Biomechanical Loading Comparison between Titanium and Unsintered Hydroxyapatite/Poly-L-Lactide Plate System for Fixation of Mandibular Subcondylar Fractures

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
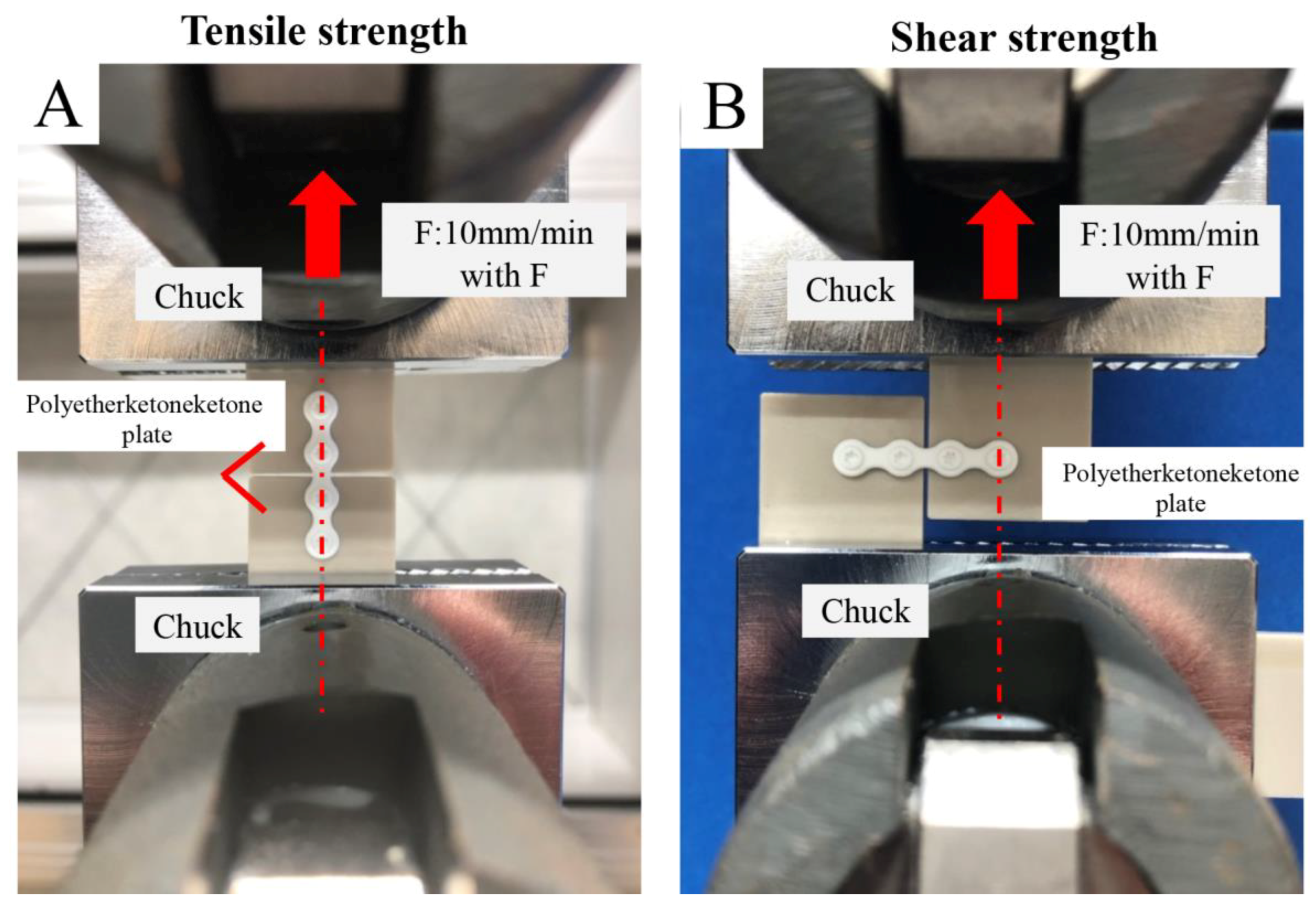
2.2. Evaluation of Tensile and Shear Strength of Titanium and Bioresorbable Plate Systems
2.2.1. Sample Preparation
- A single u-HA/PLLA bioresorbable straight plate, with the plate held in place on each side with two screws (total four screws);
- A single titanium straight plate, with the plate held in place on each side with two screws (total four screws).
