
Motion Management: The Road Map to Accurate Radiation Treatment Delivery


Department of Radiation Oncology, University of Texas MD Anderson Cancer Center, Houston, TX 77030, USA
*
Author to whom correspondence should be addressed.
Lymphatics 2024, 2(1), 1-9; https://doi.org/10.3390/lymphatics2010001
Submission received: 31 August 2023
/
Revised: 5 October 2023
/
Accepted: 13 November 2023
/
Published: 1 January 2024
(This article belongs to the Collection Radiation Oncology)
Abstract
:Radiation therapy is a key contributor to positive outcomes in hematological malignancies. However, this is contingent on minimizing the exposure of critical normal organs. The introduction of computed tomography (CT) for radiation treatment planning and the development of sophisticated dose calculation algorithms has transformed the radiation therapy field and made it possible to transition from conventional involved-field radiation to modern involved-site radiation therapy. Thanks to rapid advances in drug discovery, treatment strategies for many hematological malignancies have evolved to incorporate targeted and cellular therapies, in some cases even allowing the replacement of chemotherapy. As a result, new opportunities have been created for radiation to address relapses after more lines of therapy, identify disease-involving sanctuary sites, and bridge to the subsequent therapy. When considering radiation in patients receiving novel therapies, who may also be more heavily pretreated, respecting the critical and normal structures at all costs is imperative. In this document, we will describe modern techniques used to deliver state-of-the-art radiation therapy and practical considerations to ensure the accurate treatment of the target while avoiding normal organs at risk.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Importance of Motion Management
Controlling internal motion will reduce the radiation field and better avoid organs at risk. Accurate target localization during radiation treatment is critical and often requires that we account for variability due to daily patient setup, respiratory motion, physiologic changes in bowel position, and the effect of radiation on the tumor itself during treatment. Mitigating patient daily setup variation using immobilization devices and the accurate transfer of setup coordinates is now well established in radiation therapy treatment; however, a more significant challenge lies with internal motion management. Internal motion management allows a reduction in radiation field size, leading to the sparing of organs at risk while continuing to ensure adequate target coverage.
The following examples depict motion management techniques in different anatomic locations to illustrate how to cover the target while minimizing the dose to at-risk organs. These examples are limited to motion management and assume the best planning technique is applied.
2. Motion Management for Chest Location
In the case of radiation treatment to the chest, organs at risk that can benefit from motion management include the lungs, heart, and breasts. Deep inspiration breath hold (DIBH) has been shown to reduce the lifetime excess risk of the development of cardiovascular disease and secondary lung and breast cancer [8,9]. Comparisons between radiation plans with and without DIBH have demonstrated remarkably lower excess mean radiation doses to the surrounding critical organs. While DIBH is expanding the lungs, the heart moves craniocaudally away from the target volume, for instance, the mediastinum, with the latter action occurring in addition to being fixed, and it becomes thinner and relatively smaller than its corresponding volume in free breathing. Thus, DIBH, when planning radiation treatment, will result in relatively lower doses to the lungs, heart, and breasts.
DIBH can be achieved using many different systems; however, more important than the system used is the precision of the breath hold position, which must be reproducible to enable smaller planning target volume (PTV) expansions. As the PTV accounts for uncertainty in positioning, the target should be confirmed via CT-based image guidance prior to each fraction.
2.1. The Benefit of DIBH for Treating Mediastinal Location
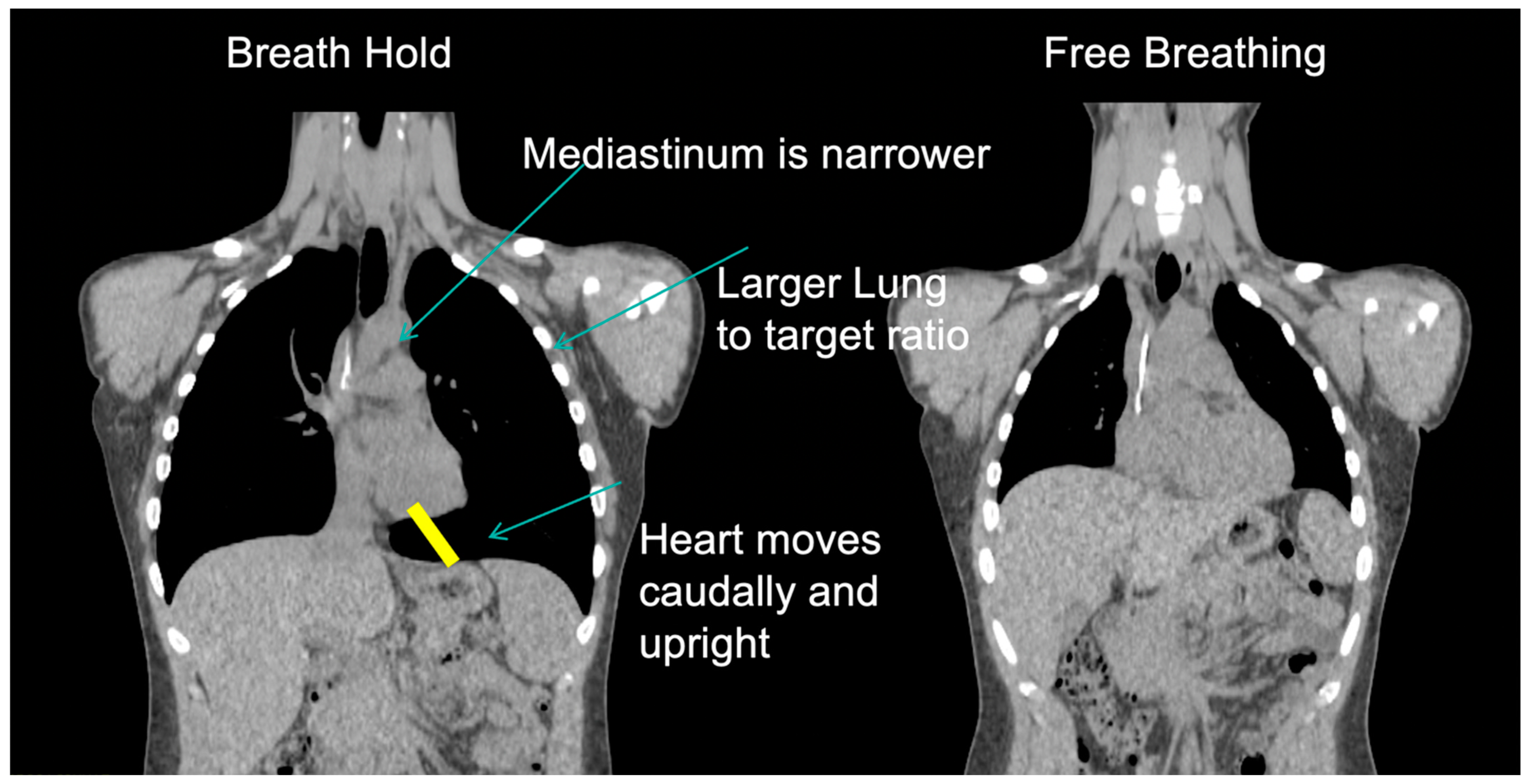
In addition to enabling the treatment of smaller volumes by limiting target motion during the respiratory cycle, the mediastinum site becomes thinner, and the orientation of the heart is more craniocaudal. The net result is a smaller target, larger lung volumes, and the displacement of the heart away from the target (Figure 1).
