
Prognostic Effect of Underlying Chronic Kidney Disease and Renal Replacement Therapy on the Outcome of Patients after Out-of-Hospital Cardiac Arrest: A Nationwide Observational Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
2.2. Data Source
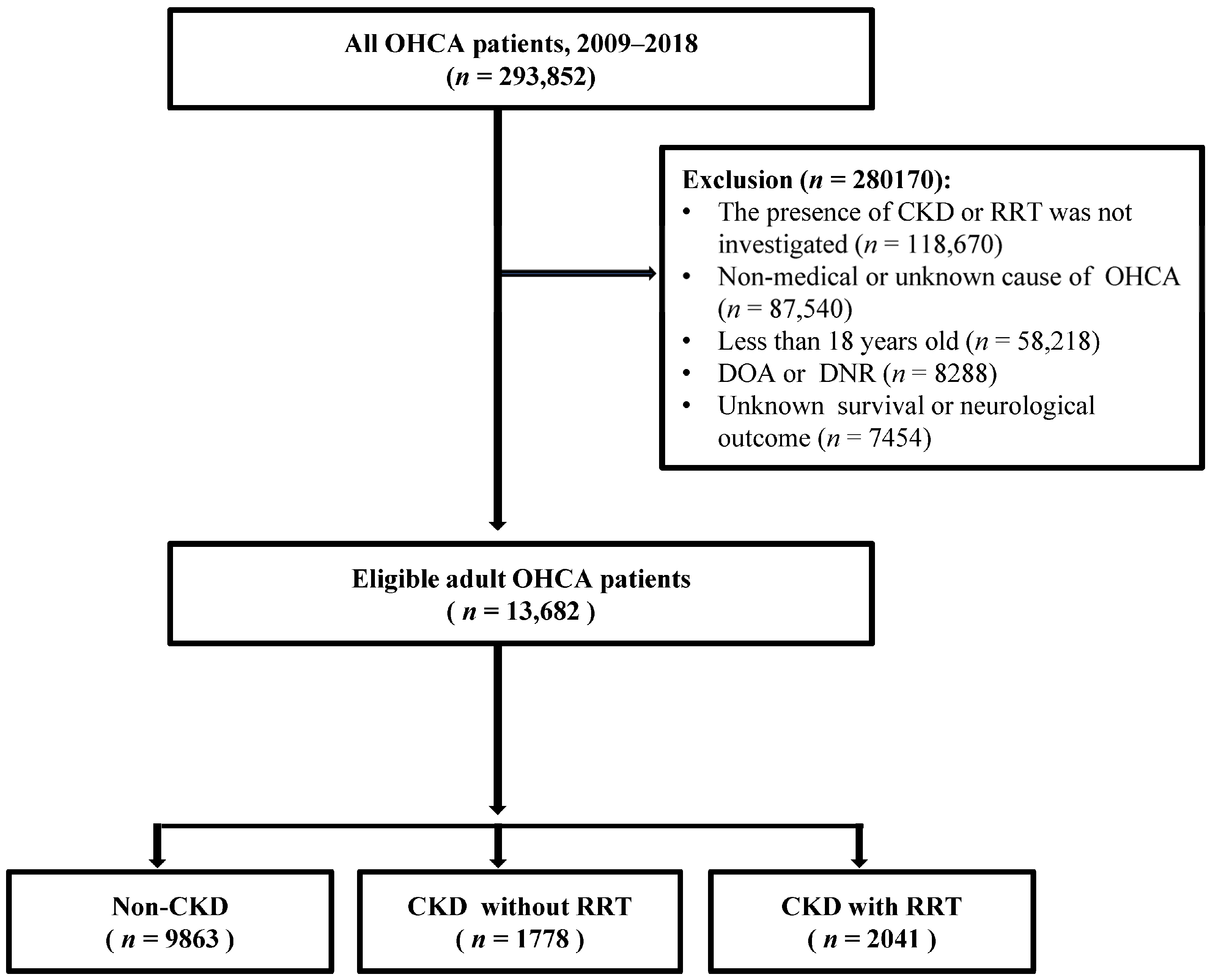
2.3. Study Population
2.4. Variables
2.5. Outcome Measures
2.6. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Outcomes Analysis
3.3. Multivariate Logistic Analysis of Survival at Hospital Discharge and Good Neurological Outcomes in the Three Patient Groups
3.4. Subgroup Analysis for Survival at Hospital Discharge and Good Neurological Outcomes According to the Existence of Diabetes Mellitus Using a Multivariate Logistic Analysis
3.5. Propensity Score-Matched Analysis of Survival at Hospital Discharge and Good Neurological Outcomes in the Three Patient Groups
3.6. Outcome Analysis
3.7. Multivariate Logistic Analysis of Survival at Hospital Discharge and Good Neurological Outcomes in the Three Patient Groups after Propensity Score Matching
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roberts, P.R.; Zachariah, D.; Morgan, J.M.; Yue, A.M.; Greenwood, E.F.; Phillips, P.C.; Kalra, P.A.; Green, D.; Lewis, R.J.; Kalra, P.R. Monitoring of arrhythmia and sudden death in a hemodialysis population: The CRASH-ILR Study. PLoS ONE 2017, 12, e0188713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obremska, M.; Madziarska, K.; Zyśko, D.; Ładny, J.R.; Gałązkowski, R.; Gąsior, M.; Nadolny, K. Out-of-hospital cardiac arrest in dialysis patients. Int. Urol. Nephrol. 2021, 53, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Makar, M.S.; Pun, P.H. Sudden Cardiac Death among Hemodialysis Patients. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2017, 69, 684–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, T.K.; Arya, V.; Navaratnarajah, N. Chronic kidney disease and cardiovascular disease: A focus on primary care. Cardiovasc. Hematol. Disord. Drug Targets 2014, 14, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Emrich, I.E.; Zawada, A.M.; Martens-Lobenhoffer, J.; Fliser, D.; Wagenpfeil, S.; Heine, G.H.; Bode-Böger, S.M. Symmetric dimethylarginine (SDMA) outperforms asymmetric dimethylarginine (ADMA) and other methylarginines as predictor of renal and cardiovascular outcome in non-dialysis chronic kidney disease. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2018, 107, 201–213. [Google Scholar] [CrossRef] [PubMed]
- Green, D.; Roberts, P.R.; New, D.I.; Kalra, P.A. Sudden cardiac death in hemodialysis patients: An in-depth review. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2011, 57, 921–929. [Google Scholar] [CrossRef] [PubMed]
