

The Efficacy of Different Laser Applications on Dentin Sealing in Preventing Discoloration Induced by Mineral Trioxide Aggregate

Abstract
:1. Introduction
2. Materials and Methods
2.1. Tooth Selection
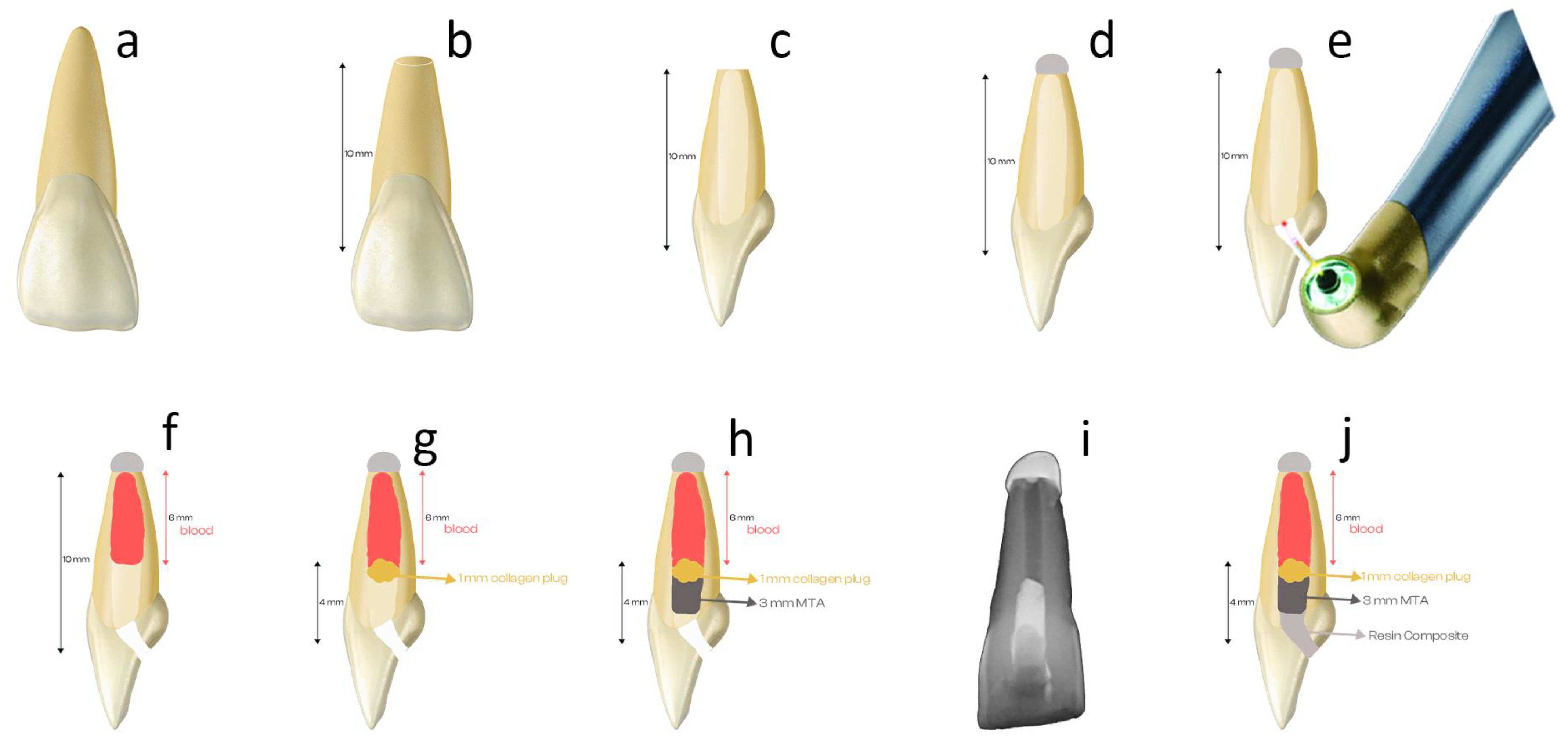
2.2. Preparation of Specimens
2.3. Tooth Color Measurements
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Glynis, A.; Foschi, F.; Kefalou, I.; Koletsi, D.; Tzanetakis, G.N. Regenerative Endodontic Procedures for the Treatment of Necrotic Mature Teeth with Apical Periodontitis: A Systematic Review and Meta-analysis of Randomized Controlled Trials. J. Endod. 2021, 47, 873–882. [Google Scholar] [CrossRef]
- Diogenes, A.H.M.; Teizeira, F.B.; Hargreaves, K.M. An update on clinical regenerative endodontics. Endod. Top. 2013, 28, 2–23. [Google Scholar] [CrossRef]
- Chen, S.J.; Karabucak, B.; Steffen, J.J.; Yu, Y.H.; Kohli, M.R. Spectrophotometric Analysis of Coronal Tooth Discoloration Induced by Tricalcium Silicate Cements in the Presence of Blood. J. Endod. 2020, 46, 1913–1919. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.G.; Malek, M.; Sigurdsson, A.; Lin, L.M.; Kahler, B. Regenerative endodontics: A comprehensive review. Int. Endod. J. 2018, 51, 1367–1388. [Google Scholar] [CrossRef] [PubMed]
- Santos, L.; Chisini, L.A.; Springmann, C.G.; Souza, B.D.M.; Pappen, F.G.; Demarco, F.F.; Felippe, M.C.S.; Felippe, W.T. Alternative to Avoid Tooth Discoloration after Regenerative Endodontic Procedure: A Systematic Review. Braz. Dent. J. 2018, 29, 409–418. [Google Scholar] [CrossRef]
- Taweewattanapaisan, P.; Jantarat, J.; Ounjai, P.; Janebodin, K. The Effects of EDTA on Blood Clot in Regenerative Endodontic Procedures. J. Endod. 2019, 45, 281–286. [Google Scholar] [CrossRef]
- Jesus, L.S.; Reis, T.; Machado, B.; Costa, A.; Savaris, J.M.; Volpato, C.A.M.; Bortoluzzi, E.A.; Teixeira, C.D.S.; Fernandes, P.; Garcia, L. Dental and composite resin discoloration induced by different hydraulic calcium silicate-based cements: Two-year in vitro assessment. J. Appl. Oral Sci. 2023, 31, e20220444. [Google Scholar] [CrossRef]