2.2. The Benefit of DIBH for Treating the Axillary Location
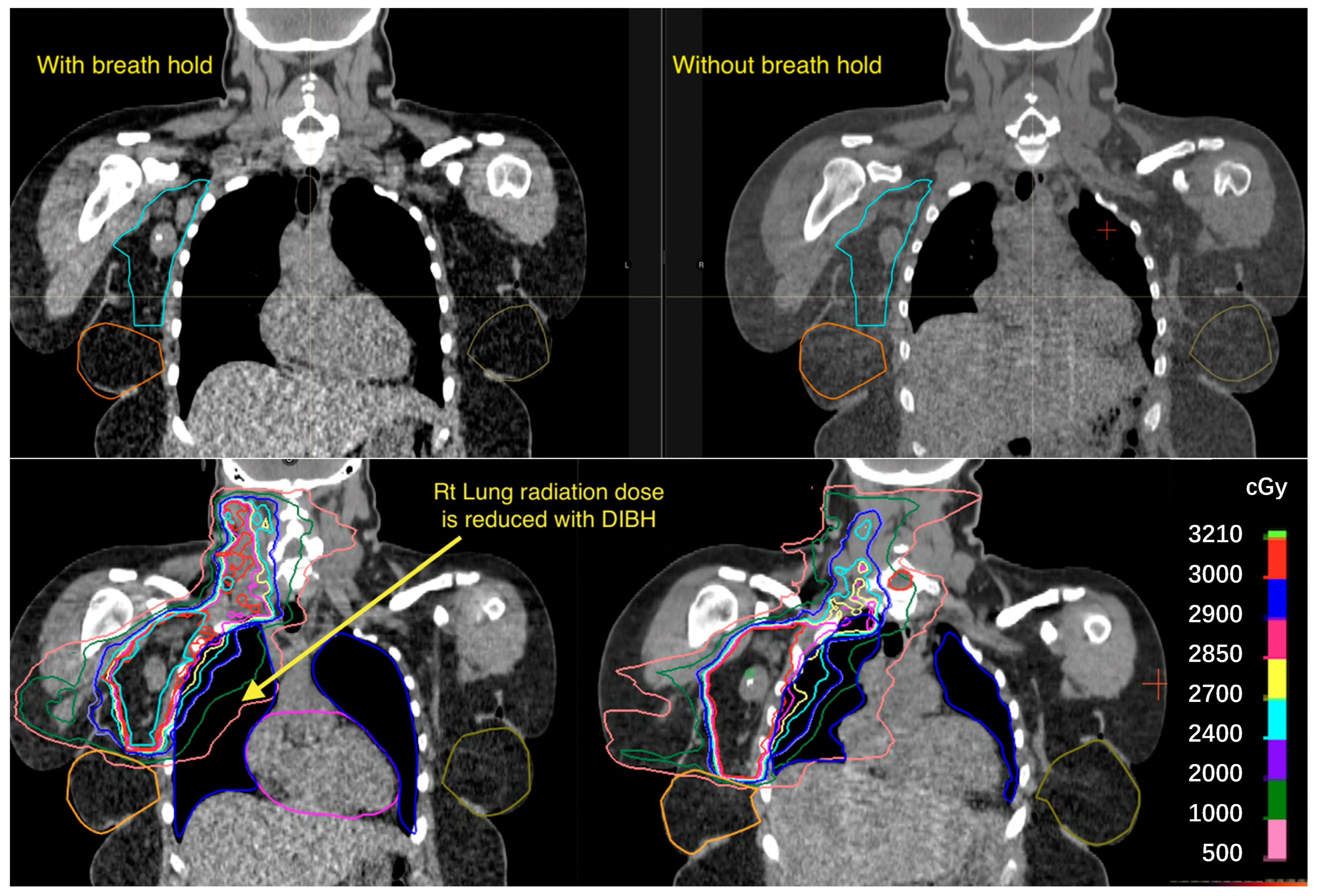
The main benefit of DIBH in terms of treating the axilla is reducing the excess dose to the lungs (Figure 2).
2.3. The Impact of Arm Positioning
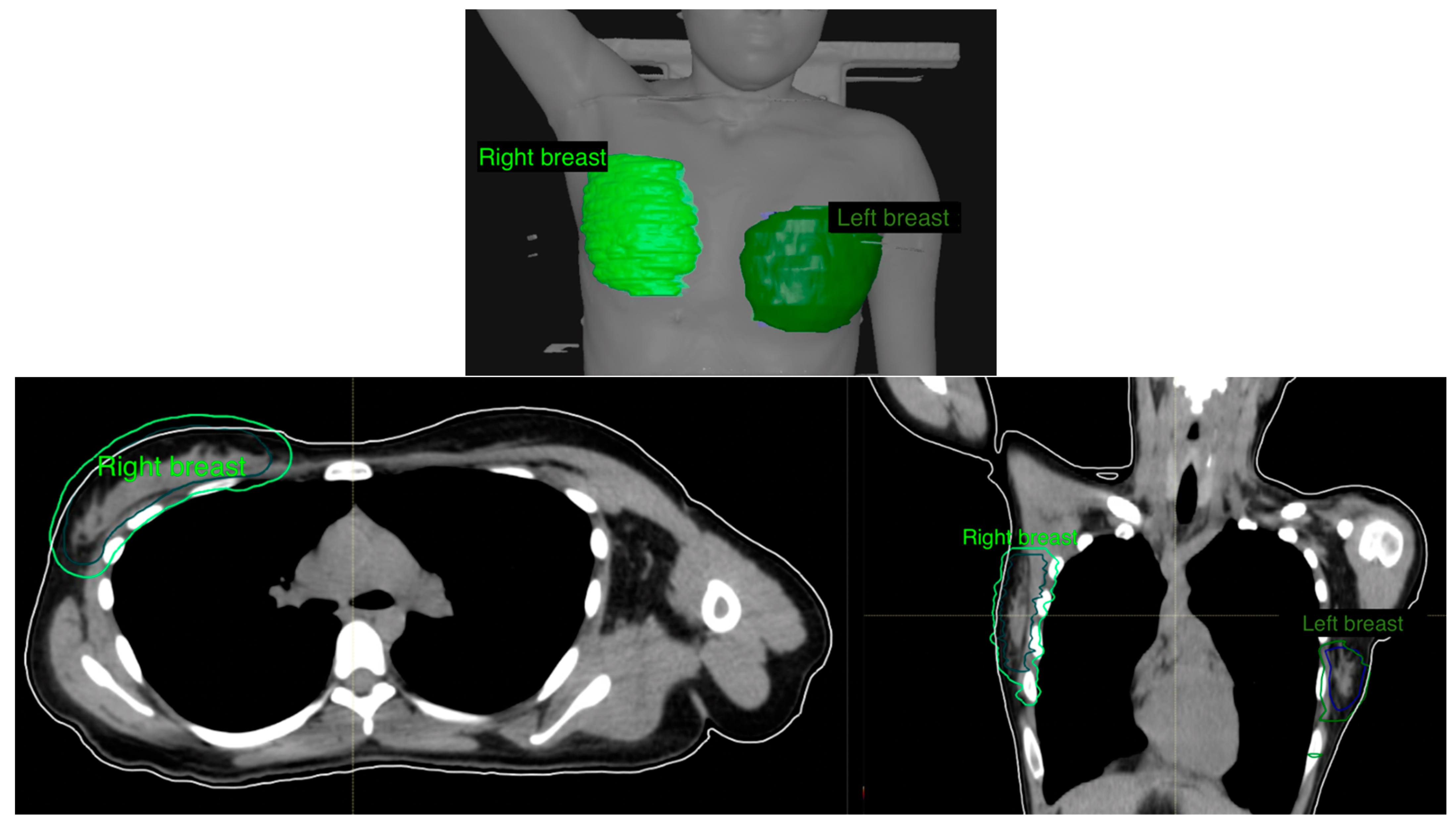
Keeping the arms down when treating the mediastinum is critical to keeping the breasts below the level of the radiation field, thus avoiding administering an excess radiation dose to the breasts, which could happen when the arm is moved up, where it pulls the breasts to the level of the target volume (Figure 3).
