

Experience with Optical Coherence Tomography Enhanced by a Novel Software (Ultreon™ 1.0 Software)—The First One Hundred Cases
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Optical Coherence Tomography—Image Aquisition and Processing
2.3. Definitions
2.4. Statistical Analysis
3. Results
3.1. General Characteristics and Concomitant Disease at Baseline (before Index Procedure)
3.2. Biochemical Characteristics at Baseline (before Index Procedure)
3.3. Procedural Characteristics (Index Procedure)
3.4. OCT Parameters (Index Procedure)
3.5. Pharmacotherapy (after Index Procedure)
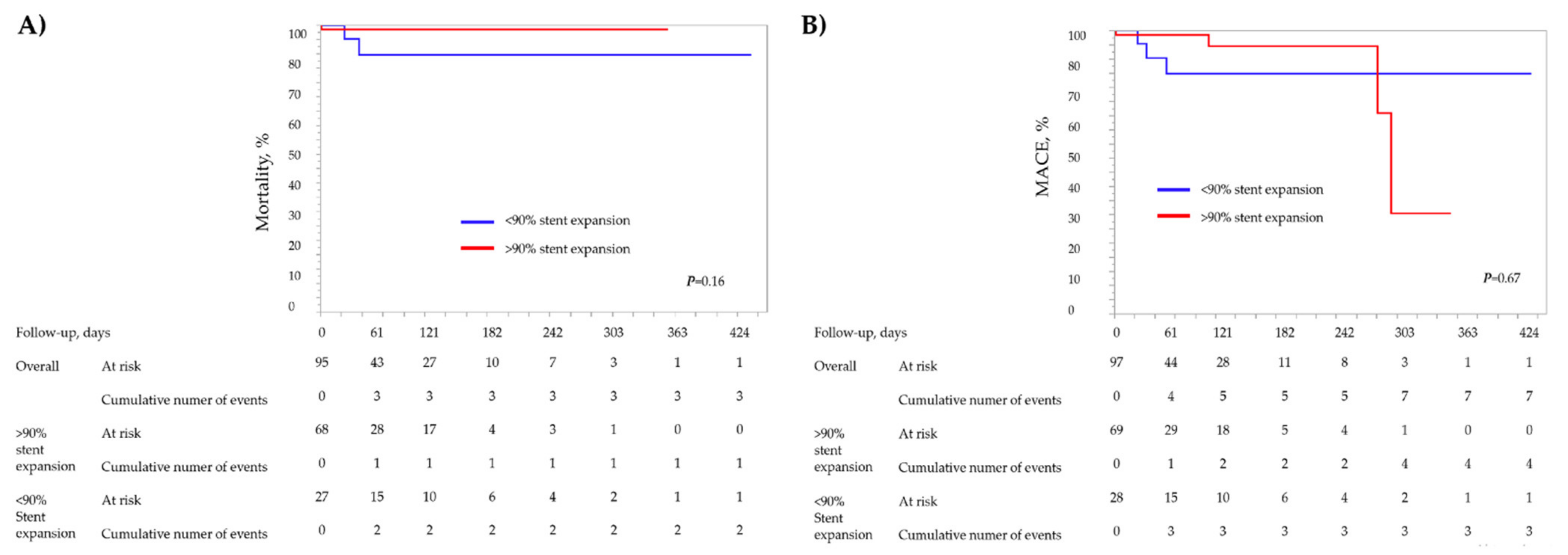
3.6. Clinical Outcomes
3.7. Predictors of Stent Underexpansion—Simple Linear Univariable Analysis
3.8. Predictors of Stent Underexpansion—Logistic Regression Univariable Analysis
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Prati, F.; Di Vito, L.; Biondi-Zoccai, G.; Occhipinti, M.; La Manna, A.; Tamburino, C.; Burzotta, F.; Trani, C.; Porto, I.; Ramazzotti, V.; et al. Angiography alone versus angiography plus optical coherence tomography to guide decision-making during percutaneous coronary intervention: The Centro per la Lotta contro l’Infarto-Optimisation of Percutaneous Coronary Intervention (CLI-OPCI) study. EuroIntervention 2012, 8, 823–829. [Google Scholar] [CrossRef] [PubMed]
- Prati, F.; Romagnoli, E.; Burzotta, F.; Limbruno, U.; Gatto, L.; La Manna, A.; Versaci, F.; Marco, V.; Di Vito, L.; Imola, F.; et al. Clinical impact of OCT findings during PCI: The CLI-OPCI II study. JACC Cardiovasc. Imaging 2015, 8, 1297–1305. [Google Scholar] [CrossRef] [PubMed]
- Wijns, W.; Shite, J.; Jones, M.R.; Lee, S.W.; Price, M.J.; Fabbiocchi, F.; Barbato, E.; Akasaka, T.; Bezerra, H.; Holmes, D. Optical coherence tomography imaging during percutaneous coronary intervention impacts physician decision-making: ILUMIEN I study. Eur. Heart J. 2015, 36, 3346–3355. [Google Scholar] [CrossRef] [PubMed]
- Ali, Z.A.; Galougahi, K.K.; Maehara, A.; Shlofmitz, R.A.; Fabbiocchi, F.; Guagliumi, G.; Alfonso, F.; Akasaka, T.; Matsumura, M.; Mintz, G.S.; et al. Outcomes of optical coherence tomography compared with intravascular ultrasound and with angiography to guide coronary stent implantation: One-year results from the ILUMIEN III: OPTIMIZE PCI trial. EuroIntervention 2021, 16, 1085–1091. [Google Scholar] [CrossRef] [PubMed]