- Rigopoulos, A.G.; Daci, S.; Pfeiffer, B.; Papadopoulou, K.; Neugebauer, A.; Seggewiss, H. Low occurrence of ventricular arrhythmias after alcohol septal ablation in high-risk patients with hypertrophic obstructive cardiomyopathy. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2016, 105, 953–961. [Google Scholar] [CrossRef] [PubMed]
- Sedaghat-Hamedani, F.; Kayvanpour, E.; Tugrul, O.F.; Lai, A.; Amr, A.; Haas, J.; Proctor, T.; Ehlermann, P.; Jensen, K.; Katus, H.A.; et al. Clinical outcomes associated with sarcomere mutations in hypertrophic cardiomyopathy: A meta-analysis on 7675 individuals. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2018, 107, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Haider, A.W.; Larson, M.G.; Benjamin, E.J.; Levy, D. Increased left ventricular mass and hypertrophy are associated with increased risk for sudden death. J. Am. Coll. Cardiol. 1998, 32, 1454–1459. [Google Scholar] [CrossRef] [Green Version]
- Franczyk-Skóra, B.; Gluba-Brzózka, A.; Wranicz, J.K.; Banach, M.; Olszewski, R.; Rysz, J. Sudden cardiac death in CKD patients. Int. Urol. Nephrol. 2015, 47, 971–982. [Google Scholar] [CrossRef]
- Burghardt, A.; van Buuren, F.; Dimitriadis, Z.; Grübbel, T.; Seggewiss, H.; Scholtz, S.; Horstkotte, D.; Faber, L. Risk marker profiles in patients treated with percutaneous septal ablation for symptomatic hypertrophic obstructive cardiomyopathy. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2018, 107, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Bleyer, A.J.; Hartman, J.; Brannon, P.C.; Reeves-Daniel, A.; Satko, S.G.; Russell, G. Characteristics of sudden death in hemodialysis patients. Kidney Int. 2006, 69, 2268–2273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weidner, K.; Behnes, M.; Schupp, T.; Rusnak, J.; Reiser, L.; Taton, G.; Reichelt, T.; Ellguth, D.; Engelke, N.; Bollow, A.; et al. Prognostic impact of chronic kidney disease and renal replacement therapy in ventricular tachyarrhythmias and aborted cardiac arrest. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2019, 108, 669–682. [Google Scholar] [CrossRef] [PubMed]
- Wetmore, J.B.; Gilbertson, D.T.; Liu, J.; Collins, A.J. Improving Outcomes in Patients Receiving Dialysis: The Peer Kidney Care Initiative. Clin. J. Am. Soc. Nephrol. CJASN 2016, 11, 1297–1304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genovesi, S.; Boriani, G.; Covic, A.; Vernooij, R.W.M.; Combe, C.; Burlacu, A.; Davenport, A.; Kanbay, M.; Kirmizis, D.; Schneditz, D.; et al. Sudden cardiac death in dialysis patients: Different causes and management strategies. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.-Eur. Ren. Assoc. 2021, 36, 396–405. [Google Scholar] [CrossRef] [Green Version]