2.2.2. Strength Measurement
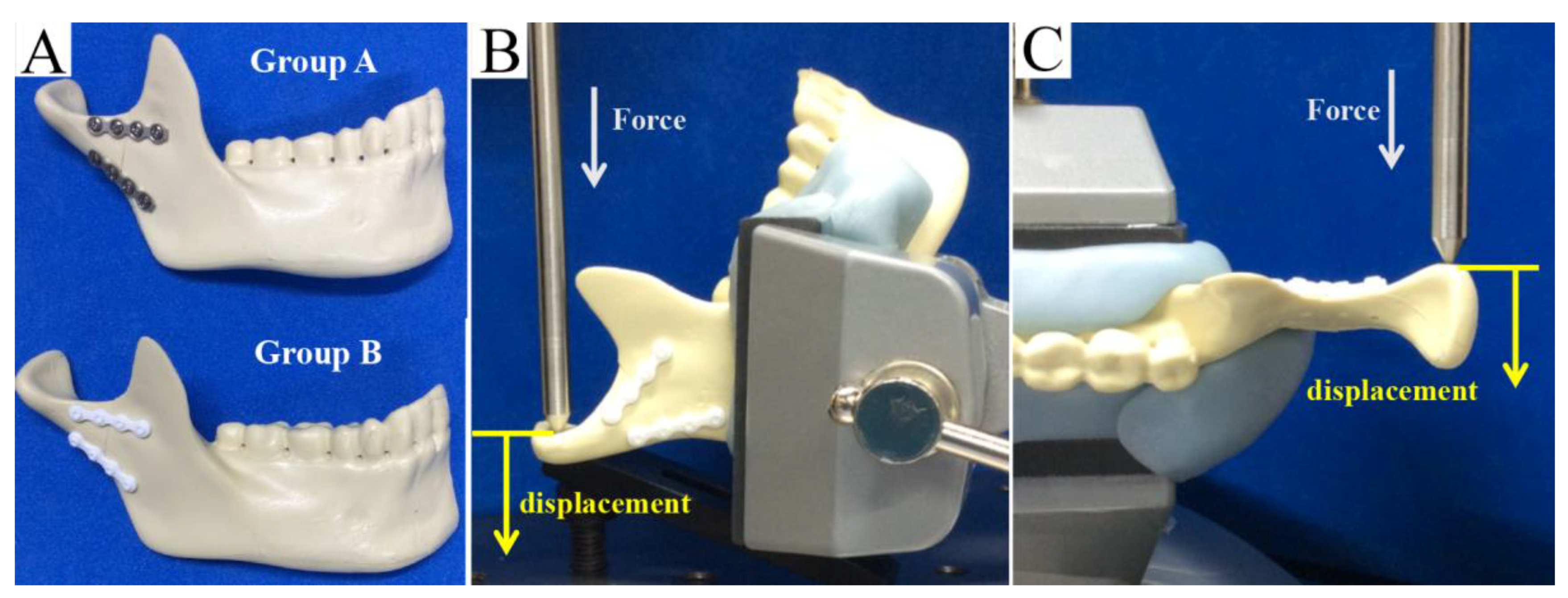
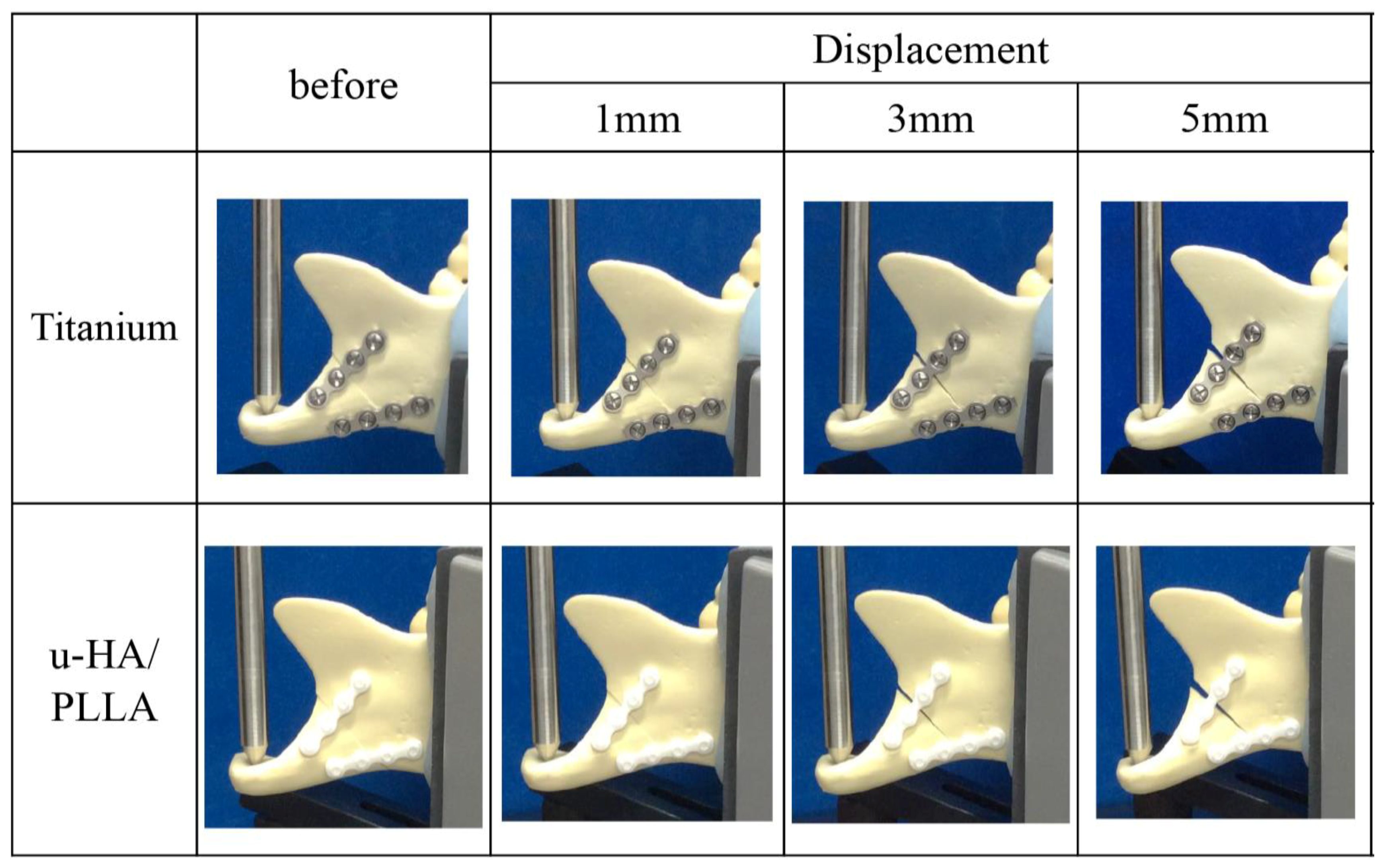
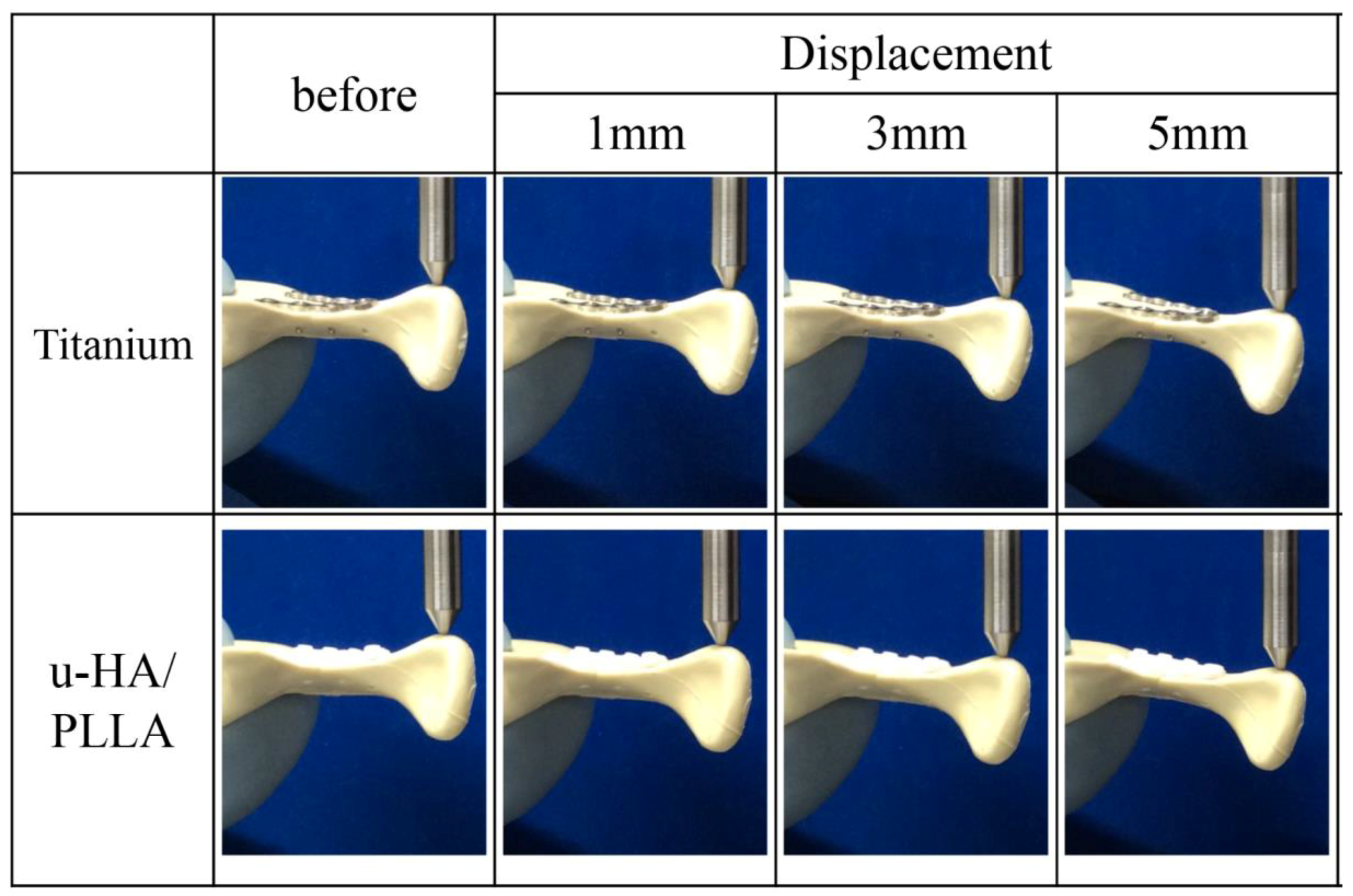
2.3. Biomechanical Loading Evaluation
2.3.1. Sample Preparation
2.3.2. Fixation Method for Mandibular Condylar Fracture
2.3.3. Biomechanical Loading Test
2.4. Statistical Analysis
3. Results
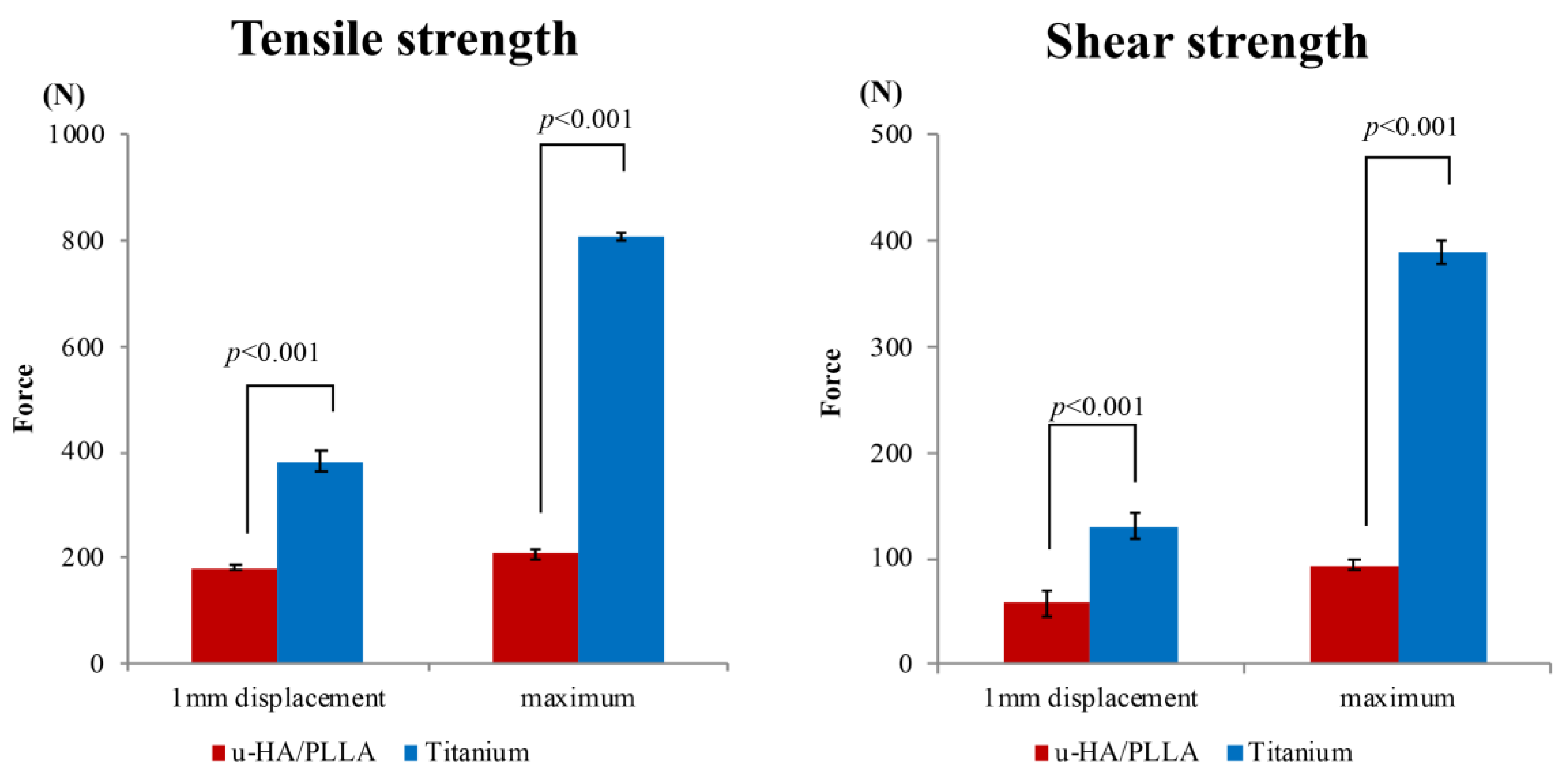
3.1. Tensile and Shear Strength Evaluation
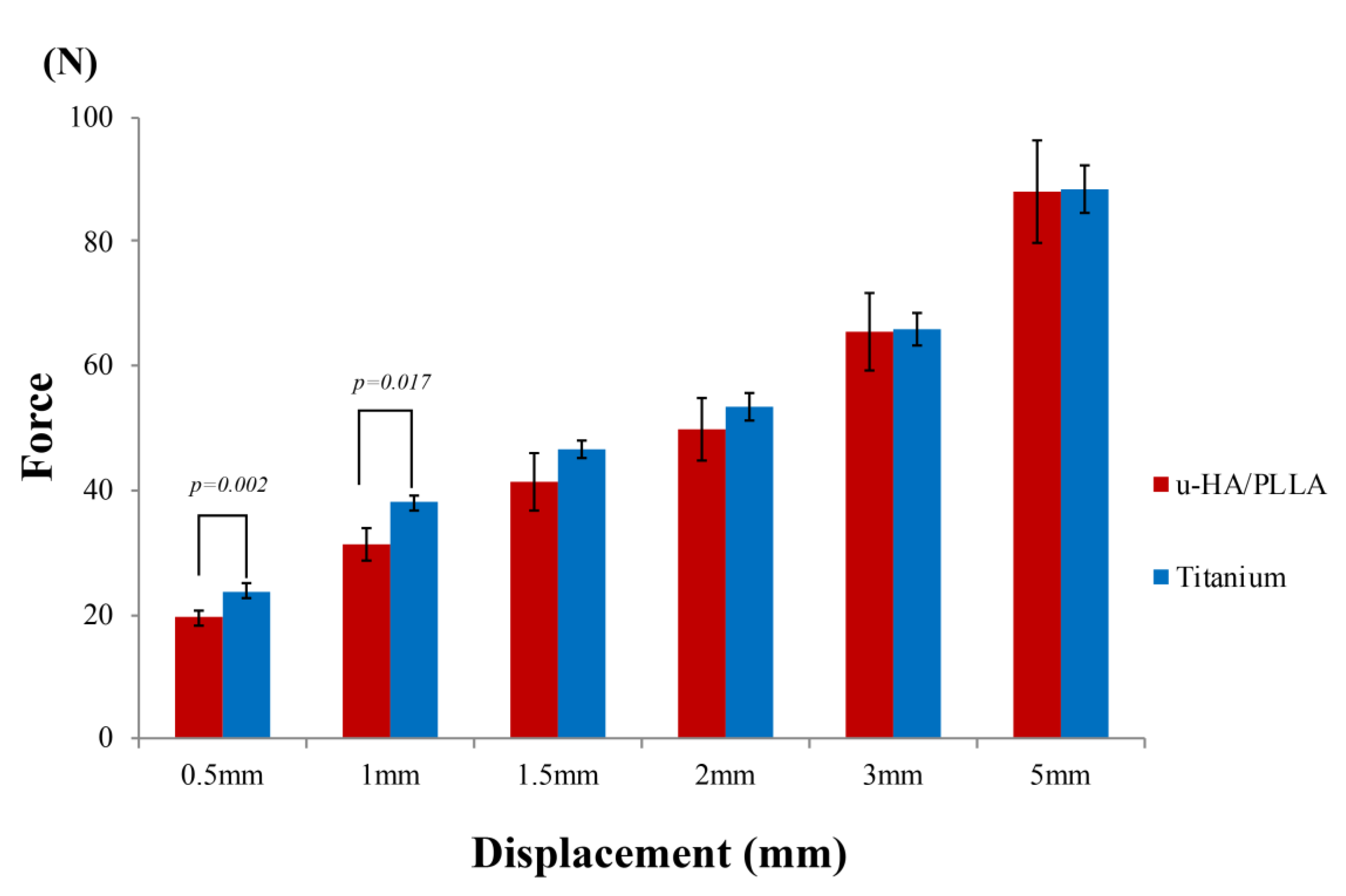
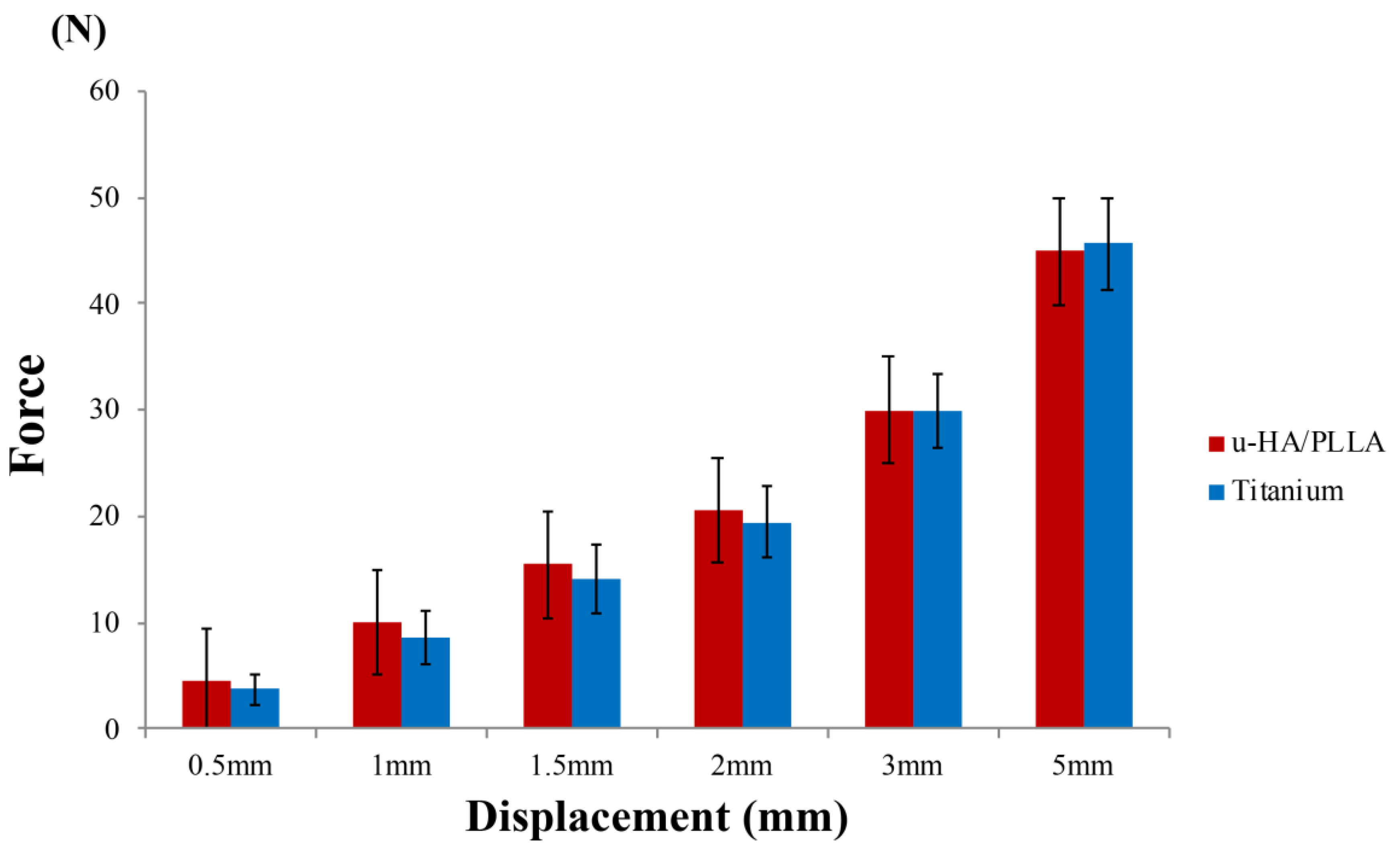
3.2. Biomechanical Loading Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ellis, E.; Throckmorton, G.S. Treatment of mandibular condylar process fractures: Biological considerations. J. Oral Maxillofac. Surg. 2005, 63, 115–134. [Google Scholar] [CrossRef]
- Fernández-Olarte, H.; Gómez-Delgado, A.; López-Dávila, D.; Rangel-Perdomo, R.; Lafaurie, G.I.; Chambrone, L. Is the Mandibular Growth Affected by Internal Rigid Fixation? A Systematic Review. J. Maxillofac. Oral Surg. 2017, 16, 277–283. [Google Scholar] [CrossRef]
- Kanno, T.; Sukegawa, S.; Fujioka, M.; Takabatake, K.; Furuki, Y. Transoral Open Reduction with Rigid Internal Fixation for Subcondylar Fractures of the Mandible Using a Small Angulated Screwdriver System: Is Endoscopic Assistance Necessary? J. Oral Maxillofac. Surg. 2011, 69, e372–e384. [Google Scholar] [CrossRef] [PubMed]
