
Zirconia versus Titanium Implants: 8-Year Follow-Up in a Patient Cohort Contrasted with Histological Evidence from a Preclinical Animal Model


Abstract
:1. Introduction
2. Materials and Methods
- Implant success was evaluated using four-field tables with the categories of success, survival, unaccounted for, and failure as per the criteria defined at the start of the trial, except that the palatal implants were defined as “surviving” since they could not have radiographic bone levels measured. Implants meeting the success criteria exhibited less than 1 mm bone loss during the first year and less than 2.4 mm over the subsequent seven years (<0.2 mm/year) and were free of mobility, pain, and neuropathy. Implants that were still functioning but did not meet the success criteria were considered as surviving. Implants in patients who dropped out of the study for any reason were considered unaccounted for. Deceased patients were included within the “unaccounted for” classification. An implant removed for any reason was considered a failure.
- Peri-implant marginal bone levels were only recorded for the six alveolar implants; the palatal implants were excluded. Radiographs were evaluated using image analysis software (Image J 1.34S; National Institutes of Health, Bethesda, MD, USA). Measurements of mesial and distal surfaces for each group were averaged and compared statistically.
- Peri-implant soft-tissue parameters, including probing depths, recession, and bleeding at four sites per implant, were only recorded for the six alveolar implants; the palatal implants were excluded. Pocket depths, recession, attachment loss, and percent bleeding scores were averaged for each group and compared statistically.
3. Anaesthesia Technique for All Surgical Procedures
3.1. Animal Euthanasia for Implants Retrieval
3.2. Statistical Analysis
4. Results
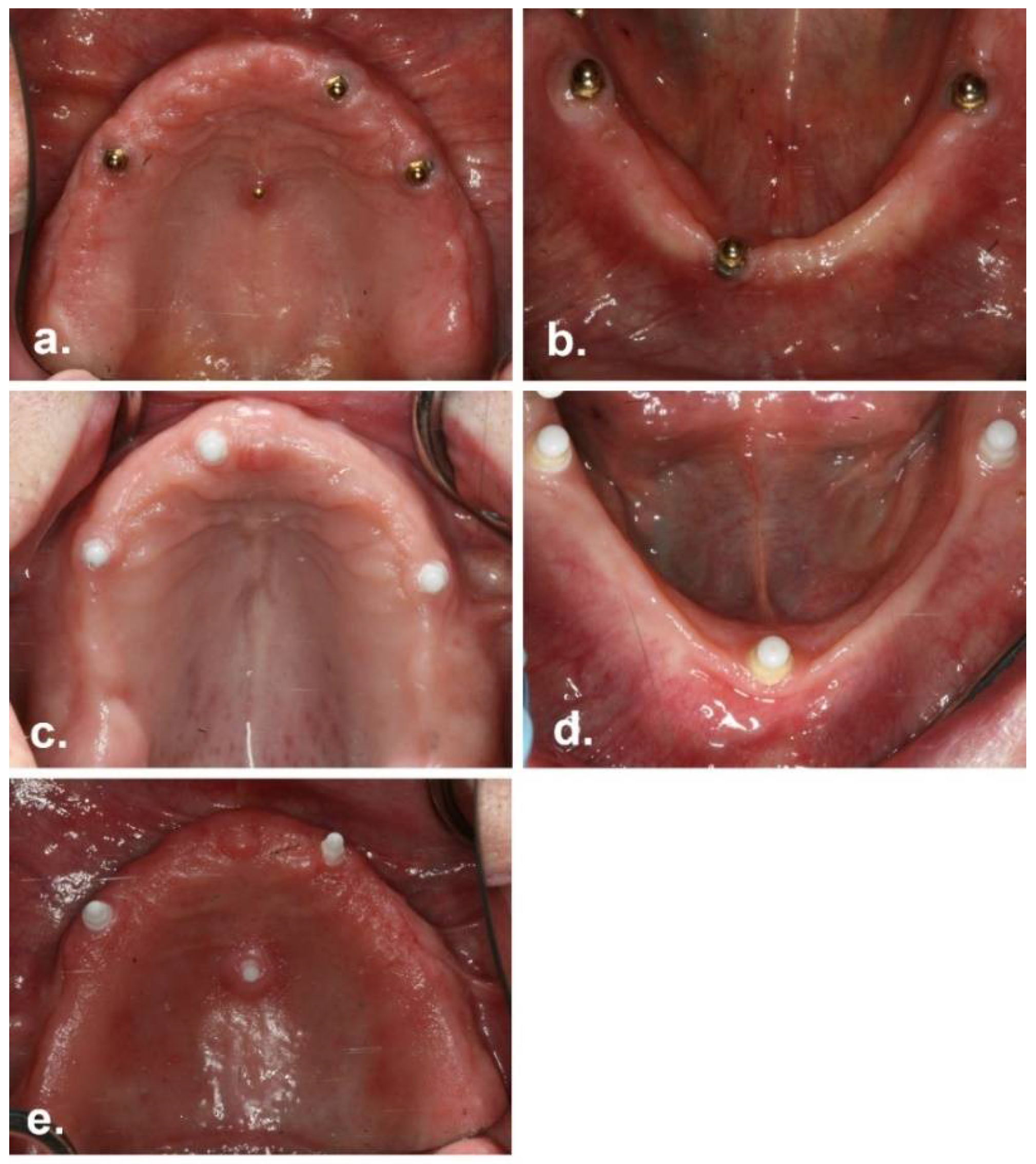
5. Implant Outcomes in the Recalled Patients
6. Peri-Implant Soft-Tissue Status
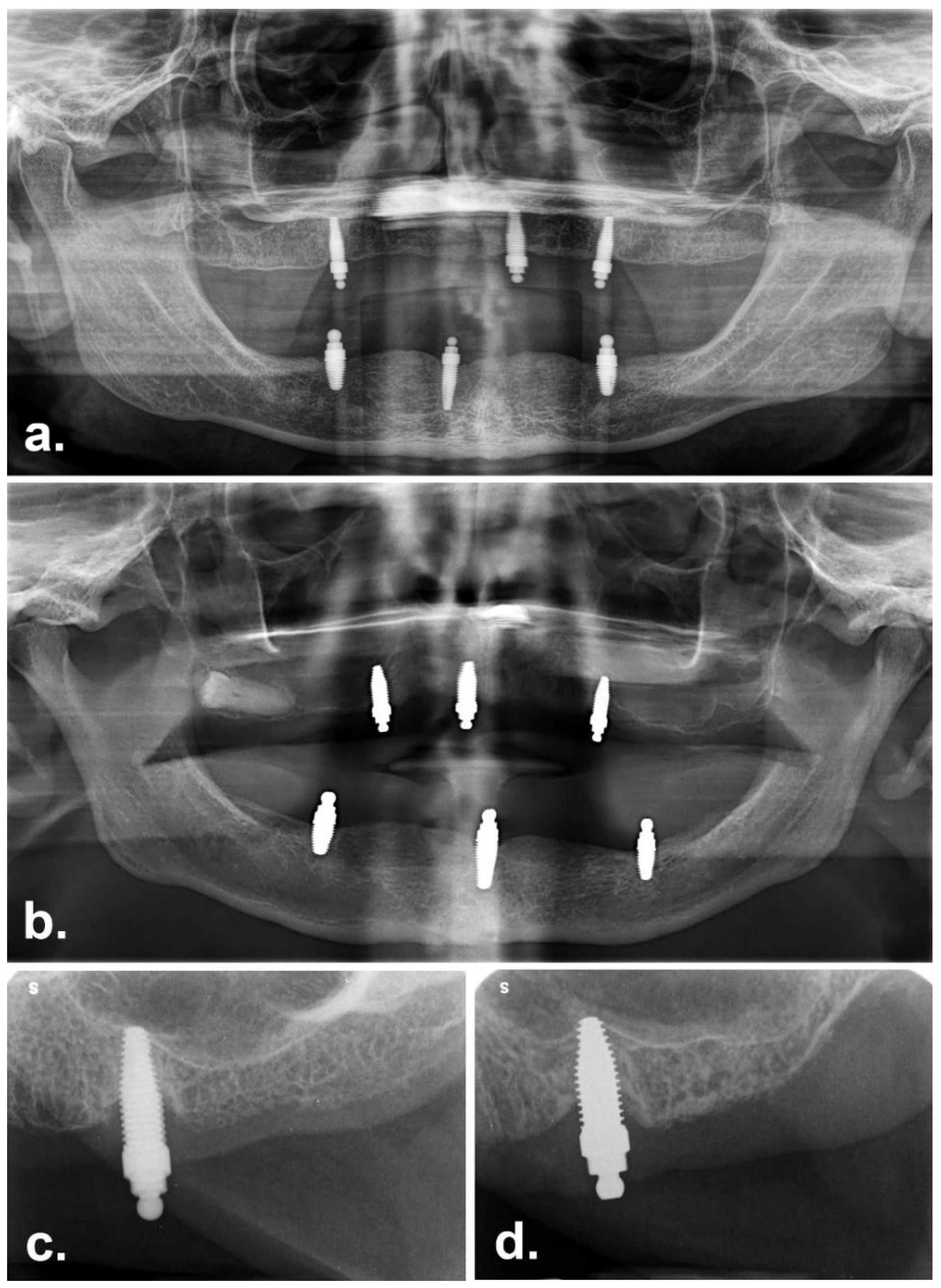
7. Radiographic Bone Level
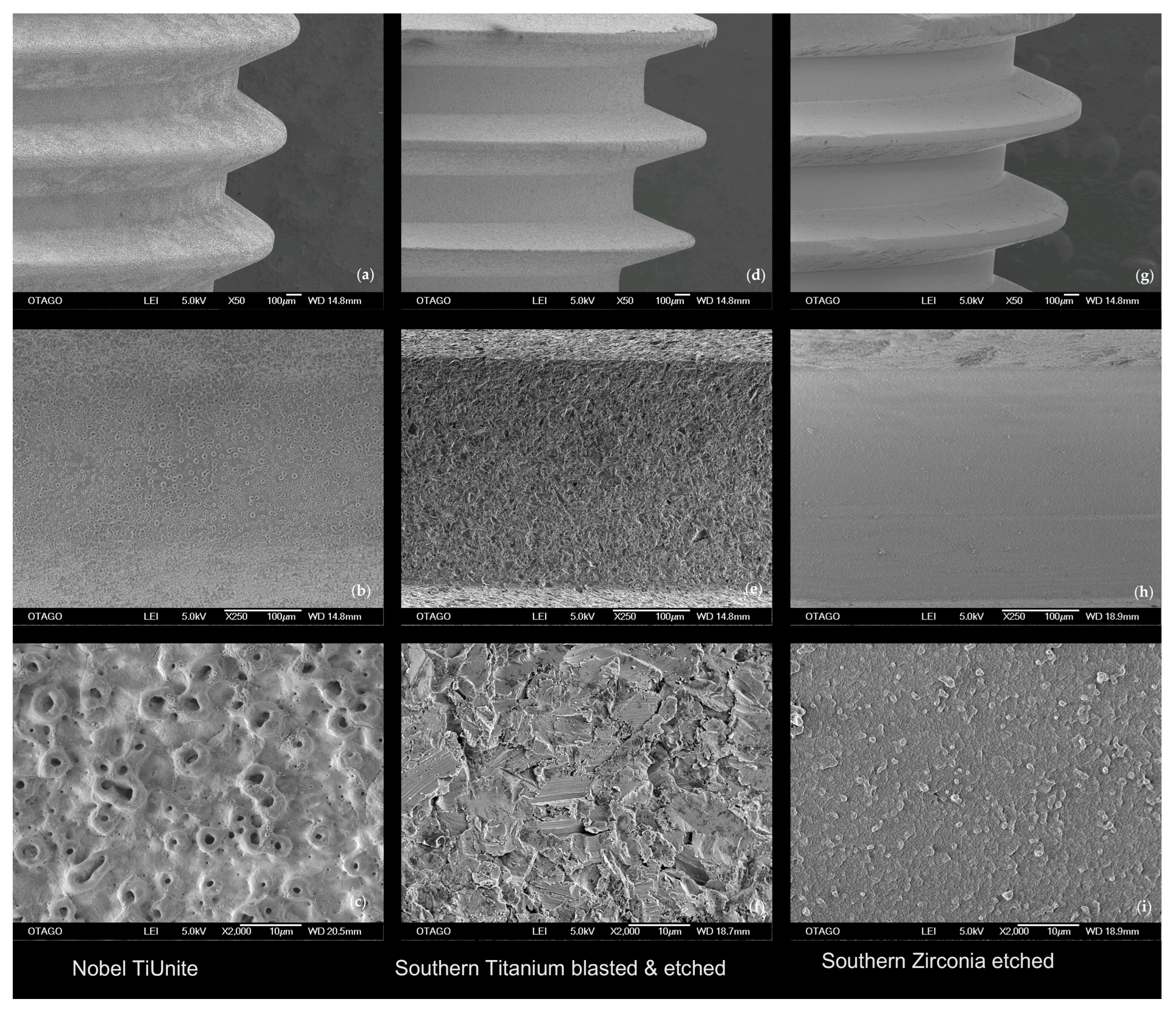
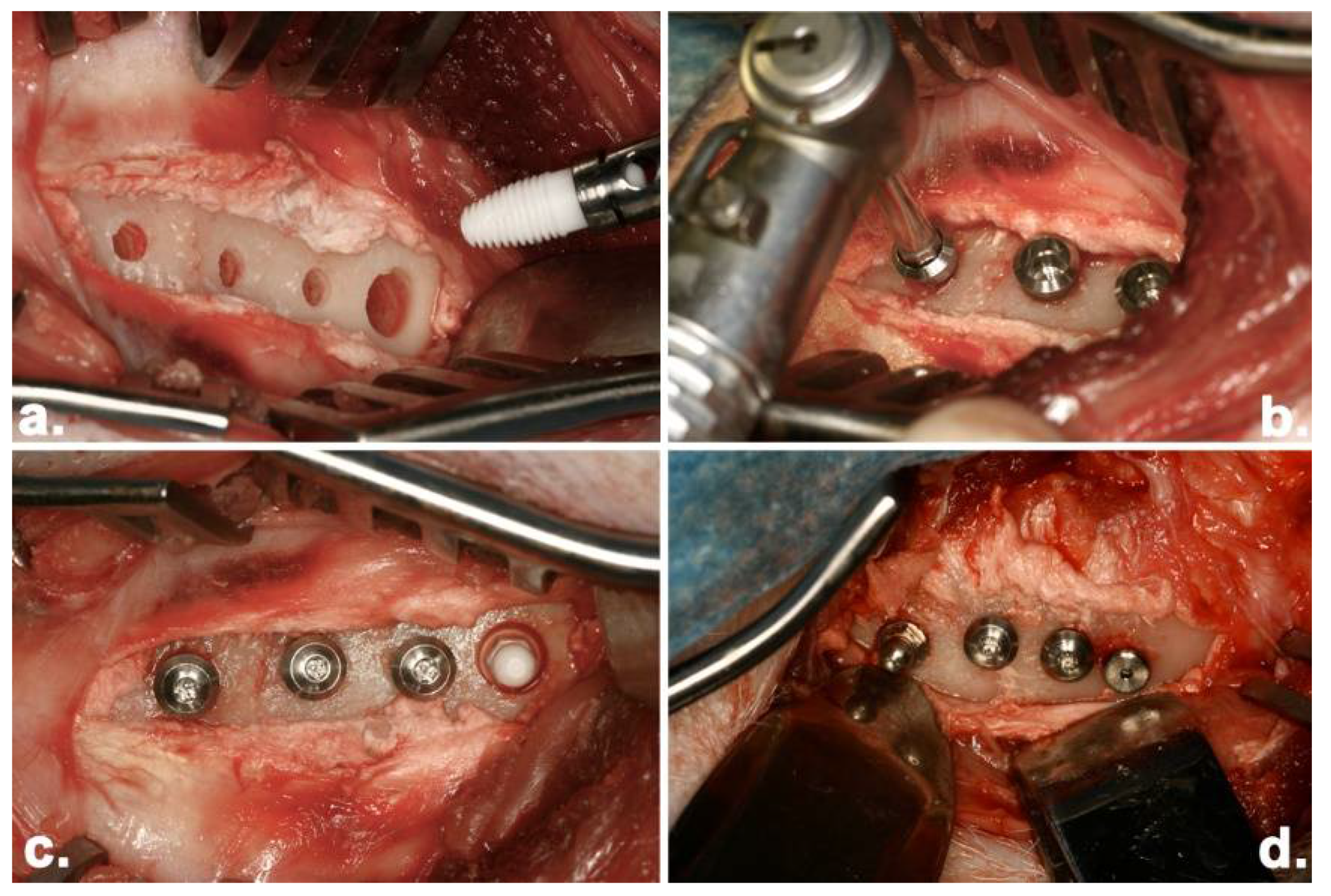