- Ali, Z.A.; Maehara, A.; Généreux, P.; Shlofmitz, R.A.; Fabbiocchi, F.; Nazif, T.M.; Guagliumi, G.; Meraj, P.M.; Alfonso, F.; Samady, H.; et al. Optical coherence tomography compared with intravascular ultrasound and with angiography to guide coronary stent implantation (ILUMIEN III: OPTIMIZE PCI): A randomised controlled trial. Lancet 2016, 388, 2618–2628. [Google Scholar] [CrossRef]
- Ma, W.; Wang, Q.; Wang, B.; Wang, C.; Niu, X.; Zhang, D.; Liu, H.; Niu, X.; Liu, Y.; Guo, W.; et al. Novel predictors of stent under-expansion regarding calcified coronary lesions assessed by optical coherence tomography. Catheter. Cardiovasc. Interv. 2022, 99, 1473–1481. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, A.; Nakamura, D.; Shutta, R.; Nakamura, H.; Matsuhiro, Y.; Okamoto, N.; Egami, Y.; Sakata, Y.; Nishino, M.; Tanouchi, J. Clinical impact of a new optical coherence tomography-derived volumetric method for evaluating stent expansion. Int. J. Cardiovasc. Imaging 2021, 37, 1121–1129. [Google Scholar] [CrossRef] [PubMed]
- Miura, K.; Tada, T.; Habara, S.; Kuwayama, A.; Shimada, T.; Ohya, M.; Murai, R.; Amano, H.; Kubo, S.; Otsuru, S.; et al. Optical Coherence Tomography Predictors for Recurrent Restenosis After Paclitaxel-Coated Balloon Angioplasty for Drug-Eluting Stent Restenosis. Circ. J. 2018, 82, 2820–2828. [Google Scholar] [CrossRef] [PubMed]
- Matsuhiro, Y.; Nakamura, D.; Shutta, R.; Yanagawa, K.; Nakamura, H.; Okamoto, N.; Egami, Y.; Sakata, Y.; Nishino, M.; Tanouchi, J. Maximum calcium thickness is a useful predictor for acceptable stent expansion in moderate calcified lesions. Int. J. Cardiovasc. Imaging 2020, 36, 1609–1615. [Google Scholar] [CrossRef] [PubMed]
- Fujino, A.; Mintz, G.; Matsumura, M.; Yamamoto, M.H.; Lee, C.; Hoshino, M.; Usui, E.; Kanaji, Y.; Murai, T.; Yonetsu, T.; et al. TCT-28 a new optical coherence tomography-based calcium scoring system to predict stent underexpansion. J. Am. Coll. Cardiol. 2017, 70, B12–B13. [Google Scholar] [CrossRef]
- Shlofmitz, E.; Shlofmitz, R.A.; Galougahi, K.K.; Rahim, H.M.; Virmani, R.; Hill, J.M.; Matsumura, M.; Mintz, G.S.; Maehara, A.; Landmesser, U.; et al. Algorithmic Approach for Optical Coherence Tomography-Guided Stent Implantation During Percutaneous Coronary Intervention. Interv. Cardiol. Clin. 2018, 7, 329–344. [Google Scholar] [CrossRef] [PubMed]
