
Retinal Structural and Vascular Changes in Patients with Coronary Artery Disease: A Systematic Review and Meta-Analysis
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Statistical Analysis
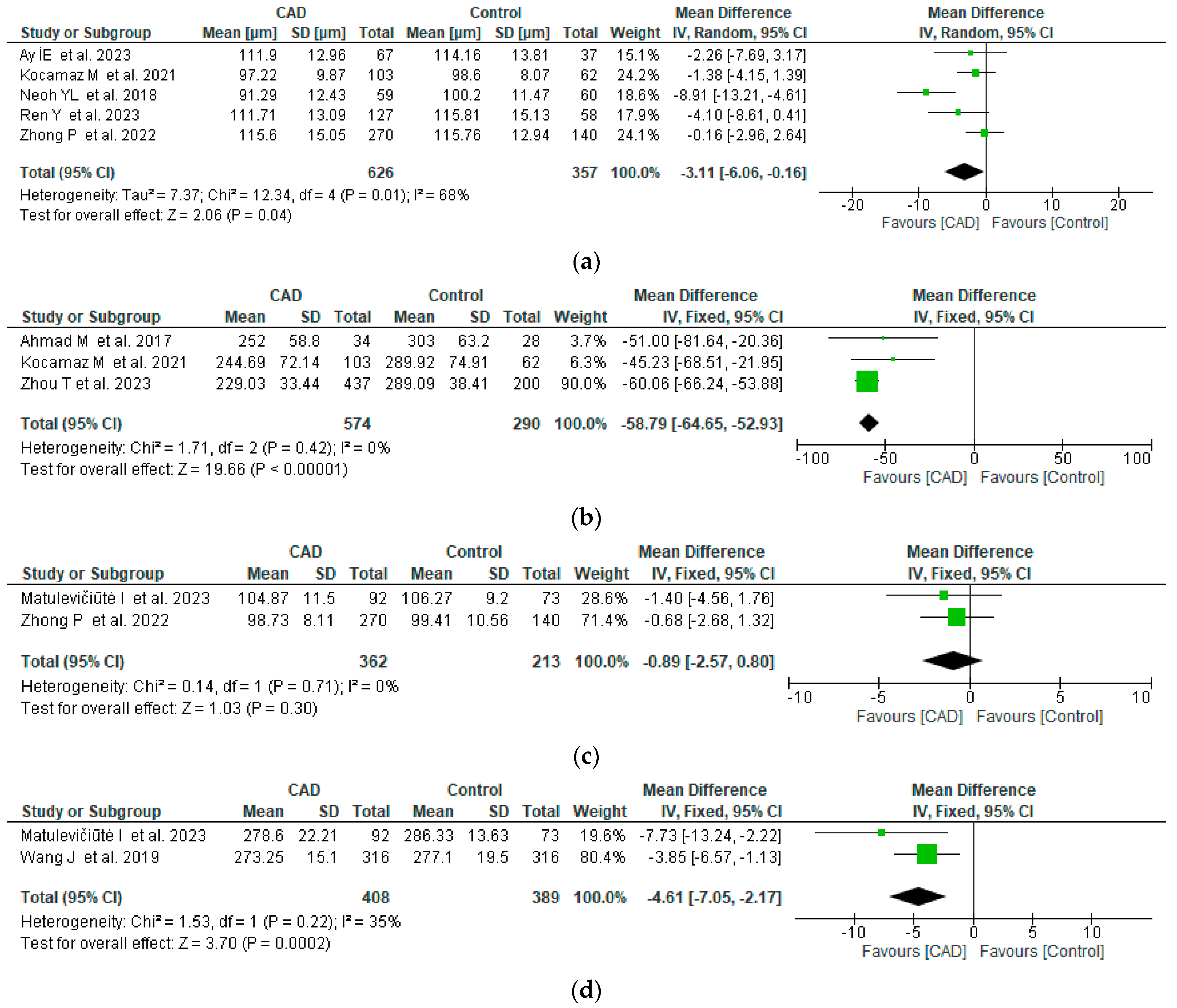
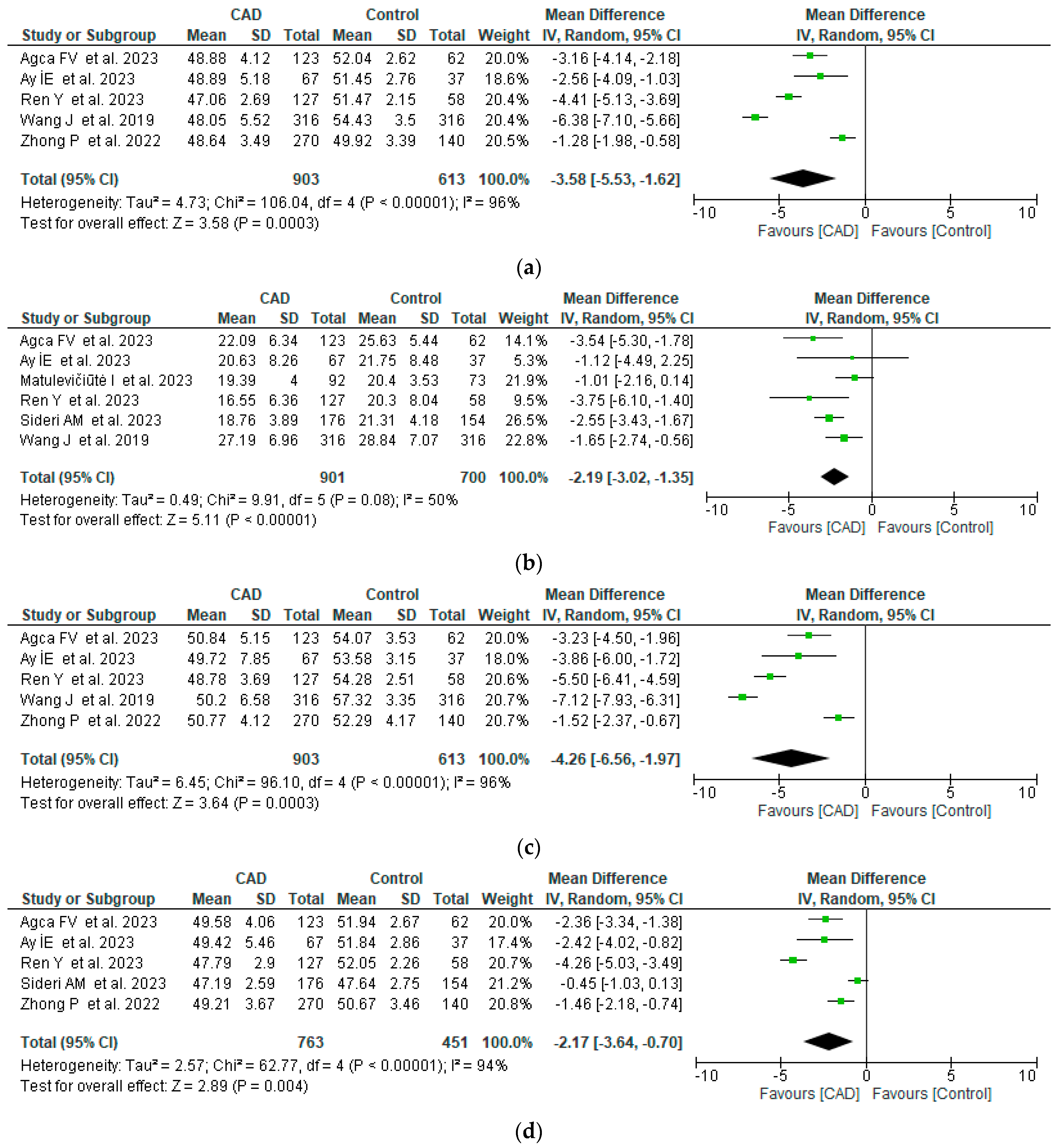