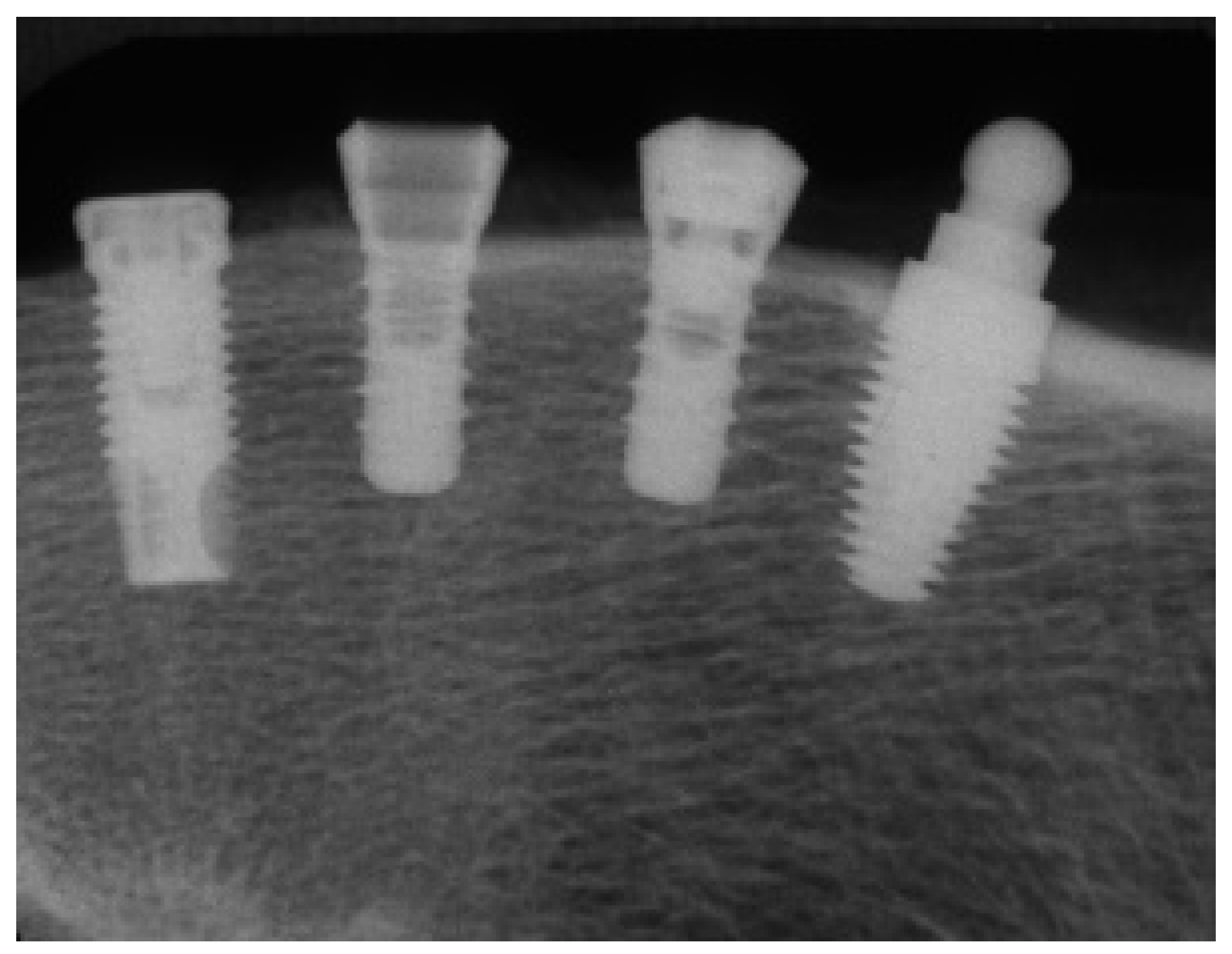
8. Preclinical Study
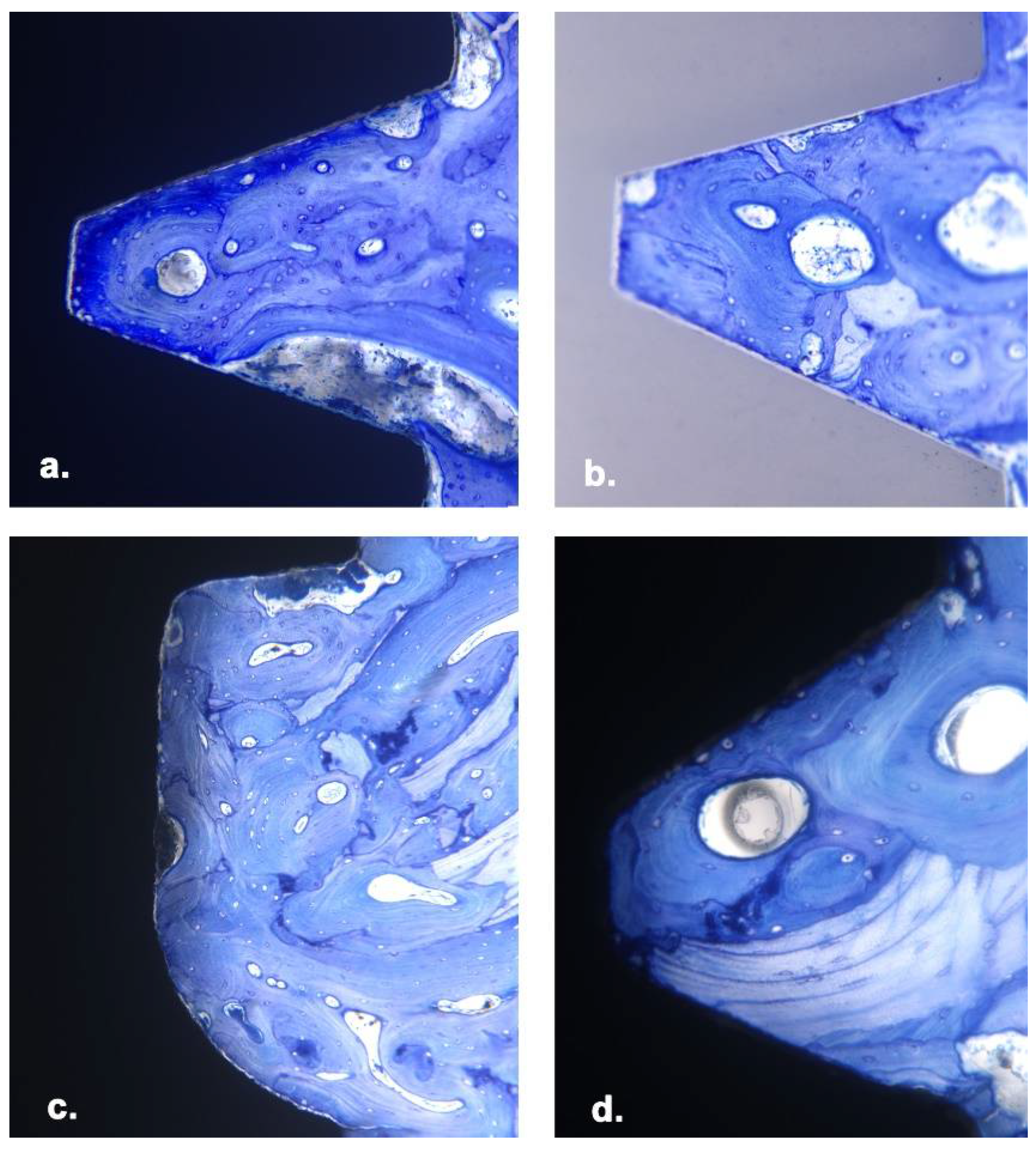
9. Histomorphometry
10. Discussion
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Edelhoff, D.; Schweiger, J.; Prandtner, O.; Stimmelmayr, M.; Güth, J.F. Metal-Free Implant-Supported Single-Tooth Restorations. Part I: Abutments and Cemented Crowns. Quintessence Int. 2019, 50, 176. [Google Scholar]
- Poggio, C.E.; Ercoli, C.; Rispoli, L.; Maiorana, C.; Esposito, M. Metal-Free Materials for Fixed Prosthodontic Restorations. Cochrane Database Syst. Rev. 2017, 20, CD009606. [Google Scholar] [CrossRef] [PubMed]
- Sadowsky, S.J. Has Zirconia Made a Material Difference in Implant Prosthodontics? A Review. Dent. Mater. 2020, 36, 1. [Google Scholar] [CrossRef]
- Cionca, N.; Hashim, D.; Mombelli, A. Zirconia Dental Implants: Where Are We Now, And Where Are We Heading? Periodontol. 2000 2017, 73, 241. [Google Scholar] [CrossRef]
- Siddiqi, A.; Payne, A.G.T.; De Silva, R.K.; Duncan, W.J. Titanium Allergy: Could It Affect Dental Implant Integration? Clin. Oral Implant. Res. 2011, 22, 673. [Google Scholar] [CrossRef]
- Tawse-Smith, A.; Ma, S.; Duncan, W.J.; Gray, A.; Reid, M.R.; Rich, A.M. Implications of Wear at the Titanium-Zirconia Implant-Abutment Interface on the Health of Peri-implant Tissues. Int. J. Oral Maxillofac. Implant. 2017, 32, 599. [Google Scholar] [CrossRef] [Green Version]
- Berryman, Z.; Bridger, L.; Hussaini, H.M.; Rich, A.M.; Atieh, M.; Tawse-Smith, A. Titanium Particles: An Emerging Risk Factor for Peri-Implant Bone Loss. Saudi Dent. J. 2020, 32, 283. [Google Scholar] [CrossRef]
- Osman, R.B.; Ma, S.; Duncan, W.; De Silva, R.K.; Siddiqi, A.; Swain, M.V. Fractured Zirconia Implants and Related Implant Designs: Scanning Electron Microscopy Analysis. Clin. Oral Implant. Res. 2013, 24, 592. [Google Scholar] [CrossRef]
- Osman, R.B.; Swain, M.V. A Critical Review of Dental Implant Materials with an Emphasis on Titanium versus Zirconia. Materials 2015, 5, 932. [Google Scholar] [CrossRef] [Green Version]
