
Effectiveness of Pelvic Floor Muscle Training on Quality of Life in Women with Urinary Incontinence: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.1.1. Inclusion Criteria
2.1.2. Exclusion Criteria
2.2. Information Sources
2.3. Search Strategy
2.4. Selection Process
2.5. Data Collection Process
2.6. Data Items
2.7. Outcomes
2.8. Study Risk of Bias Assessment
2.9. Effect Measures
2.10. Synthesis Methods
2.11. Meta-Analysis
3. Results
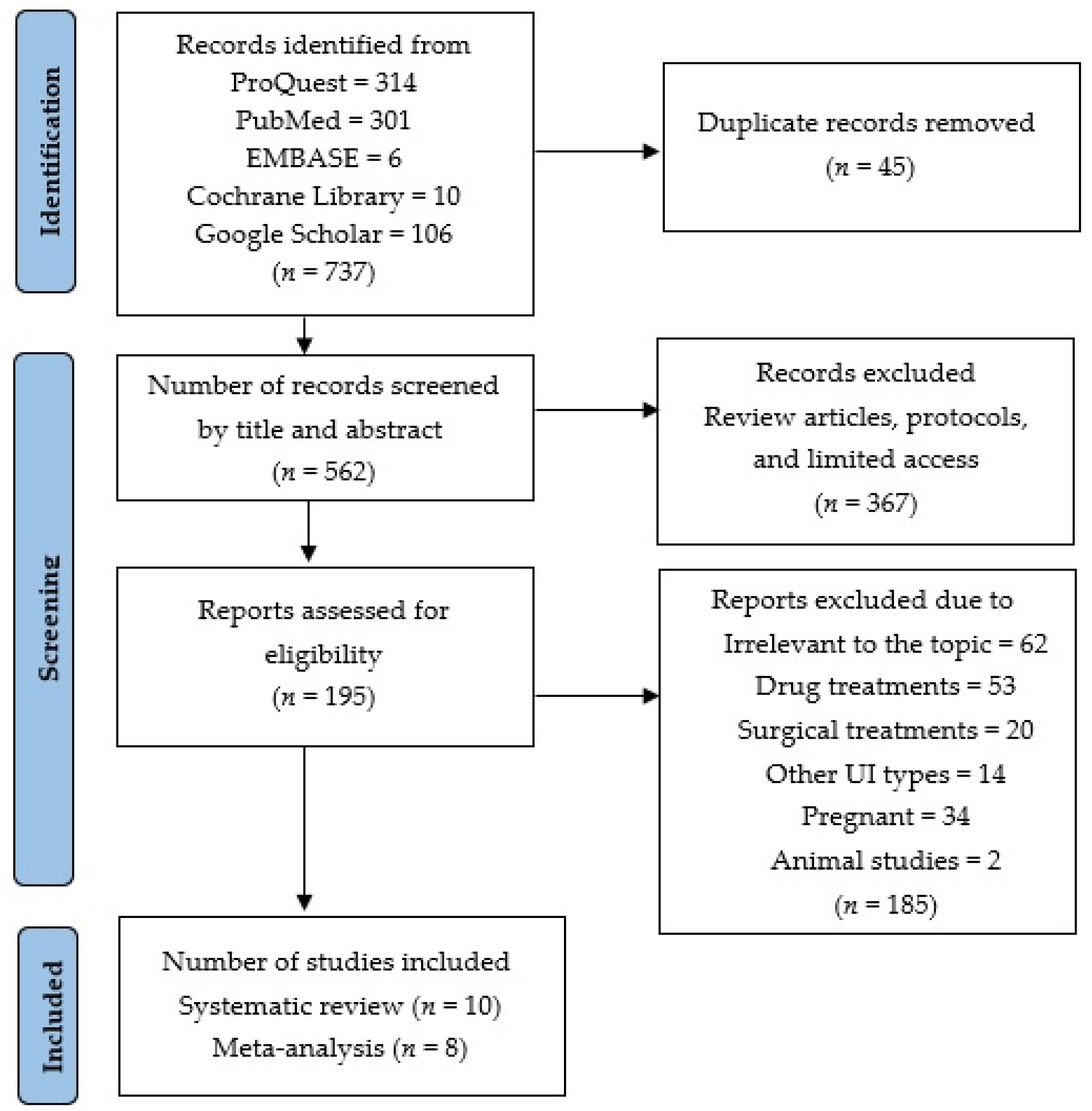
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias in Studies
4. Discussion
5. Conclusions
6. Additional Comments
7. Implications Section
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- D’Ancona, C.D.; Haylen, B.; Oelke, M.; Abranches-Monteiro, L.; Arnold, E.; Goldman, H.; Hamid, R.; Homma, Y.; Marcelissen, T.; Rademakers, K.; et al. Standardisation Steering Committee ICS and the ICS Working Group on Terminology for Male Lower Urinary Tract & Pelvic Floor Symptoms and Dysfunction. The International Continence Society (ICS) report on the terminology for adult male lower urinary tract and pelvic floor symptoms and dysfunction. Neurourol. Urodyn. 2019, 38, 433–477. [Google Scholar] [CrossRef] [PubMed]
- Tuda, C.M.; Carnero, M.P. Prevalence and factors associated with urinary incontinence in the east area of health of Valladolid. Enferm. Glob. 2020, 19, 390–412. [Google Scholar] [CrossRef]
- Wu, J.M.; Vaughan, C.P.; Goode, P.S.; Burgio, D.T. Prevalence and trends of symptomatic pelvic floor disorders in U.S. women. Obstet. Gynecol. 2014, 123, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Anger, J.T.; Saigal, C.S. The prevalence of urinary incontinence among community dwelling adult women: Results from the National Health and Nutrition Examination Survey. J. Urol. 2006, 175, 601–604. [Google Scholar] [CrossRef] [PubMed]
- Chiang, H.; Valdevenito, R.; Mercado, A. Incontinencia urinaria en el adulto mayor. Rev. Méd. Clín. Condes 2018, 29, 232–241. [Google Scholar] [CrossRef]
- Lukacz, E.S.; Lastra, Y.S.; Albo, M.E. Urinary Incontinence in Women: A review. JAMA 2017, 318, 1592–1604. [Google Scholar] [CrossRef]
- World Health Organization. Ageing and Health. 2022. Available online: https://www.who.int/es/news-room/fact-sheets/detail/ageing-and-health (accessed on 1 December 2022).