- Samra, A.P.; Pereira, S.K.; Delgado, L.C.; Borges, C.P. Color stability evaluation of aesthetic restorative materials. Braz. Oral Res. 2008, 22, 205–210. [Google Scholar] [CrossRef]
- Adl, A.; Javanmardi, S.; Abbaszadegan, A. Assessment of tooth discoloration induced by biodentine and white mineral trioxide aggregate in the presence of blood. J. Conserv. Dent. 2019, 22, 164–168. [Google Scholar]
- Marconyak, L.J., Jr.; Kirkpatrick, T.C.; Roberts, H.W.; Roberts, M.D.; Aparicio, A.; Himel, V.T.; Sabey, K.A. A Comparison of Coronal Tooth Discoloration Elicited by Various Endodontic Reparative Materials. J. Endod. 2016, 42, 470–473. [Google Scholar] [CrossRef] [PubMed]
- Fundaoglu Kucukekenci, F.; Kucukekenci, A.S.; Cakici, F. Evaluation of the preventive efficacy of three dentin tubule occlusion methods against discoloration caused by triple-antibiotic paste. Odontology 2019, 107, 186–189. [Google Scholar] [CrossRef] [PubMed]
- Shokouhinejad, N.; Khoshkhounejad, M.; Alikhasi, M.; Bagheri, P.; Camilleri, J. Prevention of coronal discoloration induced by regenerative endodontic treatment in an ex vivo model. Clin. Oral Investig. 2018, 22, 1725–1731. [Google Scholar] [CrossRef] [PubMed]
- Akbari, M.; Rouhani, A.; Samiee, S.; Jafarzadeh, H. Effect of dentin bonding agent on the prevention of tooth discoloration produced by mineral trioxide aggregate. Int. J. Dent. 2012, 2012, 563203. [Google Scholar] [CrossRef]
- Cattoni, F.; Ferrante, L.; Mandile, S.; Tete, G.; Polizzi, E.M.; Gastaldi, G. Comparison of Lasers and Desensitizing Agents in Dentinal Hypersensitivity Therapy. Dent. J. 2023, 11, 63. [Google Scholar] [CrossRef]
- Kurt, S.; Kirtiloglu, T.; Yilmaz, N.A.; Ertas, E.; Orucoglu, H. Evaluation of the effects of Er:YAG laser, Nd:YAG laser, and two different desensitizers on dentin permeability: In Vitro study. Lasers Med. Sci. 2018, 33, 1883–1890. [Google Scholar] [CrossRef] [PubMed]