- Flythe, J.E.; Assimon, M.M.; Tugman, M.J.; Chang, E.H.; Gupta, S.; Shah, J.; Sosa, M.A.; Renaghan, A.D.; Melamed, M.L.; Wilson, F.P.; et al. Characteristics and Outcomes of Individuals With Pre-existing Kidney Disease and COVID-19 Admitted to Intensive Care Units in the United States. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2021, 77, 190–203.e191. [Google Scholar] [CrossRef]
- Daya, M.R.; Schmicker, R.H.; Zive, D.M.; Rea, T.D.; Nichol, G.; Buick, J.E.; Brooks, S.; Christenson, J.; MacPhee, R.; Craig, A.; et al. Out-of-hospital cardiac arrest survival improving over time: Results from the Resuscitation Outcomes Consortium (ROC). Resuscitation 2015, 91, 108–115. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, I.; Nadkarni, V.; Bahr, J.; Berg, R.A.; Billi, J.E.; Bossaert, L.; Cassan, P.; Coovadia, A.; D’Este, K.; Finn, J.; et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: Update and simplification of the Utstein templates for resuscitation registries. A statement for healthcare professionals from a task force of the international liaison committee on resuscitation (American Heart Association, European Resuscitation Council, Australian Resuscitation Council, New Zealand Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Southern Africa). Resuscitation 2004, 63, 233–249. [Google Scholar] [CrossRef]
- Donnino, M.W.; Andersen, L.W.; Berg, K.M.; Reynolds, J.C.; Nolan, J.P.; Morley, P.T.; Lang, E.; Cocchi, M.N.; Xanthos, T.; Callaway, C.W.; et al. Temperature Management After Cardiac Arrest: An Advisory Statement by the Advanced Life Support Task Force of the International Liaison Committee on Resuscitation and the American Heart Association Emergency Cardiovascular Care Committee and the Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Resuscitation 2016, 98, 97–104. [Google Scholar] [CrossRef]
- Neumar, R.W.; Otto, C.W.; Link, M.S.; Kronick, S.L.; Shuster, M.; Callaway, C.W.; Kudenchuk, P.J.; Ornato, J.P.; McNally, B.; Silvers, S.M.; et al. Part 8: Adult advanced cardiovascular life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2010, 122, S729–S767. [Google Scholar] [CrossRef] [Green Version]
- Sherif, K.A.; Abo-Salem, E.; Panikkath, R.; Nusrat, M.; Tuncel, M. Cardiac repolarization abnormalities among patients with various stages of chronic kidney disease. Clin. Cardiol. 2014, 37, 417–421. [Google Scholar] [CrossRef]
- Chan, C.T.; Levin, N.W.; Chertow, G.M.; Larive, B.; Schulman, G.; Kotanko, P. Determinants of cardiac autonomic dysfunction in ESRD. Clin. J. Am. Soc. Nephrol. CJASN 2010, 5, 1821–1827. [Google Scholar] [CrossRef] [Green Version]
- Dinshaw, L.; Münch, J.; Dickow, J.; Lezius, S.; Willems, S.; Hoffmann, B.A.; Patten, M. The T-peak-to-T-end interval: A novel ECG marker for ventricular arrhythmia and appropriate ICD therapy in patients with hypertrophic cardiomyopathy. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2018, 107, 130–137. [Google Scholar] [CrossRef]