- National Collaborating Centre for Women’s and Children’s Health. In Urinary Incontinence in Women: The Management of Urinary Incontinence in Women; NICE Clinical Guidelines, No. 171; National Collaborating Centre for Women's and Children's Health: London, UK, 2015; Volume 171, pp. 32–38. Available online: https://www.ncbi.nlm.nih.gov/books/NBK247723/ (accessed on 2 December 2022).
- Melville, J.L.; Fan, M.Y.; Rau, H.; Nygaard, I.E.; Katon, W.J. Major depression and urinary incontinence in women: Temporal associations in an epidemiologic sample. Am. J. Obstet. Gynecol. 2009, 201, 490.e1–490.e7. [Google Scholar] [CrossRef]
- Irwin, G.M. Urinary Incontinence. Prim. Care 2019, 46, 233–242. [Google Scholar] [CrossRef]
- Campani, C.; Schreiner, L.; Picolli, T. Urinary incontinence and quality of life in female patients with obesity. Rev. Bras. Ginecol. Obstet. 2018, 40, 534–539. [Google Scholar] [CrossRef]
- Gram, M.C.; Bø, K. High level rhythmic gymnasts and urinary incontinence: Prevalence, risk factors, and influence on performance. Scand. J. Med. Sci. Sports 2020, 30, 159–165. [Google Scholar] [CrossRef]
- Daneshpajooh, A.; Naghibzadeh, T.A.; Najafipour, H.; Mirzaei, M. Prevalence and risk factors of urinary incontinence among Iranian women. Neurourol. Urodyn. 2021, 40, 642–652. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, J.A.; Tonon, S.; Brandão, S.; Da Luz, C.M.; Jorge, R.N.; Da Roza, T. Urinary Incontinence in Physically Active Young Women: Prevalence and Related Factors. Int. J. Sports Med. 2017, 38, 937–941. [Google Scholar] [CrossRef]
- Roberts, K.; Mahajan, S. Management of Urgency and Mixed Urinary Incontinence. Clin. Obstet. Gynecol. 2021, 64, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Vaughan, C.P.; Markland, A.D. Urinary Incontinence in Women. Ann. Intern. Med. 2020, 172, 17–32. [Google Scholar] [CrossRef] [PubMed]
- Betschart, C.; Singer, A.; Scheiner, D. Female pelvic floor: Anatomy and normal function. Ther. Umsch. 2019, 73, 529–534. [Google Scholar] [CrossRef]
- Bolla, S.R.; Hoare, B.S.; Varacallo, M.; Stat Pearls. Anatomy, Abdomen and Pelvis, Deep Perineal Space. 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK538272/ (accessed on 2 December 2022).