- Kanno, T.; Sukegawa, S.; Tatsumi, H.; Nariai, Y.; Ishibashi, H.; Furuki, Y.; Sekine, J. The retromandibular transparotid approach for reduction and rigid internal fixation using two locking miniplates in mandibular condylar neck fractures. Int. J. Oral Maxillofac. Surg. 2014, 43, 177–184. [Google Scholar] [CrossRef]
- Sukegawa, S.; Kanno, T.; Katase, N.; Shibata, A.; Takahashi, Y.; Furuki, Y. Which fixation methods are better between three-dimensional anatomical plate and two miniplates for the mandibular subcondylar fracture open treatment? J. Craniomaxillofac. Surg. 2019, 47, 771–777. [Google Scholar] [CrossRef]
- Parascandolo, S.; Spinzia, A.; Parascandolo, S.; Piombino, P.; Califano, L. Two load sharing plates fixation in mandibular condylar fractures: Biomechanical basis. J. Cranio-Maxillofac. Surg. 2010, 38, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.; Kshirsagar, R.; Halli, R.; Sane, V.; Chhabaria, G.; Ramanojam, S.; Joshi, S.; Patankar, A. Evaluation of bioresorbable plates in condylar fracture fixation: A case series. Int. J. Oral Maxillofac. Surg. 2013, 42, 1503–1505. [Google Scholar] [CrossRef]
- Sukegawa, S.; Kanno, T.; Katase, N.; Shibata, A.; Takahashi, Y.; Furuki, Y. Clinical Evaluation of an Unsintered Hydroxyapatite/Poly-l-Lactide Osteoconductive Composite Device for the Internal Fixation of Maxillofacial Fractures. J. Craniofac. Surg. 2016, 27, 1391–1397. [Google Scholar] [CrossRef] [PubMed]