One exception to this would be when treating the axilla, and in that case, moving the arm up may reduce the excess radiation to the lungs. However, the relative benefit of reducing the lung dose compared to the breast dose should be evaluated on a case-by-case basis.
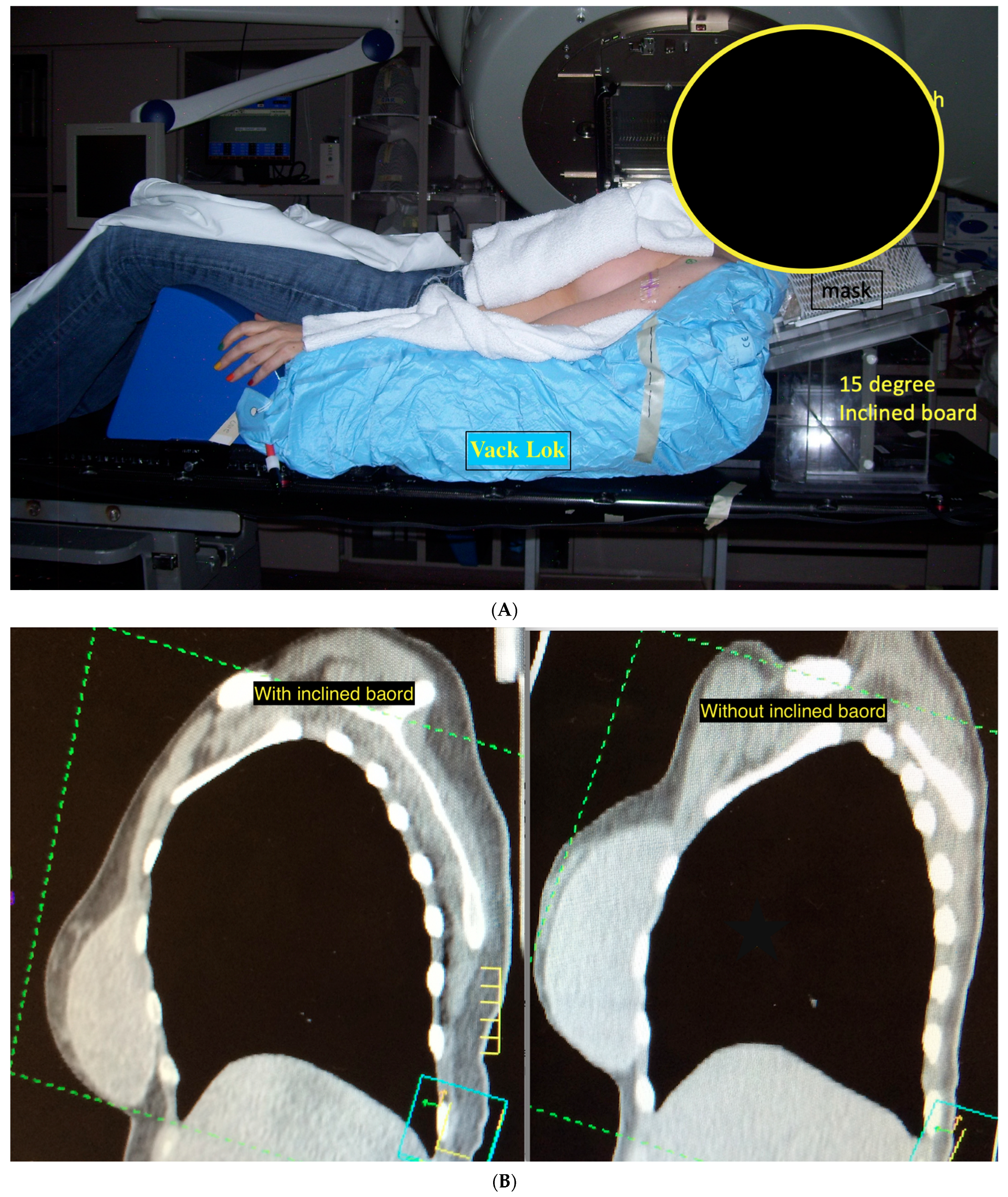
2.4. The Benefit of Using an Incline Board
3. Motion Management for Abdominal Location
In the case of radiation treatment of the abdomen, organs at risk include the spleen, heart, liver, and kidneys.