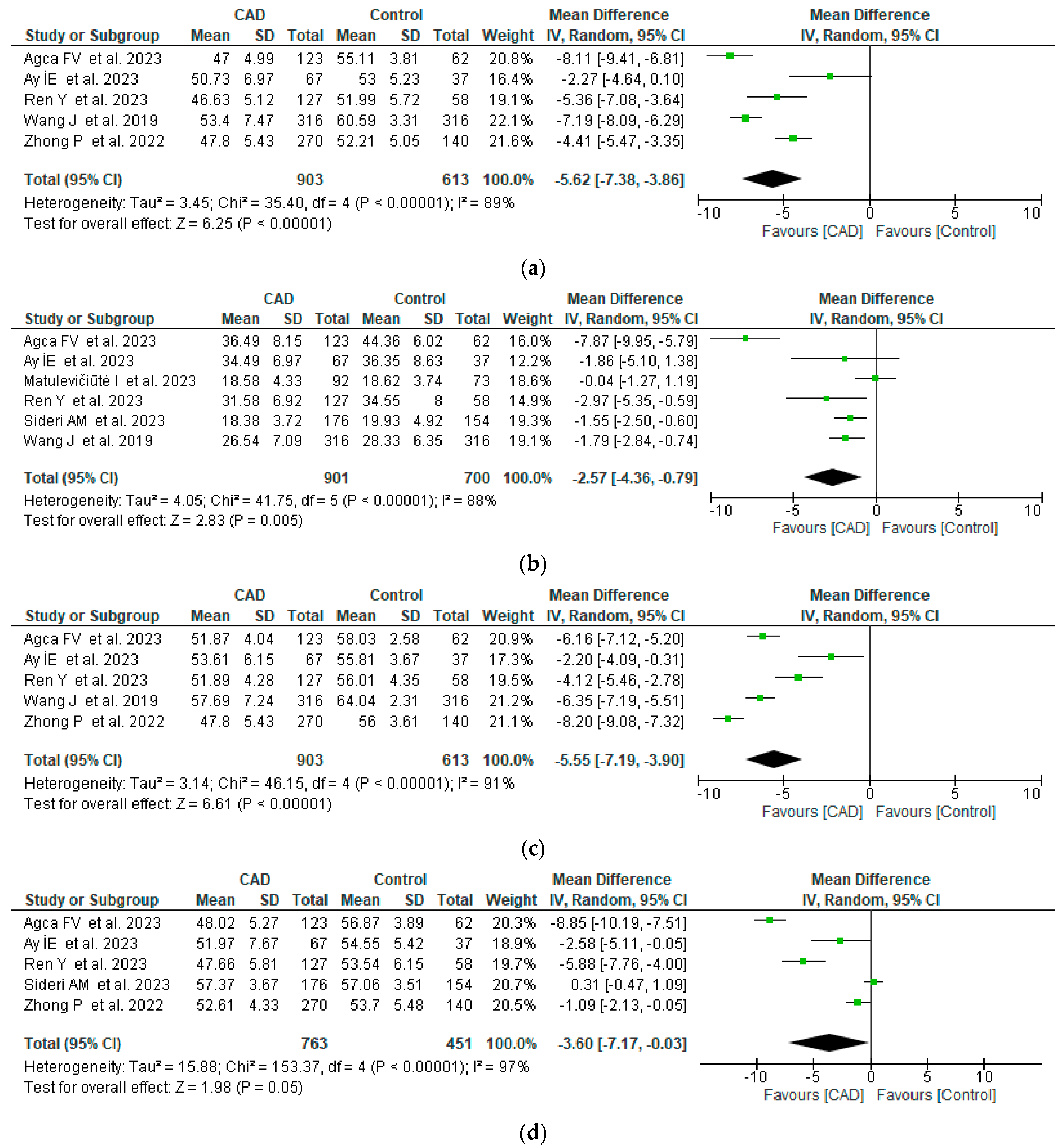
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 20 December 2023).