- Bormann, K.H.; Gellrich, N.C.; Kniha, H.; Schild, S.; Weingart, D.; Gahlert, M. A Prospective Clinical Study to Evaluate the Performance of Zirconium Dioxide Dental Implants in Single-Tooth Edentulous Area: 3-Year Follow-Up. BMC Oral Health 2018, 18, 181. [Google Scholar] [CrossRef] [Green Version]
- Sailer, I.; Karasan, D.; Todorovic, A.; Ligoutsikou, M.; Pjetursson, B.E. Prosthetic Failures in Dental Implant Therapy. Periodontol. 2000 2022, 88, 130. [Google Scholar] [CrossRef]
- Jank, S.; Hochgatterer, G. Success Rate of Two-Piece Zirconia Implants: A Retrospective Statistical Analysis. Implant. Dent. 2016, 25, 193. [Google Scholar] [CrossRef] [PubMed]
- Cionca, N.; Hashim, D.; Mombelli, A. Two-Piece Zirconia Implants Supporting All-Ceramic Crowns: Six-Year Results of a Prospective Cohort Study. Clin. Oral Implant. Res. 2021, 32, 695. [Google Scholar] [CrossRef]
- Pieralli, S.; Kohal, R.J.; Jung, R.E.; Vach, K.; Spies, B.C. Clinical Outcomes of Zirconia Dental Implants: A Systematic Review. J. Dent. Res. 2017, 96, 38. [Google Scholar] [CrossRef]
- Koller, M.; Steyer, E.; Theisen, K.; Stagnell, S.; Jakse, N.; Payer, M. Two-Piece Zirconia versus Titanium Implants After 80 Months: Clinical Outcomes from a Prospective Randomized Pilot Trial. Clin. Oral Implant. Res. 2020, 31, 388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, E.V.F.; Commar, B.C.; Bitencourt, S.B.; Bonatto, L.R.; Dos Santos, D.M.; Bittencourt, A.B.B.C.; Goiato, M.C. Titanium versus Ceramic Implants for Overdentures: A Meta-Analysis of Prospective Studies. Gen. Dent. 2021, 69, e1. [Google Scholar]
- Osman, R.B.; Swain, M.V.; Atieh, M.; Ma, S.; Duncan, W. Ceramic Implants (Y-TZP): Are They a Viable Alternative to Titanium Implants for The Support of Overdentures? A Randomized Clinical Trial. Clin. Oral Implant. Res. 2014, 25, 1366. [Google Scholar] [CrossRef]
- Siddiqi, A.; Kieser, J.A.; De Silva, R.K.; Thomson, W.M.; Duncan, W.J. Soft and Hard Tissue Response to Zirconia versus Titanium One-Piece Implants Placed in Alveolar and Palatal Sites: A Randomized Control Trial. Clin. Implant. Dent. Relat. Res. 2015, 17, 483. [Google Scholar] [CrossRef]
