
Effects of Implant–Abutment Connection Type and Inter-Implant Distance on Inter-Implant Bone Stress and Microgap: Three-Dimensional Finite Element Analysis

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
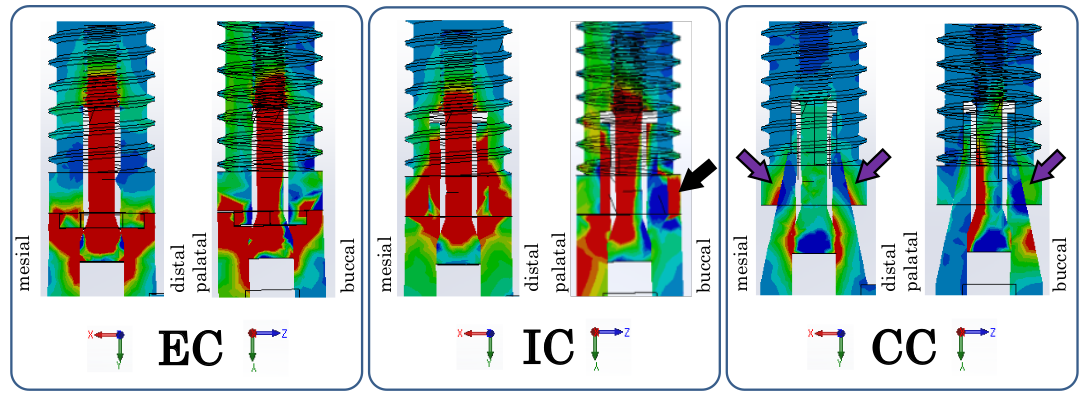
- When implanting two adjacent implants in the region of the maxillary anterior teeth, a CC implant is a mechanically advantageous implant–abutment connection type for maintenance of the inter-implant bone.
- A small inter-implant distance is mechanically disadvantageous for maintenance of the inter-implant bone.
- With an inter-implant distance of less than 3.0 mm, use of a CC implant might suppress absorption of the inter-implant bone.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Adell, R.; Lekholm, U.; Rockler, B.; Brånemark, P.-I. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int. J. Oral Surg. 1981, 10, 387–416. [Google Scholar] [CrossRef]
- Albrektsson, T.; Zarb, G.; Worthington, P.; Eriksson, A.R. The long-term efficacy of currently used dental implants: A review and proposed criteria of success. Int. J. Oral Maxillofac. Implant. 1986, 1, 11–25. [Google Scholar]
- Cardaropoli, G.; Lekholm, U.; Wennstrom, J.L. Tissue alterations at implant-supported single-tooth replacements: A 1-year prospective clinical study. Clin. Oral Implant. Res. 2006, 17, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, C.M.; Nogueira-Filho, G.; Tenenbaum, H.C.; Lai, J.Y.; Brito, C.; Döring, H.; Nonhoff, J. Performance of conical abutment (Morse Taper) connection implants: A systematic review. J. Biomed. Mater. Res. Part A 2014, 102, 552–574. [Google Scholar] [CrossRef]
- Frost, H.M. A 2003 update of bone physiology and Wolff’s Law for clinicians. Angle Orthod. 2004, 74, 3–15. [Google Scholar]
- Esposito, M.; Hirsch, J.M.; Lekholm, U.; Thomsen, P. Biological factors contributing to failures of osseointegrated oral implants (I)—Success criteria and epidemiology. Eur. J. Oral Sci. 1998, 106, 527–551. [Google Scholar] [CrossRef]
- Salama, H.; Salama, M.A.; Garber, D.; Adar, P. The interproximal height of bone: A guidepost to predictable aesthetic strategies and soft tissue contours in anterior tooth replacement. Pr. Periodontics Aesthet. Dent. PPAD 1999, 10, 1131–1141. [Google Scholar]
- Gaggl, A.; Schultes, G. Biomechanical properties in titanium implants with integrated maintenance free shock absorbing el-ements. Biomaterials 2001, 22, 3061–3066. [Google Scholar] [CrossRef]
- Heckmann, S.; Linke, J.; Graef, F.; Foitzik, C.; Wichmann, M.; Weber, H.-P. Stress and inflammation as a detrimental combination for peri-implant bone loss. J. Dent. Res. 2006, 85, 711–716. [Google Scholar] [CrossRef] [Green Version]
- Kitagawa, T.; Tanimoto, Y.; Odaki, M.; Nemoto, K.; Aida, M. Influence of implant/abutment joint designs on abutment screw loosening in a dental implant system. J. Biomed. Mater. Res. Part B Appl. Biomater. 2005, 75, 457–463. [Google Scholar] [CrossRef]
- Hermann, J.S.; Buser, D.; Schenk, R.K.; Cochran, D.L. Crestal Bone Changes Around Titanium Implants. A Histometric Evaluation of Unloaded Non-Submerged and Submerged Implants in the Canine Mandible. J. Periodontol. 2000, 71, 1412–1424. [Google Scholar] [CrossRef] [Green Version]
