
Live to Move and Move to Live: The Health of the Lymphatic System Relies on Mobility and the Foot and Calf Pump Connection
Koya Medical, Oakland, CA 94607, USA
Lymphatics 2024, 2(2), 43-49; https://doi.org/10.3390/lymphatics2020004
Submission received: 29 January 2024
/
Revised: 19 March 2024
/
Accepted: 23 March 2024
/
Published: 26 March 2024
{kind=link}
Abstract
:The foot and calf muscle pump, collectively known as the venous muscle pump, plays a crucial role in the circulatory system (veins, arteries, and lymphatics), particularly in the return of blood from the lower extremities to the heart. Further, the venous muscle pump is crucial to lymphatic health and essential in chronic edema/lymphedema management. This article will highlight the significance of the venous pump and review the functional anatomy and physiology of the foot and calf, integrating the connection to venous and lymphatic health. The complementary importance of mobility, exercise, and breathing will also be explored.
The intelligence of the human body’s design is eloquently demonstrated in the foot and lower leg. The human foot contains 26 bones, four layers of intrinsic muscles, an intricate vascular and neurological network, and complex biomechanics [1]. Every day, the human foot is subjected to various stresses, loads, and environmental factors due to its role in supporting the body’s weight, facilitating movement, offsetting gravity, and interacting with the surrounding environment. Of crucial importance is the interconnection of the foot and calf mechanics in conjunction with the veins and lymphatics to maintain vascular health and function. When functional, this prevents the formation and stagnation of interstitial edema. Alterations in tissue homeostasis can occur when there is excessive demand on the lymphatic system. This may result from a congenital or acquired abnormality of the lymphatics.
Lymphedema related to a genetic discrepancy in the structure or function of the lymphatic pathways is called primary (congenital) lymphedema [2]. Traditionally, the diagnosis of primary lymphedema was based on the age of presentation, and termed congenital (birth to two years), praecox (puberty to age 35), or tarda (onset after age 35). More recently, molecular studies have provided insight into various phenotypes of primary lymphedema. This led to the development of the St. George Classification Algorithm to describe primary lymphedema. The algorithm considers vascular malformations and primary lymphatic abnormalities and divides primary lymphedema into syndromic, generalized lymphatic dysplasia with systemic involvement, congenital-onset lymphedema, and late-onset lymphedema [2]. The intent is to help clinicians better categorize their patients and guide testing toward a molecular diagnosis. Secondary lymphedema, also referred to as acquired lymphedema, is due to some insult, injury, or obstruction to the lymphatic system and can develop at any time during the lifespan. Secondary lymphedema is more common, affecting 1/1000 individuals, whereas primary affects roughly 1/100,000 individuals in the United States [3].
To begin, it is essential to review the anatomy and physiology of the lymphatic and venous systems with a particular focus on their interdependence. The anatomy of the lymphatic system establishes a one-way drainage route to allow the return of interstitial fluid and macromolecules, known as lymph, to the circulation via the venous system to maintain tissue homeostasis. In 2010, Levick and Michel mathematically demonstrated that there is no net reabsorption of fluid back into the venous side of the blood capillaries [4]. They showed a diminishing net filtration across the capillary bed, suggesting the lymphatics are solely responsible for fluid management once in the interstitium [4]. This, coupled with the recognition of the endothelial glycocalyx layer controlling the movement of proteins and fluid across the blood capillary, has redefined Starlings Law of the Microcirculation [5,6]. Lymph contains immunologically active cells such as lymphocytes, macrophages, and antigenic organic material [7]. The lymphatic system regulates all body fluids, macromolecule homeostasis, lipid absorption, and immune function [8]. It is the body’s immune surveillance system. For this to occur, the lymphatics must move fluid and all its contents from the interstitium through the lymphatics into the lymph nodes and ultimately return it to the venous system. Pumps accomplish this transport. The lymphatic system utilizes extrinsic and intrinsic pumps to mobilize and transport lymph fluid and its constituents. Extrinsic pumps depend on the cyclical compression and expansion of lymphatics by surrounding tissue forces such as muscle contractions and breathing. The intrinsic pumps rely on the rapid phasic contractions of lymphatic collectors, and neural, humoral, and physical factors can modulate the intrinsic lymph pump function [8]. Generally, increased lymph pressure and/or stretch of the lymphatics activates the intrinsic lymph pump, while increased lymph flow and shear in the lymphatic collectors can either activate or inhibit the intrinsic lymph pump depending on the pattern and magnitude of the flow [8]. The extrinsic pumps are thought to predominate in the heart, skeletal muscle, thorax, and gut wall lymphatics, while the intrinsic pumps are essential for lymph flow in most other lymphatic beds [8].