Treatment of the Stomach
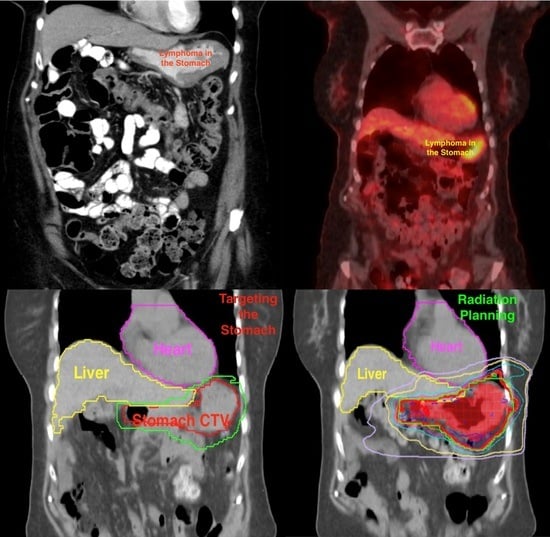
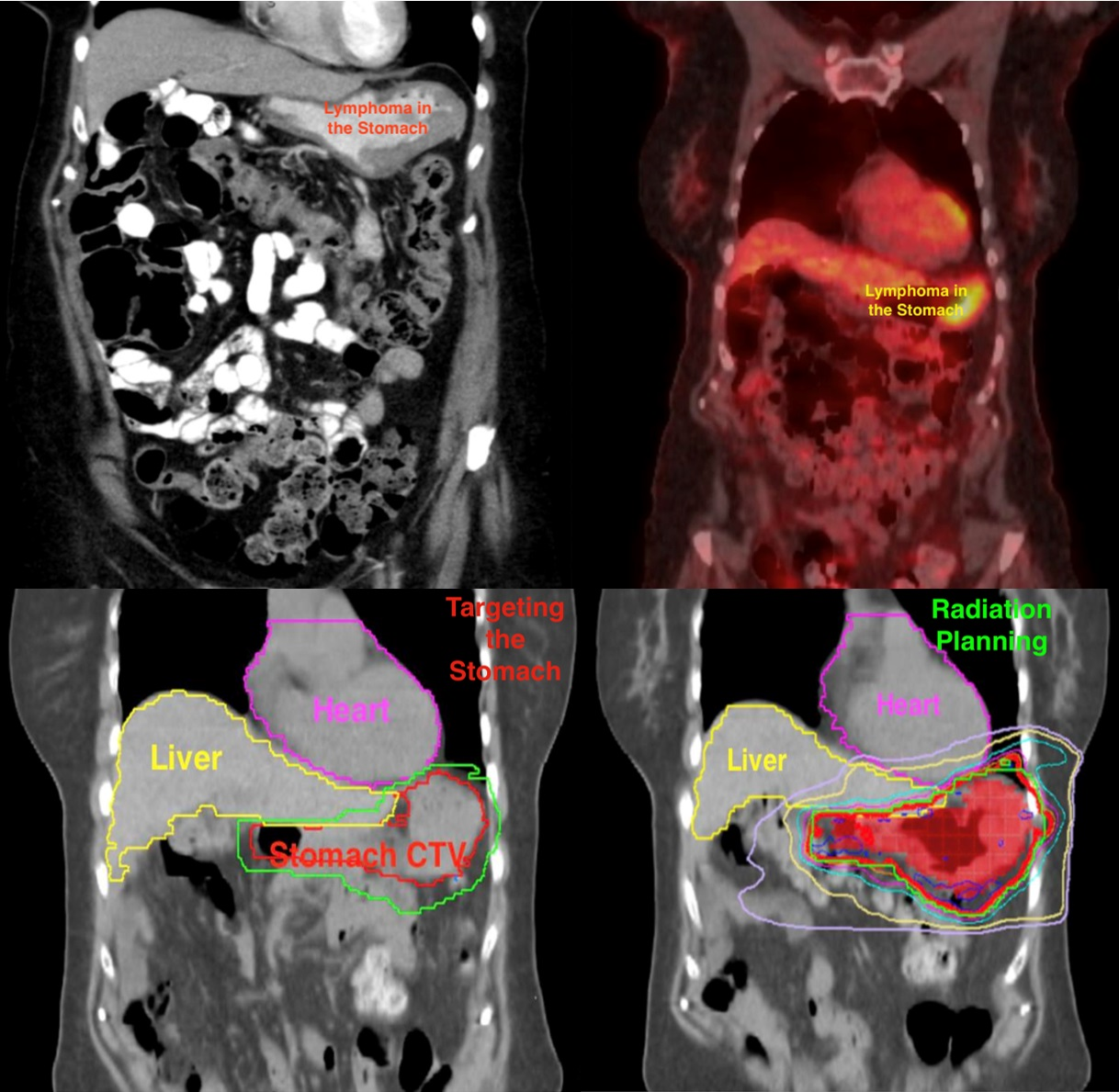
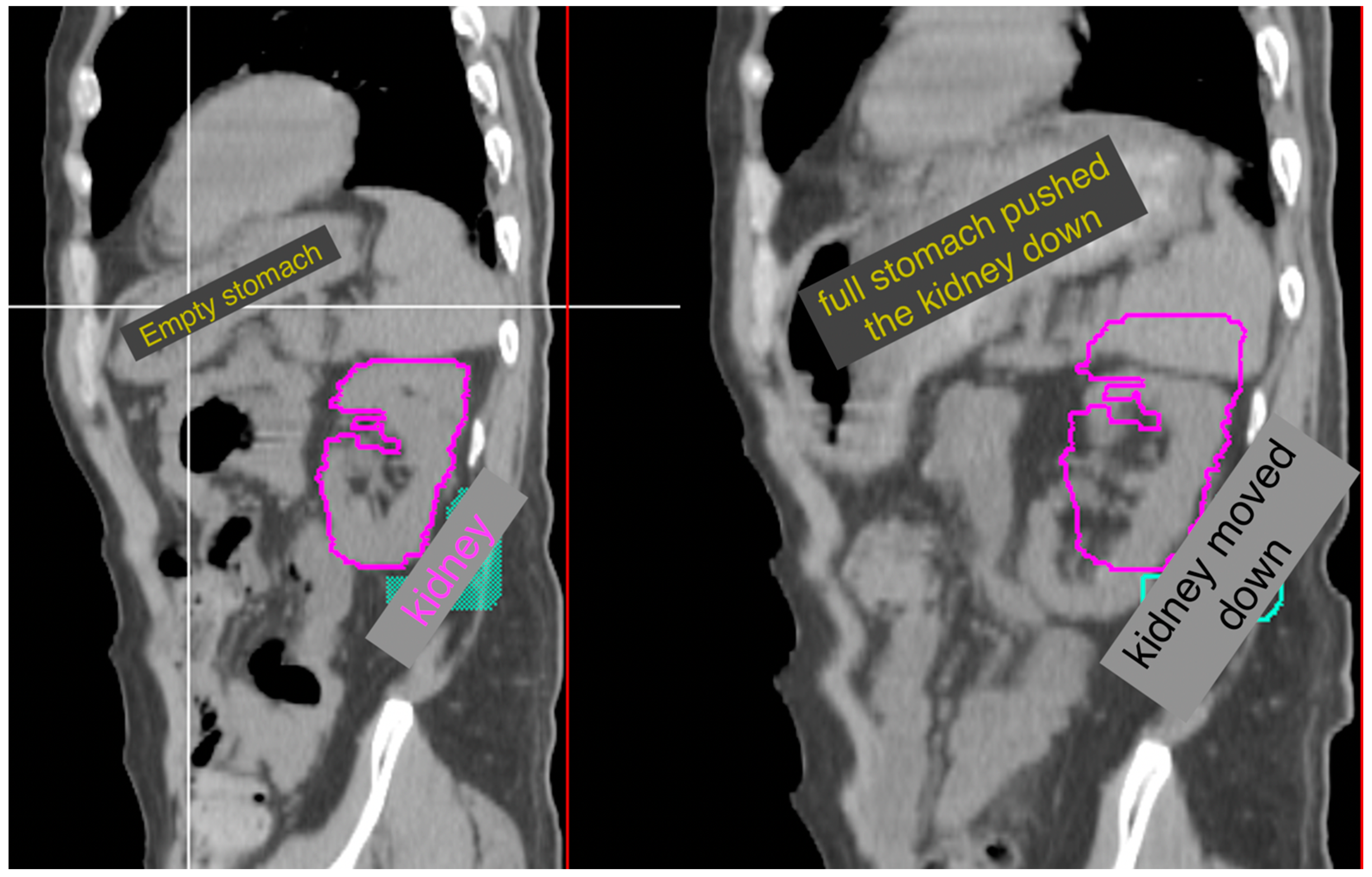
Regardless of whether the stomach is a target or an organ at risk, the stomach volume is extremely variable and dependent on many factors. In addition to the timing of the last meal, the contents of that meal and patient-specific factors (such as gastroparesis in diabetic patients) should be considered, as some patients may require more than 6 h of receiving nothing by mouth to ensure that their stomach is empty. When treating the stomach, ensuring treatment with an empty stomach will reduce the radiation field. Variable stomach filling may also impact other critical organs at risk, such as the kidneys, and this impact may be hard to predict [11] (Figure 5).
