
Impact of Exercise Modalities on Peripheral and Central Components of Cardiorespiratory Capacity in Heart Transplantation Patients: A Systematic Review and Meta-Analysis

 ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Searches
2.2. Study Inclusion and Exclusion Criteria
2.3. Types of Interventions and Outcomes
2.4. Data Extraction, Synthesis, and Presentation
3. Results
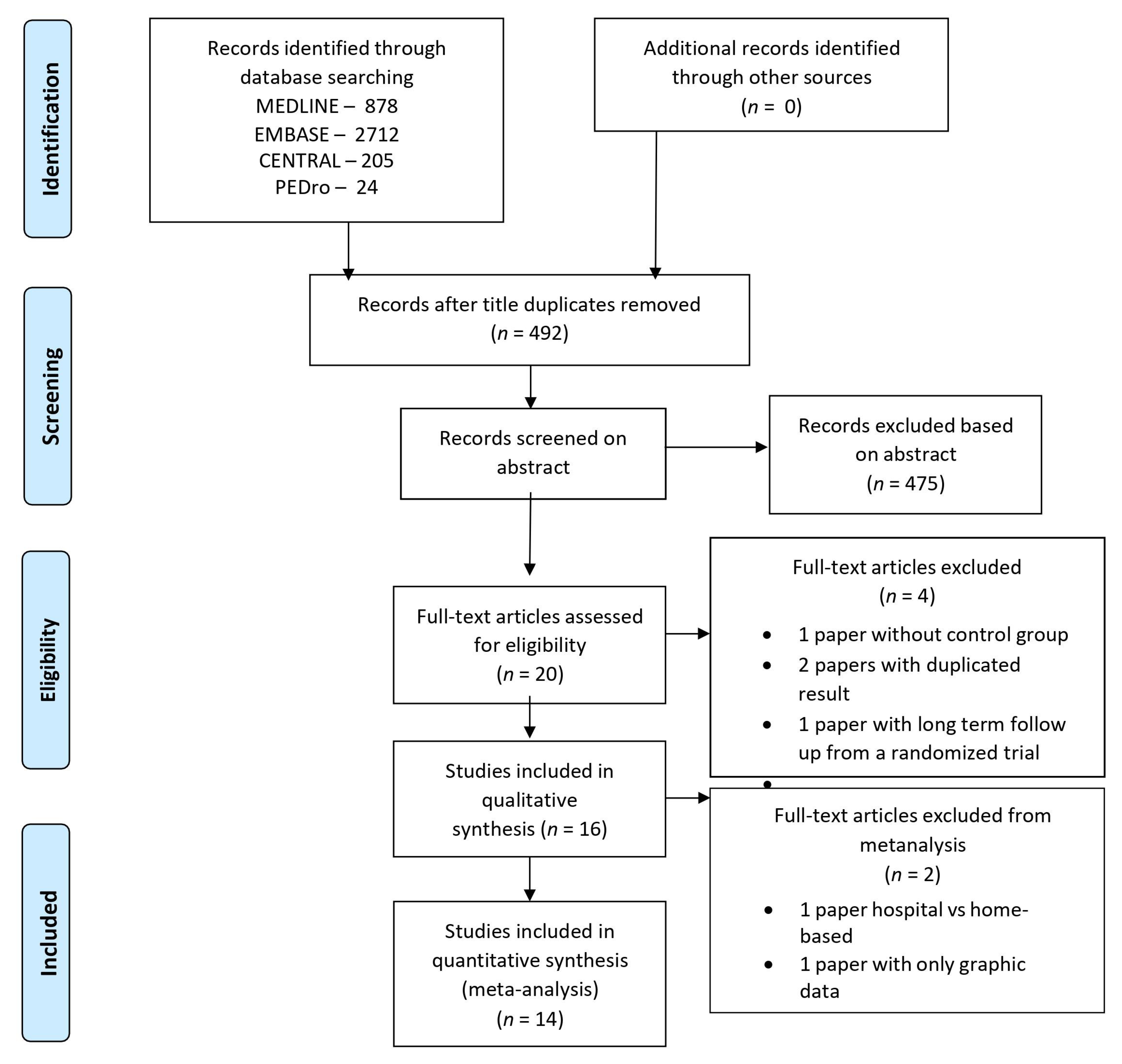
3.1. Selection, Evaluation of Studies, and Quality Assessment
3.2. Studies Included in the Systematic Review
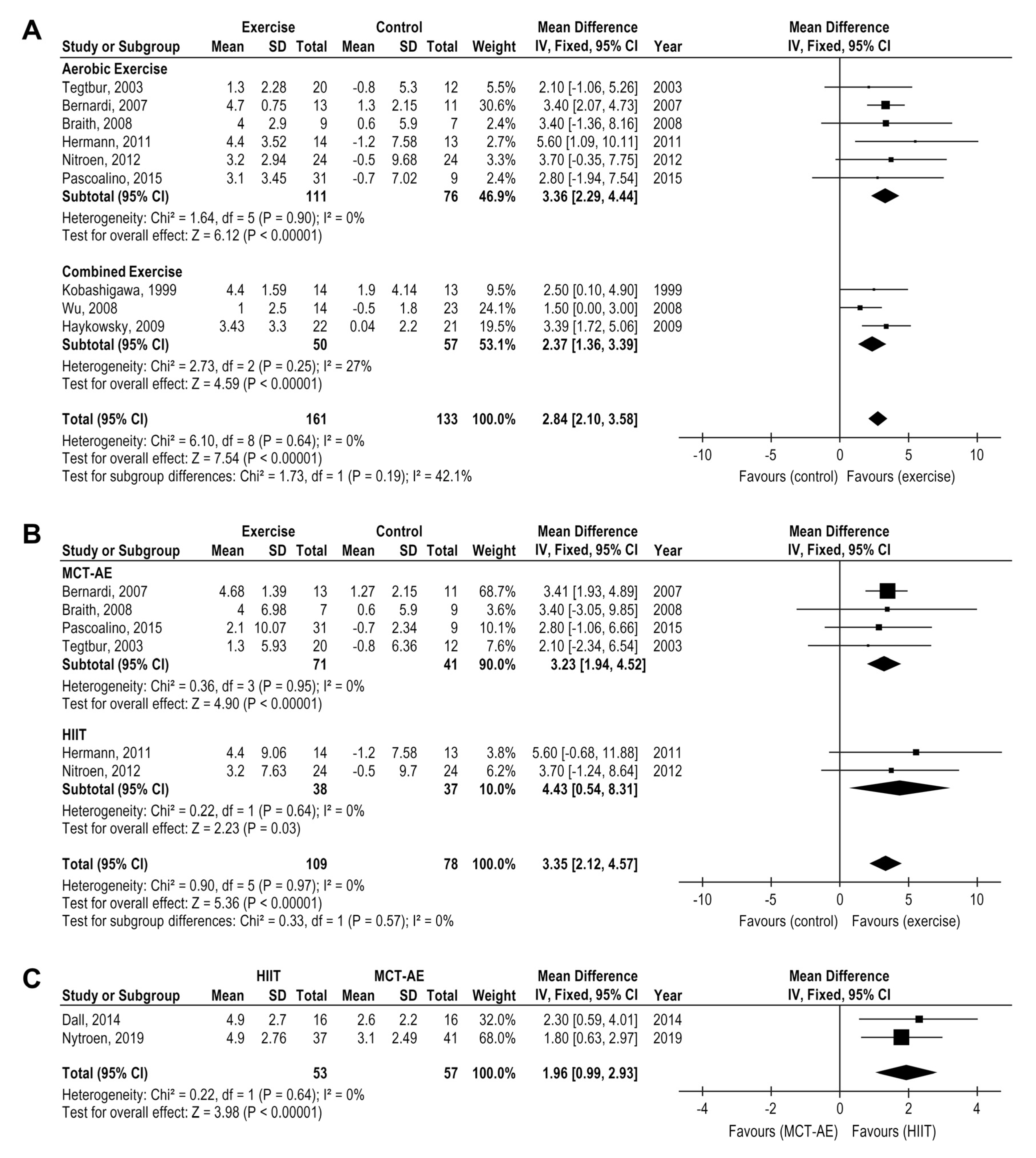
3.3. Exercise Effects on Peak Heart Rate
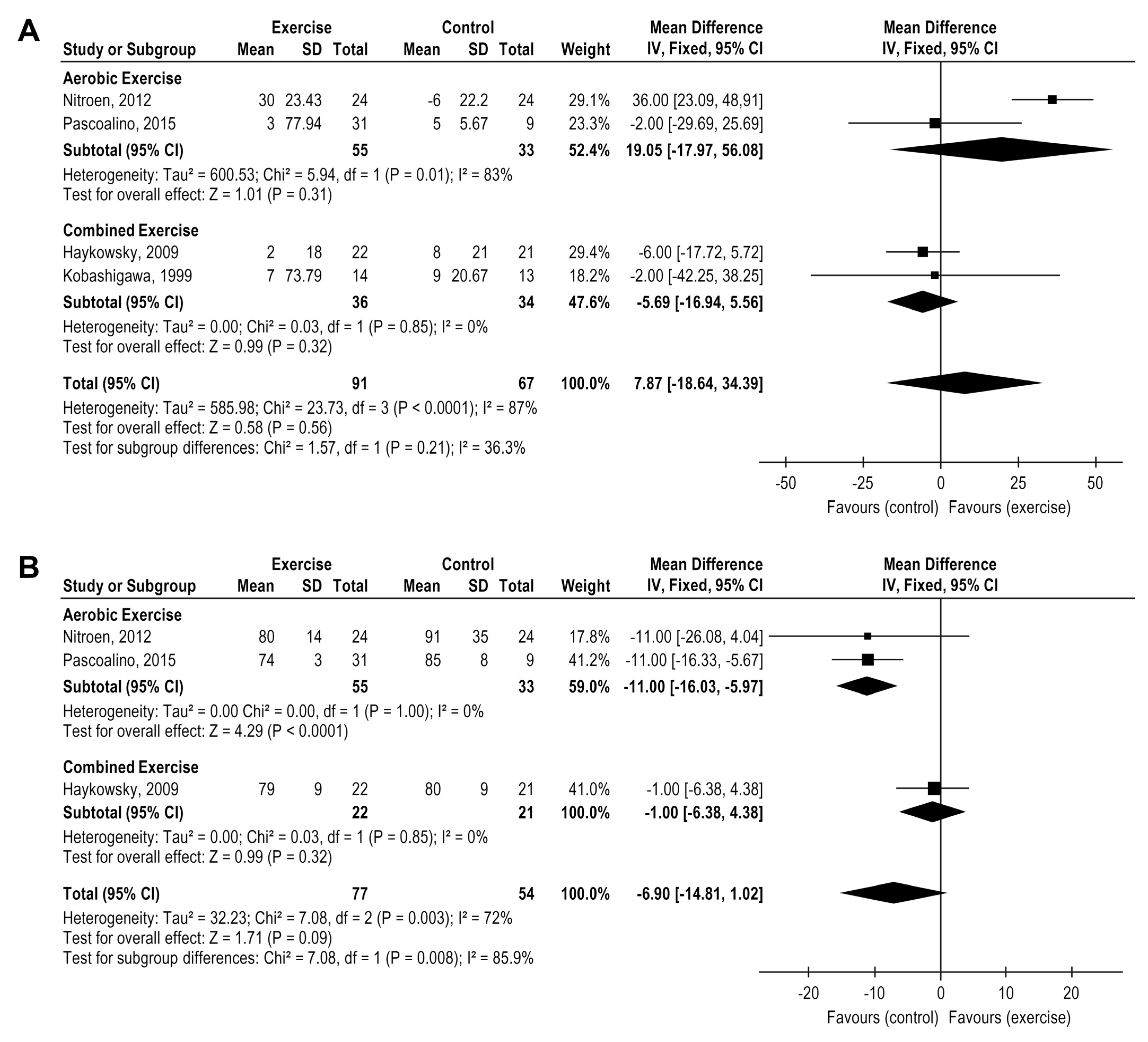
3.4. Exercise Effects on Peak Systolic and Diastolic Blood Pressure
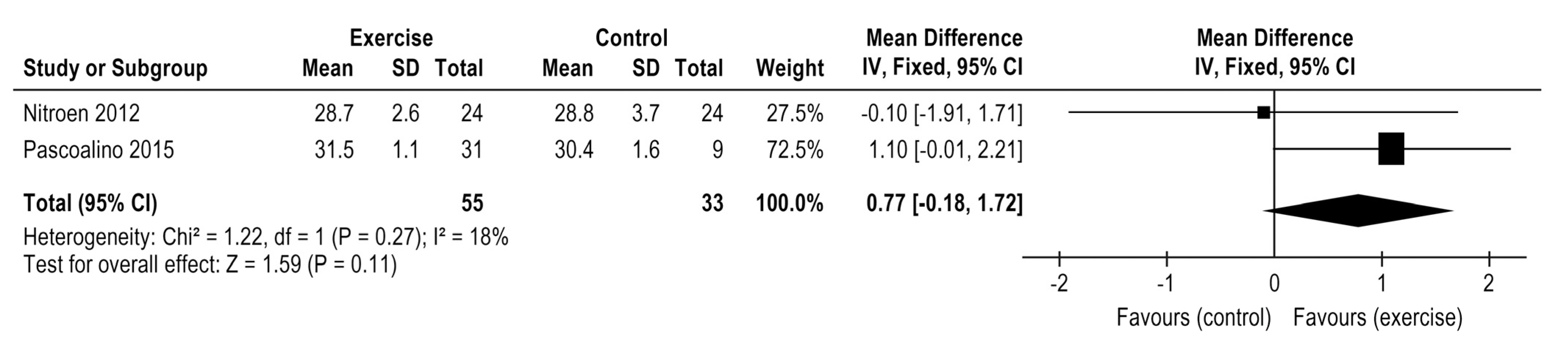
3.5. Exercise Effects on VE/V′CO2 Slope
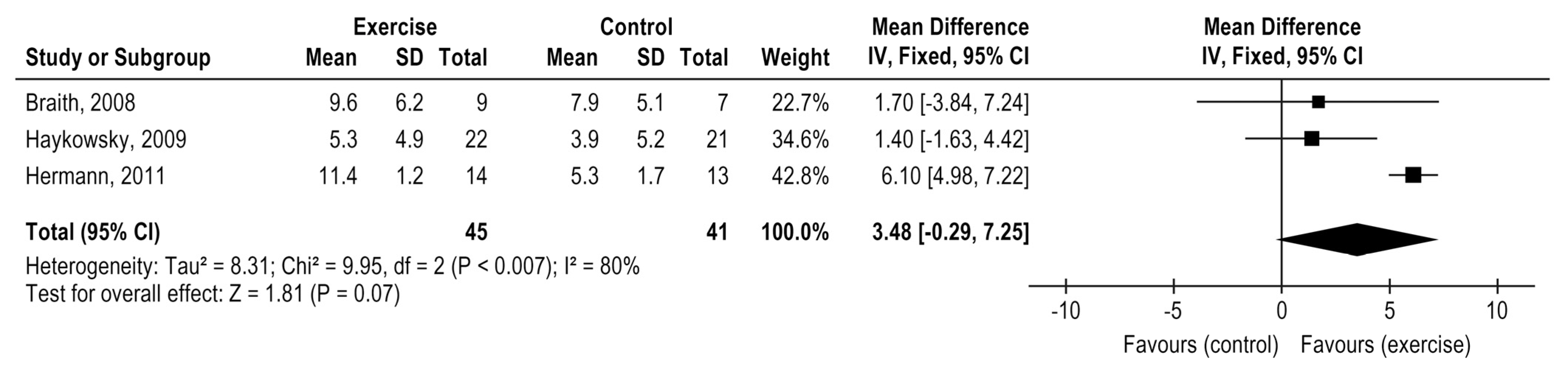
3.6. Exercise Effects on Flow-Mediated Dilation
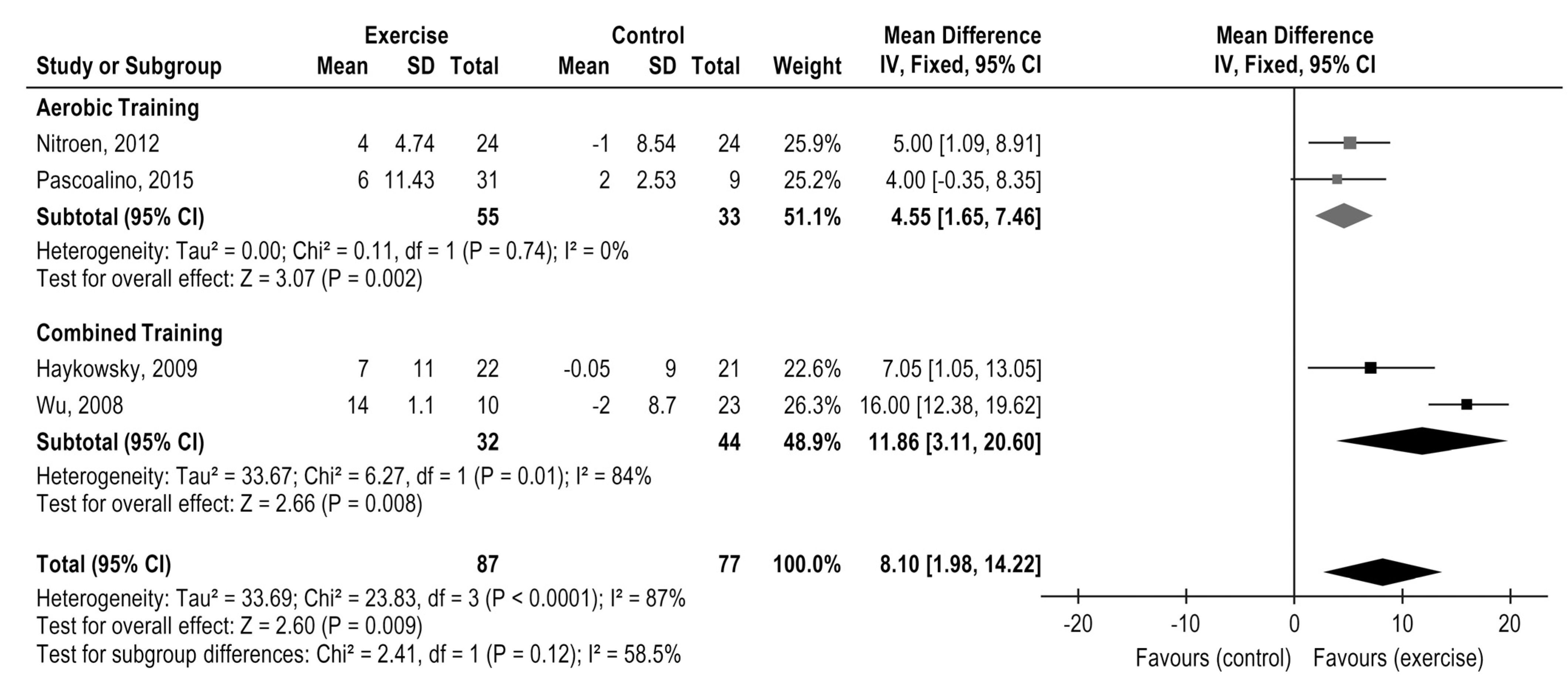
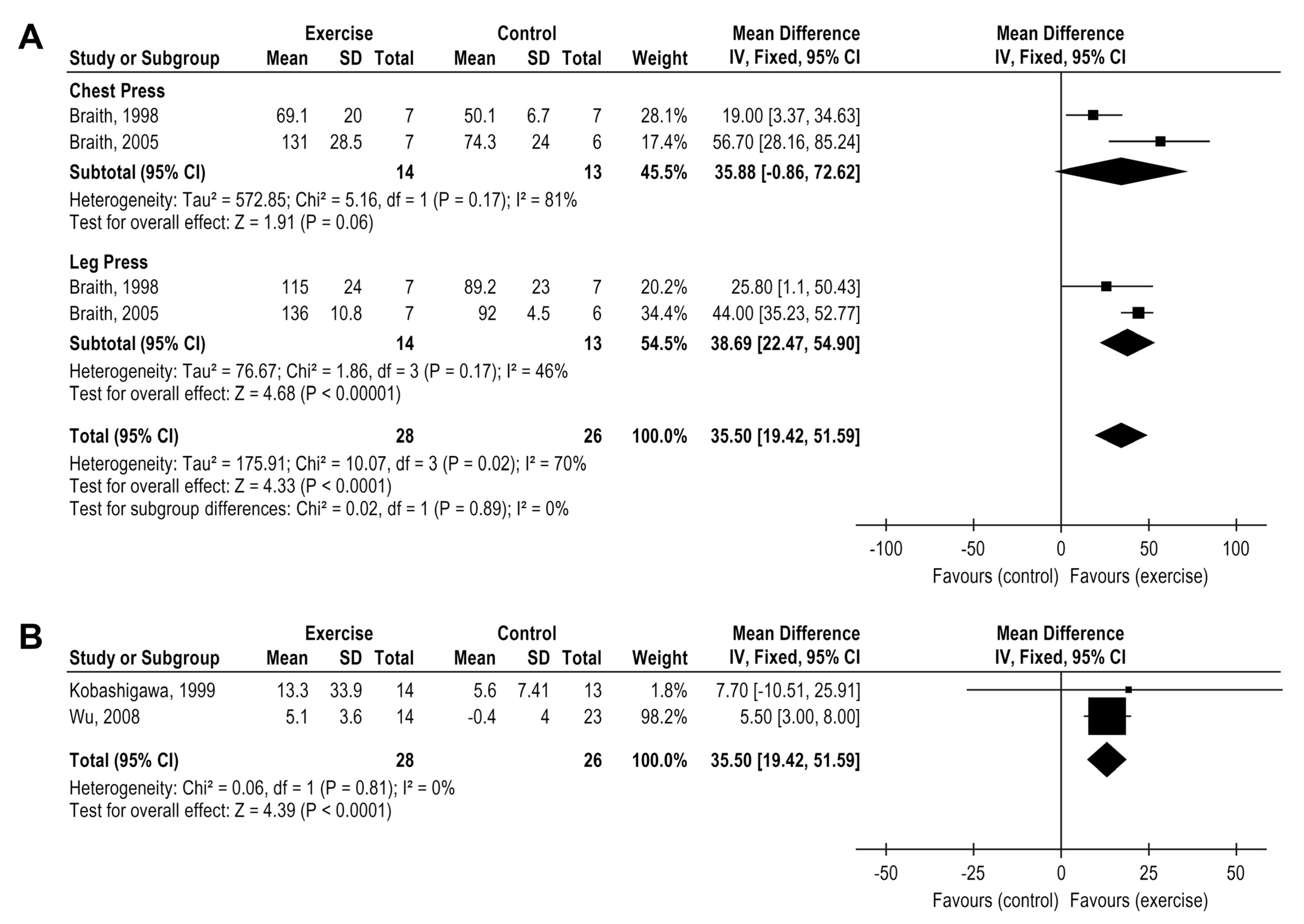
3.7. Exercise Effects on Muscle Strength
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Theochari, C.A.; Michalopoulos, G.; Oikonomou, E.K.; Giannopoulos, S.; Doulamis, I.P.; Villela, M.A.; Kokkinidis, D.G. Heart transplantation versus left ventricular assist devices as destination therapy or bridge to transplantation for 1-year mortality: A systematic review and meta-analysis. Ann. Cardiothorac. Surg. 2018, 7, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Yusen, R.D.; Edwards, L.B.; Dipchand, A.I.; Goldfarb, S.B.; Kucheryavaya, A.Y.; Levvey, B.J.; Lund, L.H.; Meiser, B.; Rossano, J.W.; Stehlik, J. The Registry of the International Society for Heart and Lung Transplantation: Thirty-third Adult Heart Transplantation Report—2016; Focus Theme: Primary Diagnostic Indications for Transplant. J. Heart Lung Transpl. 