- Pereira, R.; Campuzano, O.; Sarquella-Brugada, G.; Cesar, S.; Iglesias, A.; Brugada, J.; Cruz Filho, F.E.S.; Brugada, R. Short QT syndrome in pediatrics. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2017, 106, 393–400. [Google Scholar] [CrossRef]
- Storm, C.; Krannich, A.; Schachtner, T.; Engels, M.; Schindler, R.; Kahl, A.; Otto, N.M. Impact of acute kidney injury on neurological outcome and long-term survival after cardiac arrest—A 10 year observational follow up. J. Crit. Care 2018, 47, 254–259. [Google Scholar] [CrossRef]
- Lu, R.; Kiernan, M.C.; Murray, A.; Rosner, M.H.; Ronco, C. Kidney-brain crosstalk in the acute and chronic setting. Nat. Rev. Nephrol. 2015, 11, 707–719. [Google Scholar] [CrossRef]
- Kang, D.H.; Kanellis, J.; Hugo, C.; Truong, L.; Anderson, S.; Kerjaschki, D.; Schreiner, G.F.; Johnson, R.J. Role of the microvascular endothelium in progressive renal disease. J. Am. Soc. Nephrol. JASN 2002, 13, 806–816. [Google Scholar] [CrossRef]
- Xiong, Y.; Zhan, H.; Lu, Y.; Guan, K.; Okoro, N.; Mitchell, D.; Dwyer, M.; Leatham, A.; Salazar, G.; Liao, X.; et al. Out-of-hospital cardiac arrest without return of spontaneous circulation in the field: Who are the survivors? Resuscitation 2017, 112, 28–33. [Google Scholar] [CrossRef]
- Kitamura, T.; Iwami, T.; Kawamura, T.; Nitta, M.; Nagao, K.; Nonogi, H.; Yonemoto, N.; Kimura, T. Nationwide improvements in survival from out-of-hospital cardiac arrest in Japan. Circulation 2012, 126, 2834–2843. [Google Scholar] [CrossRef] [Green Version]
- Wolbinski, M.; Swain, A.H.; Harding, S.A.; Larsen, P.D. Out-of-hospital Cardiac Arrest Patient Characteristics: Comparing ventricular arrhythmia and Pulseless Electrical Activity. Heart Lung Circ. 2016, 25, 639–644. [Google Scholar] [CrossRef] [Green Version]
- Na, M.K.; Kim, W.; Lim, T.H.; Jang, B.; Cho, Y.; Choi, K.S.; Shin, H.G.; Ahn, C.; Lee, J.; Kim, J.G. Gray matter to white matter ratio for predicting neurological outcomes in patients treated with target temperature management after cardiac arrest: A systematic review and meta-analysis. Resuscitation 2018, 132, 21–28. [Google Scholar] [CrossRef]
- Kim, M.W.; Park, J.H.; Ro, Y.S.; Shin, S.D.; Song, K.J.; Hong, K.J.; Jeong, J.; Kim, T.H.; Hong, W.P. End stage renal disease modifies the effect of targeted temperature management after out-of-hospital cardiac arrest. Am. J. Emerg. Med. 2020, 38, 2283–2290. [Google Scholar] [CrossRef]
- Hsieh, M.J.; Chen, Y.C.; Chen, C.C.; Wang, C.L.; Wu, L.S.; Wang, C.C. Renal dysfunction on admission, worsening renal function, and severity of acute kidney injury predict 2-year mortality in patients with acute myocardial infarction. Circ. J. Off. J. Jpn. Circ. Soc. 2013, 77, 217–223. [Google Scholar] [CrossRef] [Green Version]