- Tarnow, D.; Cho, S.; Wallace, S. The Effect of Inter-Implant Distance on the Height of Inter-Implant Bone Crest. J. Periodontol. 2000, 71, 546–549. [Google Scholar] [CrossRef] [Green Version]
- Ersoy, A.E.; Turkyilmaz, I.; Ozan, O.; McGlumphy, E.A. Reliability of Implant Placement with Stereolithographic Surgical Guides Generated from Computed Tomography: Clinical Data From 94 Implants. J. Periodontol. 2008, 79, 1339–1345. [Google Scholar] [CrossRef]
- Quaresma, S.E.; Cury, P.R.; Sendyk, W.R.; Sendyk, C. A finite element analysis of two different dental implants: Stress dis-tribution in the prosthesis, abutment, implant, and supporting bone. J. Oral Implantol. 2008, 34, 1–6. [Google Scholar] [CrossRef]
- Pessoa, R.S.; Muraru, L.; Júnior, E.M.; Vaz, L.G.; Sloten, J.V.; Duyck, J.; Jaecques, S.V. Influence of Implant Connection Type on the Biomechanical Environment of Immediately Placed Implants—CT-Based Nonlinear, Three-Dimensional Finite Element Analysis. Clin. Implant. Dent. Relat. Res. 2009, 12, 219–234. [Google Scholar] [CrossRef]
- Rodríguez-Ciurana, X.; Vela-Nebot, X.; Segalà-Torres, M.; Calvo-Guirado, J.L.; Cambra, J.; Méndez-Blanco, V.; Tarnow, D.P. The effect of interimplant distance on the height of the interimplant bone crest when using platform-switched implants. Int. J. Periodontics Restor. Dent. 2009, 29, 141–151. [Google Scholar]
- Elian, N.; Bloom, M.; Dard, M.; Cho, S.-C.; Trushkowsky, R.D.; Tarnow, D. Effect of Interimplant Distance (2 and 3 mm) on the Height of Interimplant Bone Crest: A Histomorphometric Evaluation. J. Periodontol. 2011, 82, 1749–1756. [Google Scholar] [CrossRef]
- Kaminaka, A.; Nakano, T.; Ono, S.; Kato, T.; Yatani, H. Cone-Beam Computed Tomography Evaluation of Horizontal and Vertical Dimensional Changes in Buccal Peri-Implant Alveolar Bone and Soft Tissue: A 1-Year Prospective Clinical Study. Clin. Implant. Dent. Relat. Res. 2014, 17, e576–e585. [Google Scholar] [CrossRef]
- Weng, D.; Nagata, M.J.H.; Bell, M.; Bosco, A.F.; De Melo, L.G.N.; Richter, E.-J. Influence of microgap location and configuration on the periimplant bone morphology in submerged implants. An experimental study in dogs. Clin. Oral Implant. Res. 2008, 19, 1141–1147. [Google Scholar] [CrossRef]
- Lin, C.-L.; Chang, S.-H.; Chang, W.-J.; Kuo, Y.-C. Factorial analysis of variables influencing mechanical characteristics of a single tooth implant placed in the maxilla using finite element analysis and the statistics-based Taguchi method. Eur. J. Oral Sci. 2007, 115, 408–416. [Google Scholar] [CrossRef]
- Yamanishi, Y.; Yamaguchi, S.; Imazato, S.; Nakano, T.; Yatani, H. Influences of implant neck design and implant–abutment joint type on peri-implant bone stress and abutment micromovement: Three-dimensional finite element analysis. Dent. Mater. 2012, 28, 1126–1133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Streckbein, P.; Streckbein, R.; Wilbrand, J.; Malik, C.; Schaaf, H.; Howaldt, H.; Flach, M. Non-linear 3D Evaluation of Different Oral Implant-Abutment Connections. J. Dent. Res. 2012, 91, 1184–1189. [Google Scholar] [CrossRef] [PubMed]
- Helkimo, E.; Carlsson, G.E.; Helkimo, M. Bite force and state of dentition. Acta Odontol. Scand. 1977, 35, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Clelland, N.L.; Seidt, J.D.; Daroz, L.G.D.; McGlumphy, E.A. Comparison of strains for splinted and nonsplinted implant prostheses using three-dimensional image correlation. Int. J. Oral Maxillofac. Implant. 2010, 25, 953–959. [Google Scholar]
