
Incidental Axillary Dose of Tomotherapy in Hypofractionated Whole Breast Radiotherapy for Early Breast Cancer: A Dosimetrical Analysis
 , ,
, ,
Abstract
:1. Introduction
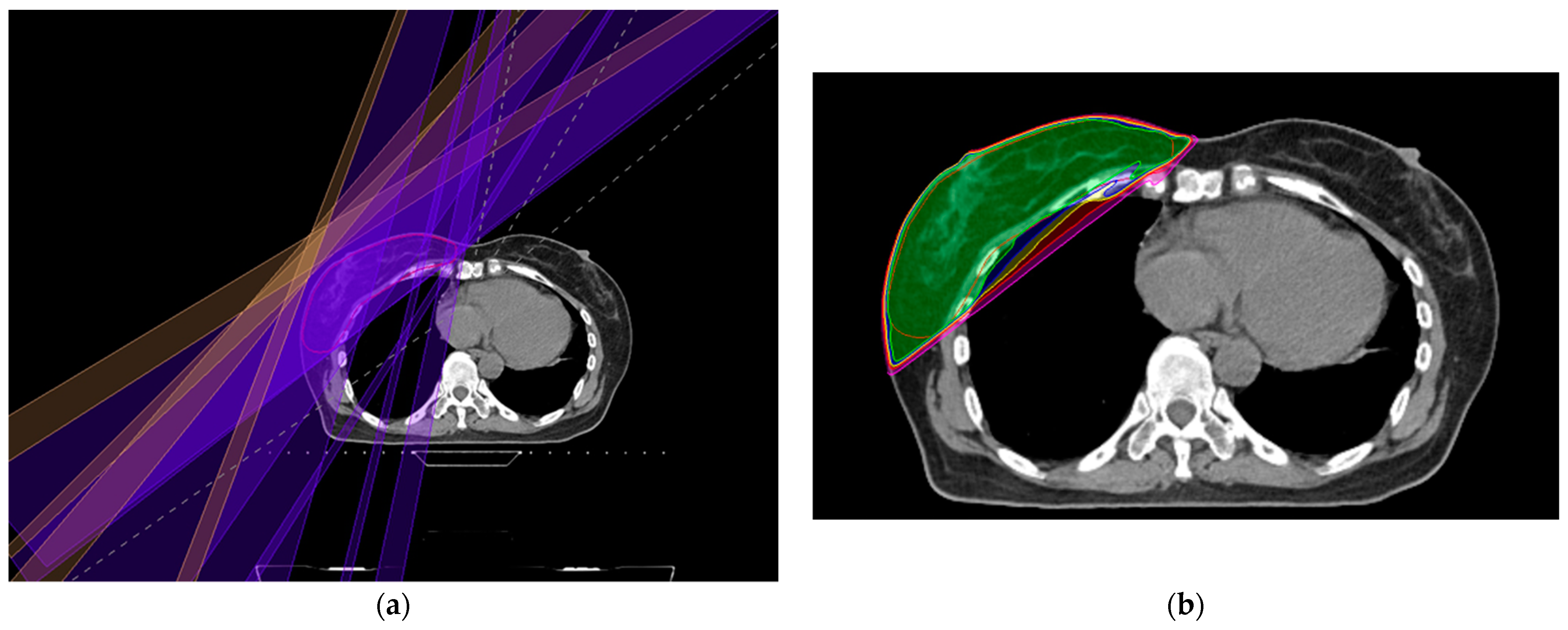
2. Materials and Methods
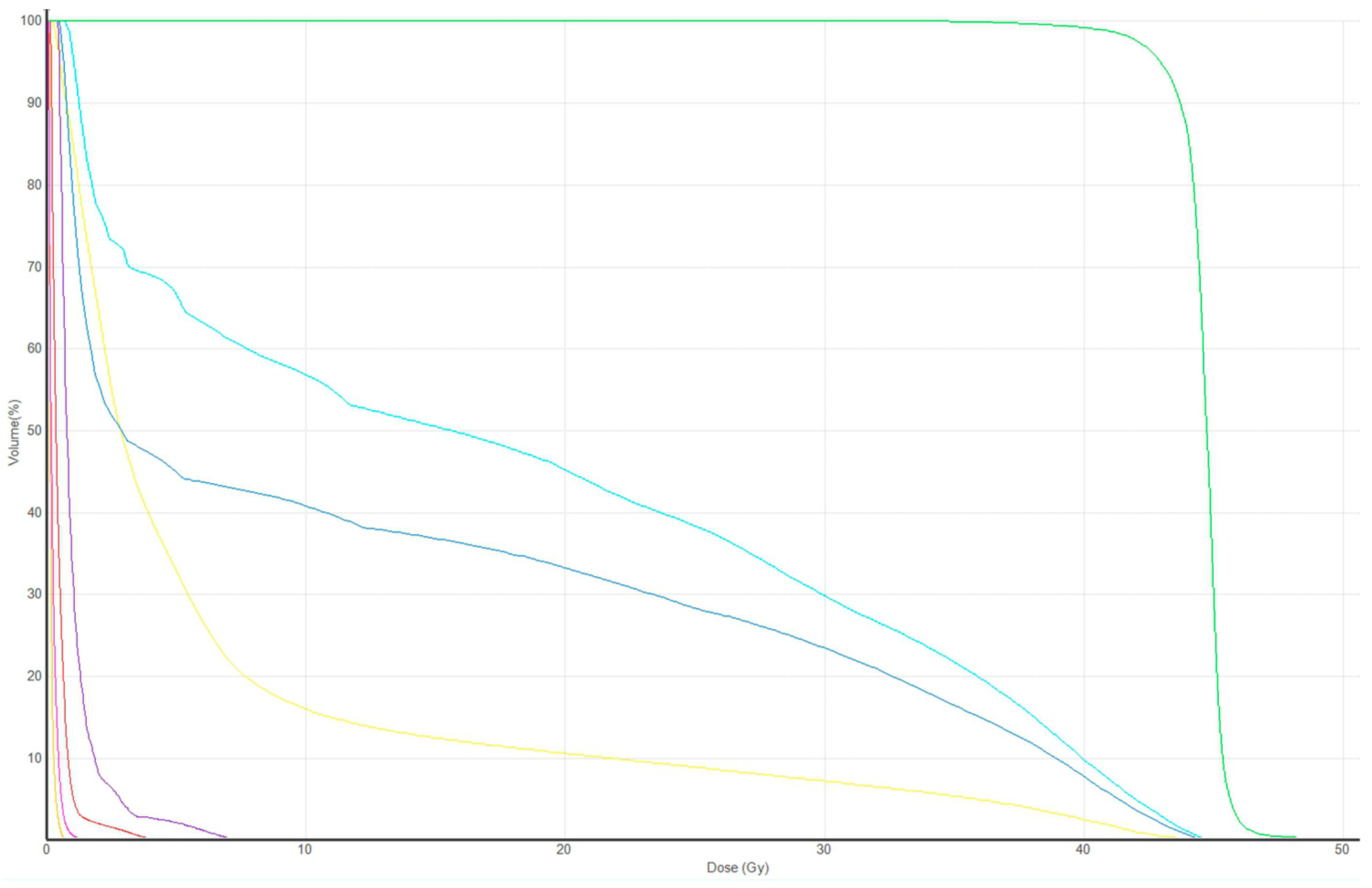
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schmitt, M.; Pin, Y.; Pflumio, C.; Mathelin, C.; Pivot, X.; Noel, G. Incidental axillary dose delivery to axillary lymph node levels I-III by different techniques of whole-breast irradiation: A systematic literature review. Strahlenther. Onkol. 2021, 197, 820–828. [Google Scholar] [CrossRef] [PubMed]
- Jagsi, R.; Chadha, M.; Moni, J.; Ballman, K.; Laurie, F.; Buchholz, T.A.; Giuliano, A.; Haffty, B.G. Radiation field design in the ACOSOG Z0011 (Alliance) Trial. J. Clin. Oncol. 2014, 32, 3600–3606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, J.S.; Chang, J.H.; Kim, N.; Kim, Y.B.; Shin, K.H.; Kim, K. Intensity Modulated Radiotherapy and Volumetric Modulated Arc Therapy in the Treatment of Breast Cancer: An Updated Review. J. Breast Cancer 2022, 25, 349–365. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.C.; Kim, S.H.; Suh, Y.J.; Chung, M.J.; Kang, D.G.; Choi, H.J.; Lee, J.H. A prospective cohort study on postoperative radiotherapy with TomoDirect using simultaneous integrated boost technique in early breast cancer. Radiat. Oncol. 2014, 9, 244. [Google Scholar] [CrossRef] [Green Version]
- Squires, M.; Hu, Y.; Byrne, M.; Archibald-Heeren, B.; Cheers, S.; Bosco, B.; Teh, A.; Fong, A. Static beam tomotherapy as an optimisation method in whole-breast radiation therapy (WBRT). J. Med. Radiat. Sci. 2017, 64, 281–289. [Google Scholar] [CrossRef] [Green Version]
- Mayinger, M.; Borm, K.J.; Dreher, C.; Dapper, H.; Duma, M.N.; Oechsner, M.; Kampfer, S.; Combs, S.E.; Habermehl, D. Incidental dose distribution to locoregional lymph nodes of breast cancer patients undergoing adjuvant radiotherapy with tomotherapy—Is it time to adjust current contouring guidelines to the radiation technique? Radiat. Oncol. 