- Hajar, R. Risk Factors for Coronary Artery Disease: Historical Perspectives. Heart Views 2017, 18, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Spione, F.; Arevalos, V.; Gabani, R.; Sabaté, M.; Brugaletta, S. Coronary Microvascular Angina: A State-of-the-Art Review. Front. Cardiovasc. Med. 2022, 9, 800918. [Google Scholar] [CrossRef]
- Yun, C.-H.; Hung, C.-L.; Wen, M.-S.; Wan, Y.-L.; So, A. CT Assessment of Myocardial Perfusion and Fractional Flow Reserve in Coronary Artery Disease: A Review of Current Clinical Evidence and Recent Developments. Korean J. Radiol. 2021, 22, 1749–1763. [Google Scholar] [CrossRef] [PubMed]
- Gunn, R.M. Ophthalmoscopic evidence of general arterial disease. Trans. Ophthalmol. Soc. UK 1898, 18, 356–381. [Google Scholar]
- Gunn, R.M. Ophthalmoscopic Evidence of (1) Arterial Changes Associated with Chronic Renal Diseases and (2) of Increased Arterial Tension. Trans. Ophthalmol. Soc. UK 1892, 12, 124–125. [Google Scholar]
- Wong, T.Y.; Klein, R.; Klein, B.E.; Tielsch, J.M.; Hubbard, L.; Nieto, F. Retinal Microvascular Abnormalities and Their Relationship with Hypertension, Cardiovascular Disease, and Mortality. Surv. Ophthalmol. 2001, 46, 59–80. [Google Scholar] [CrossRef] [PubMed]
- Papathanasiou, K.A.; Kazantzis, D.; Vrachatis, D.A.; Giotaki, S.G.; Papaconstantinou, E.; Kanakis, M.; Avramides, D.; Deftereos, S.; Chatziralli, I.; Georgalas, I. Choroidal Thickness in Patients with Systemic Arterial Hypertension: A Systematic Review and Meta-Analysis. Ther. Adv. Ophthalmol. 2022, 14, 25158414221132825. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.; Yao, X.; Le, T.-T.; Tan, A.C.S.; Cheung, C.Y.; Chin, C.W.L.; Schmetterer, L.; Chua, J. The Application of Optical Coherence Tomography Angiography in Systemic Hypertension: A Meta-Analysis. Front. Med. 2021, 8, 778330. [Google Scholar] [CrossRef] [PubMed]
- Alnawaiseh, M.; Eckardt, F.; Mihailovic, N.; Frommeyer, G.; Diener, R.; Rosenberger, F.; Eckardt, L.; Eter, N.; Lahme, L.; Lange, P.S. Ocular Perfusion in Patients with Reduced Left Ventricular Ejection Fraction Measured by Optical Coherence Tomography Angiography. Graefe’s Arch. Clin. Exp. Ophthalmol. 2021, 259, 3605–3611. [Google Scholar] [CrossRef]
- Zhong, P.; Qin, J.; Li, Z.; Jiang, L.; Peng, Q.; Huang, M.; Lin, Y.; Liu, B.; Li, C.; Wu, Q.; et al. Development and Validation of Retinal Vasculature Nomogram in Suspected Angina Due to Coronary Artery Disease. J. Atheroscler. Thromb. 2022, 29, 579–596. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Ahmad, M.; Kaszubski, P.A.; Cobbs, L.; Reynolds, H.; Smith, R.T. Choroidal thickness in patients with coronary artery disease. PLoS ONE 2017, 12, e0175691. [Google Scholar] [CrossRef] [PubMed]
- Neoh, Y.L.; Neoh, P.F.; Salleh, A.; Bin Yusof, Z.; Gurusamy, B.; Tajudin, L.-S.A. Triple Vessel Coronary Artery Disease and Retinal Nerve Fibre Layer Thickness. Ann. Acad. Med. Singap. 2018, 47, 226–229. [Google Scholar] [CrossRef]