- Januszek, R.; Siłka, W.; Sabatowski, K.; Malinowski, K.P.; Heba, G.; Surowiec, S.; Chyrchel, M.; Rzeszutko, Ł.; Bryniarski, L.; Surdacki, A.; et al. Procedure-Related Differences and Clinical Outcomes in Patients Treated with Percutaneous Coronary Intervention Assisted by Optical Coherence Tomography between New and Earlier Generation Software (Ultreon™ 1.0 Software vs. AptiVue™ Software). J. Cardiovasc. Dev. Dis. 2022, 9, 218. [Google Scholar] [CrossRef] [PubMed]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.M.; Capodanno, D. ESC National Cardiac Societies; ESC Scientific Document Group. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, Y.; Okura, H.; Kume, T.; Yamada, R.; Kobayashi, Y.; Fukuhara, K.; Koyama, T.; Nezuo, S.; Neishi, Y.; Hayashida, A.; et al. Impact of target lesion coronary calcification on stent expansion. Circ. J. 2014, 78, 2209–2214. [Google Scholar] [CrossRef] [PubMed]
- Fujii, K.; Carlier, S.G.; Mintz, G.S.; Yang, Y.M.; Moussa, I.; Weisz, G.; Dangas, G.; Mehran, R.; Lansky, A.J.; Kreps, E.M.; et al. Stent underexpansion and residual reference segment stenosis are related to stent thrombosis after sirolimus-eluting stent implantation: An intravascular ultrasound study. J. Am. Coll. Cardiol. 2005, 45, 995–998. [Google Scholar] [CrossRef] [PubMed]
- Sonoda, S.; Morino, Y.; Ako, J.; Terashima, M.; Hassan, A.H.; Bonneau, H.N.; Leon, M.B.; Moses, J.W.; Yock, P.G.; Honda, Y.; et al. Impact of final stent dimensions on long-term results following sirolimus-eluting stent implantation: Serial intravascular ultrasound analysis from the sirius trial. J. Am. Coll. Cardiol. 2004, 43, 1959–1963. [Google Scholar] [CrossRef] [PubMed]
- Fujii, K.; Mintz, G.S.; Kobayashi, Y.; Carlier, S.G.; Takebayashi, H.; Yasuda, T.; Moussa, I.; Dangas, G.; Mehran, R.; Lansky, A.J.; et al. Contribution of stent underexpansion to recurrence after sirolimus-eluting stent implantation for in-stent restenosis. Circulation 2004, 109, 1085–1088. [Google Scholar] [CrossRef] [PubMed]
- Ali, Z.A.; Brinton, T.J.; Hill, J.M.; Maehara, A.; Matsumura, M.; Karimi Galougahi, K.; Illindala, U.; Götberg, M.; Whitbourn, R.; Van Mieghem, N.; et al. Optical coherence tomography characterization of coronary lithoplasty for treatment of calcified lesions: First description. JACC Cardiovasc. Imaging 2017, 10, 897–906. [Google Scholar] [CrossRef] [PubMed]
- Guo, N.; Maehara, A.; Mintz, G.S.; He, Y.; Xu, K.; Wu, X.; Lansky, A.J.; Witzenbichler, B.; Guagliumi, G.; Brodie, B.; et al. Incidence, mechanisms, predictors, and clinical impact of acute and late stent malapposition after primary intervention in patients with acute myocardial infarction: An intravascular ultrasound sub-study of the Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction (HORIZONS-AMI) trial. Circulation 2010, 122, 1077–1084. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Total N = 100 | Stent Expansion <90% N = 29 | Stent Expansion ≥90% N = 71 | p-Value | |