- Shlipak, M.G.; Katz, R.; Kestenbaum, B.; Siscovick, D.; Fried, L.; Newman, A.; Rifkin, D.; Sarnak, M.J. Rapid decline of kidney function increases cardiovascular risk in the elderly. J. Am. Soc. Nephrol. JASN 2009, 20, 2625–2630. [Google Scholar] [CrossRef]
- Tamura, T.; Suzuki, M.; Hayashida, K.; Sasaki, J.; Yonemoto, N.; Sakurai, A.; Tahara, Y.; Nagao, K.; Yaguchi, A.; Morimura, N. Renal Function and Outcome of Out-of-Hospital Cardiac Arrest—Multicenter Prospective Study (SOS-KANTO 2012 Study). Circ. J. Off. J. Jpn. Circ. Soc. 2018, 83, 139–146. [Google Scholar] [CrossRef] [Green Version]
- Engdahl, J.; Holmberg, M.; Karlson, B.W.; Luepker, R.; Herlitz, J. The epidemiology of out-of-hospital ‘sudden’ cardiac arrest. Resuscitation 2002, 52, 235–245. [Google Scholar] [CrossRef]
- Spaulding, C.M.; Joly, L.M.; Rosenberg, A.; Monchi, M.; Weber, S.N.; Dhainaut, J.F.; Carli, P. Immediate coronary angiography in survivors of out-of-hospital cardiac arrest. N. Engl. J. Med. 1997, 336, 1629–1633. [Google Scholar] [CrossRef]
- Dumas, F.; Cariou, A.; Manzo-Silberman, S.; Grimaldi, D.; Vivien, B.; Rosencher, J.; Empana, J.P.; Carli, P.; Mira, J.P.; Jouven, X.; et al. Immediate percutaneous coronary intervention is associated with better survival after out-of-hospital cardiac arrest: Insights from the PROCAT (Parisian Region Out of hospital Cardiac ArresT) registry. Circ. Cardiovasc. Interv. 2010, 3, 200–207. [Google Scholar] [CrossRef] [Green Version]
- Bray, J.E.; Stub, D.; Bernard, S.; Smith, K. Exploring gender differences and the “oestrogen effect” in an Australian out-of-hospital cardiac arrest population. Resuscitation 2013, 84, 957–963. [Google Scholar] [CrossRef]
- Al-Dury, N.; Rawshani, A.; Israelsson, J.; Strömsöe, A.; Aune, S.; Agerström, J.; Karlsson, T.; Ravn-Fischer, A.; Herlitz, J. Characteristics and outcome among 14,933 adult cases of in-hospital cardiac arrest: A nationwide study with the emphasis on gender and age. Am. J. Emerg. Med. 2017, 35, 1839–1844. [Google Scholar] [CrossRef]
- Israelsson, J.; Bremer, A.; Herlitz, J.; Axelsson, Å.B.; Cronberg, T.; Djärv, T.; Kristofferzon, M.-L.; Larsson, I.-M.; Lilja, G.; Sunnerhagen, K.S.; et al. Health status and psychological distress among in-hospital cardiac arrest survivors in relation to gender. Resuscitation 2017, 114, 27–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tseng, Z.H.; Ramakrishna, S.; Salazar, J.W.; Vittinghoff, E.; Olgin, J.E.; Moffatt, E. Sex and Racial Differences in Autopsy-Defined Causes of Presumed Sudden Cardiac Death. Circ. Arrhythm. Electrophysiol. 2021, 14, e009393. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Total | Non-CKD | CKD without RRT | CKD with RRT | p-Value |