- Siddiqi, A.; Khan, A.S.; Zafar, S. Thirty Years of Translational Research in Zirconia Dental Implants: A Systematic Review of The Literature. J. Oral Implant. 2017, 43, 314. [Google Scholar] [CrossRef]
- Thomé, G.; Sandgren, R.; Bernardes, S.; Trojan, L.; Warfving, N.; Bellón, B.; Pippenger, B.E. Osseointegration of A Novel Injection Molded 2-Piece Ceramic Dental Implant: A Study in Minipigs. Clin. Oral Investig. 2021, 25, 603. [Google Scholar] [CrossRef]
- Chacun, D.; Lafon, A.; Courtois, N.; Reveron, H.; Chevalier, J.; Margossian, P.; Alves, A.; Gritsch, K.; Grosgogeat, B. Histologic and Histomorphometric Evaluation of New Zirconia-Based Ceramic Dental Implants: A Preclinical Study in Dogs. Dent. Mater. 2021, 37, 1377. [Google Scholar] [CrossRef] [PubMed]
- Janner, S.F.M.; Gahlert, M.; Bosshardt, D.D.; Roehling, S.; Milz, S.; Higginbottom, F.; Buser, D.; Cochran, D.L. Bone Response to Functionally Loaded.; Two-Piece Zirconia Implants: A Preclinical Histometric Study. Clin. Oral Implant. Res. 2018, 29, 277. [Google Scholar] [CrossRef]
- Siddiqi, A.; Duncan, W.J.; De Silva, R.K.; Zafar, S. One-Piece Zirconia Ceramic versus Titanium Implants in the Jaw and Femur of a Sheep Model: A Pilot Study. BioMed Res. Int. 2016, 2016, 6792972. [Google Scholar] [CrossRef] [Green Version]
- Osman, R.B.; Ma, S. Prosthodontic Maintenance of Overdentures on Zirconia Implants: 1-Year Results of a Randomized Controlled Trial. Int J. Prosthodont. 2014, 27, 461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT. CONSORT 2010 Explanation and Elaboration: Updated Guidelines for Reporting Parallel Group Randomised Trials. Int. J. Surg. 2012, 10, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albrektsson, T.; Zarb, G.A. Current Interpretations of the Osseointegrated Response: Clinical Significance. Int. J. Prosthodont. 1993, 6, 95. [Google Scholar]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-Implant Diseases and Conditions: Consensus Report of Workgroup 4 Of The 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chappard, D.; Aguado, E.; Huré, G.; Grizon, F.; Basle, M.F. The Early Remodeling Phases around Titanium Implants: A Histomorphometric Assessment of Bone Quality in A 3- And 6-Month Study in Sheep. Int. J. Oral Maxillofac. Implant. 1999, 14, 189. [Google Scholar]