- Eickmeyer, S.M. Anatomy and Physiology of the Pelvic Floor. Phys. Med. Rehabil. Clin. N. Am. 2017, 28, 455–460. [Google Scholar] [CrossRef]
- Imamura, M.; Williams, K.; Wells, M.; McGrother, C. Lifestyle interventions for the treatment of urinary incontinence in adults. Cochrane Database Syst. Rev. 2015, 12, 50–62. [Google Scholar] [CrossRef]
- Kegel, A.H.; Powell, T. The physiologic treatment of urinary stress incontinence. J. Urol. 1950, 63, 808–814. [Google Scholar] [CrossRef]
- Hay-Smith, E.; Herderschee, R.; Dumoulin, C.; Herbison, G. Comparisons of approaches to pelvic floor muscle training for urinary incontinence in women. Cochrane Database Syst. Rev. 2011, 12, CD009508. [Google Scholar] [CrossRef]
- Riemsma, R.; Hagen, S.; Kirschner-Hermanns, R.; Norton, C.; Wijk, H.; Andersson, K.E.; Chapple, C.; Spinks, J.; Wagg, A.; Hutt, E.; et al. Can incontinence be cured? A systematic review of cure rates. BMC Med. 2017, 15, 63. [Google Scholar] [CrossRef]
- Lucas, M.G.; Bosch, R.J.; Burkhar, F.C.; Cruz, F.; Madden, T.B.; Nambiar, A.K.; Neisius, A.; de Ridder, D.J.; Tubaro, A.; Turner, W.H.; et al. European Association of Urology. EAU guidelines on assessment and nonsurgical management of urinary incontinence. Eur. Urol. 2012, 62, 1130–1142. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 15–88. [Google Scholar] [CrossRef]
- Shafaq, S.; Khan, A.A.; Kazi, M. Effects of Iyengar Yoga on pelvic floor muscle strength and endurance among young females with stress urinary incontinence. Pak. Armed Forces Med. J. 2022, 72, 1518–1521. [Google Scholar] [CrossRef]
- Luginbuehl, H.; Lehmann, C.; Koenig, I.; Kuhn, A.; Buergin, R.; Radlinger, L. Involuntary reflexive pelvic floor muscle training in addition. Int. Urogynecol. J. 2021, 33, 531–540. [Google Scholar] [CrossRef]
- Bezerra, L.O.; de Oliveira, M.C.E.; da Silva Filho, E.M.; Vicente da Silva, H.K.; Menezes de Oliveira, G.F.; da Silveira Gonçalves, A.K.; Pegado, R.; Micussi, M.T.A.B.C. Impact of Pelvic Floor Muscles Training Isolated and Associated with Game Therapy on Mixed Urinary Incontinence. Games Health J. 2020, 9, 43–49. [Google Scholar] [CrossRef]
- Hagen, S.; Elders, A.; Stratton, S.; Sergenson, N.; Bugge, C.; Dean, S.; Hay-Smith, J.; Kilonzo, M.; Dimitrova, M.; Abdel-Fattah, M.; et al. Effectiveness of pelvic floor muscle training with and without electromyographic biofeedback for urinary incontinence in women. BMJ 2020, 371, m3719. [Google Scholar] [CrossRef]
- Al Belushi, Z.I.; Al Kiyumi, M.H.; Al-Mazrui, A.A.; Jaju, S.; Alrawahi, A.H.; Al Mahrezi, A.M. Effects of home-based pelvic floor muscle training on decreasing symptoms of stress urinary incontinence and improving the quality of life of urban adult Omani women. Neurourol. Urodyn. 2020, 39, 1557–1566. [Google Scholar] [CrossRef]
