubMed]
- Saji, N.; Murotani, K.; Hisada, T.; Tsuduki, T.; Sugimoto, T.; Kimura, A.; Niida, S.; Toba, K.; Sakurai, T. The relationship between the gut microbiome and mild cognitive impairment in patients without dementia: A cross-sectional study conducted in Japan. Sci. Rep. 2019, 9, 19227. [Google Scholar] [CrossRef]
- Khedr, E.M.; Ali, A.M.; Deaf, E.; Hassan, H.M.; Alaa, A.; Gamea, A. Gut microbiota in Parkinson’s disease patients: Hospital-based study. Egypt. J. Neurol. Psychiatry Neurosurg. 2021, 57, 153. [Google Scholar] [CrossRef]
- Keshavarzian, A.; Green, S.J.; Engen, P.A.; Voigt, R.M.; Naqib, A.; Forsyth, C.B.; Mutlu, E.; Shannon, K.M. Colonic bacterial composition in Parkinson’s disease. Mov. Disord. 2015, 30, 1351–1360. [Google Scholar] [CrossRef]
- Hasegawa, S.; Goto, S.; Tsuji, H.; Okuno, T.; Asahara, T.; Nomoto, K.; Shibata, A.; Fujisawa, Y.; Minato, T.; Okamoto, A.; et al. Intestinal dysbiosis and lowered serum lipopolysaccharide-binding protein in Parkinson’s disease. PLoS ONE 2015, 10, e0142164. [Google Scholar] [CrossRef]
- Barichella, M.; Severgnini, M.; Cilia, R.; Cassani, E.; Bolliri, C.; Caronni, S.; Ferri, V.; Cancello, R.; Ceccarani, C.; Faierman, S.; et al. Unraveling gut microbiota in Parkinson’s disease and atypical parkinsonism. Mov. Disord. 2019, 34, 396–405. [Google Scholar] [CrossRef]
- Tian, H.; Wang, J.; Feng, R.; Zhang, R.; Liu, H.; Qin, C.; Meng, L.; Chen, Y.; Fu, Y.; Liang, D.; et al. Efficacy of faecal microbiota transplantation in patients with progressive supranuclear palsy-Richardson’s syndrome: A phase 2, single centre, randomised clinical trial. eClinicalMedicine 2023, 58, 101888. [Google Scholar] [CrossRef] [PubMed]
- Zhan, S.; Liu, C.; Meng, J.; Mao, R.; Tu, T.; Lin, J.; Chen, M.; Zeng, Z.; Zhuang, X. Mucosa-Associated Oscillospira sp. Is Related to Intestinal Stricture and Post-Operative Disease Course in Crohn’s Disease. Microorganisms 2023, 11, 794. [Google Scholar] [CrossRef] [PubMed]
- Huber-Ruano, I.; Calvo, E.; Mayneris-Perxachs, J.; Rodríguez-Peña, M.M.; Ceperuelo-Mallafré, V.; Cedó, L.; Núñez-Roa, C.; Miro-Blanch, J.; Arnoriaga-Rodríguez, M.; Balvay, A.; et al. Orally administered Odoribacter laneus improves glucose control and inflammatory profile in obese mice by depleting circulating succinate. Microbiome 2022, 10, 135. [Google Scholar] [CrossRef] [PubMed]
- Biagi, E.; Franceschi, C.; Rampelli, S.; Severgnini, M.; Ostan, R.; Turroni, S.; Consolandi, C.; Quercia, S.; Scurti, M.; Monti, D.; et al. Gut Microbiota and Extreme Longevity. Curr. Biol. 2016, 26, 1480–1485. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Unaffected Twin | Affected Twin | Difference | |
|---|---|---|---|