The lower extremities are of particular importance for venous and lymphatic health. In the leg, superficial and deep lymphatic vessel systems, as well as the corresponding arteries and veins, are separated by the deep fascia, which envelops the four muscle compartments of the leg. Three major lymphatic trunks associated with the lower extremity drain lymph from different foot regions, including the heel. The superficial compartment follows the great saphenous vein to drain to the inguinal lymph nodes. Another area drains from the heel and follows the course of the small saphenous vein to the popliteal lymph nodes. The deep system drains the muscles, bones, joints, and fascia via trunks that run closely with the deep veins [7]. A healthy and functional venous system supports a healthy and functional lymphatic system and vice versa. From this anatomical orientation, it becomes evident how impairments in the musculoskeletal, neuromuscular, or vascular systems can negatively impact lymphatic flow and drainage, highlighting the interdependence of these systems.
Veins and lymphatics have a similar embryological origin and anatomical structure. With new imaging and technological advances, a deeper understanding of the origins of the lymphatic system is emerging. Historically, the lymphatic vessels were first described by Gaspare Aselli in 1627. In 1902, Florence Sabin proposed that lymph sacs originated from endothelial cells budding from the cardinal vein, and in 1993, Karl Alitalo demonstrated that VEGF-C/VEGF-D/VEGFR-3 signaling plays a key role in the development and growth of lymphatic vessels [9]. Venous disease is associated with microangiopathic changes in the vascular and lymphatic networks [7]. The disruption or loss of lymphatic function results in the development of edema, commonly seen in chronic venous insufficiency (CVI).
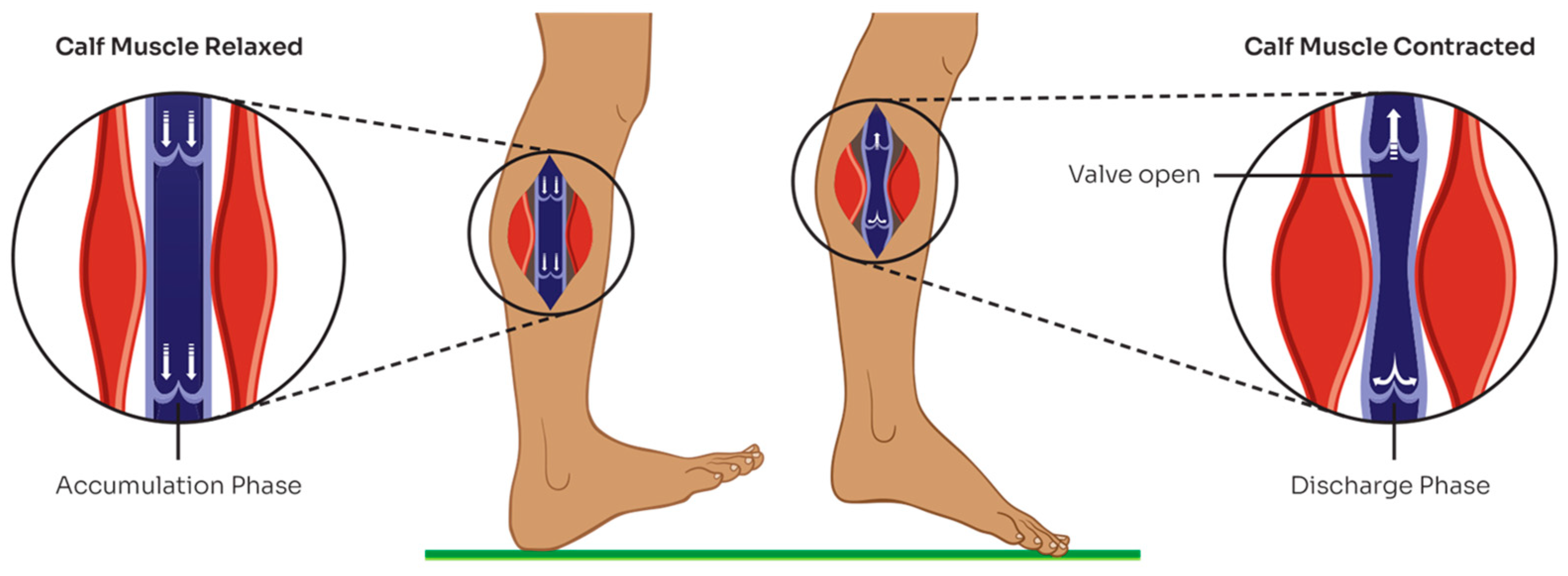
Emptying the venous plexus in the muscles of the calf during plantar flexion of the ankle in the presence of a competent valvular system and the absence of obstruction in the prominent veins is a critical component of healthy venous circulation [10,11,12,13,14] (see Figure 1).