- Szatmári, E.; Balla, B.J.; Simon-Ugron, Á.; Hock, M. Efficacy of pelvic floor muscle training in improving symptoms of urinary incontinence and health related quality of life among parous and nulliparous women. Timişoara Phys. Educ. Rehabil. J. 2020, 13, 36–45. [Google Scholar] [CrossRef]
- Fitz, F.F.; Gimenez, M.M.; de Azevedo Ferreira, L.; Matias, M.M.P.; Bortolini, M.A.T.; Castro, R.A. Pelvic floor muscle training for female stress urinary incontinence: A randomised control trial comparing home and outpatient training. Int. Urogynecol. J. 2020, 31, 989–998. [Google Scholar] [CrossRef]
- Ptak, M.; Ciećwież, S.; Brodowska, A.; Starczewski, A.; Nawrocka-Rutkowska, J.; Diaz-Mohedo, E.; Rotter, I. The Effect of Pelvic Floor Muscles Exercise on Quality of Life in Women with Stress Urinary Incontinence and Its Relationship with Vaginal Deliveries. Biomed. Res. Int. 2019, 2019, 5321864. [Google Scholar] [CrossRef]
- Wagg, A.; Chowdhury, Z.; Galarneau, J.M.; Haque, R.; Kabir, F.; MacDonald, D.; Naher, K.; Yasui, Y.; Cherry, N. Exercise intervention in the management of urinary incontinence in older women in villages in Bangladesh. Lancet Glob. Health 2019, 7, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Lausen, A.; Marsland, L.; Head, S.; Jackson, J.; Lausen, B. Modified Pilates as an adjunct to standard physiotherapy care for urinary incontinence. BMC Womens Health 2018, 18, 16. [Google Scholar] [CrossRef] [PubMed]
- Grøn Jensen, L.C.; Boie, S.; Axelsen, S. International consultation on incontinence questionnaire-Urinary incontinence short form ICIQ-UI SF: Validation of its use in a Danish speaking population of municipal employees. PLoS ONE 2022, 17, e0266479. [Google Scholar] [CrossRef] [PubMed]
- Viktrup, L.; Summers, K.; Dennett, S. Clinical practice guidelines for the initial management of urinary incontinence in women: A European-focused review. BJU Int. 2004, 94, 14–22. [Google Scholar] [CrossRef]
- Pizzol, D.; Demurtas, J.; Celotto, S.; Maggi, S.; Smith, L.; Angiolelli, G.; Trott, M.; Yang, L.; Veronese, N. Urinary incontinence and quality of life: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2021, 33, 25–35. [Google Scholar] [CrossRef]
- Fenocchi, L.; Collins, M.; Andrew, E.; Hagen, S. Assessment of the Relative Performance of the EQ-5D-3L, ICIQ-UI SF and POP-SS Using Data from the OPAL Trial. Int. J. Environ. Res. Public Health 2022, 19, 1351. [Google Scholar] [CrossRef]
- Mangir, N.; Sahan, A.; Tarcan, T. ICIQ-UI SF Is an Accurate Non-Invasive Tool that Can Be Used in Primary Care Setting to Determine the Type of Urinary Incontinence. In ICS 2011 Glasgow Istanbul; Marmara University School of Medicine: Istanbul, Turkey, 2011; p. 144. Available online: https://www.ics.org/2011/abstract/144 (accessed on 6 January 2023).