|---|---|---|---|---|
| Age, years | 67.9 (62.3; 75.5) | 67.4 (62.3; 74.6) | 68.2 (62.4; 75.6) | 0.66 |
| Gender, male | 80 (80) | 26 (89.7) | 54 (76.1) | 0.1 |
| Euroscore II, % | 2.3 (1.2; 3.5) | 2.4 (1.4; 4.7) | 2.2 (1.2; 3.3) | 0.22 |
| STS score | 1.6 (0.8; 3) | 2.1 (0.9; 3.5) | 1.4 (0.7; 2.8) | 0.24 |
| Syntax I | 15.5 (8; 24) | 14 (8; 24.8) | 16 (9; 24) | 0.92 |
| Syntax II PCI 4-year mortality, % | 15.2 (6.8; 29.9) | 23.5 (8.7; 42.6) | 10.8 (5.9; 23.8) | 0.08 |
| Syntax II CABG 4-year mortality, % | 11 (4.8; 17.4) | 12.9 (5; 22.6) | 10.4 (4.8; 14.6) | 0.29 |
| Diabetes mellitus | 37 (37) | 10 (34.5) | 27 (38) | 0.74 |
| Hypercholesterolemia | 56 (56) | 17 (58.6) | 39 (54.9) | 0.68 |
| Arterial hypertension | 83 (83) | 25 (86.2) | 58 (81.7) | 0.58 |
| Kidney failure | 7 (7) | 2 (6.9) | 5 (7) | 0.98 |
| Dialysis therapy | 1 (1) | 1 (3.5) | 0 (0) | 0.11 |
| Prior PCI | 58 (58) | 19 (65.5) | 39 (65.9) | 0.33 |
| Prior CABG | 4 (4) | 1 (3.5) | 3 (4.2) | 0.86 |
| COPD/Bronchial asthma | 16 (16) | 7 (24.1) | 9 (12.7) | 0.17 |
| Smoking | 23 (23) | 8 (27.6) | 15 (21.1) | 0.61 |
| Family history of CVD | 11 (11) | 5 (17.2) | 6 (8.5) | 0.22 |
| Heart failure | 59 (59) | 18 (62.1) | 41 (57.8) | 0.69 |
| LVEF, % | 40 (20.5; 53.8) | 38 (20; 55.5) | 40 (23; 50) | 0.69 |
| Peripheral arterial disease | 14 (14) | 7 (24.1) | 7 (9.9) | 0.07 |
| Prior PTA | 2 (2) | 2 (6.9) | 0 (0) | 0.02 |
| Prior stroke | 7 (7) | 3 (10.3) | 4 (5.6) | 0.42 |
| Total N = 100 | Stent Expansion <90% N = 29 | Stent Expansion ≥90% N = 71 | p-Value | |
|---|---|---|---|---|
| Creatinine before PCI, µmol/L | 90.5 (73.9; 106) | 99.1 (83.1; 123) | 87.7 (72.1; 102) | 0.02 |
| Creatinine after PCI, µmol/L | 90.2 (78; 117) | 105 (82.9; 137) | 89.1 (77.7; 110.3) | 0.09 |
| GFR, mL/min. | 74 (60; 83) | 64 (52.5; 80) | 76 (64; 84) | 0.11 |
| PLT, × 103/µL | 235.5 (185; 310) | 246 (199; 346.5) | 227 (185; 295) | 0.22 |
| Hemoglobin before PCI, mg/dL | 13.7 ± 1.8 | 13.3 ± 1.7 | 13.9 ± 1.8 | 0.26 |
| Hemoglobin after PCI, mg/dL | 12.6 ± 2.2 | 12.6 ± 2.4 | 12.6 ± 2.1 | 0.89 |
| RBC, × 106/µL | 4.5 ± 0.6 | 4.4 ± 0.5 | 4.5 ± 0.6 | 0.67 |
| CRP, mg/dL | 10 (2.6; 19) | 8.9 (2.6; 17.8) | 10.3 (2.6; 20.4) | 0.94 |
| Total cholesterol, mmol/L | 3.8 (3.3; 4.8) | 3.7 (3.2; 4.7) | 3.9 (3.3.; 4.8) | 0.49 |
| LDL cholesterol, mmol/L | 2 (1.5; 2.6) | 1.8 (1.5; 2.6) | 2 (1.5; 2.7) | 0.45 |
| TGL, mmol/L | 1.4 (1; 1.8) | 1.3 (0.9; 1.7) | 1.4 (1.1.; 1.9) | 0.55 |
| HDL cholesterol, mmol/L | 1.1 (1; 1.3) | 1.2 (0.9; 1.4) | 1.1 (1; 1.3) | 0.63 |