- Lopes, A.O.; Aranha, A.C. Comparative evaluation of the effects of Nd:YAG laser and a desensitizer agent on the treatment of dentin hypersensitivity: A clinical study. Photomed. Laser Surg. 2013, 31, 132–138. [Google Scholar] [CrossRef]
- De Jesus, L.S.; Volpato, C.A.M.; Bortoluzzi, E.A.; da Silveira Teixeira, C.; Rossetto, H.L.; de Carvalho Panzeri Pires-de-Souza, F.; da Fonseca Roberti Garcia, L. Tooth discoloration induced by the different phases of a calcium aluminate cement: One-year assessment. J. Esthet. Restor. Dent. 2021, 33, 999–1009. [Google Scholar] [CrossRef] [PubMed]
- Khedmat, S.; Ahmadi, E.; Meraji, N.; Fallah, Z.F. Colorimetric Comparison of Internal Bleaching with and without Removing Mineral Trioxide Aggregate (MTA) on Induced Coronal Tooth Discoloration by MTA. Int. J. Dent. 2021, 2021, 8319986. [Google Scholar] [CrossRef]
- Nagas, E.; Ertan, A.; Eymirli, A.; Uyanik, O.; Cehreli, Z.C. Tooth Discoloration Induced by Different Calcium Silicate-Based Cements: A Two-Year Spectrophotometric and Photographic Evaluation in vitro. J. Clin. Pediatr. Dent. 2021, 45, 112–116. [Google Scholar] [CrossRef]
- Palma, P.J.; Marques, J.A.; Santos, J.; Falacho, R.I.; Sequeira, D.; Diogo, P.; Caramelo, F.; Ramos, J.C.; Santos, J.M. Tooth Discoloration after Regenerative Endodontic Procedures with Calcium Silicate-Based Cements—An Ex Vivo Study. Appl. Sci. 2020, 10, 5793. [Google Scholar] [CrossRef]
- Ates, M.O.; Ugur Aydin, Z. Evaluation of the effectiveness of different treatment approaches in preventing coronal discoloration caused by regenerative endodontic treatment. Clin. Oral Investig. 2023, 27, 4595–4603. [Google Scholar] [CrossRef]