New evidence suggests the muscle pump functions differently during the natural gait cycle compared to activities such as ankle pump exercises. According to Tauraginskii et al., the muscle pump involves the synergistic work of antagonist muscles, the ankle joint, and the posterior calf muscle group [15]. This is further explained by looking at the gait cycle: during the stance phase, the gastrocnemius contracts while the anterior tibial muscle relaxes, creating high pressure in intramuscular veins. On the contrary, during the swing phase, the anterior tibial muscle contracts while the gastrocnemius relaxes, essentially generating negative pressure in the intramuscular veins. The pump redirects blood flow from superficial to intramuscular veins during natural locomotion, acting like a “stream diversion pump” [15].
In simple terms, when the calf pump is properly functioning, the blood is collected from superficial veins via perforators and is transported to the deep venous system and ultimately toward the heart. Lack of physiological emptying of veins results in ambulatory venous hypertension, which ultimately leads to the development of skin ulceration [16]. Chronic venous insufficiency is the result of continuous venous hypertension caused by a combination of venous reflux, venous obstruction, and a poorly functioning calf muscle pump [17]. The proper outflow of venous blood from the lower extremities depends on vein patency, valve competency, and proper calf muscle function. Any disturbance in these three components results in venous hypertension and chronic venous insufficiency (CVI). Interestingly, failure of the muscle pump is the most underestimated pathophysiological factor [16]. This highlights the importance of vein health, which can be enhanced through mobility, ambulation, exercise, and compression.
Gravity is an additional external factor that must be overcome to prevent edema of the legs. The valves of the veins prevent reflux (or regurgitation) towards the feet. However, efficient venous blood flow requires three other mechanisms that are often not considered or recognized for their importance in this role: breathing, muscle activity, and ground reaction forces (GRF) [1]. First, during breathing, changes in the thorax and abdominal pressures create a respiratory pump. During inspiration, the diaphragm moves downward, decreasing pressure in the thoracic body cavity while increasing pressure in the abdomen. This motion results in blood being pulled towards the lower chest cavity. This action provides a sump effect on the lymphatics, helping to mobilize fluid, given that the thoracic duct (the largest lymph vessel in the body) is stimulated during the breath cycle [18]. With expiration, the valves in the veins prevent the blood from regurgitating as the pressures reverse [19,20]. Next, muscle activity also creates skeletal muscle pumps, moving blood and fluid with each muscular contraction. Additionally, the lymph nodes are strategically located near joints and are naturally compressed or pumped with range of motion and the natural movement of inhalation and exhalation, further supporting lymph flow through the nodes. Collectively, this facilitates blood and lymph fluid to move cephalad. Finally, ground reaction forces on the foot during stance and gait create a foot pump, highlighting the importance of mobility and ambulation to help move blood and lymph. These mechanisms and hydrodynamic flow rely on competent and functional vein valves and help preserve vascular and tissue health [21].