2016, 35, 1158–1169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jessup, M.; Drazner, M.H.; Book, W.; Cleveland, J.C.; Dauber, I.; Farkas, S.; Ginwalla, M.; Katz, J.N.; Kirkwood, P.; Kittleson, M.M.; et al. 2017 ACC/AHA/HFSA/ISHLT/ACP Advanced Training Statement on Advanced Heart Failure and Transplant Cardiology (Revision of the ACCF/AHA/ACP/HFSA/ISHLT 2010 Clinical Competence Statement on Management of Patients with Advanced Heart Failure and Cardiac Trans. J. Am. Coll. Cardiol. 2017, 69, 2977–3001. [Google Scholar] [CrossRef] [PubMed]
- Di Nora, C.; Livi, U. Heart transplantation in cardiac storage diseases: Data on Fabry disease and cardiac amyloidosis. Curr. Opin. Organ Transplant. 2020, 25, 211–217. [Google Scholar] [CrossRef]
- Habedank, D.; Ewert, R.; Hummel, M.; Wensel, R.; Hetzer, R.; Anker, S.D. Changes in exercise capacity, ventilation, and body weight following heart transplantation. Eur. J. Heart Fail. 2007, 9, 310–316. [Google Scholar] [CrossRef]
- Carter, R.; Al-Rawas, O.; Stevenson, A.; McDonagh, T.; Stevenson, R. Exercise Responses Following Heart Transplantation: 5 Year Follow-Up. Scott. Med. J. 2006, 51, 6–14. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.G.R.; Baumbach, A.; Bo, M.B.H.; Butler, J.; Celutkiene, J.; Chioncel, O.C.J.G.; Coats, A.J.S.; Crespo-Leiro, M.G.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Savin, W.M.; Haskell, W.L.; Schroeder, J.S.; Stinson, E.B. Cardiorespiratory responses of cardiac transplant patients to graded, symptom-limited exercise. Circulation 1980, 62, 55–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, L.; Nguyen, T.T.; Dall, C.H.; Burgess, L.; Bridges, C.; Taylor, R.S. Exercise-based cardiac rehabilitation in heart transplant recipients. Cochrane Database Syst. Rev. 2017, 2017, CD012264. [Google Scholar] [CrossRef]