- Choi, Y.L.; Jang, Y.E.; Kim, B.S.; Kim, J.W.; Kim, Y. Pre-application of dentin bonding agent prevents discoloration caused by mineral trioxide aggregate. BMC Oral Health 2020, 20, 163. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Da Silva, V.A.; Da Silva, S.A.; Pecho, O.E.; Bacchi, A. Influence of composite type and light irradiance on color stability after immersion in different beverages. J. Esthet. Restor. Dent. 2018, 30, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Paravina, R.D.; Ghinea, R.; Herrera, L.J.; Bona, A.D.; Igiel, C.; Linninger, M.; Sakai, M.; Takahashi, H.; Tashkandi, E.; Perez Mdel, M. Color difference thresholds in dentistry. J. Esthet. Restor. Dent. 2015, 27 (Suppl. S1), S1–S9. [Google Scholar] [CrossRef] [PubMed]
- Ghisi, A.C.; Kopper, P.M.; Baldasso, F.E.; Sturmer, C.P.; Rossi-Fedele, G.; Steier, L.; de Figueiredo, J.A.; Morgental, R.D.; Vier-Pelisser, F.V. Effect of superoxidized water and sodium hypochlorite, associated or not with EDTA, on organic and inorganic components of bovine root dentin. J. Endod. 2015, 41, 925–930. [Google Scholar] [CrossRef]
- Zou, L.; Shen, Y.; Li, W.; Haapasalo, M. Penetration of sodium hypochlorite into dentin. J. Endod. 2010, 36, 793–796. [Google Scholar] [CrossRef]
- Kang, S.H.; Shin, Y.S.; Lee, H.S.; Kim, S.O.; Shin, Y.; Jung, I.Y.; Song, J.S. Color changes of teeth after treatment with various mineral trioxide aggregate-based materials: An ex vivo study. J. Endod. 2015, 41, 737–741. [Google Scholar] [CrossRef]
- Valles, M.; Roig, M.; Duran-Sindreu, F.; Martinez, S.; Mercade, M. Color Stability of Teeth Restored with Biodentine: A 6-month In Vitro Study. J. Endod. 2015, 41, 1157–1160. [Google Scholar] [CrossRef]
- Mozynska, J.; Metlerski, M.; Lipski, M.; Nowicka, A. Tooth Discoloration Induced by Different Calcium Silicate-based Cements: A Systematic Review of In Vitro Studies. J. Endod. 2017, 43, 1593–1601. [Google Scholar] [CrossRef] [PubMed]
- Chu, S.J.; Paravina, R.D.; Saaler, I.; Maeleszko, A.J. Color in Dentistry: A Clinical Guide to Predictable Esthetics, 1st ed.; Quintessence Publishing: New Malden, UK, 2017. [Google Scholar]