| Birth weight (g) | 3500 | 3500 | - |
| Sport activity throughout the life | Yes (Running) | No | * |
| Coffee consumption | Yes (1 cup/day) | No | * |
| Smoking | Never | Yes (21.5 packs a years) | * |
| Hypertension | Yes (40 years) | Yes (20 years) | |
| Cardiovascular disease | No | No | - |
| Diabetes | No | Yes (4 years) | * |
| Dyslipidemia | No | No | - |
| Cancer | No | Breast cancer | * |
| Year at menopause | 55 | 60 | * |
| Birth control pills | No | Yes (30 years) | * |
| COVID infection | No | Yes (In the 2nd wave in 2022) | * |
| Unaffected Twin | Affected Twin | |
|---|---|---|
| BMI (kg/m2) | 29.4 | 21.7 |
| Body fat (%) | 38.4 | 30.5 |
| Visceral fat scale (1–30) | 12 | 7 |
| Body muscle (%) | 27.2 | 27.9 |
| SBP (mmHg) | 151 | 167 |
| DBP (mmHg) | 79 | 82 |
| Total cholesterol (mmol/L) | 5.1 | 4.9 |
| LDL-C (mmol/L) | 3.47 | 3.36 |
| HDL-C (mmol/L) | 1.55 | 1.30 |
| Triglyceride (mmol/L) | 1.1 | 1.2 |
| ApoA1 (mg/dL) | 1.79 | 1.5 |
| ApoB (mg/dL) | 1 | 0.98 |
| Lp(a) | 0.03 | 0.03 |
| ApoE genotype | 3/3 | 3/3 |
| Apo-AII (mg/dL) | 119.85 | 115.27 |
| Apo-CII (mg/dL) | 73.23 | 59.35 |
| Apo-CIII (mg/dL) | 17.50 | 15.72 |
| Apo-D (mg/dL) | 24.68 | 21.36 |
| Apo-E (mg/dL) | 71.26 | 61.65 |
| Apo-H (mg/dL) | 23.96 | 13.59 |
| Apo-J (mg/dL) | 45.27 | 42.14 |
| Apo-M (mg/dL) | 15.35 | 11.82 |
| Aβ40 (pg/mL) | 462.02 | 416.79 |
| Aβ42 (pg/mL) | 77.00 | 70.75 |
| TAU (pg/mL) | 48.79 | 36.83 |
| NFL (pg/mL) | 71.11 | 67.73 |
| αSyn (pg/mL) | 11.42 | 42.95 |
| ICAM1 (ng/mL) | 5.71 | 4.63 |
| VCAM1 (ng/mL) | 0.84 | 0.62 |
| MMP2 (ng/mL) | 76.08 | 36.59 |
| MMP9 (ng/mL) | 26.60 | 21.94 |
| NGAL (ng/mL) | 45.74 | 48.98 |
| CysC (ng/mL) | 162.33 | 130.66 |
| MB (ng/mL) | 42.09 | 10.48 |
| MPO (ng/mL) | 417.61 | 479.68 |
| MRP8/14 (ng/mL) | 2.62 | 2.51 |
| OPN (ng/mL) | 12.38 | 12.66 |
| SAA (ng/mL) | 45.75 | 46.74 |
| MMP9/MMP2 | 0.3497 | 0.5997 |
| Aβ42/Aβ40 | 0.1667 | 0.1697 |
| TAU/Aβ42 | 0.6336 | 0.5205 |
| ApoA1/SAA | 0.5015 | 0.3150 |
| ApoA1 | 22.00 | 14.00 |
| ApoA1/SAA | 4.8091 | 2.9950 |
| ApoB/ApoA1 | 0.56 | 0.65 |
| HDL/SAA | 3.39 | 2.78 |
| HDL/ApoD | 6.28 | 6.09 |
| HDL/ApoM | 10.10 | 11.00 |
| HDL/ApoJ | 3.42 | 3.09 |
| Unaffected Twin | Affected Twin | ||
|---|---|---|---|
| Handedness | Right | Right | |
| Addenbrooke Cognitive Examination | Attention | 18 points | 13 points |
| Memory | 29 points | 21 points | |
| Fluency | 10 points | 2 points | |
| Language | 27 points | 25 points | |
| Visuospatial skills | 5 points | 0 point | |
| Total points | 89 points * | 61 points * | |
| Mini-Mental State Examination | 30 points * | 22 points * | |
| Montreal Cognitive Assessment | 28 points * | 13 points * | |
| Beck Depression Inventory | 2 points | 4 points | |