- Tucker, W.J.; Beaudry, R.I.; Samuel, T.J.; Nelson, M.D.; Halle, M.; Baggish, A.L. Performance Limitations in Heart Transplant Recipients. Exerc. Sport Sci. Rev. 2018, 46, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Notarius, C.F.; Levy, R.D.; Tully, A.; Fitchett, D.; Magder, S. Cardiac versus noncardiac limits to exercise after heart transplantation. Am. Heart J. 1998, 135, 339–348. [Google Scholar] [CrossRef]
- Hollenberg, S.M.; Klein, L.W.; Parrillo, J.E.; Scherer, M.; Burns, D.; Tamburro, P.; Oberoi, M.; Johnson, M.R.; Costanzo, M.R. Coronary Endothelial Dysfunction After Heart Transplantation Predicts Allograft Vasculopathy and Cardiac Death. Circulation 2001, 104, 3091–3096. [Google Scholar] [CrossRef] [Green Version]
- Przybylowski, P.; Koc-Zorawska, E.; Malyszko, J.; Mysliwiec, M. Renalase and Endothelial Dysfunction in Heart Transplant Recipients. Transplant. Proc. 2013, 45, 394–396. [Google Scholar] [CrossRef]
- Stehlik, J.; Edwards, L.B.; Kucheryavaya, A.Y.; Benden, C.; Christie, J.; Dipchand, A.I.; Dobbels, F.; Kirk, R.; Rahmel, A.O.; Hertz, M.I. The Registry of the International Society for Heart and Lung Transplantation: 29th Official Adult Heart Transplant Report—2012. J. Heart Lung Transpl. 2012, 31, 1052–1064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tepperman, E.; Ramzy, D.; Prodger, J.; Sheshgiri, R.; Badiwala, M.; Ross, H. Surgical biology for the clinician: Vascular effects of immunosuppression. Can. J. Surg. 2010, 53, 57–63. [Google Scholar]