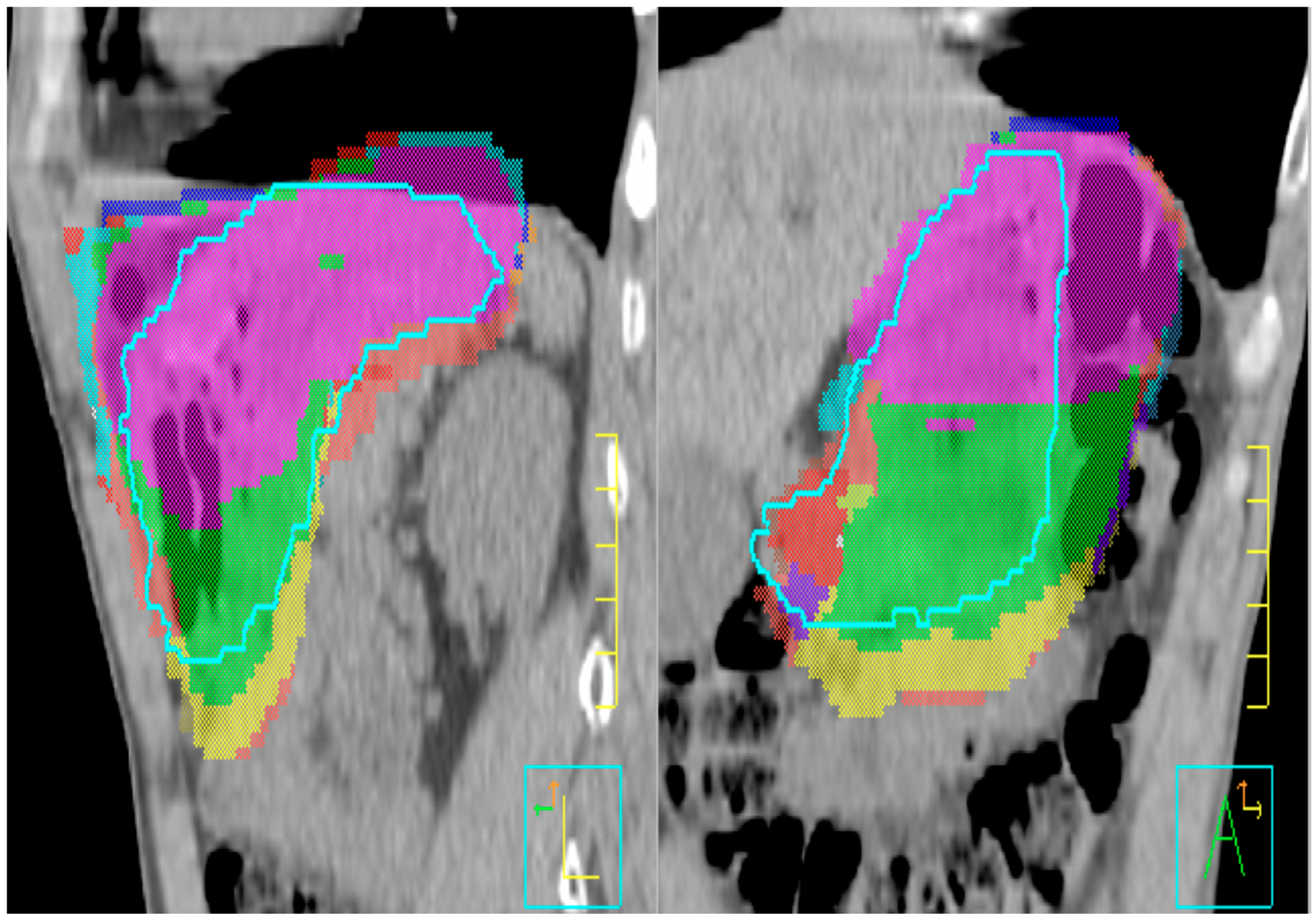
In a study of 12 patients treated with radiation to the stomach using the breath-hold technique and the restriction of oral intake and dosimetry calculations of 229 daily CT images during treatment, there was substantial inter-fractional variation in the stomach volume, suggesting that daily CT scan is necessary to ensure accurate coverage [1] (Figure 6).
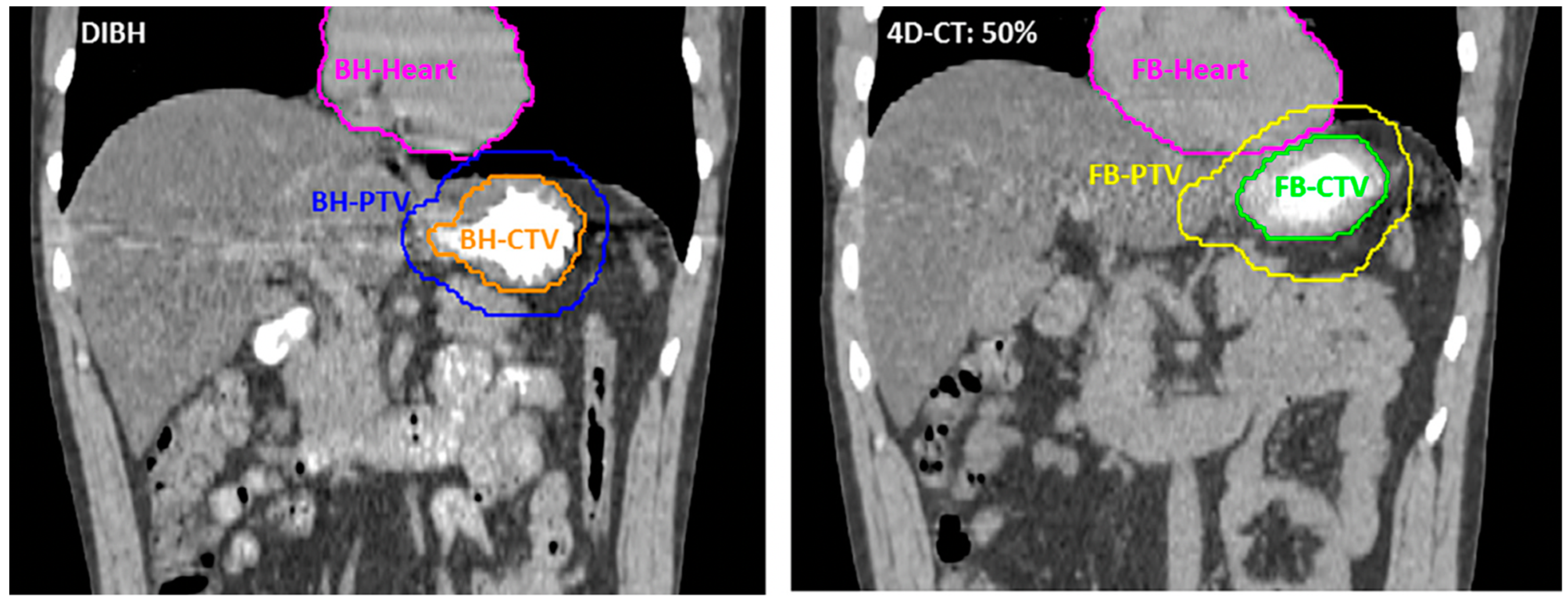
When treating the stomach, using the deep inspiration breath hold is essential to create a gap between the stomach and organs at risk in the upper abdomen, such as the heart [12] (Figure 7).