| Maximal CK-Mb, IU/L | 22.5 (14.8; 46.3) | 20.5 (16; 25.3) | 22.5 (14; 48.8) | 0.6 |
| Maximal troponin T, pg/mL | 274 (65.1; 1307) | 246 (92.5; 829) | 274 (63.7; 1646) | 0.47 |
| NT-pro BNP, pg/mL | 786 (773; 3312) | 2636 (773; 5287) | 1673 (740; 3008) | 0.27 |
| Glucose, mmol/L | 6.2 (5.4; 8.3) | 8.3 (6; 9.4) | 6.1 (5.3; 7.5) | 0.14 |
| Total N = 100 | Stent Expansion <90% N = 29 | Stent Expansion ≥90% N = 71 | p-Value | |
|---|---|---|---|---|
| LMCA | 34 (34) | 6 (20.7) | 28 (39.4) | 0.07 |
| LAD | 78 (78) | 22 (75.9) | 56 (78.9) | 0.74 |
| Diagonal branch | 16 (16) | 7 (24.1) | 9 (12.7) | 0.17 |
| Circumflex branch | 33 (33) | 8 (27.6) | 25 (35.2) | 0.46 |
| Marginal branch | 6 (6) | 2 (6.9) | 4 (5.6) | 0.81 |
| Right coronary artery | 28 (28) | 7 (24.1) | 21 (29.6) | 0.58 |
| Chronic total occlusion | 10 (10) | 2 (6.9) | 8 (11.3) | 0.49 |
| PCI + stent | 97 (97) | 29 (100) | 68 (95.8) | 0.15 |
| Drug-eluting balloon | 3 (3) | 0 (0) | 3 (4.2) | 0.15 |
| Drug-eluting stent | 97 (97) | 29 (100) | 68 (95.8) | 0.15 |
| Bioresorbable scaffold | 0 (0) | 0 (0) | 0 (0) | - |
| Type of antimitotic agent: | ||||
| Ewerolimus | 87 (87) | 25 (86.2) | 62 (87.3) | 0.88 |
| Sirolimus | 13 (13) | 4 (13.8) | 9 (12.7) | 0.88 |
| Zotarolimus | 3 (3) | 1 (3.5) | 2 (2.8) | 0.87 |
| Number of stents | 2 (1; 3) | 2 (1; 2.5) | 2 (1; 3) | 0.87 |
| Number of stents | 0.31 | |||
| 0 | 3 (3) | 0 (0) | 3 (4.2) | |
| 1 | 26 (26) | 9 (31) | 17 (23.9) | |
| 2 | 43 (43) | 13 (44.8) | 30 (42.3) | |
| 3 | 14 (14) | 2 (6.9) | 12 (16.9) | |
| 4 | 11 (11) | 3 (10.3) | 8 (11.3) | |
| 5 | 3 (3) | 2 (6.9) | 1 (1.4) | |
| Overall stent length, mm | 56 (33; 76) | 50 (36; 63.5) | 56 (33; 76) | 0.39 |
| Maximal stent diameter, mm | 3.5 (3; 3.5) | 3.5 (3; 3.5) | 3.5 (3; 3.5) | 1 |
| Minimal stent diameter, mm | 3 (2.5; 3) | 2.8 (2.5; 3) | 3 (2.5; 3.4) | 0.16 |
| Maximal balloon diameter, mm | 4 (3.5; 5) | 3.6 (3.5; 4.5) | 4 (3.5; 5) | 0.26 |
| Maximal balloon pressure, atm. | 20 (18; 24) | 22 (18; 25) | 20 (18; 24) | 0.76 |
| Rotablation | 27 (27) | 10 (34.5) | 17 (23.9) | 0.29 |
| IVL | 12 (12) | 2 (6.9) | 10 (14.1) | 0.29 |
| Impella pump | 35 (35) | 13 (44.8) | 22 (31) | 0.19 |
| IABP | 3 (3) | 0 (0) | 3 (4.2) | 0.15 |
| Total N = 100 | Stent Expansion <90% N = 29 | Stent Expansion ≥90% N = 71 | p-Value | |
|---|---|---|---|---|
| Before PCI | ||||
| Type of plaque | 0.56 | |||
| - lipidic | 10 (10) | 2 (6.9) | 8 (11.3) | |
| - fibrotic | 13 (13) | 3 (10.3) | 10 (14.1) | |
| - mild/moderate calcium | 26 (26) | 6 (20.7) | 20 (28.2) | |