- Holm, T.; Aukrust, P.; Andreassen, A.K.; Ueland, T.; Brosstad, F.; Froland, S.S.; Simonsen, S.; Gullestad, L. Peripheral endothelial dysfunction in heart transplant recipients: Possible role of proinflammatory cytokines. Clin. Transplant. 2000, 14, 218–225. [Google Scholar] [CrossRef]
- Montero, D. The association of cardiorespiratory fitness with endothelial or smooth muscle vasodilator function. Eur. J. Prev. Cardiol. 2014, 22, 1200–1211. [Google Scholar] [CrossRef] [PubMed]
- Jendzjowsky, N.G.; Tomczak, C.R.; Lawrance, R.; Taylor, D.A.; Tymchak, W.J.; Riess, K.J.; Warburton, D.E.R.; Haykowsky, M.J. Impaired pulmonary oxygen uptake kinetics and reduced peak aerobic power during small muscle mass exercise in heart transplant recipients. J. Appl. Physiol. 2007, 103, 1722–1727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costanzo, M.R.; Dipchand, A.; Starling, R.; Anderson, A.; Chan, M.; Desai, S.; Fedson, S.; Fisher, P.; Gonzales-Stawinski, G.; Martinelli, L.; et al. The International Society of Heart and Lung Transplantation Guidelines for the care of heart transplant recipients. J. Heart Lung Transplant. 2010, 29, 914–956. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, P.-L.; Wu, Y.-T.; Chao, W.-J. Effects of Exercise Training in Heart Transplant Recipients: A Meta-Analysis. Cardiology 2011, 120, 27–35. [Google Scholar] [CrossRef]
- Mandic, S.; Tymchak, W.; Kim, D.; Daub, B.; Quinney, H.A.; Taylor, D.; Al-Kurtass, S.; Haykowsky, M.J. Effects of aerobic or aerobic and resistance training on cardiorespiratory and skeletal muscle function in heart failure: A randomized controlled pilot trial. Clin. Rehabil. 2009, 23, 207–216. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.0. Available online: www.training.cochrane.org/handbook (accessed on 18 December 2021).