The deep veins in the legs often exist in pairs and are more variable than the corresponding arteries. Superficial veins (e.g., great and small saphenous veins) run superficial to the deep fascia and connect with the deep veins by an average of 64 perforator veins between the ankle and the groin [22]. This allows blood to flow by aspiration into the deep veins [23]. Within the deep veins of the calf lie intramuscular venous sinuses that act as conduits, transferring blood from the intramuscular veins to the axial deep veins for the muscular pump of the calf [15]. Muscular pumps compress stiff vein walls running through the muscles and their fascial compartments, supporting flow out of the lower extremities [22,23,24]. During contraction, muscles tighten the fascia and compress the veins, raising pressures within the muscle compartment. Proximal valves open, and blood moves into the next section of the vein towards the heart, with the valves preventing reflux during muscle relaxation when competent. This physiological process partly explains the mechanism of action of compression garments. If valves are incompetent, the external force produced by the compression textile resists the expansion of the muscle, helping to restore valve function and promote cephalad fluid flow.
The plantar surface of the foot distorts under GRF during gait, allowing the heel and forefoot to behave like ‘compression pumps’, expelling blood into calf veins together with the action of plantar intrinsic muscles [25,26]. With each step, GRFs act on deep plantar veins like a hydraulic pump, with the valves in the perforating veins preventing reflux to the deep foot veins during offloading [21]. Each pump of the foot and calf during weight-bearing (toe curls, electrical stimulation, passive compression, and posture) is estimated to move approximately 33 mL of blood into the popliteal vein at the knee, with 20% of this flow arising from the veins passing the ankle [25]. The foot, calf, and thigh muscle pumps overcome pressures of approximately 90 mmHg in standing and 20 mmHg during walking [27]. Failure in any of these pumps through valve dysfunction or vein obstruction will cause a compromise in venous return and negatively impact the local lymphatics. If this becomes ongoing or chronic, venous and lymphatic dysfunction will ensue along with impaired tissue integrity.
Impaired venous return typically results in the signs and symptoms of chronic venous insufficiency. Venous reflux is due to valve incompetence resulting from congenital, primary, or secondary thrombotic diseases. The main cause of venous reflux in the case of valve incompetence is a poorly functioning muscle pump [15,28]. Most venous reflux affects superficial and perforating veins, but sometimes, only deep veins or all three vein types are affected [29]. Leg vein dysfunction results in aching/heaviness, foot–ankle swelling, skin changes, and the potential for ulceration, which can be mild or incapacitating [27,29,30]. Skin changes may include the characteristic venous stasis changes noted with CVI, such as hemosiderin staining, lipodermatosclerosis, and ulceration. If not adequately managed, venous reflux and resulting lymphedema can increase the risk of serious infections in the lower extremities. Recurrent infections and cellulitis further damage veins and lymphatics, creating a vicious vascular and tissue compromise cycle. Further risk involves the formation of blood clots or thrombosis, both deep and superficial (thrombophlebitis). This can cause local damage at the thrombus site. If the clot becomes dislodged from the deep system, it can travel to the heart and the lungs, resulting in a pulmonary embolus. Occasionally, in the setting of patent foramen ovale, it can even reach the arterial circulation and travel to the brain, resulting in stroke. This sequela also negatively impacts the local lymphatics by anatomical proximity and through the direct effects of the characteristic changes noted with CVI, reiterating the interconnection of these systems. For example, research has shown that heme-containing proteins suppress lymphatic pumping [31]. With venous reflux, blood escapes the veins into the interstitial tissues. The hemoglobin and iron lyse and stain the tissues from the inside out, resulting in hemosiderin staining. The presence of these blood constituents in the interstitial tissues, rather than contained within the vein wall, can suppress local lymphatic contractility and pumping, further contributing to edema formation. The subsequent edema can also limit arterial inflow, which may lead to inadequate perfusion, further contributing to the vicious cycle of vascular and tissue compromise. Management should involve a combination of skincare, compression, and exercise.
A related topic relevant to the health of both the venous and lymphatic systems is obesity. Obesity can cause ‘obesity-induced lymphedema’ or OIL, and a body mass index (BMI) threshold exists between 50 and 60 where lymphatic dysfunction occurs [32,33]. Adipose tissue, an endocrine organ, produces the hormone adipokinase. Too many adipokines harm the lymphatics, rendering them leaky and impairing contractility. As the lymph stagnates, this stimulates new adipose tissue, creating a vicious cycle [34]. Additionally, many obese individuals suffer from immobility, which can negatively impact the muscle pump supporting venous health, and an overhanging abdominal wall can compress lymphatic and venous structures, further inducing negative consequences on both systems. Lipedema, a fat disorder separate from obesity, shares similar clinical features with lymphedema, such as edema, adipose expansion, and fibrosis [35]. Mechanistic understandings of these diseases are being explored as they have similar pathophysiological aspects, suggesting a link between the two disease manifestations [35]. Further evidence must be explored looking at lipedema’s impact on venous health and physiology.