- Lasserre, A.; Pelat, C.; Guéroult, V.; Hanslik, T.; Chartier-Kastler, E.; Blanchon, T.; Ciofu, C.; Montefiore, E.D.; Alvarez, F.P.; Bloch, J. Urinary incontinence in French women: Prevalence, risk factors, and impact on quality of life. Eur. Urol. 2009, 56, 177–183. [Google Scholar] [CrossRef]
- Özdemır, Ö.; Bakar, Y.; Özengın, N.; Duran, B. The effect of parity on pelvic floor muscle strength and quality of life in women with urinary incontinence: A cross sectional study. J. Phys. Ther. Sci. 2015, 27, 2133–2137. [Google Scholar] [CrossRef]
- Pang, H.; Lv, J.; Xu, T.; Li, Z.; Gong, J.; Liu, Q.; Wang, Y.; Wang, J.; Xia, Z.; Li, Z.; et al. Incidence and risk factors of female urinary incontinence: A 4-year longitudinal study among 24,985 adult women in China. BJOG Int. J. Obstet. Gynaecol. 2021, 129, 580–589. [Google Scholar] [CrossRef]
- NICE Guidance. Urinary incontinence and pelvic organ prolapse in women: Management. BJU Int. 2019, 123, 777–803. [Google Scholar] [CrossRef]
- Hadizadeh-Talasaz, Z.; Sadeghi, R.; Khadivzadeh, T. Effect of pelvic floor muscle training on postpartum sexual function and quality of life: A systematic review and meta-analysis of clinical trials. Taiwan. J. Obstet. Gynecol. 2019, 58, 737–747. [Google Scholar] [CrossRef] [PubMed]
- Radzimińska, A.; Strączyńska, A.; Weber-Rajek, M.; Styczyńska, H.; Strojek, K.; Piekorz, Z. The impact of pelvic floor muscle training on the quality of life of women with urinary incontinence. Clin. Interv. Aging 2018, 17, 957–965. [Google Scholar] [CrossRef] [PubMed]
- Alouini, S.; Memic, S.; Couillandre, A. Pelvic Floor Muscle Training for Urinary Incontinence with or without Biofeedback or Electrostimulation in Women: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 15, 2789. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.; Feng, S.; Tong, B.; Lu, S.; Jin, Y. Effect of pelvic floor muscle training using mobile health applications for stress urinary incontinence in women: A systematic review. BMC Womens Health 2022, 22, 400. [Google Scholar] [CrossRef] [PubMed]
- Åström, Y.; Asklund, I.; Lindam, A.; Sjöström, M. Quality of life in women with urinary incontinence seeking care using e-health. BMC Womens Health 2021, 21, 337. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N° | Author (s) | Journal/Publication | Title | Year | Place |
|---|---|---|---|---|---|
| 1 | Shafaq, S et al. [26]. | Pakistan Armed Forces Medical Journal | Effects of Iyengar yoga on pelvic floor muscle strength and endurance among young females with SUI. | 2022 | Pakistan |
| 2 | Luginbuehl, H et al. [27]. | International Urogynecology Journal | Involuntary reflexive PFMT in addition to standard training versus standard training alone for women with SUI. | 2021 | Switzerland |
| 3 | Bezerra, L et al. [28]. | Games for Health Journal | Impact of PFMT isolated and associated with game therapy on MUI. | 2021 | Brazil |
| 4 | Hagen, S et al. [29]. | BMJ | Effectiveness of PFMT with and without electromyographic biofeedback for urinary incontinence in women | 2020 | Scotland and England |
| 5 | Al Belushi, Z et al. [30]. | Neuro-urology and Urodynamics | Effects of home-based PFMT on decreasing symptoms of stress urinary incontinence and improving the quality of life of urban adult Omani women | 2020 | Oman |
| 6 | Szatmári, E et al. [31]. | Timisoara Physical Education and Rehabilitation | Efficacy of PFMT in improving symptoms of urinary incontinence and health related quality of life among parous and nulliparous women | 2020 | Romania |
| 7 | Fitz, F et al. [32]. | International Urogynecology Journal | PFMT for female stress urinary incontinence | 2019 | Brazil |
| 8 | Ptak, M et al. [33]. | BioMed Research International | The effect of PFMT on quality of life in women with SUI and its relationship with vaginal deliveries | 2019 | Poland |