- Tegtbur, U.; Busse, M.W.; Jung, K.; Markofsky, A.; Machold, H.; Brinkmeier, U.; Haverich, A.; Pethig, K. Phase III Rehabilitation nach Herztransplantation; Springer: Berlin/Heidelberg, Germany, 2003; Volume 92, pp. 908–915. [Google Scholar] [CrossRef]
- Bernardi, L.; Radaelli, A.; Passino, C.; Falcone, C.; Auguadro, C.; Martinelli, L.; Rinaldi, M.; Viganò, M.; Finardi, G. Effects of physical training on cardiovascular control after heart transplantation. Int. J. Cardiol. 2007, 118, 356–362. [Google Scholar] [CrossRef]
- Braith, R.W.; Schofield, R.S.; Hill, J.A.; Casey, D.; Pierce, G.L. Exercise Training Attenuates Progressive Decline in Brachial Artery Reactivity in Heart Transplant Recipients. J. Heart Lung Transplant. 2008, 27, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Hermann, T.S.; Dall, C.H.; Christensen, S.B.; Goetze, J.P.; Prescott, E.; Gustafsson, F. Effect of High Intensity Exercise on Peak Oxygen Uptake and Endothelial Function in Long-Term Heart Transplant Recipients. Arab. Archaeol. Epigr. 2011, 11, 536–541. [Google Scholar] [CrossRef]
- Nytrøen, K.; Rustad, L.A.; Aukrust, P.; Ueland, T.; Hallén, J.; Holm, I.; Rolid, K.; Lekva, T.; Fiane, A.E.; Amlie, J.P.; et al. High-Intensity Interval Training Improves Peak Oxygen Uptake and Muscular Exercise Capacity in Heart Transplant Recipients. Arab. Archaeol. Epigr. 2012, 12, 3134–3142. [Google Scholar] [CrossRef]
- Pascoalino, L.N.; Ciolac, E.G.; Tavares, A.C.; Castro, R.E.; Ayub-Ferreira, S.M.; Bacal, F.; Issa, V.S.; Bocchi, E.A.; Guimarães, G.V. Exercise training improves ambulatory blood pressure but not arterial stiffness in heart transplant recipients. J. Heart Lung Transplant. 2015, 34, 693–700. [Google Scholar] [CrossRef]
- Pierce, G.L.; Schofield, R.S.; Casey, D.; Hamlin, S.A.; Hill, J.A.; Braith, R.W. Effects of exercise training on forearm and calf vasodilation and proinflammatory markers in recent heart transplant recipients: A pilot study. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Nytrøen, K.; Rolid, K.; Andreassen, A.K.; Yardley, M.; Gude, E.; Dahle, D.O.; Bjørkelund, E.; Authen, A.R.; Grov, I.; Wigh, J.P.; et al. Effect of High-Intensity Interval Training in De Novo Heart Transplant Recipients in Scandinavia. Circulation 2019, 139, 2198–2211. [Google Scholar] [CrossRef]
- Dall, C.H.; Snoer, M.; Christensen, S.; Monk-Hansen, T.; Frederiksen, M.; Gustafsson, F.; Langberg, H.; Prescott, E. Effect of High-Intensity Training Versus Moderate Training on Peak Oxygen Uptake and Chronotropic Response in Heart Transplant Recipients: A Randomized Crossover Trial. Arab. Archaeol. Epigr. 2014, 14, 2391–2399. [Google Scholar] [CrossRef] [Green Version]
- Haykowsky, M.; Taylor, D.; Kim, D.; Tymchak, W. Exercise Training Improves Aerobic Capacity and Skeletal Muscle Function in Heart Transplant Recipients. Arab. Archaeol. Epigr. 2009, 9, 734–739. [Google Scholar] [CrossRef] [PubMed]
- Kobashigawa, J.A.; Leaf, D.A.; Lee, N.; Gleeson, M.P.; Liu, H.; Hamilton, M.A.; Moriguchi, J.D.; Kawata, N.; Einhorn, K.; Herlihy, E.; et al. A Controlled Trial of Exercise Rehabilitation after Heart Transplantation. N. Engl. J. Med. 1999, 340, 272–277. [Google Scholar] [CrossRef]
- Wu, Y.-T.; Chien, C.-L.; Chou, N.-K.; Wang, S.-S.; Lai, J.-S.; Wu, Y.-W. Efficacy of a Home-Based Exercise Program for Orthotopic Heart Transplant Recipients. Cardiology 2008, 111, 87–93. [Google Scholar] [CrossRef]
- Braith, R.; Welsch, M.; Mills, R.; Keller, J.; Pollock, M. Resistance exercise prevents glucocorticoid-induced myopathy in heart transplant recipients. Med. Sci. Sport Exerc. 1998, 30, 483–489. [Google Scholar] [CrossRef]
- Braith, R.W.; Magyari, P.M.; Pierce, G.L.; Edwards, D.G.; Hill, J.A.; White, L.J.; Aranda, J.M. Effect of Resistance Exercise on Skeletal Muscle Myopathy in Heart Transplant Recipients. Am. J. Cardiol. 2005, 95, 1192–1198. [Google Scholar] [CrossRef] [PubMed]
- Karapolat, H.; Demir, E.; Bozkaya, Y.T.; Eyigor, S.; Nalbantgil, S.; Durmaz, B.; Zoghi, M. Comparison of hospital-based versus home-based exercise training in patients with heart failure: Effects on functional capacity, quality of life, psychological symptoms, and hemodynamic parameters. Clin. Res. Cardiol. 2009, 98, 635–642. [Google Scholar] [CrossRef]
- Karapolat, H.; Eyigör, S.; Zoghi, M.; Yagdi, T.; Nalbangil, S.; Durmaz, B. Comparison of Hospital-Supervised Exercise Versus Home-Based Exercise in Patients After Orthotopic Heart Transplantation: Effects on Functional Capacity, Quality of Life, and Psychological Symptoms. Transplant. Proc. 2007, 39, 1586–1588. [Google Scholar] [CrossRef]
- Monk-Hansen, T.; Dall, C.H.; Christensen, S.B.; Snoer, M.; Gustafsson, F.; Rasmusen, H.; Prescott, E. Interval training does not modulate diastolic function in heart transplant recipients. Scand. Cardiovasc. J. 2014, 48, 91–98. [Google Scholar] [CrossRef]
- Braith, R.W.; Limacher, M.C.; Leggett, S.H.; Pollock, M.L. Skeletal muscle strength in heart transplant recipients. J. Heart Lung Transplant. 1993, 12, 1018–1023. [Google Scholar] [PubMed]
- Lampert, E.; Mettauer, B.; Hoppeler, H.; Charloux, A.; Charpentier, A.; Lonsdorfer, J. Skeletal muscle response to short endurance training in heart transplant recipients. J. Am. Coll. Cardiol. 1998, 32, 420–426. [Google Scholar] [CrossRef] [Green Version]