- Sukegawa, S.; Kanno, T.; Kawai, H.; Shibata, A.; Takahashi, Y.; Nagatsuka, H.; Furuki, Y. Long-Term Bioresorption of Bone Fixation Devices Made from Composites of Unsintered Hydroxyapatite Particles and Poly-l-Lactide. J. Hard Tissue Biol. 2015, 24, 219–224. [Google Scholar] [CrossRef]
- De Santis, R.; Sarracino, F.; Mollica, F.; Netti, P.A.; Ambrosio, L.; Nicolais, L. Continuous fiber reinforced polymers as connective tissue replacement. Compos. Sci. Technol. 2004, 64, 861–871. [Google Scholar] [CrossRef]
- Meyer, C.; Serhir, L.; Boutemi, P. Experimental evaluation of three osteosynthesis devices used for stabilizing condylar fractures of the mandible. J. Cranio-Maxillofac. Surg. 2006, 34, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Meyer, C.; Kahn, J.-L.; Lambert, A.; Boutemy, P.; Wilk, A. Development of a static simulator of the mandible. J. Cranio-Maxillofac. Surg. 2000, 28, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Ballon, A.; Laudemann, K.; Sader, R.; Landes, C.A. Segmental stability of resorbable P(L/DL)LA-TMC osteosynthesis versus titanium miniplates in orthognatic surgery. J. Cranio-Maxillofac. Surg. 2012, 40, e408–e414. [Google Scholar] [CrossRef]
- Sukegawa, S.; Kawai, H.; Nakano, K.; Kanno, T.; Takabatake, K.; Nagatsuka, H.; Furuki, Y. Feasible Advantage of Bioactive/Bioresorbable Devices Made of Forged Composites of Hydroxyapatite Particles and Poly-l-lactide in Alveolar Bone Augmentation: A Preliminary