2019, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Offersen, B.V.; Boersma, L.J.; Kirkove, C.; Hol, S.; Aznar, M.C.; Biete Sola, A.; Kirova, Y.M.; Pignol, J.-P.; Remouchamps, V.; Verhoeven, K.; et al. ESTRO consensus guideline on target volume delineation for elective radiation therapy of early stage breast cancer. Radiother. Oncol. 2015, 114, 3–10. [Google Scholar] [CrossRef]
- Kainz, K.; Huang, M.; Xiao, Y.; Li, X.A.; Moran, J.M.; Chen, G.-P. NRG Protocol Radiation Therapy Template (Whole Breast Photon and Proton Therapy). NRG Oncol. 2022. [Google Scholar]
- Reznik, J.; Cicchetti, M.G.; Degaspe, B.; Fitzgerald, T.J. Analysis of axillary coverage during tangential radiation therapy to the breast. Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 163–168. [Google Scholar] [CrossRef]
- Zhang, L.; Yang, Z.Z.; Chen, X.X.; Tuan, J.; Ma, J.L.; Mei, X.; Yu, X.-L.; Zhou, Z.-R.; Shao, Z.-M.; Liu, G.-Y.; et al. Dose coverage of axillary level I-III areas during whole breast irradiation with simplified intensity modulated radiation therapy in early stage breast cancer patients. Oncotarget 2015, 6, 18183–18191. [Google Scholar] [CrossRef] [Green Version]
- De Santis, M.C.; Bonfantini, F.; Dispinzieri, M.; Meroni, S.; Diletto, B.; Mantero, E.D.; Franceschini, M.; Soncini, F.; Di Cosimo, S.; Cosentino, V.; et al. Axillary coverage by whole breast irradiation in 1 to 2 positive sentinel lymph nodes in breast cancer patients. Tumori 2016, 102, 409–413. [Google Scholar] [CrossRef]
- Aguiar, A.; Gomes Pereira, H.; Azevedo, I.; Gomes, L. Evaluation of axillary dose coverage following whole breast radiotherapy: Variation with the breast volume and shape. Radiother. Oncol. 2015, 114, 22–27. [Google Scholar] [CrossRef]