|---|---|---|---|---|---|
| (n = 13682) | (n = 9863) | (n = 1778) | (n = 2041) | ||
| Sex, n (%) Male | 9377 (68.5%) | 7037 (71.3%) | 1077 (60.6%) | 1263 (61.9%) | <0.01 |
| Age, years (IQR) | 64 (52–76) | 61 (49–75) | 75 (66–81) | 66 (57–74) | <0.01 |
| Location of CA | <0.01 | ||||
| Residential CA | 7414 (54.2%) | 5152 (52.2%) | 1106 (62.2%) | 1156 (56.6%) | |
| Non-residential CA | 6268 (45.8%) | 4711 (47.8%) | 672 (37.8%) | 885 (43.4%) | |
| Witnessed CA | 8426 (61.6%) | 6167 (62.5%) | 1033 (58.1%) | 1226 (60.1%) | <0.01 |
| Bystander CPR | 3684 (26.9%) | 2936 (29.8%) | 383 (21.5%) | 365 (17.9%) | <0.01 |
| Bystander AED use | 39 (0.3%) | 33 (0.3%) | 1 (0.1%) | 5 (0.2%) | <0.01 |
| Cause of CA | <0.01 | ||||
| Cardiac origin | 12723 (93.0%) | 9128 (92.5%) | 1702 (95.7%) | 1893 (92.7%) | |
| Non-cardiac origin | 959 (7.0%) | 735 (7.5%) | 76 (4.3%) | 148 (7.3%) | |
| Initial cardiac rhythm Shockable | <0.01 | ||||
| 2814 (20.6%) | 2470 (25.1%) | 148 (8.3%) | 196 (9.6%) | ||
| Non-shockable | 10,868 (79.4%) | 7393 (74.9%) | 1630 (91.7%) | 1845 (90.4%) | |
| Prehospital ROSC | 2075 (15.2%) | 1817 (18.4%) | 105 (5.9%) | 153 (7.5%) | <0.01 |
| Underlying disease | |||||
| DM | 3158 (23.1%) | 878 (8.9%) | 1050 (59.1%) | 1230 (60.3%) | <0.01 |
| HTN | 4411 (32.2%) | 2028 (20.6%) | 1115 (62.7%) | 1268 (62.1%) | <0.01 |
| Dyslipidemia | 320 (2.3%) | 195 (2.0%) | 83 (4.7%) | 42 (2.1%) | <0.01 |
| Heart disease | 1907 (13.9%) | 603 (6.1%) | 672 (37.8%) | 632 (31.0%) | <0.01 |
| Respiratory disease | 534 (3.9%) | 285 (2.9%) | 149 (8.4%) | 100 (4.9%) | <0.01 |
| Stroke | 658 (4.8%) | 256 (2.6%) | 218 (12.3%) | 184 (9.0%) | <0.01 |
| Post-CA care | |||||
| PCI | 1097 (8.0%) | 979 (9.9%) | 55 (3.1%) | 63 (3.1%) | <0.01 |
| TTM | 1017 (7.4%) | 824 (8.4%) | 69 (3.9%) | 124 (6.1%) | <0.01 |
| Outcomes at hospital discharge | |||||
| Survival | 2051 (15.0%) | 1825 (18.5%) | 91 (5.1%) | 135 (6.6%) | <0.01 |
| Good neurological outcome | 1894 (13.8%) | 1711 (17.3%) | 73 (4.1%) | 110 (5.4%) | <0.01 |
| Outcome | Groups | Reference = Non-CKD | Reference = CKD without RRT | ||||||
|---|---|---|---|---|---|---|---|---|---|
| AOR | 95% CI | p-Value | AOR | 95% CI | p-Value | ||||
| Survival at hospital discharge * | Non-CKD | 1.00 | 1.01 | 0.71 | 1.44 | 0.93 | |||
| CKD without RRT | 0.98 | 0.69 | 1.40 | 0.93 | 1.00 | ||||
| CKD with RRT | 0.94 | 0.69 | 1.28 | 0.73 | 0.96 | 0.66 | 1.40 | 0.84 | |
| Good neurological outcome * | Non-CKD | 1.00 | 1.79 | 1.24 | 2.58 | <0.01 | |||
| CKD without RRT | 0.55 | 0.38 | 0.80 | <0.01 | 1.00 | ||||
| CKD with RRT | 0.59 | 0.43 | 0.81 | <0.01 | 1.06 | 0.71 | 1.59 | 0.74 | |