Study. Int. J. Med. Sci. 2019, 16, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Sukegawa, S.; Kanno, T.; Nagano, D.; Shibata, A.; Sukegawa-Takahashi, Y.; Furuki, Y. The Clinical Feasibility of Newly Developed Thin Flat-Type Bioresorbable Osteosynthesis Devices for the Internal Fixation of Zygomatic Fractures: Is There a Difference in Healing Between Bioresorbable Materials and Titanium Osteosynthesis? J. Craniofac. Surg. 2016, 27, 2124–2129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, Q.N.; Karino, M.; Koike, T.; Ide, T.; Okuma, S.; Kaneko, I.; Osako, R.; Kanno, T. Navigation-Assisted Isolated Medial Orbital Wall Fracture Reconstruction Using an U-HA/PLLA Sheet via a Transcaruncular Approach. J. Investig. Surg. 2019, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Sukegawa, S.; Kanno, T.; Tanaka, S.; Matsumoto, K.; Sukegawa-Takahashi, Y.; Masui, M.; Koyama, Y.; Furuki, Y. Precision of Post-Traumatic Orbital Reconstruction Using Unsintered Hydroxyapatite Particles/Poly-l-Lactide Composite Bioactive/Resorbable Mesh Plate with and without Navigation: A Retrospective Study. J. Hard Tissue Biol. 2017, 26, 274–280. [Google Scholar] [CrossRef]
- Leno, M.B.; Liu, S.Y.; Chen, C.-T.; Liao, H.-T. Comparison of functional outcomes and patient-reported satisfaction between titanium and absorbable plates and screws for fixation of mandibular fractures: A one-year prospective study. J. Cranio-Maxillofac. Surg. 2017, 45, 704–709. [Google Scholar] [CrossRef]