| Geriatric Depression Scale | 0 point | 1 point | |
| Zung Self-Rating Depression Scale | 27 points | 28 points | |
| Variable | Unaffected Twin | Affected Twin |
|---|---|---|
| Total lesions count | 24 | 36 |
| Total lesions volume (cm3) | 3.9192 | 30.0650 |
| Periventricular lesions count | 9 | 8 |
| Periventricular lesions volume (cm3) | 3.3902 | 29.4052 |
| Deep white lesions count | 12 | 17 |
| Deep white lesions volume (cm3) | 0.3136 | 0.3823 |
| Juxtacortical lesions count | 2 | 8 |
| Juxtacortical lesions volume (cm3) | 0.0362 | 0.2238 |
| Infratentorial cerebellar lesions count | 1 | 2 |
| Infratentorial cerebellar lesions volume (cm3) | 0.1793 | 0.0403 |
| Infratentorial medullary lesions count | 0 | 1 |
| Infratentorial medullary lesions volume (cm3) | 0 | 0.0132 |
| Volumes | Unaffected Twin | Affected Twin |
|---|---|---|
| Total white matter volume (cm3) | 403.59 | 387.12 |
| Total gray matter volume (cm3) | 664.13 | 623.45 |
| Total brainstem volume (cm3) | 20.34 | 16.14 |
| Frontal lobe volume (cm3) | 168.08 | 155.58 |
| Temporal lobe volume (cm3) | 103.83 | 103.51 |
| Parietal lobe volume (cm3) | 97.28 | 89.20 |
| Occipital lobe volume (cm3) | 80.16 | 76.79 |
| CSF Volume | Unaffected Twin | Affected Twin |
|---|---|---|
| Total CSF volume (cm3) | 220.89 | 272.12 |
| Inferior lateral ventricle volume (cm3) | 4 | 7.30 |
| Lateral ventricle volume (cm3) | 64.49 | 94.48 |
| 3rd ventricle volume (cm3) | 2.93 | 3.85 |
| 4th ventricle volume (cm3) | 3.55 | 5.27 |
| External CSF volume (cm3) | 145.92 | 161.23 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Persely, A.; Beszedics, B.; Paloczi, K.; Piroska, M.; Alijanpourotaghsara, A.; Strelnikov, D.; Vessal, A.; Szabo, H.; Hernyes, A.; Zoldi, L.; et al. Analysis of Genetic and MRI Changes, Blood Markers, and Risk Factors in a Twin Pair Discordant of Progressive Supranuclear Palsy. Medicina 2023, 59, 1696. https://doi.org/10.3390/medicina59101696
Persely A, Beszedics B, Paloczi K, Piroska M, Alijanpourotaghsara A, Strelnikov D, Vessal A, Szabo H, Hernyes A, Zoldi L, et al. Analysis of Genetic and MRI Changes, Blood Markers, and Risk Factors in a Twin Pair Discordant of Progressive Supranuclear Palsy. Medicina. 2023; 59(10):1696. https://doi.org/10.3390/medicina59101696
Chicago/Turabian StylePersely, Aliz, Beatrix Beszedics, Krisztina Paloczi, Marton Piroska, Amirreza Alijanpourotaghsara, David Strelnikov, Arsalan Vessal, Helga Szabo, Anita Hernyes, Luca Zoldi, and et al. 2023. "Analysis of Genetic and MRI Changes, Blood Markers, and Risk Factors in a Twin Pair Discordant of Progressive Supranuclear Palsy" Medicina 59, no. 10: 1696. https://doi.org/10.3390/medicina59101696