Exercise and mobility are known to positively affect venous and lymphatic health. A systematic review found that exercise training (ET) benefits patients with mild and severe CVI. In cases of mild CVI, ET improves venous reflux, ankle range of motion, muscle strength, and health-related quality of life [36]. For those with severe CVI and associated skin impairments, improvements in ejection fraction, residual volume, ankle range of motion, and muscle strength are evident without changing venous reflux parameters [36]. The benefits of exercise are enhanced with compression and mobility, specifically walking. The benefits of reducing venous hypertension through exercise and compression help produce nitric oxide, a potent neuromodulator of venous tone. This also offsets hypoxic injury resulting from platelet aggregation and neutrophil adhesion, a common venous disease sequela [37].
In conclusion, the homeostasis of the circulatory system involves a delicate balance maintained through the anatomy and healthy physiology of the veins, arteries, and lymphatics of the foot and lower leg, the pumping action of the muscles and respiratory cycle, and the skin. All must work collectively and effectively to prevent dysregulation of the organism. Industrialized and developed nations have higher incidence rates of venous disease, likely attributed to more sedentary lifestyles [38]. The simple act of walking, regular exercise, proper breathing, and wearing compression can mitigate the deleterious effects of venous and lymphatic dysfunction by supporting vein valve functioning. When appropriate, weight loss and BMI modification are also beneficial. Empowering patients to be mobile and exercise within the context of their clinical and medical presentation is vital to maintaining health. The benefits of such simple actions should not be overlooked, and regular treatment interventions should be included in the care plan of such individuals. Hence, “live to move and move to live” should be a mantra adopted by all within each person’s individual abilities.
Funding
This research received no external funding.
Conflicts of Interest
Heather Barnhart is the Director of Clinical Affairs for Koya Medical.
References
- Tehan, P.; Piller, N. The often-ignored importance of the lymphatics of the foot and legs: The sole of the lymphatic system. J. Lymphoedema 2023, 18, 5–6. [Google Scholar]
- Gordon, K.; Varney, R.; Keeley, V.; Riches, K.; Jeffery, S.; Van Zanten, M.; Mortimer, P.; Ostergaard, P.; Mansour, S. Update and audit of the St George’s classification algorithm of primary lymphatic anomalies: A clinical and molecular approach to diagnosis. J. Med. Genet. 2020, 57, 653–659. [Google Scholar] [CrossRef]
- Sleigh, B.; Mann, B. Lymphedema; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK537239/ (accessed on 19 April 2021).