- Duncan, W.J.; Lee, M.H.; Dovban, A.S.; Hendra, N.; Ershadi, S.; Rumende, H. Anodization Increases Early Integration of Osstem Implants in Sheep Femurs. Ann. R. Australas. Coll. Dent. Surg. 2008, 19, 152. [Google Scholar]
- Schenk, R.; Olah, A.; Herrmann, W. Preparation of Calcified Tissues for Light Microscopy. In Methods of Calcified Tissue Preparation; Dickson, G., Ed.; Elsevier: Amsterdam, The Netherlands, 1984. [Google Scholar]
- Hammerle, C.H.; Chiantella, G.C.; Karring, T.; Lang, N.P. The Effect of a Deproteinized Bovine Bone Mineral on Bone Regeneration Around Titanium Dental Implants. Clin. Oral Implant. Res. 1998, 9, 151. [Google Scholar] [CrossRef]
- Duncan, W. Sheep Mandibular Animal Models for Dental Implantology Research. Ph.D. Thesis, University of Otago, Dunedin, New Zealand, 2005. [Google Scholar]
- Sachdeo, A.; Haffajee, A.D.; Socransky, S.S. Biofilms in the Edentulous Oral Cavity. J. Prosthodont. 2008, 17, 348. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, C.B.; Aquino, D.R.; Franco, G.C.; Cortelli, S.C.; Costa, F.O.; Cortelli, J.R. Do Elderly Edentulous Patients with a History of Periodontitis Harbor Periodontal Pathogens? Clin. Oral Implant. Res. 2010, 21, 618. [Google Scholar] [CrossRef] [PubMed]
- Andjelkovic, M.; Sojic, L.T.; Lemic, A.M.; Nikolic, N.; Kannosh, I.Y.; Milasin, J. Does the Prevalence of Periodontal Pathogens Change in Elderly Edentulous Patients after Complete Denture Treatment? J. Prosthodont. 2017, 26, 364. [Google Scholar] [CrossRef]
- Kniha, K.; Milz, S.; Kniha, H.; Ayoub, N.; Hölzle, F.; Modabber, A. Peri-implant Crestal Bone Changes Around Zirconia Implants in Periodontally Healthy and Compromised Patients. Int. J. Oral Maxillofac. Implant. 2018, 33, 217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duncan, W.J.; Lee, M.H.; Bae, T.S.; Lee, S.J.; Gay, J.; Loch, C. Anodisation Increases Integration of Unloaded Titanium Implants in Sheep Mandible. BioMed Res. Int. 2015, 2015, 857969. [Google Scholar] [CrossRef]