| Outcome | Groups | Reference = Non-CKD | Reference = CKD without RRT | ||||||
|---|---|---|---|---|---|---|---|---|---|
| AOR | 95% CI | p-Value | AOR | 95% CI | p-Value | ||||
| Patients with DM | |||||||||
| Survival at hospital discharge * | Non-CKD | 1.00 | 0.88 | 0.55 | 1.42 | 0.61 | |||
| CKD without RRT | 1.12 | 0.70 | 1.82 | 0.61 | 1.00 | ||||
| CKD with RRT | 1.03 | 0.67 | 1.58 | 0.89 | 0.91 | 0.59 | 1.40 | 0.67 | |
| Good neurological outcome * | Non-CKD | 1.00 | 1.57 | 0.95 | 2.59 | 0.07 | |||
| CKD without RRT | 0.63 | 0.38 | 1.04 | 0.07 | 1.00 | ||||
| CKD with RRT | 0.67 | 0.43 | 1.04 | 0.07 | 1.06 | 0.66 | 1.71 | 0.78 | |
| Patients without DM | |||||||||
| Survival at hospital discharge * | Non-CKD | 1.00 | 1.47 | 0.84 | 2.58 | 0.17 | |||
| CKD without RRT | 0.67 | 0.38 | 1.18 | 0.17 | 1.00 | ||||
| CKD with RRT | 0.68 | 0.42 | 1.09 | 0.11 | 1.01 | 0.51 | 2.00 | 0.96 | |
| Good neurological outcome * | Non-CKD | 2.17 | 1.26 | 3.73 | <0.01 | ||||
| CKD without RRT | 0.46 | 0.26 | 0.78 | <0.01 | 1.00 | ||||
| CKD with RRT | 0.42 | 0.25 | 0.68 | <0.01 | 0.91 | 0.46 | 1.80 | 0.80 | |
| Outcomes | Groups | Non-CKD (Ref.) vs. CKD without RRT (Test) | Non-CKD (Ref.) vs. CKD with RRT (Test) | CKD without RRT (Ref.) vs. CKD with RRT (Test) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| AOR | 95% CI | p-Value | AOR | 95% CI | p-Value | AOR | 95% CI | p-Value | ||
| Survival at hospital discharge * | Ref. | 1.00 | 1.00 | 1.00 | ||||||
| Test | 0.91 | 0.58–1.41 | 0.67 | 0.87 | 0.61–1.24 | 0.46 | 1.07 | 0.73–1.59 | 0.70 | |
| Good neurological outcome * | Ref. | 1.00 | 1.00 | 1.00 | ||||||
| Test | 0.45 | 0.27–0.75 | <0.01 | 0.53 | 0.36–0.79 | <0.01 | 1.16 | 0.74–1.81 | 0.50 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, W.; Kim, J.-G.; Kang, G.-H.; Jang, Y.-S.; Kim, W.; Choi, H.-Y.; Lee, Y. Prognostic Effect of Underlying Chronic Kidney Disease and Renal Replacement Therapy on the Outcome of Patients after Out-of-Hospital Cardiac Arrest: A Nationwide Observational Study. Medicina 2022, 58, 444. https://doi.org/10.3390/medicina58030444
Yang W, Kim J-G, Kang G-H, Jang Y-S, Kim W, Choi H-Y, Lee Y. Prognostic Effect of Underlying Chronic Kidney Disease and Renal Replacement Therapy on the Outcome of Patients after Out-of-Hospital Cardiac Arrest: A Nationwide Observational Study. Medicina. 2022; 58(3):444. https://doi.org/10.3390/medicina58030444
Chicago/Turabian StyleYang, Won, Jae-Guk Kim, Gu-Hyun Kang, Yong-Soo Jang, Wonhee Kim, Hyun-Young Choi, and Yoonje Lee. 2022. "Prognostic Effect of Underlying Chronic Kidney Disease and Renal Replacement Therapy on the Outcome of Patients after Out-of-Hospital Cardiac Arrest: A Nationwide Observational Study" Medicina 58, no. 3: 444. https://doi.org/10.3390/medicina58030444