- Lauer, G.; Pradel, W.; Leonhardt, H.; Loukota, R.; Eckelt, U. Resorbable triangular plate for osteosynthesis of fractures of the condylar neck. Br. J. Oral Maxillofac. Surg. 2010, 48, 532–535. [Google Scholar] [CrossRef]
- Shikinami, Y.; Okuno, M. Bioresorbable devices made of forged composites of hydroxyapatite (HA) particles and poly L-lactide (PLLA). Part II: practical properties of miniscrews and miniplates. Biomaterials 2001, 22, 3197–3211. [Google Scholar] [CrossRef]
- de Souza, G.M.; Rodrigues, D.C.; Celegatti Filho, T.S.; Moreira, R.W.F.; Falci, S.G.M. In vitro comparison of mechanical resistance between two straight plates and a Y-plate for fixation of mandibular condyle fractures. J. Craniomaxillofac. Surg. 2018, 46, 168–172. [Google Scholar] [CrossRef] [PubMed]
- Koolstra, J.H.; Van Eijden, T.M. Dynamics of the human masticatory muscles during a jaw open-close movement. J. Biomech. 1997, 30, 883–889. [Google Scholar] [CrossRef]
- Champy, M.; Lodde, J. Mandibular synthesis. Positioning of the syntheses according to mandibular stress. Rev. Stomatol. Chir Maxillofac. 1976, 77, 971–976. [Google Scholar] [PubMed]
- Sukegawa, S.; Kanno, T.; Matsumoto, K.; Sukegawa-Takahashi, Y.; Masui, M.; Furuki, Y. Complications of a poly-l-lactic acid and polyglycolic acid osteosynthesis device for internal fixation in maxillofacial surgery. Odontology 2018, 106, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Daniels, A.U.; Chang, M.K.O.; Andriano, K.P.; Heller, J. Mechanical properties of biodegradable polymers and composites proposed for internal fixation of bone. J. Appl. Biomater. 1990, 1, 57–78. [Google Scholar] [CrossRef]
- Bergsma, J.E.; de Bruijn, W.C.; Rozema, F.R.; Bos, R.R.; Boering, G. Late degradation tissue response to poly(L-lactide) bone plates and screws. Biomaterials 1995, 16, 25–31. [Google Scholar] [CrossRef]
- Matsusue, Y.; Nakamura, T.; Iida, H.; Shimizu, K. A long-term clinical study on drawn poly-l-lactide implants in orthopaedic surgery. J. Long. Term. Eff. Med. Implants 1997, 7, 119–137. [Google Scholar]
- Matsusue, Y.; Yamamuro, T.; Yoshii, S.; Oka, M.; Ikada, Y.; Hyon, S.-H.; Shikinami, Y. Biodegradable screw fixation of rabbit tibia proximal osteotomies. J. Appl. Biomater. 1991, 2, 1–12. [Google Scholar] [CrossRef]
- Sukegawa, S.; Kanno, T.; Hotaka, K.; Akane, S.; Matsumoto, K.; Sukegawa-Takahashi, Y.; Sakaida, K.; Nagatsuka, H.; Furuki, Y. Surgical Treatment and Dental Implant Rehabilitation after the Resection of an Osseous Dysplasia. J. Hard Tissue Biol. 2016, 25, 437–441. [Google Scholar] [CrossRef] [Green Version]
- Shikinami, Y.; Okuno, M. Bioresorbable devices made of forged composites of hydroxyapatite (HA) particles and poly-l-lactide (PLLA): Part I. Basic characteristics. Biomaterials 1999, 20, 859–877. [Google Scholar] [CrossRef]