- Nytrøen, K.; Rustad, L.A.; Gude, E.; Hallén, J.; Fiane, A.E.; Rolid, K.; Holm, I.; Aakhus, S.; Gullestad, L. Muscular exercise capacity and body fat predict VO2peak in heart transplant recipients. Eur. J. Prev. Cardiol. 2012, 21, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Nytrøen, K.; Myers, J.; Chan, K.N.; Geiran, O.R.; Gullestad, L. Chronotropic Responses to Exercise in Heart Transplant Recipients. Am. J. Phys. Med. Rehabil. 2011, 90, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Bengel, F.M.; Ueberfuhr, P.; Schiepel, N.; Nekolla, S.G.; Reichart, B.; Schwaiger, M. Effect of Sympathetic Reinnervation on Cardiac Performance after Heart Transplantation. N. Engl. J. Med. 2001, 345, 731–738. [Google Scholar] [CrossRef]
- Salles, A.F.; Machado, C.V.; Cordovil, A.; Leite, W.A.; Moisés, V.A.; de Almeida, D.R. A elevação da pressão arterial sistólica durante o teste ergométrico após transplante cardíaco: Correlação com o quadro clínico e a função ventricular avaliada pela ecocardiografia sob estresse com dobutamina. Arq. Bras. Cardiol. 2006, 87, 628–633. [Google Scholar] [CrossRef] [Green Version]
- Geny, B.; Saini, J.; Mettauer, B.; Lampert, E.; Piquard, F.; Follenius, M.; Epailly, E.; Schnedecker, B.; Eisenmann, B.; Haberey, P.; et al. Effect of short-term endurance training on exercise capacity, haemodynamics and atrial natriuretic peptide secretion in heart transplant recipients. Graefe’s Arch. Clin. Exp. Ophthalmol. 1996, 73, 259–266. [Google Scholar] [CrossRef]
- Kavanagh, T.; Yacoub, M.H.; Mertens, D.J.; Kennedy, J.; Campbell, R.B.; Sawyer, P. Cardiorespiratory responses to exercise training after orthotopic cardiac transplantation. Circulation 1988, 77, 162–171. [Google Scholar] [CrossRef] [Green Version]
- Franzoni, F.; Ghiadoni, L.; Galetta, F.; Plantinga, Y.; Lubrano, V.; Huang, Y.; Salvetti, A.; Regoli, F.; Taddei, S.; Santoro, G. Physical activity, plasma antioxidant capacity, and endothelium-dependent vasodilation in young and older men. Am. J. Hypertens. 2005, 18, 510–516. [Google Scholar] [CrossRef] [PubMed]
- Tinken, T.M.; Thijssen, D.H.J.; Black, M.A.A.; Cable, N.; Green, D.J. Time course of change in vasodilator function and capacity in response to exercise training in humans. J. Physiol. 2008, 586, 5003–5012. [Google Scholar] [CrossRef] [PubMed]
- Buscemi, S.; Canino, B.; Batsis, J.A.; Buscemi, C.; Calandrino, V.; Mattina, A.; Arnone, M.; Caimi, G.; Cerasola, G.; Verga, S. Relationships between maximal oxygen uptake and endothelial function in healthy male adults: A preliminary study. Acta Diabetol. 2010, 50, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Linke, A.; Schoene, N.; Gielen, S.; Hofer, J.; Erbs, S.; Schuler, G.; Hambrecht, R. Endothelial dysfunction in patients with chronic heart failure: Systemic effects of lower-limb exercise training. J. Am. Coll. Cardiol. 2001, 37, 392–397. [Google Scholar] [CrossRef] [Green Version]
- Gokce, N.; Vita, J.A.; Bader, D.S.; Sherman, D.L.; Hunter, L.M.; Holbrook, M.; O’Malley, C.; Keaney, J.F., Jr.; Balady, G.J. Effect of exercise on upper and lower extremity endothelial function in patients with coronary artery disease. Am. J. Cardiol. 2002, 90, 124–127. [Google Scholar] [CrossRef]
- Walsh, J.; Bilsborough, W.; Maiorana, A.; Best, M.; O’Driscoll, G.J.; Taylor, R.R.; Green, D.J. Exercise training improves conduit vessel function in patients with coronary artery disease. J. Appl. Physiol. 2003, 95, 20–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higashi, Y.; Sasaki, S.; Sasaki, N.; Nakagawa, K.; Ueda, T.; Yoshimizu, A.; Kurisu, S.; Matsuura, H.; Kajiyama, G.; Oshima, T. Daily Aerobic Exercise Improves Reactive Hyperemia in Patients with Essential Hypertension. Hypertension 1999, 33, 591–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gullestad, L.; Myers, J.; Edvardsen, T.; Kjekshus, J.; Geiran, O.; Simonsen, S. Predictors of exercise capacity and the impact of angiographic coronary artery disease in heart transplant recipients. Am. Heart J. 2004, 147, 49–54. [Google Scholar] [CrossRef]
- Watanabe, T.; Seguchi, O.; Nishimura, K.; Yanase, M.; Sato, T.; Sunami, H.; Nakajima, S.; Hisamatsu, E.; Sato, T.; Kuroda, K.; et al. Is Brachial Flow-Mediated Dilation the Predictor of Development of Cardiac Allograft Vasculopathy in Recipients with Heart Transplantation? Circulation 2014, 130, 11585. [Google Scholar] [CrossRef]
- Cuppoletti, A.; Sitges, M.; Pérez Villa, F.; Orús, J.; Magriñá, J.; Roig, E. Impairment in forearm endothelium-dependent vasodilation after heart transplantation. Transplant. Proc. 2003, 35, 2011–2013. [Google Scholar] [CrossRef]
- Roig, E.; Cuppoletti, A.; Masotti, M.; Kianco, R.; Vallejos, I.; Sitges, M. Assessment of Peripheral Endothelial-Dependent Vasodilatation Within the First Year After Heart Transplantation. J. Heart Lung Transplant. 2009, 28, 299–304. [Google Scholar] [CrossRef]
- Ferreira, A.M.; Tabet, J.-Y.; Frankenstein, L.; Metra, M.; Mendes, M.; Zugck, C.; Beauvais, F.; Cohen-Solal, A. Ventilatory Efficiency and the Selection of Patients for Heart Transplantation. Circ. Heart Fail. 2010, 3, 378–386. [Google Scholar] [CrossRef] [Green Version]
- Tsai, W.-J.; Tsai, H.-Y.; Kuo, L.-Y.; Lin, Y.-S.; Chen, B.-Y.; Lin, W.-H.; Shen, S.-L.; Huang, H.-Y. VE/VCO2 Slope and Functional Capacity in Patients Post-Heart Transplantation. Transplant. Proc. 2018, 50, 2733–2737. [Google Scholar] [CrossRef]