| 9 | Wagg, A et al. [34]. | Lancet Global Health | Exercise intervention in the management of urinary incontinence in older women in villages in Bangladesh | 2019 | Bangladesh |
| 10 | Lausen, A et al. [35]. | BMC Women’s Health | Modified Pilates as an adjunct to standard physiotherapy care for urinary incontinence | 2018 | England |
| Reference | Year | Country | Study Type | Number of Participants | Training Protocol | Outcome Measures | Main Findings |
|---|---|---|---|---|---|---|---|
| Shafaq, S et al. [26]. | 2022 | Pakistan | IS | 44 | Two days of supervised group yoga courses and one day of home yoga conducted once a week for 8 weeks. | ICIQ-UI SF | Improving PMS and endurance, decreasing UI symptoms and distress hence improving the QoL. |
| Luginbuehl, H et al. [27]. | 2021 | Switzerland | RCT | 92 | Involuntary reflexive PFMT triggered by whole-body movements such as jumps, for 16 weeks. | ICIQ-UI SF ICIQ-LUTS QoL | Score decreased about 3 points with no group differences at any point in time. |
| Bezerra, L et al. [28]. | 2021 | Brazil | RCT | 32 | PFMT+GT group, interventions occurred twice a week for 8 weeks. | Manometry, Pad test, ICIQ-UI SF, PGI-I | Both treatments proved to be effective. All women reported being ‘‘much better or better’’ |
| Hagen, S et al. [29]. | 2020 | Scotland and England | RCT | 593 | Biofeedback PFMT, were given six appointments with a continence therapist over 16 weeks. | ICIQ-UI SF Oxford classification | Routine use of electromyographic biofeedback with PFMT should not be recommended. |
| Al Belushi, Z et al. [30]. | 2020 | Oman | RCT | 73 | Unsupervised PFMT or a lecture with no PFMT for 12 weeks. | ICIQ-UI SF, MOGS, Manometry | PFMT is an effective treatment in reducing the severity of symptoms and improving the QoL. |
| Szatmári, E et al. [31]. | 2020 | Romania | IS | 42 | PFMT among parous and nulliparous women for 10 weeks. | ICIQ-UI SF, KHQ | Parous women were 2 times more likely to report UI. They also had more severe symptoms and lower QoL. |
| Fitz, F et al. [32]. | 2019 | Brazil | RCT | 69 | Outpatient PFMT and home PFMT under the guidance of a physiotherapist twice a week for 12 weeks. | Pad test, MOGS, I-QoL, | Both groups were satisfied after the treatment, even though this difference was not statistically significant. |
| Ptak, M et al. [33]. | 2019 | Poland | RCT | 137 | Combined training of the PFMT and the transversus abdominis muscle was executed for 12 weeks. | ICIQ-LUTS QoL | Both exercises improve the QoL of women with SUI. |
| Wagg, A et al. [34]. | 2019 | Bangladesh | RCT | 579 | PFMT was held twice a week for 12 weeks, with home exercises between classes. | EQ5D, CES-D-10, | Showed improvement in both intervention groups in the QoL and depression scales. |
| Lausen, A et al. [35]. | 2018 | England | RCT | 73 | Modified Pilates classes as an adjunct therapy to standard physiotherapy care for UI, for 6 weeks. | I-QOL, ICIQ-UI SF, ICIQ-LUTS QoL, RSE | Improved self-esteem, decreased social embarrassment and lower impact on normal daily activities. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Curillo-Aguirre, C.A.; Gea-Izquierdo, E. Effectiveness of Pelvic Floor Muscle Training on Quality of Life in Women with Urinary Incontinence: A Systematic Review and Meta-Analysis. Medicina 2023, 59, 1004. https://doi.org/10.3390/medicina59061004
Curillo-Aguirre CA, Gea-Izquierdo E. Effectiveness of Pelvic Floor Muscle Training on Quality of Life in Women with Urinary Incontinence: A Systematic Review and Meta-Analysis. Medicina. 2023; 59(6):1004. https://doi.org/10.3390/medicina59061004
Chicago/Turabian StyleCurillo-Aguirre, César Adrián, and Enrique Gea-Izquierdo. 2023. "Effectiveness of Pelvic Floor Muscle Training on Quality of Life in Women with Urinary Incontinence: A Systematic Review and Meta-Analysis" Medicina 59, no. 6: 1004. https://doi.org/10.3390/medicina59061004