- Duncan, W.J.; Gay, J.H.; Lee, M.H.; Bae, T.S.; Lee, S.J.; Loch, C. The Effect of Hydrothermal Spark Discharge Anodization in the Early Integration of Implants in Sheep Sinuses. Clin. Oral Implant. Res. 2016, 27, 975. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; McQuillan, A.J.; Shibata, Y.; Sharma, L.A.; Waddell, J.N.; Duncan, W.J. Histomorphometric and Histologic Evaluation of Titanium-Zirconium (Atizr) Implants with Anodized Surfaces. J. Mater. Sci. Mater. Med. 2016, 27, 86. [Google Scholar] [CrossRef]
- Lee, J.; Sieweke, J.H.; Rodriguez, N.A.; Schüpbach, P.; Lindström, H.; Susin, C.; Wikesjö, U.M. Evaluation of Nano-Technology-Modified Zirconia Oral Implants: A Study in Rabbits. J. Clin. Periodontol. 2009, 36, 610. [Google Scholar] [CrossRef]
- Kohal, R.J.; Knauf, M.; Larsson, B.; Sahlin, H.; Butz, F. One-Piece Zirconia Oral Implants: One-Year Results from a Prospective Cohort Study. 1. Single Tooth Replacement. J. Clin. Periodontol. 2012, 39, 590. [Google Scholar] [CrossRef] [PubMed]
- Kohal, R.J.; Spies, B.C.; Bauer, A.; Butz, F. One-Piece Zirconia Oral Implants for Single-Tooth Replacement: Three-Year Results from a Long-Term Prospective Cohort Study. J. Clin. Periodontol. 2018, 45, 114. [Google Scholar] [CrossRef] [Green Version]
- Hafezeqoran, A.; Koodaryan, R. Effect of Zirconia Dental Implant Surfaces on Bone Integration: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2017, 2017, 9246721. [Google Scholar] [CrossRef] [PubMed]
- Bacchelli, B.; Giavaresi, G.; Franchi, M.; Martini, D.; De Pasquale, V.; Trirè, A.; Fini, M.; Giardino, R.; Ruggeri, A. Influence of a Zirconia Sandblasting Treated Surface on Peri-Implant Bone Healing: An Experimental Study in Sheep. Acta Biomater. 2009, 5, 2246. [Google Scholar] [CrossRef] [PubMed]
- Langhoff, J.D.; Voelter, K.; Scharnweber, D.; Schnabelrauch, M.; Schlottig, F.; Hefti, T.; Kalchofner, K.; Nuss, K.; von Rechenberg, B. Comparison of Chemically and Pharmaceutically Modified Titanium and Zirconia Implant Surfaces in Dentistry: A Study in Sheep. Int. J. Oral Maxillofac. Surg. 2008, 37, 1125. [Google Scholar] [CrossRef] [PubMed]