- Ahrouch, I.; Van Gestel, D.; Koshariuk, O.; Kirkove, C.; Desmet, A.; Philippson, C.; Reynaert, N.; De Caluwe, A. Unintended dose to the lower axilla in adjuvant radiotherapy for breast cancer: Differences between tangential beam and VMAT. Radiother. Oncol. 2021, 164, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Kataria, T.; Bisht, S.S.; Gupta, D.; Goyal, S.; Jassal, K.; Abhishek, A.; Sharma, K.; Pareek, P.; Kumar, V.; Jain, S.; et al. Incidental radiation to axilla in early breast cancer treated with intensity modulated tangents and comparison with conventional and 3D conformal tangents. Breast 2013, 22, 1125–1129. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kim, S.W.; Son, S.H. Dosimetric evaluation of incidental irradiation to the axilla during whole breast radiotherapy for patients with left-sided early breast cancer in the IMRT era. Medicine 2016, 95, e4036. [Google Scholar] [CrossRef]
- Jo, I.Y.; Kim, E.S.; Kim, W.C.; Min, C.K.; Yeo, S.G. Dosimetric comparison of incidental axillary irradiation between three-dimensional conformal and volumetric modulated arc techniques for breast cancer. Mol. Clin. Oncol. 2020, 12, 551–556. [Google Scholar] [CrossRef] [Green Version]
- Giuliano, A.E.; Ballman, K.V.; McCall, L.; Beitsch, P.D.; Brennan, M.B.; Kelemen, P.R.; Ollila, D.W.; Hansen, N.M.; Whitworth, P.W.; Leitch, A.M.; et al. Effect of Axillary Dissection vs. No Axillary Dissection on 10-Year Overall Survival among Women with Invasive Breast Cancer and Sentinel Node Metastasis: The ACOSOG Z0011 (Alliance) Randomized Clinical Trial. JAMA 2017, 318, 918–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giuliano, A.E.; McCall, L.; Beitsch, P.; Whitworth, P.W.; Blumencranz, P.; Leitch, A.M.; Saha, S.; Hunt, K.K.; Morrow, M.; Ballman, K. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: The American College of Surgeons Oncology Group Z0011 randomized trial. Ann. Surg. 2010, 252, 426–432; discussion 432–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.S.; Shin, K.H.; Choi, N.; Lee, S.W. Hypofractionated whole breast irradiation: New standard in early breast cancer after breast-conserving surgery. Radiat. Oncol. J. 2016, 34, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Borm, K.J.; Oechsner, M.; Düsberg, M.; Buschner, G.; Wolfgang, W.; Combs, S.E.; Duma, M.N. Effect of hypofractionation on the incidental axilla dose during tangential field radiotherapy in breast cancer. Strahlenther. Onkol. 2020, 196, 771–778. [Google Scholar] [CrossRef]