| - severe calcium | 51 (51) | 18 (62.1) | 33 (46.5) | |
| Maximum calcium angle, ° | 189 (93; 299) | 230 (122; 299) | 181 (0; 300.3) | 0.41 |
| Maximal calcium thickness, mm | 1.1 (0.6; 1.4) | 1.1 (0.7 ± 1.4) | 1.1 (0; 1.4) | 0.71 |
| Total calcium length, mm | 5 (2; 20) | 8 (3; 20) | 4 (0; 20) | 0.28 |
| Minimal lumen diameter, mm | 1.4 (1.2; 1.7) | 1.4 (1.1; 1.6) | 1.4 (1.3; 1.8) | 0.43 |
| Distal EEL reference diameter, mm | 3.3 ± 0.7 | 3.3 ± 0.7 | 3.3 ± 0.7 | 1 |
| Distal EEL reference to minimum stent diameter ratio | 1.1 (1; 1.2) | 1.1 (1; 1.2) | 1.1 (1; 1.2) | 0.71 |
| Distal lumen diameter, mm | 2.3 (1.9; 2.9) | 2.4 (1.9; 2.8) | 2.3 (1.9; 2.9) | 0.91 |
| Distal lumen to minimum stent diameter ratio | 0.8 (0.7; 0.9) | 0.8 (0.7; 0.9) | 0.8 (0.7; 0.9) | 0.41 |
| After PCI | ||||
| Medial dissection | 7 (7) | 1 (3.5) | 6 (8.5) | 0.34 |
| Malapposition | 3 (3) | 2 (6.9) | 1 (1.4) | 0.17 |
| Minimum stent expansion, % | 95 (87.3; 104) | 82 (75.5; 85.5) | 101 (94; 112) | <0.001 |
| Minimal lumen diameter, mm | 2.6 (2.3; 3) | 2.5 (2.1; 2.9) | 2.7 (2.3; 3.1) | 0.19 |
| Minimal lumen to minimum stent diameter ratio | 0.9 (0.8; 1) | 0.9 (0.8; 1) | 0.9 (0.8; 1) | 0.34 |
| Total N = 100 | Stent Expansion <90% N = 29 | Stent Expansion ≥90% N = 71 | p-Value | |
|---|---|---|---|---|
| Acetyl-salicylic acid | 96 (96) | 28 (96.6) | 68 (95.8) | 0.86 |
| P2Y12 inhibitor | ||||
| - clopidogrel | 49 (49) | 14 (48.3) | 35 (49.3) | 0.93 |
| - prasugrel | 13 (13) | 2 (6.9) | 11 (15.5) | 0.22 |
| - ticagrelor | 37 (37) | 13 (44.8) | 24 (33.8) | 0.30 |
| Antithrombotic treatment(heparins, old and new oral anticoagulants) | 17 (17) | 4 (13.8) | 13 (18.3) | 0.58 |
| Lipid-lowering treatment | ||||
| - statin | 95 (95) | 28 (96.6) | 67 (94.4) | 0.64 |
| - fibrate | 2 (2) | 1 (3.5) | 1 (1.4) | 0.53 |
| - ezetimibe | 12 (12) | 3 (10.3) | 9 (12.7) | 0.74 |
| Insulin therapy | 18 (18) | 6 (20.7) | 12 (16.9) | 0.66 |
| Oral anti-diabetic therapy | 30 (30) | 6 (20.7) | 24 (33.8) | 0.18 |
| Angiotensin converting enzyme inhibitors | 80 (80) | 24 (82.8) | 56 (78.9) | 0.66 |
| Calcium channel blockers | 21 (21) | 9 (31) | 12 (16.9) | 0.13 |
| Beta blocker | 86 (86) | 25 (86.2) | 61 (85.9) | 0.97 |
| Inhalators (bronchodilators/GCSs) | 11 (11) | 6 (20.7) | 5 (7) | 0.06 |
| Total N = 100 | Stent Expansion <90% N = 29 | Stent Expansion ≥90% N = 71 | p-Value | |
|---|---|---|---|---|
| Completed follow-up | 99 (99) | 29 (100) | 70 (98.6) | 0.41 |
| TLR | 1 (1) | 0 (0) | 1 (1.5) | 0.41 |
| TVR | 1 (1) | 0 (0) | 1 (1.5) | 0.41 |