- Koch, F.P.; Weng, D.; Krämer, S.; Biesterfeld, S.; Jahn-Eimermacher, A.; Wagner, W. Osseointegration of One-Piece Zirconia Implants Compared with A Titanium Implant of Identical Design: A Histomorphometric Study in the Dog. Clin. Oral Implant. Res. 2010, 21, 350. [Google Scholar] [CrossRef]
- Depprich, R.; Zipprich, H.; Ommerborn, M.; Naujoks, C.; Wiesmann, H.P.; Kiattavorncharoen, S.; Lauer, H.C.; Meyer, U.; Kübler, N.R.; Handschel, J. Osseointegration of Zirconia Implants Compared with Titanium: An In Vivo Study. Head Face Med. 2008, 4, 30. [Google Scholar] [CrossRef] [Green Version]
- Gredes, T.; Kubasiewicz-Ross, P.; Gedrange, T.; Dominiak, M.; Kunert-Keil, C. Comparison of Surface Modified Zirconia Implants with Commercially Available Zirconium and Titanium Implants: A Histological Study in Pigs. Implant. Dent. 2014, 23, 502. [Google Scholar] [CrossRef]
- Möller, B.; Terheyden, H.; Açil, Y.; Purcz, N.M.; Hertrampf, K.; Tabakov, A.; Behrens, E.; Wiltfang, J. A Comparison of Biocompatibility and Osseointegration of Ceramic and Titanium Implants: An In Vivo and In Vitro Study. Int. J. Oral Maxillofac. Surg. 2012, 41, 638. [Google Scholar] [CrossRef]
- Schliephake, H.; Hefti, T.; Schlottig, F.; Gédet, P.; Staedt, H. Mechanical Anchorage and Peri-Implant Bone Formation of Surface-Modified Zirconia in Minipigs. J. Clin. Periodontol. 2010, 37, 818. [Google Scholar] [CrossRef]
- Kohal, R.J.; Weng, D.; Bächle, M.; Strub, J.R. Loaded Custom-Made Zirconia and Titanium Implants Show Similar Osseointegration: An Animal Experiment. J. Periodontol. 2004, 75, 1262. [Google Scholar] [CrossRef]
- Rohr, N.; Hoda, B.; Fischer, J. Surface Structure of Zirconia Implants: An Integrative Review Comparing Clinical Results with Preclinical and In Vitro Data. Materials 2022, 15, 3664. [Google Scholar] [CrossRef]
- Gündoğar, H.; Uzunkaya, M.; Öğüt, S.; Sarı, F. Effect of Peri-Implant Disease on Oral Health-Related Quality of Life in Geriatric Patients. Gerodontology 2021, 38, 414. [Google Scholar] [CrossRef] [PubMed]
- Pearce, A.I.; Richards, R.G.; Milz, S.; Schneider, E.; Pearce, S.G. Animal Models for Implant Biomaterial Research in Bone: A Review. Eur. Cells Mater. 2007, 13, 1. [Google Scholar] [CrossRef] [PubMed]