- NCCN Practice Guidelines for Breast Cancer (Version 3. 2023); National Comprehensive Cancer Network: Bethesda, MD, USA, 2023.
- Lee, T.H.; Chang, J.H.; Jang, B.S.; Kim, J.S.; Kim, T.H.; Park, W.; Kim, Y.B.; Kim, S.S.; Han, W.; Lee, H.-B.; et al. Protocol for the postoperative radiotherapy in N1 breast cancer patients (PORT-N1) trial, a prospective multicenter, randomized, controlled, non-inferiority trial of patients receiving breast-conserving surgery or mastectomy. BMC Cancer 2022, 22, 1179. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Ward, R.; Jia, D.; Ashworth, S.; Estoesta, E.; Moodie, T.; Ahern, V.; Stuart, K.; Ngui, N.; French, J.; et al. Location of arm draining lymph node in relation to breast cancer radiotherapy field and target volume. Radiother. Oncol. 2019, 133, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Gross, J.P.; Lynch, C.M.; Flores, A.M.; Jordan, S.W.; Helenowski, I.B.; Gopalakrishnan, M.; Cutright, D.; Donnelly, E.D.; Strauss, J.B. Determining the Organ at Risk for Lymphedema After Regional Nodal Irradiation in Breast Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, 649–658. [Google Scholar] [CrossRef] [PubMed]
- Schlafstein, A.; Liu, Y.; Goyal, S.; Kahn, S.; Godette, K.; Lin, J.; Torres, M.A.; Royce, T.J.; Patel, S.A. Regional Nodal Irradiation for Clinically Node-Positive Breast Cancer Patients with Pathologic Negative Nodes after Neoadjuvant Chemotherapy. Clin. Breast Cancer 2022, 22, 127–135. [Google Scholar] [CrossRef]
- Pilewskie, M.; Morrow, M. Axillary Nodal Management Following Neoadjuvant Chemotherapy: A Review. JAMA Oncol. 2017, 3, 549–555. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristics | N (%) | |
|---|---|---|
| Age, median (range) | 51 (40–66) | |
| Laterality | Left | 18 (60.0) |
| Right | 12 (40.0) | |
| pT stage * | T1a | 2 (6.7) |
| T1b | 10 (33.3) | |
| T1c | 10 (33.3) | |