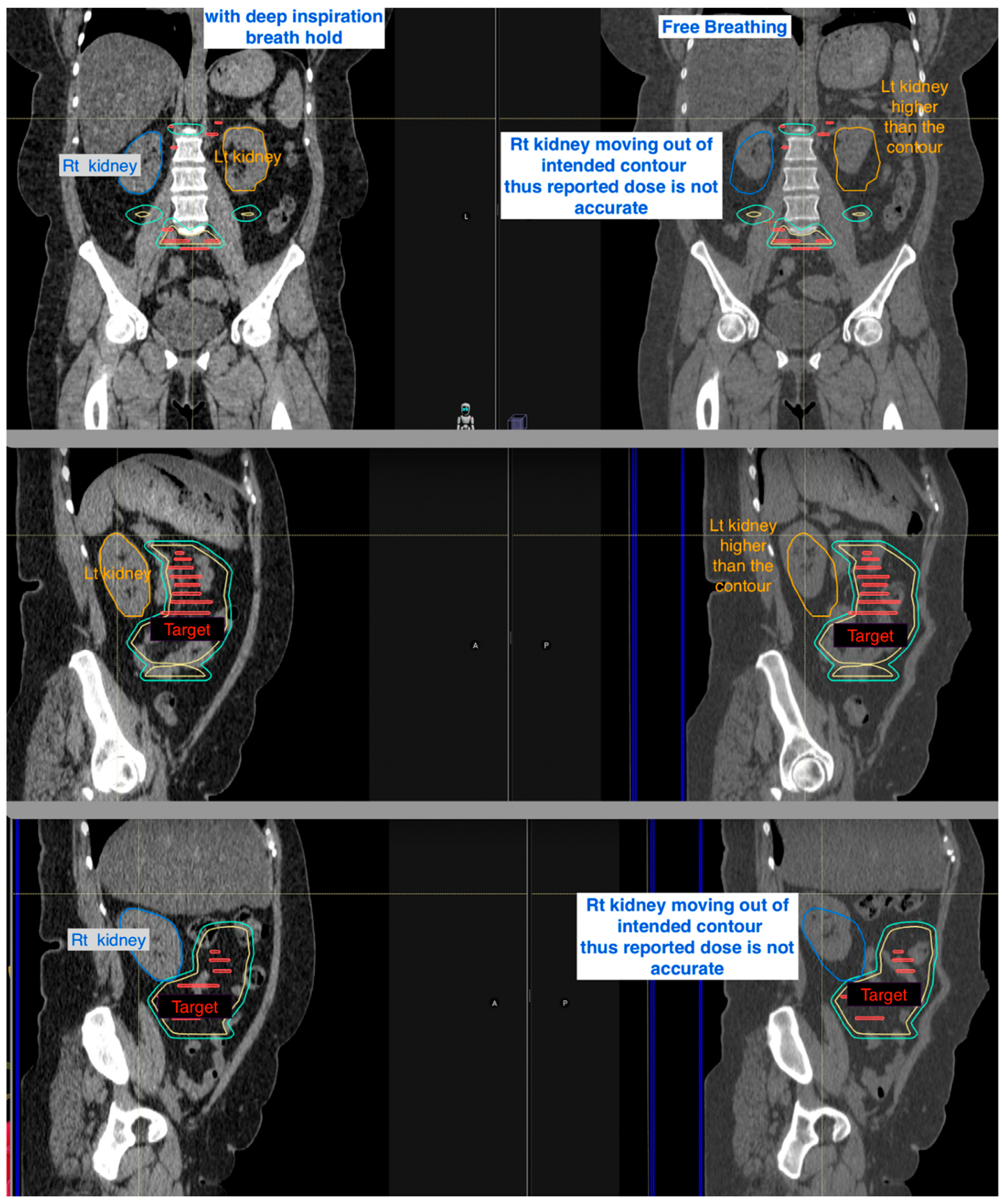
Additionally, the benefit of DIBH can be seen for mesenteric sites is to reduce the planning target volume and stabilize the position of the kidneys (Figure 8).
4. Onboard Image Guidance and Adaptive Treatment Planning
Image guidance helps to confirm the positions of both the radiation target and organs at risk. This ensures that the target is not missed while also ensuring the organs at risk do not receive an extra radiation dose. Onboard imaging can also help to detect changes in the tumor volume, both in terms of response and progression.
Therefore, in order to responsibly apply motion management with the goal of limiting toxicity related to treatment, as described above, image guidance is a necessity.
Onboard imaging/image guidance helps to ensure the reproducibility of daily setup and internal motion control while also locating a moving target [1,11].
Abdominal masses are often mobile and may be in different positions from day to day. Daily image guidance is critical to localize the tumor in order to successfully guide treatment delivery.