- Paravina, R.D.; Perez, M.M.; Ghinea, R. Acceptability and perceptibility thresholds in dentistry: A comprehensive review of clinical and research applications. J. Esthet. Restor. Dent. 2019, 31, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Nahsan, F.P.; Mondelli, R.F.; Franco, E.B.; Naufel, F.S.; Ueda, J.K.; Schmitt, V.L.; Baseggio, W. Clinical strategies for esthetic excellence in anterior tooth restorations: Understanding color and composite resin selection. J. Appl. Oral Sci. 2012, 20, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Schembri, M.; Peplow, G.; Camilleri, J. Analyses of heavy metals in mineral trioxide aggregate and Portland cement. J. Endod. 2010, 36, 1210–1215. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, H.; Liang, Y.; Xiang, S.; Li, H.; Dai, X.; Zhao, W. Dentinal tubule occlusion using Er:YAG Laser: An in vitro study. J. Appl. Oral Sci. 2021, 29, e20200266. [Google Scholar] [CrossRef]
- Sesen Uslu, Y.; Donmez, N. The effects on dentin tubules of two desensitising agents in combination with Nd:YAG laser: An in vitro analysis (CLSM and SEM). Opt. Laser Technol. 2020, 129, 106225. [Google Scholar] [CrossRef]
- Lan, W.H.; Liu, H.C. Treatment of dentin hypersensitivity by Nd:YAG laser. J. Clin. Laser Med. Surg. 1996, 14, 89–92. [Google Scholar] [CrossRef]
- White, J.M.; Goodis, H.E.; Setcos, J.C.; Eakle, S.; Hulscher, B.E.; Rose, C.L. Effects of pulsed Nd:YAG laser energy on human teeth: A three-year follow-up study. J. Am. Dent. Assoc. 1993, 124, 45–51. [Google Scholar] [CrossRef]
- Oncu, E.; Karabekiroglu, S.; Unlu, N. Effects of different desensitizers and lasers on dentine tubules: An in-vitro analysis. Microsc. Res. Tech. 2017, 80, 737–744. [Google Scholar] [CrossRef]
- Schwarz, F.; Arweiler, N.; Georg, T.; Reich, E. Desensitizing effects of an Er:YAG laser on hypersensitive dentine. J. Clin. Periodontol. 2002, 29, 211–215. [Google Scholar] [CrossRef]