- Levick, J.; Michel, C. Microvascular fluid exchange and the revised Starling principle. Cardiovasc. Res. 2010, 87, 198–210. [Google Scholar] [CrossRef] [PubMed]
- Reitsma, S.; Slaaf, D.; Vink, H. The endothelial glycocalyx: Composition, functions, and visualization. Pflug. Arc. 2007, 454, 345–359. [Google Scholar] [CrossRef] [PubMed]
- Weinbaum, S.; Tarbell, J.; Damiano, E. The structure and function of the endothelial glycocalyx layer. Annu. Rev. Biomed. Eng. 2007, 9, 121–167. [Google Scholar] [CrossRef]
- Mortimer, P.; Pearson, I. Lymphatic function in severe chronic venous insufficiency. Phlebolymphology 2004, 44, 253–257. [Google Scholar]
- Zawieja, D.C. Contractile physiology of lymphatics. Lymphat. Res. Biol. 2009, 7, 87–96. [Google Scholar] [CrossRef]
- Domenico, R. Historical overview of lymphangiogenesis. Curr. Opin. Immunol. 2018, 53, 161–166. [Google Scholar] [CrossRef]
- Arnoldi, C. On the Conditions for the Venous Return From the Lower Leg in Healthy Subjects and in Patients with Chronic Venous Insufficiency. Angiology 1966, 17, 153–171. [Google Scholar] [CrossRef]
- Hojensgard, C.; Sturup, H.; Hojensgard, H. Static and Dynamic Pressures in Superficial and Deep Veins of the Lower Extremity in Man. Acta Physiol. Scand. 1952, 27, 49–67. [Google Scholar] [CrossRef]
- Kuiper, P. Venous pressure determination (direct method). Dermatologica 1966, 132, 206–217. [Google Scholar] [CrossRef] [PubMed]
- Pollack, A.; Taylor, E. The effect of exercise and body position on the venous pressure at the ankle in patients having venous valvular defects. J. Clin. Investig. 1949, 28, 559–563. [Google Scholar] [CrossRef] [PubMed]
- Stegall, F. Muscle Pumping in the Dependent Leg. Circ. Res. 1966, 19, 180–190. [Google Scholar] [CrossRef]
- Tauraginskii, R.; Lurie, F.; Simakov, S.; Agalarov, R.; Khramtsov, P.; Babushkin, M.; Borsuk, D.; Galchenko, M. Human lower leg muscle pump acts like a stream diversion pump during locomotion. bioRxiv 2023. [Google Scholar] [CrossRef]
- Simka, M. Calf muscle pump dysfunction in patients with severe chronic venous insufficiency. Phlebolymphology 2004, 47, 299–303. [Google Scholar]
- Araki, C.T.; Back, T.L.; Padberg, F.T.; Thompson, P.N.; Jamil, Z.; Lee, B.C.; Duran, W.N.; Hobson, R.W. The significance of the calf muscle pump function in venous ulceration. J. Vasc. Surg. 1994, 20, 872–879. [Google Scholar] [CrossRef] [PubMed]
- Jamalian, S.; Jafarnejad, M.; Zawieja, S.D.; Bertram, C.D.; Gashev, A.A.; Zawieja, D.C.; Davis, M.J.; Moore, J.E. Demonstration and Analysis of the Suction Effect for Pumping Lymph from Tissue Beds at Subatmospheric Pressure. Sci. Rep. 2017, 7, 12080. [Google Scholar] [CrossRef]
- Takata, M.; Robotham, J.L. Effects of inspiratory diaphragmatic descent on inferior vena canal venous return. J. App. Phys. 1992, 72, 597–607. [Google Scholar]
- Miller, J.D.; Pegelow, D.F.; Jacques, A.J.; Dempsey, J.A. Skeletal muscle pump versus respiratory muscle pump: Modulation of venous return from the locomotor limb in humans. J. Phys. 2005, 563, 925–943. [Google Scholar]
- Horwood, A. The venous foot pump: Modelling its function in gait. Podiatry Rev. 2021, 78, 19–23. [Google Scholar]
- Meissner, M.H. Lower extremity venous anatomy. Sem. Int. Radiol. 2005, 22, 147–156. [Google Scholar] [CrossRef]
- Ricci, S. The venous system of the foot: Anatomy, physiology, and clinical aspects. Phlebolymphology 2015, 22, 64–75. [Google Scholar]
- Ricci, S.; Moro, L.; Incalzi, R.A. The foot venous system: Anatomy, physiology, and relevance to clinical practice. Derm. Surg. 2014, 40, 225–233. [Google Scholar] [CrossRef]
- Broderick, B.J.; Corley, G.J.; Quondamatteo, F.; Breen, P.P.; Serrador, J.; ÓLaighin, G. Venous emptying of the foot: Influences of weight bearing, toe curls, electrical stimulation, passive compression, and posture. J. App. Phys. 2010, 109, 1045–1052. [Google Scholar] [CrossRef]