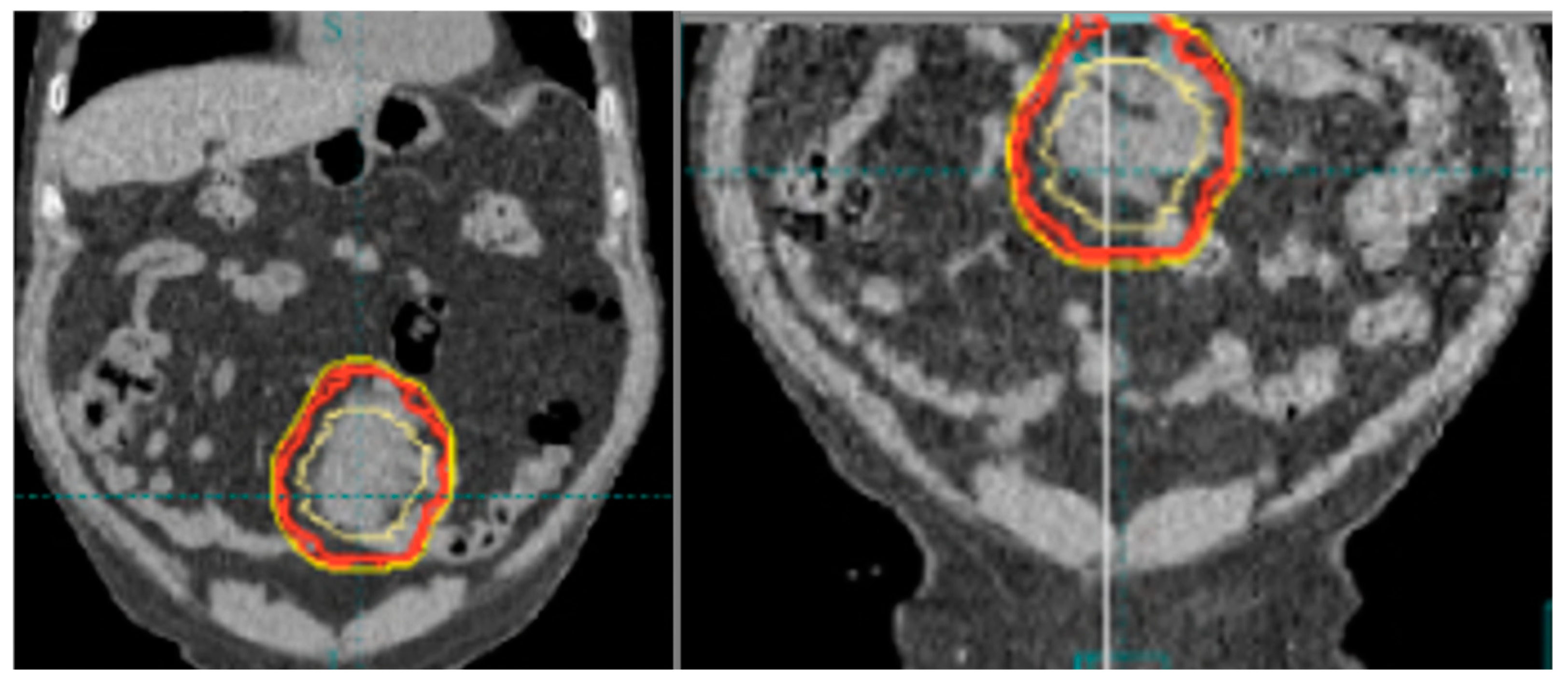
Below (Figure 9) are two examples of the benefits of using onboard imaging to successfully treat movable masses that could only be treated thanks to technological advancement.
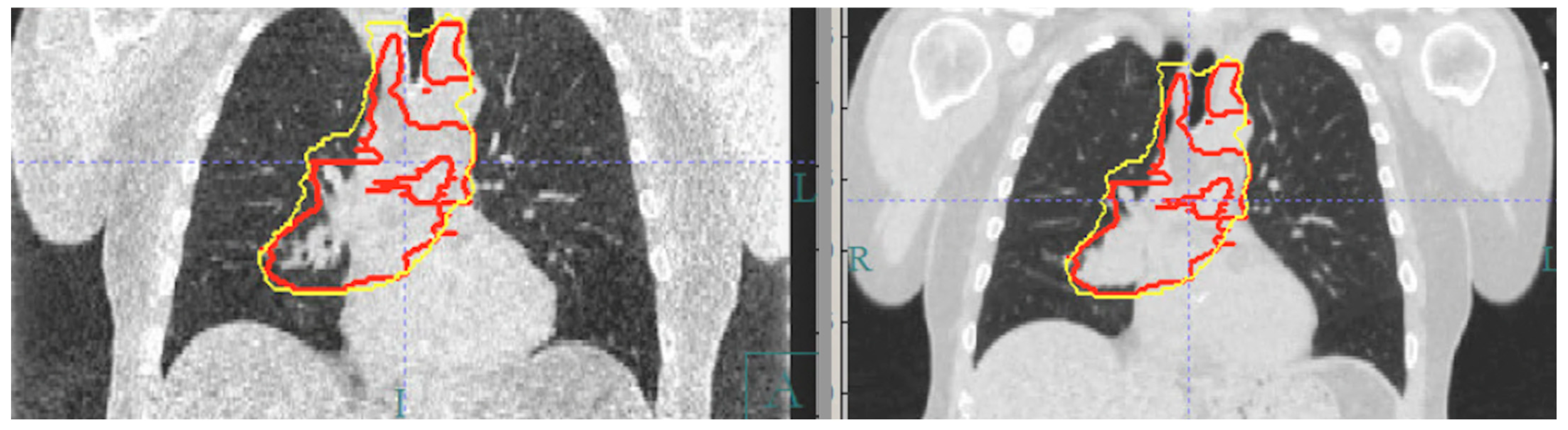
Image guidance can also help to monitor changes in the target during a treatment course, which is particularly important for radiosensitive tumors. As tumors respond to radiation, normal organs at risk may wind up in the treatment field. Adaptive replanning can account for these changes and limit radiation dose to normal tissues while maintaining coverage of the tumor (Figure 10).
5. Conclusions
Together, modern image guidance and DIBH ensure safe, effective radiation treatment delivery in locations where limiting the dose to organs at risk is of paramount importance. In the thorax, DIBH decreases the dose to the heart and lungs, while in the abdomen, DIBH helps to limit the dose to the heart and kidneys. Practical considerations at simulation, including arm position, the use of an incline board, and requiring patients to fast when treating GI locations, can further limit the dose to the breasts, heart, and kidneys. Daily image guidance also enables the close monitoring of disease response, so that plans can be adapted to further limit the dose to normal tissues. By routinely incorporating all of these considerations into patient setup and treatment planning, we were able to limit both the acute and late side effects of radiation. As we identify new opportunities to incorporate radiation with novel systemic therapies, minimizing treatment-related toxicity without compromising treatment delivery is critical.
Author Contributions
All authors contributed to the conception and editing of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available in article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Dabaja, B.; Perrin, K.J.; Romaguera, J.E.; Horace, P.; Wogan, C.F.; Shihadeh, F.; Salehpour, M.R. Successful treatment of a free-moving abdominal mass with radiation therapy guided by cone-beam computed tomography: A case report. J. Med. Case Rep. 2010, 4, 329. [Google Scholar] [CrossRef] [PubMed]
- Katsuta, T.; Matsuura, K.; Kashiwado, K. Analysis of Chronic Kidney Disease after Radiation Therapy for Gastric/Duodenal Mucosa-Associated Lymphoid Tissue Lymphoma. Adv. Radiat. Oncol. 2021, 6, 100788. [Google Scholar] [CrossRef] [PubMed]
- Chadha, A.S.; Liu, G.; Chen, H.C.; Das, P.; Minsky, B.D.; Mahmood, U.; Delclos, M.E.; Suh, Y.; Sawakuchi, G.O.; Beddar, S.; et al. Does Unintentional Splenic Radiation Predict Outcomes after Pancreatic Cancer Radiation Therapy? Int. J. Radiat. Oncol. Biol. Phys. 2017, 97, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Pinnix, C.C.; Smith, G.L.; Milgrom, S.; Osborne, E.M.; Reddy, J.P.; Akhtari, M.; Reed, V.; Arzu, I.; Allen, P.K.; Wogan, C.F.; et al. Predictors of radiation pneumonitis in patients receiving intensity modulated radiation therapy for Hodgkin and non-Hodgkin lymphoma. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Hahn, E.; Jiang, H.; Ng, A.; Bashir, S.; Ahmed, S.; Tsang, R.; Sun, A.; Gospodarowicz, M.; Hodgson, D. Late Cardiac Toxicity After Mediastinal Radiation Therapy for Hodgkin Lymphoma: Contributions of Coronary Artery and Whole Heart Dose-Volume Variables to Risk Prediction. Int. J. Radiat. Oncol. Biol. Phys. 2017, 98, 1116–1123. [Google Scholar] [CrossRef] [PubMed]
- Mulrooney, D.A.; Yeazel, M.W.; Kawashima, T.; Mertens, A.C.; Mitby, P.; Stovall, M.; Donaldson, S.S.; Green, D.M.; Sklar, C.A.; Robison, L.L.; et al. Cardiac outcomes in a cohort of adult survivors of childhood and adolescent cancer: Retrospective analysis of the Childhood Cancer Survivor Study cohort. BMJ 2009, 339, b4606. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.nccn.org/professionals/physician_gls/pdf/hodgkins.pdf (accessed on 31 August 2023).