- Di Nora, C.; Guidetti, F.; Livi, U.; Antonini-Canterin, F. Role of Cardiac Rehabilitation After Ventricular Assist Device Implantation. Heart Fail. Clin. 2021, 17, 273–278. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Studyref, Year, Type | Time after HTx and Local | Sample Size (n) | Age (yrs) (mean ± SD) | Outcomes | Intervention Description | Frequency (d/wk) | Session Duration (min) | Program Duration (wk) | PEDro Score | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| AEROBIC TRAINING VS. CONTROL | |||||||||||
| Tegtbur [23] RCT | 2003 | 5 years | AT | 20 | 55.0 ± 7.0 | VO2peak | Outpatient–home-based-controlled remotely AT: bicycle ergometer (10% below the Anaerobic threshold); CG: usual medical care | 3 | 28 | 48 | 4 |
| CG | 12 | 54.0 ± 8.0 | |||||||||
| Bernardi et al. [24] RCT | 2007 | 6 months | AT | 13 | 34.9 ± 4.0 | VO2peak | Outpatient–home-based–non-supervised AT: bicycle ergometer (50 rpm for 30 min at 60–70% of VO2peak. New training load calculated after 3 months by a new exercise test to exhaustion); CG: avoid exercise above their regular pre-study routine and specifically to avoid exercise that would lead to feelings of dyspnoea or exhaustion. | 5 | 30 | 24 | 4 |
| CG | 11 | 33.9 ± 4.3 | |||||||||
| Pierce et al. [29] RCT | 2008 | 8 weeks | AT | 08 | 53.6 ± 13.6 | VO2peak, HRpeak | Outpatient–clinic-supervised. AT: Training protocol started with 30 min of continuous exercise and progressed to 34 to 40 min as tolerated after the initial 4 weeks. Continuous treadmill walking (Borg RPE between 11–13, or ‘moderate’ to ‘somewhat hard’ range, following ACSM guidelines. Progression to an RPE in the 12–14 Borg scale range ‘as tolerated’ by each participant) CG: standard medical care and encouragement to engage in regular walking, but did not participate in a supervised exercise. | - | Initial: 30 After 4 wk: 40 | 12 | 4 |
| CG | 06 | 54.2 ± 6.4 | |||||||||
| Braith et al. [25] RCT | 2008 | 8 weeks | AT | 09 | 54.3 ± 9.5 | VO2peak, FMD | Hospital-supervised AT: initial 4 weeks: 5 min warm-up + 30 min continuous treadmill walking + 5 min cool-down. Exercise progressed to 35 to 40 min thereafter. The intensity in a range from Borg RPE between 11–13, or ‘moderate’ to ‘somewhat hard’ range and progressing to RPE in the 12–14 Borg scale range ‘as tolerated’ following ACSM guidelines. CG: standard medical care and encouragement to engage in regular walking but did not participate in a supervised exercise. | 3 | Initial: 30 After: 35 to 40 as tolerated | 12 | 5 |
| CG | 07 | 54.4 ± 13.1 | |||||||||
| Hermann et al. [26] RCT | 2011 | 1 year | AT | 14 | 53.0 ± 11.0 | VO2peak, FMD | Outpatient–clinic-supervised. AT: warm-up (above 50% VO2peak) + HIIT on bicycle (interval blocks of 4 min/2 min/30 s according to 80%, 85%, and 90% of VO2 peak and 30 s recovery periods) + staircase running (80% of peak VO2 peak); CG: Patient education (4 h of teaching to the patients about the benefits of exercise training together with information on nutrition) | 3 | 42 | 8 | 7 |
| CG | 13 | 47.0 ± 18.0 | |||||||||
| Nytrøen et al. [27] RCT | 2012 | 1–8 years | AT | 24 | 48.0 ± 17.0 | VO2peak, HRpeak, SBPpeak DBPpeak, VE/VCO2 slope, Muscle strength | Outpatient–clinic-supervised. AT: HIIT on a treadmill (10 min warm-up + 4 min exercise bouts at 85–95% of HRpeak, separated by 3 min active pauses at Borg scale 11–13, 6–20 RPE). Additionally, the patients were encouraged to continue any physical activity on their own. CG: No intervention was given to the control group other than basic. | 3 | 35 | 24 | 5 |
| CG | 24 | 53.0 ± 14.0 | |||||||||
| Pascoalino et al. [28] RCT | 2015 | ≥1 year | AT | 31 | 45.0 ± 3.0 | VO2peak, VE/VCO2 slope, HRpeak, SBPpeak, DBPpeak | Outpatient–clinic-supervised. AT: Supervised: 5 min warm-up + 40 min walking/jogging on a treadmill (80% HR of the RCP - 69.0% ± 1.9 % of VO2 max. Endurance Exercise Intensity was continually adjusted) + 5 min cool down. Non-supervised: Same exercise protocol following exercise intensity of 11–13 on the rate of Borg scale (range: 16–20); CG: maintain their daily activities without AE during the 12-week period. | 3 | 40 | 12 | 6 |
| CG | 09 | 45.0 ± 6.0 | |||||||||
| COMBINED TRAINING VS. CONTROL GROUP | |||||||||||
| Kobachigawa et al. [33] RCT | 1999 | 2 weeks | CT | 14 | 55.0 ± 8.0 | VO2peak, HRpeak, SBPpeak, Muscle strength | Outpatient–clinic-supervised. RT: closed-chain resistive activities + abdominal exercises; AT: Treadmill or bicycle ergometer (a goal of at least 30 min of continuous exercise at a moderate intensity according to patient’s tolerance) CG: Written guidelines (exercises at home) | 1–3 | AT: ≥30 | 24 | 5 |
| CG | 13 | 50.0 ± 12.0 | |||||||||
| Wu et al. [34] RCT | 2008 | 1 year | CT | 12 | 60.6 ± 6.2 | VO2peak, HRpeak, Muscle strength | Outpatient–home-based–supervised every 1–2 weeks. RT: 5 min warm-up + upper and lower extremity light-weight; AT: 15–20 min walking at a prescribed intensity with 60–70% VO2 peak + stepping exercise with a stool + 5 min cool down. CG: control group was asked to keep their usual activity lifestyle during the study period. | 3 | 40 | 8 | 5 |
| CG | 19 | 51.6 ± 12.8 | |||||||||
| Haykowsky et al. [32] RCT | 2009 | ≥0.5 year | CT | 22 | 57.0 ± 11.0 | VO2peak, HRpeak, SBPpeak, DBPpeak, FMD | Outpatient–hospital-supervised. AT: treadmill and bicycle (HR: 60–80% VO2 peak) for 30–45 min. After 4 weeks, continuous aerobic training 3 days/week (HR = 80% VO2 peak) + Interval training 2 days/week (10 to 25 rep–gradually increase-of 30 s exercise at 90–100% baseline peak power output followed by 60 s rest); RT: upper (chest press, latissimus dorsi pulldown, arms curls) and lower extremity (leg press) strength training 10 rep, gradually increased until 25 rep at 50% of maximal strength (1 rep = 30 s exercise and 60 s rest); CG: continued with their usual activities of daily living. | AT: 5 RT: 2 | 30–45 45 | 12 | 4 |