- Vigolo, P.; Mutinelli, S.; Zaccaria, M.; Stellini, E. Clinical Evaluation of Marginal Bone Level Change Around Multiple Adjacent Implants Restored with Splinted and Nonsplinted Restorations: A 10-Year Randomized Controlled Trial. Int. J. Oral Maxillofac. Implant. 2015, 30, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Pilkey, W.D.; Peterson, R.E. Peterson’s Stress Concentration Factors, 2nd ed.; John Wiley & Sons: New York, NY, USA, 1997. [Google Scholar]
- Yamaguchi, S.; Tsutsui, K.; Satake, K.; Morikawa, S.; Shirai, Y.; Tanaka, H.T. Dynamic analysis of a needle insertion for soft materials: Arbitrary Lagrangian–Eulerian-based three-dimensional finite element analysis. Comput. Biol. Med. 2014, 53, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, S.; Katsumoto, Y.; Hayashi, K.; Aoki, M.; Kunikata, M.; Nakase, Y.; Lee, C.; Imazato, S. Fracture origin and crack propagation of CAD/CAM composite crowns by combining of in vitro and in silico approaches. J. Mech. Behav. Biomed. Mater. 2020, 112, 104083. [Google Scholar] [CrossRef]
- Karaer, O.; Yamaguchi, S.; Nakase, Y.; Lee, C.; Imazato, S. In silico non-linear dynamic analysis reflecting in vitro physical properties of CAD/CAM resin composite blocks. J. Mech. Behav. Biomed. Mater. 2020, 104, 103697. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Component | Material | Elastic Modulus (MPa) | Poisson Ratio | References |
|---|---|---|---|---|
| Cortical bone | Cortical bone | 13,000 | 0.3 | [16] |
| Cancellous bone | Cancellous bone | 1370 | 0.3 | [16] |
| Implant body | Titanium | 117,000 | 0.3 | [16] |
| abutment | ||||
| Abutment screw | Titanium alloy | 120,000 | 0.36 | [17] |
| Superstructure | Gold alloy | 96,600 | 0.35 | [14] |
| Connection Type, Inter-Implant Distance | Number of Elements |
|---|---|
| External connection, 3.0 mm | 162,963 |
| External connection, 2.5 mm | 173,526 |
| External connection, 2.0 mm | 171,671 |
| Internal connection, 3.0 mm | 156,325 |
| Internal connection, 2.5 mm | 172,679 |
| Internal connection, 2.0 mm | 171,898 |
| Conical connection, 3.0 mm | 155,243 |
| Conical connection, 2.5 mm | 152,925 |
| Conical connection, 2.0 mm | 152,115 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsuoka, T.; Nakano, T.; Yamaguchi, S.; Ono, S.; Watanabe, S.; Sato, T.; Yatani, H. Effects of Implant–Abutment Connection Type and Inter-Implant Distance on Inter-Implant Bone Stress and Microgap: Three-Dimensional Finite Element Analysis. Materials 2021, 14, 2421. https://doi.org/10.3390/ma14092421
Matsuoka T, Nakano T, Yamaguchi S, Ono S, Watanabe S, Sato T, Yatani H. Effects of Implant–Abutment Connection Type and Inter-Implant Distance on Inter-Implant Bone Stress and Microgap: Three-Dimensional Finite Element Analysis. Materials. 2021; 14(9):2421. https://doi.org/10.3390/ma14092421
Chicago/Turabian StyleMatsuoka, Takashi, Tamaki Nakano, Satoshi Yamaguchi, Shinji Ono, Shota Watanabe, Takumi Sato, and Hirofumi Yatani. 2021. "Effects of Implant–Abutment Connection Type and Inter-Implant Distance on Inter-Implant Bone Stress and Microgap: Three-Dimensional Finite Element Analysis" Materials 14, no. 9: 2421. https://doi.org/10.3390/ma14092421