- Aznar, M.C.; Maraldo, M.V.; Schut, D.A.; Lundemann, M.; Brodin, N.P.; Vogelius, I.R.; Berthelsen, A.K.; Specht, L.; Petersen, P.M. Minimizing late effects for patients with mediastinal Hodgkin lymphoma: Deep inspiration breath-hold, IMRT, or both? Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.M.; Aznar, M.C.; Berthelsen, A.K.; Loft, A.; Schut, D.A.; Maraldo, M.; Josipovic, M.; Klausen, T.L.; Andersen, F.L.; Specht, L. Prospective phase II trial of image-guided radiotherapy in Hodgkin lymphoma: Benefit of deep inspiration breath-hold. Acta Oncol. 2015, 54, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Dabaja, B.S.; Rebueno, N.C.; Mazloom, A.; Thorne, S.; Perrin, K.J.; Tolani, N.; Das, P.; Delclos, M.E.; Iyengar, P.; Reed, V.K.; et al. Radiation for Hodgkin’s lymphoma in young female patients: A new technique to avoid the breasts and decrease the dose to the heart. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 503–507. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Milgrom, S.A.; Dabaja, B.S.; Smith, G.L.; Martel, M.; Pinnix, C.C. Daily CT guidance improves target coverage during definitive radiation therapy for gastric MALT lymphoma. Pract. Radiat. Oncol. 2017, 7, e471–e478. [Google Scholar] [CrossRef] [PubMed]
- Christopherson, K.M.; Gunther, J.R.; Fang, P.; Peterson, S.L.; Roach, K.E.; Wong, P.F.; Mirkovic, D.; Lim, T.Y.; Wang, H.; Wang, X.A.; et al. Decreased heart dose with deep inspiration breath hold for the treatment of gastric lymphoma with IMRT. Clin. Transl. Radiat. Oncol. 2020, 24, 79–82. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
DIBH (on the left), free-breathing scan (on the right), demonstrating the difference in position of the mediastinum and heart, as well as expansion of lung volumes with DIBH.
Figure 1.
DIBH (on the left), free-breathing scan (on the right), demonstrating the difference in position of the mediastinum and heart, as well as expansion of lung volumes with DIBH.

Figure 2.
DIBH scans (left) and free breathing scans (right) demonstrate how DIBH increases lung volume and, therefore, reduces the relative volume of the lung in the treatment field.
Figure 2.
DIBH scans (left) and free breathing scans (right) demonstrate how DIBH increases lung volume and, therefore, reduces the relative volume of the lung in the treatment field.

Figure 3.
Impact of arm position on breast position when treating the axilla, with the arm abducted on the right and positioned to the side on the left.
Figure 3.
Impact of arm position on breast position when treating the axilla, with the arm abducted on the right and positioned to the side on the left.

Figure 4.
(A) Example of setup to using an incline board at simulation. (B) This benefit is still appreciated even in the case of breast implants.
Figure 4.
(A) Example of setup to using an incline board at simulation. (B) This benefit is still appreciated even in the case of breast implants.

Figure 5.
Impact of stomach filling on kidney position, with the stomach empty on the left and full on the right.
Figure 5.
Impact of stomach filling on kidney position, with the stomach empty on the left and full on the right.

Figure 6.
Inter-fraction variation in the stomach on daily CT images. Each color represents the stomach shape on different day.
Figure 6.
Inter-fraction variation in the stomach on daily CT images. Each color represents the stomach shape on different day.

Figure 7.
DIBH scan (on the left) and free breathing scan (on the right) demonstrate how DIBH can create space between the heart and the stomach, allowing us to limit the cardiac dose during treatment planning further.
Figure 7.
DIBH scan (on the left) and free breathing scan (on the right) demonstrate how DIBH can create space between the heart and the stomach, allowing us to limit the cardiac dose during treatment planning further.

Figure 8.
DIBH scans (on the left) and free breathing scans (on the right) demonstrate the effects of DIBH on kidney position. Coronal CT images (top panel); Sagittal images focusing on the left kidney in orange color (middle panel); Sagittal images concentrate on the right kidney in blue color (bottom panel).
Figure 8.
DIBH scans (on the left) and free breathing scans (on the right) demonstrate the effects of DIBH on kidney position. Coronal CT images (top panel); Sagittal images focusing on the left kidney in orange color (middle panel); Sagittal images concentrate on the right kidney in blue color (bottom panel).

Figure 9.
Two different daily CT images (left and right) (conventional CT with reduced tube potentials (kV)) of the same patient, and abdominal mass demonstrate how the position of the abdominal mass (gross tumor contoured in yellow and planning margins contoured in red and orange) moved thus emphasize the importance of daily image guidance in these locations.
Figure 9.
Two different daily CT images (left and right) (conventional CT with reduced tube potentials (kV)) of the same patient, and abdominal mass demonstrate how the position of the abdominal mass (gross tumor contoured in yellow and planning margins contoured in red and orange) moved thus emphasize the importance of daily image guidance in these locations.

Figure 10.
The original reference CT image on the right and daily CT image on the left demonstrate a response to treatment, warranting replanning to minimize lung in the treatment field. CT images were created via conventional CT with reduced tube potentials (kV).
Figure 10.
The original reference CT image on the right and daily CT image on the left demonstrate a response to treatment, warranting replanning to minimize lung in the treatment field. CT images were created via conventional CT with reduced tube potentials (kV).

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Dabaja, B.; Wu, S.; Short, N.J. Motion Management: The Road Map to Accurate Radiation Treatment Delivery. Lymphatics 2024, 2, 1-9. https://doi.org/10.3390/lymphatics2010001
AMA Style
Dabaja B, Wu S, Short NJ. Motion Management: The Road Map to Accurate Radiation Treatment Delivery. Lymphatics. 2024; 2(1):1-9. https://doi.org/10.3390/lymphatics2010001
Chicago/Turabian StyleDabaja, Bouthaina, Susan Wu, and Nicholas J. Short. 2024. "Motion Management: The Road Map to Accurate Radiation Treatment Delivery" Lymphatics 2, no. 1: 1-9. https://doi.org/10.3390/lymphatics2010001