| CG | 21 | 57.0 ± 11.0 | |||||||||
| RESISTANCE TRAINING VS. CONTROL GROUP | |||||||||||
| Braith et al. [35] RCT | 1998 | 2 months | RT | 7 | 54 ± 3 | Muscle strength | Outpatient–clinic–supervised. RT: 5 min of warm-up walking on a treadmill + lumbar extensor training 1 day/week and upper and lower body resistance training 2 days/week. A single set of 10–15 repetitions was completed for each exercise: lumbar extension, duo-decline chest press, knee extension, pullover, knee flexion, triceps extension, biceps flexion, shoulder press, and the abdominal machine. The initial training weight represented 50% of the one-repetition maximum (1-RM) test. The transplant recipients were not permitted to exceed 15 repetitions. Rather, when 15 repetitions were successfully achieved, the weight was increased by 5–10% at the next training session. CG: No resistance training intervention | 3 | Not described | 12 24 | 4 |
| CG | 7 | 51 ± 8 | |||||||||
| Braith et al. [36] RCT | 2005 | 2 months | RT | 8 | 52 ± 2 | Muscle strength | Outpatient–home-based-supervised RT: standard care home-based walking program (not supervised) associated with resistance training. 5 min warming-up + a single set from 10 to 15 repetitions were completed for each exercise: chest press, knee extension, pulldown, seated leg curl, shoulder press, seated triceps dip, biceps curl, and lumbar extension at 50% of 1 RM. The resistance was increased by 5% to 10% at the next training session when 15 repetitions were successfully achieved. Upper body exercises were alternated with lower body exercises. CG: standard care home-based walking program (not supervised) | 2 | Not described | 24 | 6 |
| CG | 7 | 53 ± 2 | |||||||||
| HIIT VS. MCT | |||||||||||
| Dall [31] RCT | 2014 | ≥1 year | HIIT MCT | 16 | 51.9 (33–70) Cross-over | VO2peak, HRpeak | Outpatient–clinic-supervised. AT–HIIT: Each HIIT session consisted of 16 min interval training with intervals of 4-, 2-and1-min duration at >80% of VO2peak, separated by a 2-min active rest period (approx. 60% of VO2peak) | 3 | 16 45 | 12 | 7 |
| AT–MCT-AE: The CON sessions consisted of biking for 45 min with an intensity corresponding to 60–70% of VO2peak. All sessions began with a 10 min warm-up and ended with a 10-min cooldown. | |||||||||||
| Nytrøen [30] RCT | 2019 | 11 weeks | HIIT | 37 | 50 ± 12 | VO2peak, HRpeak, VE/VCO2 slope, Muscle strength, FMD | Outpatient–clinic-supervised. AT; HIIT: 2- to 4-min intervals at 85% to 95% of peak effort (85%–95% of peak HR or ≈81–93% of Vo2peak-16 to 18 on Borg scale). 3–6 months after HTx, training consisted of 1 HIT session, 1 resistance training session (core musculature and large muscle groups), and 1 combined session per week. From 6–9 months after HTx, 2 HIT sessions and 1 resistance training session per week. The last 2 to 3 months of the intervention consisted of 3 HIT sessions per week | 2–3 | 40 | 48 | 7 |
| MCT | 41 | 48 ± 14 | AT; MCT-AE: 60% to 80% of peak effort, regular core strengthening exercises, and exercises for large muscle groups | ||||||||
| HOSPITAL VS. HOME-BASED | |||||||||||
| 45.27 ± 13.10 35.61 ± 12.91 | CT–Hospital-supervised: Exercise sessions included flexibility exercises, aerobic exercises, strengthening exercises, breathing exercises, and relaxation exercises. 30 min of aerobic exercises on either a treadmill or a stationary bicycle at 60% to 70% of the maximal VO2 and a level of 13 to 15 on the Borg scale. After 2 weeks, strengthening exercises were added: abdominal, upper limb, and lower limb muscle groups, using progressively heavier "light-weights", ranging from 250 to 500 g. In the end, all patients performed relaxation exercises according to the Jacobson technique of progressive muscle relaxation | ||||||||||
| Karapolat [38] RCT | 2007 | 15 months | CT Hosp CT Home | 15 13 | VO2peak | CT–Home-based–non-supervised: All exercises taught to group CT-Hosp patients were the same ones as those performed by the patients in CT–Home-based group. In addition, a walking program was performed. | 3 | 90 | 8 | 3 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turri-Silva, N.; Santos, F.V.; Rodrigues, W.C.C.; Freire, J.S.; Cahalin, L.C.; Verboven, K.; Quaglioti Durigan, J.L.; Hansen, D.; Cipriano, G., Jr. Impact of Exercise Modalities on Peripheral and Central Components of Cardiorespiratory Capacity in Heart Transplantation Patients: A Systematic Review and Meta-Analysis. Medicina 2022, 58, 32. https://doi.org/10.3390/medicina58010032
Turri-Silva N, Santos FV, Rodrigues WCC, Freire JS, Cahalin LC, Verboven K, Quaglioti Durigan JL, Hansen D, Cipriano G Jr. Impact of Exercise Modalities on Peripheral and Central Components of Cardiorespiratory Capacity in Heart Transplantation Patients: A Systematic Review and Meta-Analysis. Medicina. 2022; 58(1):32. https://doi.org/10.3390/medicina58010032
Chicago/Turabian StyleTurri-Silva, Natália, Francisco Valdez Santos, Wanessa Camilly Caldas Rodrigues, Josuelir Silva Freire, Lawrence C. Cahalin, Kenneth Verboven, João Luiz Quaglioti Durigan, Dominique Hansen, and Gerson Cipriano, Jr. 2022. "Impact of Exercise Modalities on Peripheral and Central Components of Cardiorespiratory Capacity in Heart Transplantation Patients: A Systematic Review and Meta-Analysis" Medicina 58, no. 1: 32. https://doi.org/10.3390/medicina58010032