- Corley, G.J.; Broderick, B.J.; Nestor, S.M.; Breen, P.P.; Grace, P.A.; Quondamatteo, F.; Ólaighin, G. The anatomy and physiology of the venous foot pump. Anat. Rec. 2010, 293, 370–378. [Google Scholar] [CrossRef]
- Reeder, S.; Maessen-Visch, M.; Langendoen, S.; de Roos, K.; Neumann, H. The recalcitrant venous leg ulcer—A never ending story? Phlebologie 2013, 42, 332–339. [Google Scholar]
- Tauraginskii, A.; Lurie, F.; Simakov, S.; Agalarov, R. Venous reflux in the great saphenous vein is driven by a suction force provided by the calf muscle pump in the compression–decompression maneuver. J. Vasc. Surg. Venous Lymphat. Disord. 2021, 9, 1282–1290. [Google Scholar] [CrossRef] [PubMed]
- Labropoulos, N.; Touloupakis, E.; Giannoukas, A.D.; Leon, M.; Katsamouris, A.; Nicolaides, A.N. Recurrent varicose veins: Investigation of the pattern and extent of reflux with color flow duplex scanning. Surgery 1996, 119, 406–409. [Google Scholar] [CrossRef]
- Brandjes, D.P.M.; Büller, H.R.; Heijboer, H.; Huisman, M.V.; de Rijk, M.; Jagt, H.; ten Cate, J.W. Randomised trial of effect of compression stockings in patients with symptomatic proximal-vein thrombosis. Lancet 1997, 349, 759–762. [Google Scholar] [CrossRef] [PubMed]
- Wandolo, G.; Elia, R.; Ranadive, N.; Johnston, M. Heme-containing proteins suppress lymphatic pumping. J. Vasc. Res. 1992, 29, 248–255. [Google Scholar] [CrossRef]
- Greene, A.; Grant, F.; Slavin, S. Lower-extremity lymphedema and elevated body-mass index. N. Engl. J. Med. 2012, 366, 2136–2137. [Google Scholar] [CrossRef] [PubMed]
- Greene, A.K.; Grant, F.D.; Slavin, S.A.; Maclellan, R.A. Obesity-induced lymphedema: Clinical and lymphoscintrigraphic features. Plast. Reconstr. Surg. 2015, 135, 1715–1719. [Google Scholar] [CrossRef] [PubMed]
- Kataru, R.P.; Park, H.J.; Baik, J.E.; Li, C.; Shin, J.; Mehrara, B.J. Regulation of lymphatic function in obesity. Front. Physiol. 2020, 11, 459. [Google Scholar] [CrossRef] [PubMed]
- Duhon, B.H.; Phan, T.T.; Taylor, S.L.; Crescenzi, R.L.; Rutkowski, J.M. Current mechanistic understandings of lymphedema and lipedema: Tales of fluid, fat and fibrosis. Int. J. Mol. Sci. 2022, 23, 6621. [Google Scholar] [CrossRef] [PubMed]
- Silva, K.; Figueiredo, E.; Lopes, C.; Vianna, M.; Lima, V.; Figueiredo, P.; Costa, H. The impact of exercise training on calf pump function, muscle strength, ankle range of motion, and health-related quality of life in patients with chronic venous insufficiency at different stages of severity: A systematic review. J. Vasc. Bras. 2021, 20, e20200125. [Google Scholar] [CrossRef]
- Elsisi, H.; Mahmoud, T.; Serry, Z.; Rahmy, A.; Osman, N. Effect of strengthening exercise versus intermittent pneumatic compression device to calf muscle on blood flow in patients with varicose Veins. Biosci. Res. 2019, 16, 2360–2368. [Google Scholar]
- Singh, A.; Zahra, F. Chronic Venous Insufficiency. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK587341/ (accessed on 27 April 2023).
Figure 1.
Calf muscle pump effects on venous return (image Koya Medical Inc.).

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Barnhart, H. Live to Move and Move to Live: The Health of the Lymphatic System Relies on Mobility and the Foot and Calf Pump Connection. Lymphatics 2024, 2, 43-49. https://doi.org/10.3390/lymphatics2020004
AMA Style
Barnhart H. Live to Move and Move to Live: The Health of the Lymphatic System Relies on Mobility and the Foot and Calf Pump Connection. Lymphatics. 2024; 2(2):43-49. https://doi.org/10.3390/lymphatics2020004
Chicago/Turabian StyleBarnhart, Heather. 2024. "Live to Move and Move to Live: The Health of the Lymphatic System Relies on Mobility and the Foot and Calf Pump Connection" Lymphatics 2, no. 2: 43-49. https://doi.org/10.3390/lymphatics2020004