| T2 | 8 (26.7) | |
| pN stage * | N0 | 28 (93.3) |
| Nmi | 2 (6.7) | |
| Pathology | Invasive ductal carcinoma | 26 (86.6) |
| Invasive lobular carcinoma | 2 (6.7) | |
| Invasive carcinoma, no special type | 2 (6.7) |
| Axilla Levels | Dmean, % (Gy ± SD) | V95%[%] | V90%[%] | V80%[%] | V50%[%] |
|---|---|---|---|---|---|
| Level I | 35.5 (15.5 ± 4.8) | 4.7 ± 3.9 | 7.7 ± 5.8 | 14.0 ± 8.6 | 35.3 ± 14.4 |
| Level II | 35.1 (14.9 ± 4.2) | 4.8 ± 3.7 | 9.2 ± 5.1 | 18.0 ± 7.8 | 36.1 ± 11.9 |
| Level III | 3.5 (1.5 ± 1.6) | 0 ± 0 | 0 ± 0 | 0 ± 0 | 0.7 ± 2.3 |
| RT Techniques | Axilla Levels | Dmean, % (Gy) | V95%[%] | V90%[%] | V80%[%] |
|---|---|---|---|---|---|
| HT [9] | Level I | 86 | 79 | ND | ND |
| Level II | 71 | 51 | ND | ND | |
| Level III | 73 | 49 | ND | ND | |
| ST [9] | Level I | 66 | 51 | ND | ND |
| Level II | 44 | 26 | ND | ND | |
| Level III | 31 | 15 | ND | ND | |
| s-IMRT [10] | Level I | 55.4 (27.7) | 16.9 | 22.1 | 31.3 |
| Level II | 21.2 (10.6) | 1.7 | 2.7 | 5.7 | |
| Level III | 5 (2.5) | 0 | 0 | 0.1 | |
| VMAT * [11] | Level I | 26.66 | 2.6 | 6 | ND |
| Level II | 17.83 | 2.6 | 2.4 | ND | |
| Level III | 5.96 | ND | ND | ND |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeo, S.-G.; Lim, C.W.; Hur, S.-M.; Kim, Z.; Cho, K.H.; Kim, M.-J. Incidental Axillary Dose of Tomotherapy in Hypofractionated Whole Breast Radiotherapy for Early Breast Cancer: A Dosimetrical Analysis. Medicina 2023, 59, 1081. https://doi.org/10.3390/medicina59061081
Yeo S-G, Lim CW, Hur S-M, Kim Z, Cho KH, Kim M-J. Incidental Axillary Dose of Tomotherapy in Hypofractionated Whole Breast Radiotherapy for Early Breast Cancer: A Dosimetrical Analysis. Medicina. 2023; 59(6):1081. https://doi.org/10.3390/medicina59061081
Chicago/Turabian StyleYeo, Seung-Gu, Cheol Wan Lim, Sung-Mo Hur, Zisun Kim, Kwang Hwan Cho, and Min-Jeong Kim. 2023. "Incidental Axillary Dose of Tomotherapy in Hypofractionated Whole Breast Radiotherapy for Early Breast Cancer: A Dosimetrical Analysis" Medicina 59, no. 6: 1081. https://doi.org/10.3390/medicina59061081