- Wancket, L.M. Animal Models for Evaluation of Bone Implants and Devices: Comparative Bone Structure and Common Model Uses. Vet. Pathol. 2015, 52, 842. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment Group | Success No. (%) ± * | Survival No. (%) | Unaccounted for No. (%) | Failure No. (%) |
|---|---|---|---|---|
| Ti group (control) | 16 (22.9) | 9 (10) | 42 (60) | 5 (7.1) |
| ZC group (test) | 10 (12.5) | 13 (16.3) | 59 (73.8) | 5 (6.3) |
| Maxillary | Mandibular | Combined | |
|---|---|---|---|
| Titanium | |||
| Alveolar | 3 | - | 3 |
| Palatal | 2 | - | 2 |
| Total | 5 | ||
| Zirconia | |||
| Alveolar | 5 | - | 5 |
| Palatal | 1 | - | 1 |
| Total | 6 | ||
| Combined | |||
| 8 | - | 8 | |
| 3 | - | 3 | |
| 11 |
| Ti | ZC | p | |
|---|---|---|---|
| Mean pocket depths (mm) [SD] | 2.2 [0.6] | 1.9 [0.7] | 0.04 |
| Mean recession (mm) [SD] | 0.3 [0.9] | 0.4 [1.0] | 0.6 |
| Mean attachment loss (mm) [SD] | 1.9 [0.6] | 1.4 [0.7] | 0.02 |
| Mean bleeding score (%) [range] | 18 [0–83] | 22 [5–40] | NS |
| Implant Type | N | BIC% [SD] |
|---|---|---|
| Southern Zirconia one-piece (ZC) | 10 | 80.0 [17.4] |
| Southern Titanium one-piece (TI) | 10 | 75.7 [20.6] |
| Southern Titanium two-piece (ITC) | 10 | 75.1 [16.1] |
| Nobel Titanium two-piece (NBC) | 10 | 84.2 [16.7] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duncan, W.J.; Ma, S.; Siddiqi, A.; Osman, R.B. Zirconia versus Titanium Implants: 8-Year Follow-Up in a Patient Cohort Contrasted with Histological Evidence from a Preclinical Animal Model. Materials 2022, 15, 5322. https://doi.org/10.3390/ma15155322
Duncan WJ, Ma S, Siddiqi A, Osman RB. Zirconia versus Titanium Implants: 8-Year Follow-Up in a Patient Cohort Contrasted with Histological Evidence from a Preclinical Animal Model. Materials. 2022; 15(15):5322. https://doi.org/10.3390/ma15155322
Chicago/Turabian StyleDuncan, Warwick J., Sunyoung Ma, Allauddin Siddiqi, and Reham B. Osman. 2022. "Zirconia versus Titanium Implants: 8-Year Follow-Up in a Patient Cohort Contrasted with Histological Evidence from a Preclinical Animal Model" Materials 15, no. 15: 5322. https://doi.org/10.3390/ma15155322