- Al-Moraissi, E.A.; Ellis, E.; Neff, A. Does encountering the facial nerve during surgical management of mandibular condylar process fractures increase the risk of facial nerve weakness? A systematic review and meta-regression analysis. J. Cranio-Maxillofac. Surg. 2018, 46, 1223–1231. [Google Scholar] [CrossRef] [PubMed]







© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sukegawa, S.; Kanno, T.; Yamamoto, N.; Nakano, K.; Takabatake, K.; Kawai, H.; Nagatsuka, H.; Furuki, Y. Biomechanical Loading Comparison between Titanium and Unsintered Hydroxyapatite/Poly-L-Lactide Plate System for Fixation of Mandibular Subcondylar Fractures. Materials 2019, 12, 1557. https://doi.org/10.3390/ma12091557
Sukegawa S, Kanno T, Yamamoto N, Nakano K, Takabatake K, Kawai H, Nagatsuka H, Furuki Y. Biomechanical Loading Comparison between Titanium and Unsintered Hydroxyapatite/Poly-L-Lactide Plate System for Fixation of Mandibular Subcondylar Fractures. Materials. 2019; 12(9):1557. https://doi.org/10.3390/ma12091557
Chicago/Turabian StyleSukegawa, Shintaro, Takahiro Kanno, Norio Yamamoto, Keisuke Nakano, Kiyofumi Takabatake, Hotaka Kawai, Hitoshi Nagatsuka, and Yoshihiko Furuki. 2019. "Biomechanical Loading Comparison between Titanium and Unsintered Hydroxyapatite/Poly-L-Lactide Plate System for Fixation of Mandibular Subcondylar Fractures" Materials 12, no. 9: 1557. https://doi.org/10.3390/ma12091557