- Okur, E.; Eyuboglu, G.B. Evaluation of Dentin Tubule Plugging Efficiencies and Effects on Dentin Surface Roughness of Dentin Desensitizing Agents, the Er,Cr:YSGG Laser, and Their Combination After Erosion-abrasion Cycles: An In Vitro Study. Oper. Dent. 2022, 47, E35–E51. [Google Scholar] [CrossRef]
- Gholami, G.A.; Fekrazad, R.; Esmaiel-Nejad, A.; Kalhori, K.A. An evaluation of the occluding effects of Er;Cr:YSGG, Nd:YAG, CO(2) and diode lasers on dentinal tubules: A scanning electron microscope in vitro study. Photomed. Laser Surg. 2011, 29, 115–121. [Google Scholar] [CrossRef]
- Aranha, A.C.; Eduardo Cde, P. In Vitro effects of Er,Cr:YSGG laser on dentine hypersensitivity. Dentine permeability and scanning electron microscopy analysis. Lasers Med. Sci. 2012, 27, 827–834. [Google Scholar] [CrossRef] [PubMed]
- Meng, Y.; Huang, F.; Wang, S.; Huang, X.; Lu, Y.; Li, Y.; Dong, Y.; Pei, D. Evaluation of dentinal tubule occlusion and pulp tissue response after using 980-nm diode laser for dentin hypersensitivity treatment. Clin. Oral Investig. 2023, 27, 4843–4854. [Google Scholar] [CrossRef] [PubMed]
- Sgolastra, F.; Petrucci, A.; Severino, M.; Gatto, R.; Monaco, A. Lasers for the treatment of dentin hypersensitivity: A meta-analysis. J. Dent. Res. 2013, 92, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Umana, M.; Heysselaer, D.; Tielemans, M.; Compere, P.; Zeinoun, T.; Nammour, S. Dentinal tubules sealing by means of diode lasers (810 and 980 nm): A preliminary in vitro study. Photomed. Laser Surg. 2013, 31, 307–314. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | n | ΔE1 (T0–T1) Mean ± SEM | ΔE2 (T0–T2) Mean ± SEM | ΔE3 (T0–T3) Mean ± SEM | ΔE4 (T0–T4) Mean ± SEM | Group | p Time | Group*Time |
|---|---|---|---|---|---|---|---|---|
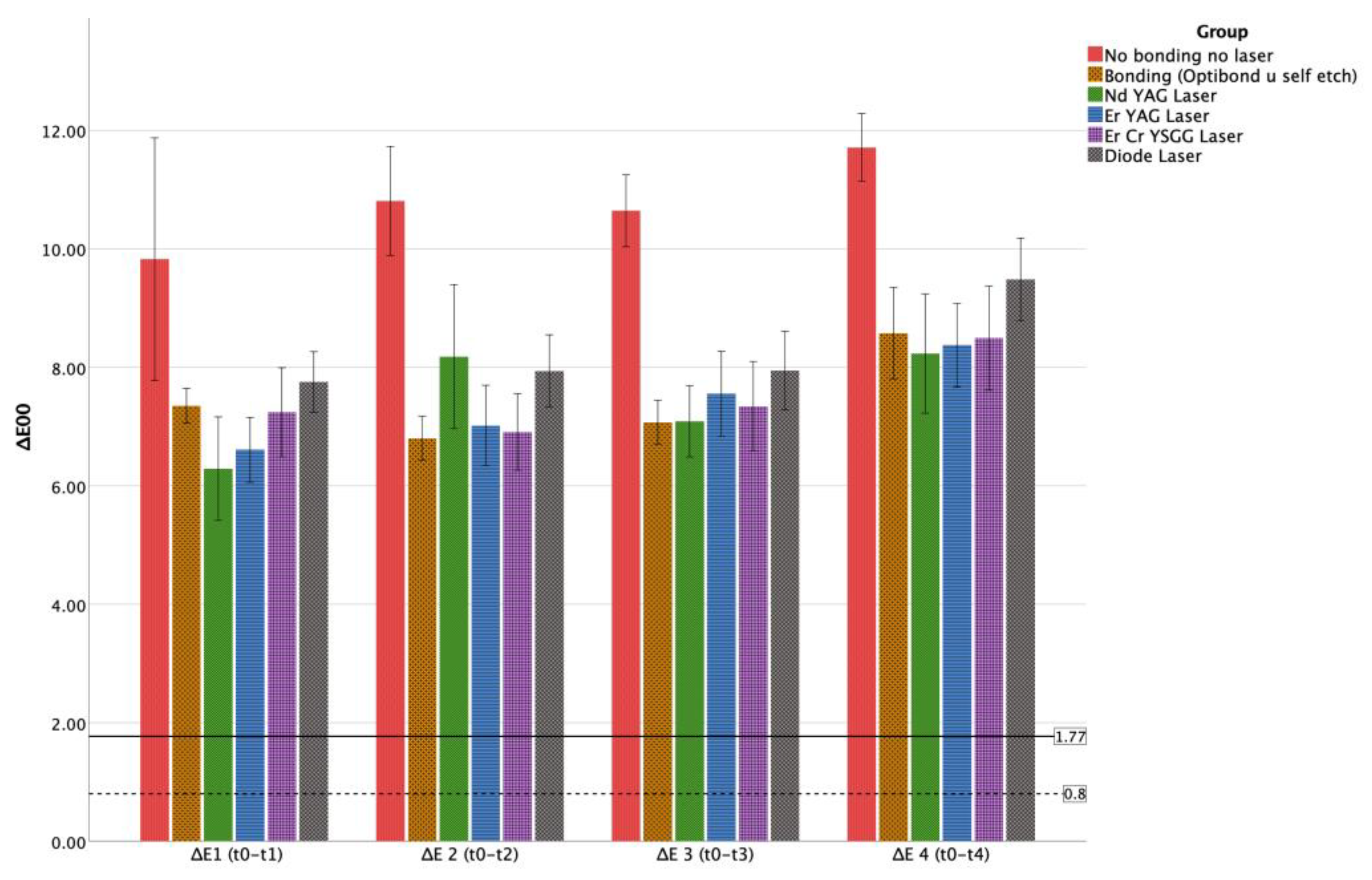
| Control | 10 | 9.83 ± 2.05 a,B | 10.81 ± 0.92 a,B | 10.64 ± 0.61 a,B | 11.71 ± 0.57 a,A | <0.001 | 0.002 | 0.977 |
| DBA | 10 | 7.35 ± 0.29 b,B | 6.8 ± 0.37 b,B | 7.07 ± 0.37 b,B | 8.58 ± 0.77 b,A | |||