| Myocardial infarction | 1 (1) | 1 (3.6) | 0 (0) | 0.11 |
| Stroke | 2 (2) | 0 (0) | 2 (2.9) | 0.24 |
| Re-PCI | 3 (3) | 2 (7.1) | 1 (1.5) | 0.17 |
| CABG | 0 (0) | 0 (0) | 0 (0) | - |
| DOCE | 5 (5.1) | 2 (7.1) | 3 (4.3) | 0.57 |
| Cardiac death | 4 (4) | 2 (7.1) | 2 (2.9) | 0.36 |
| TV-MI | 0 (0) | 0 (0) | 0 (0) | - |
| MACE | 10 (10) | 4 (13.8) | 6 (8.5) | 0.43 |
| Death overall | 6 (6) | 3 (10.3) | 3 (4.2) | 0.26 |
| Mean follow-up duration, days | 42 (22; 136.3) | 65 (23; 177) | 41 (20; 126) | 0.24 |
| Variable | Estimate | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Hypercholesterolemia, 1 vs. 0 | −28.16 | −40.34–(−15.98) | <0.01 |
| COPD/Bronchial asthma, 0 vs. 1 | 6.19 | 1.05–11.34 | 0.02 |
| Familiar history of CVD, 0 vs. 1 | 6.24 | 0.16–12.31 | 0.04 |
| PCI within LMCA, 0 vs. 1 | −4.45 | −8.45–(−0.45) | 0.03 |
| Stent implantation, 0 vs. 1 | 11.7 | 0.56–22.84 | 0.04 |
| PCI with DEB, 0 vs. 1 | −11.7 | −22.84–(−0.56) | 0.04 |
| Stent type, DES, 0 vs. 1 | 11.7 | 0.56–22.84 | 0.04 |
| Paclitaxel antimitotic agent vs. other | −40.25 | −58.02–(−22.49) | <0.001 |
| Inhalators, 0 vs. 1 | 6.64 | 0.58–12.7 | 0.03 |
| Euroscore II, % | 1.41 | 0.04–2.77 | 0.04 |
| Maximal stent diameter, mm | −1.24 | −2.41–(−0.06) | 0.04 |
| Variable | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Creatinine before PCI | 0.97 | 0.95–0.99 | 0.01 |
| Creatinine after PCI | 0.98 | 0.96–0.99 | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bartuś, S.; Siłka, W.; Kasprzycki, K.; Sabatowski, K.; Malinowski, K.P.; Rzeszutko, Ł.; Chyrchel, M.; Bryniarski, L.; Surdacki, A.; Bartuś, K.; et al. Experience with Optical Coherence Tomography Enhanced by a Novel Software (Ultreon™ 1.0 Software)—The First One Hundred Cases. Medicina 2022, 58, 1227. https://doi.org/10.3390/medicina58091227
Bartuś S, Siłka W, Kasprzycki K, Sabatowski K, Malinowski KP, Rzeszutko Ł, Chyrchel M, Bryniarski L, Surdacki A, Bartuś K, et al. Experience with Optical Coherence Tomography Enhanced by a Novel Software (Ultreon™ 1.0 Software)—The First One Hundred Cases. Medicina. 2022; 58(9):1227. https://doi.org/10.3390/medicina58091227
Chicago/Turabian StyleBartuś, Stanisław, Wojciech Siłka, Karol Kasprzycki, Karol Sabatowski, Krzysztof Piotr Malinowski, Łukasz Rzeszutko, Michał Chyrchel, Leszek Bryniarski, Andrzej Surdacki, Krzysztof Bartuś, and et al. 2022. "Experience with Optical Coherence Tomography Enhanced by a Novel Software (Ultreon™ 1.0 Software)—The First One Hundred Cases" Medicina 58, no. 9: 1227. https://doi.org/10.3390/medicina58091227