| Nd YAG Laser | 10 | 6.29 ± 0.87 b,B | 8.18 ± 1.22 b,B | 7.09 ± 0.6 b,B | 8.23 ± 1.01 b,A | |||
| Er YAG Laser | 10 | 6.61 ± 0.55 b,B | 7.02 ± 0.68 b,B | 7.55 ± 0.72 b,B | 8.37 ± 0.7 b,A | |||
| Er Cr YSGG Laser | 10 | 7.24 ± 0.75 b,B | 6.91 ± 0.65 b,B | 7.34 ± 0.75 b,B | 8.49 ± 0.88 b,A | |||
| Diode Laser | 10 | 7.75 ± 0.51 b,B | 7.94 ± 0.61 b,B | 7.95 ± 0.66 b,B | 9.48 ± 0.7 b,A |
| Measurement | Time | Mean ± SEM | Median (Min.–Max.) |
|---|---|---|---|
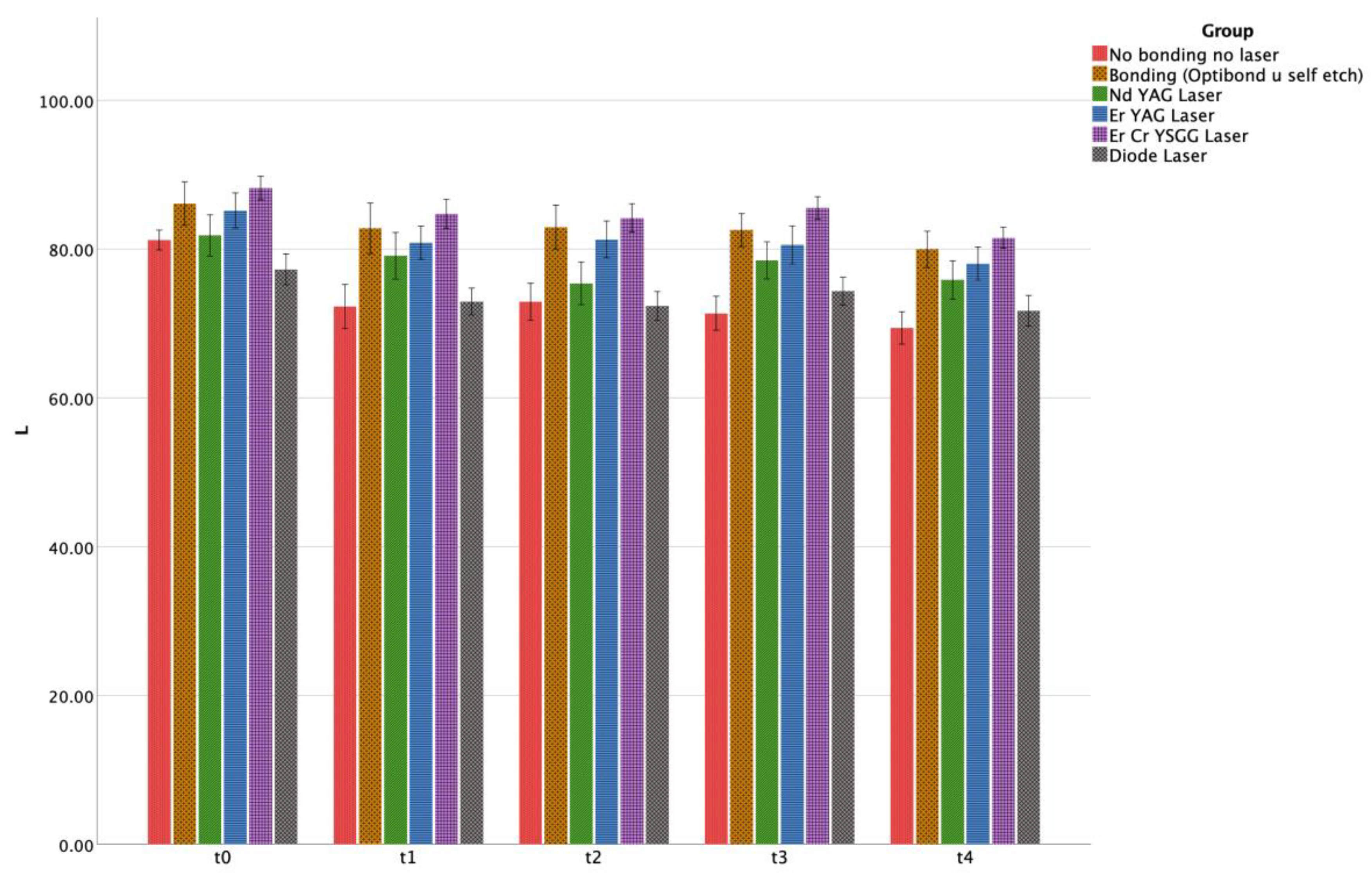
| L | T0 | 83.3 ± 1 | 84.4 (62.35–99.6) |
| T1 | 78.78 ± 1.2 | 78.93 (60.65–95.95) | |
| T2 | 78.18 ± 1.15 | 79.43 (61–97.4) | |
| T3 | 78.8 ± 1.06 | 81.1 (61.6–91.75) | |
| T4 | 76.08 ± 1.02 | 77.2 (63.05–90.05) | |
| a | T0 | 5.78 ± 0.38 | 5.25 (0.3–14) |
| T1 | 2.6 ± 0.32 | 1.88 (0.05–10) | |
| T2 | 1.88 ± 0.16 | 1.63 (0.25–5.95) | |
| T3 | 1.6 ± 0.15 | 1.28 (0–5.1) | |
| T4 | 1.33 ± 0.12 | 1.08 (0.15–3.9) | |
| b | T0 | 42.68 ± 0.68 | 42.58 (30.9–51.1) |
| T1 | 28.84 ± 0.77 | 27.98 (16.2–41.15) | |
| T2 | 28.59 ± 0.7 | 27.9 (15.1–40.1) | |
| T3 | 28.58 ± 0.7 | 28.05 (17.2–42.3) | |
| T4 | 27.18 ± 0.66 | 26.88 (16.9–41) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sesen Uslu, Y.; Arıcan Alpay, B.; Sesen, P.; Özyürek, T. The Efficacy of Different Laser Applications on Dentin Sealing in Preventing Discoloration Induced by Mineral Trioxide Aggregate. Materials 2024, 17, 1015. https://doi.org/10.3390/ma17051015
Sesen Uslu Y, Arıcan Alpay B, Sesen P, Özyürek T. The Efficacy of Different Laser Applications on Dentin Sealing in Preventing Discoloration Induced by Mineral Trioxide Aggregate. Materials. 2024; 17(5):1015. https://doi.org/10.3390/ma17051015
Chicago/Turabian StyleSesen Uslu, Yesim, Burçin Arıcan Alpay, Pinar Sesen, and Taha Özyürek. 2024. "The Efficacy of Different Laser Applications on Dentin Sealing in Preventing Discoloration Induced by Mineral Trioxide Aggregate" Materials 17, no. 5: 1015. https://doi.org/10.3390/ma17051015