- Wang, J.; Jiang, J.; Zhang, Y.; Qian, Y.W.; Zhang, J.F.; Wang, Z.L. Retinal and choroidal vascular changes in coronary heart disease: An optical coherence tomography angiography study. Biomed. Opt. Express 2019, 10, 1532–1544. [Google Scholar] [CrossRef]
- Kocamaz, M.; Karadağ, O.; Onder, S.E. Comparison of choroidal thicknesses in patients with coronary artery disease and patients at risk of coronary artery disease. Int. Ophthalmol. 2021, 41, 2117–2124. [Google Scholar] [CrossRef]
- Agca, F.V.; Sensoy, B.; Aslanci, M.E.; Ulutas, H.G.; Gunes, A. Retinal microvascular changes in patients with coronary artery disease and apnea. Microvasc. Res. 2023, 148, 104514. [Google Scholar] [CrossRef]
- Ay, I.E.; Dural, I.E.; Er, A.; Doğan, M.; Gobeka, H.H.; Yilmaz, F. Is it useful to do OCTA in coronary artery disease patients to improve SYNTAX-based cardiac revascularization decision? Photodiagnosis Photodyn. Ther. 2023, 42, 103540. [Google Scholar] [CrossRef] [PubMed]
- Matulevičiūtė, I.; Tatarūnas, V.; Skipskis, V.; Čiapienė, I.; Veikutienė, A.; Lesauskaitė, V.; Dobilienė, O.; Žaliūnienė, D. Coronary artery disease, its associations with ocular, genetic and blood lipid parameters. Eye 2023, 38, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Hu, Y.; Li, C.; Zhong, P.; Liu, H.; Wang, H.; Kuang, Y.; Fu, B.; Wang, Y.; Zhao, H.; et al. Impaired retinal microcirculation in patients with non-obstructive coronary artery disease. Microvasc. Res. 2023, 148, 104533. [Google Scholar] [CrossRef]
- Sideri, A.-M.; Kanakis, M.; Katsimpris, A.; Karamaounas, A.; Brouzas, D.; Petrou, P.; Papakonstaninou, E.; Droutsas, K.; Kandarakis, S.; Giannopoulos, G.; et al. Correlation Between Coronary and Retinal Microangiopathy in Patients With STEMI. Transl. Vis. Sci. Technol. 2023, 12, 8. [Google Scholar] [CrossRef]
- Zhou, T.; Wan, T.; Jin, X.; Chen, Y.; Shen, C. The clinical implications of choroidal thickness combined with tear VEGFA in coronary artery disease. Coron. Artery Dis. 2023, 34, 510–516. [Google Scholar] [CrossRef] [PubMed]
- Furnica, C.; Chistol, R.O.; Chiran, D.A.; Stan, C.I.; Sargu, G.D.; Girlescu, N.; Tinica, G. The Impact of the Early COVID-19 Pandemic on ST-Segment Elevation Myocardial Infarction Presentation and Outcomes—A Systematic Review and Me-ta-Analysis. Diagnostics 2022, 12, 588. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [Updated March 2011]; The Cochrane Collaboration: London, UK, 2011. Available online: www.handbook.cochrane.org (accessed on 2 December 2023).
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Ucak, T.; Unver, E. Alterations in Parafoveal and Optic Disc Vessel Densities in Patients with Obstructive Sleep Apnea Syndrome. J. Ophthalmol. 2020, 2020, 4034382. [Google Scholar] [CrossRef] [PubMed]
- Machalińska, A.; Kawa, M.P.; Marlicz, W.; Machaliński, B. Complement System Activation and Endothelial Dysfunction in Patients with Age-Related Macular Degeneration (AMD): Possible Relationship between AMD and Atherosclerosis. Acta Ophthalmol. 2011, 90, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Vong, Q.P.; Liu, C.; Zheng, Y.; Brouillet, S.; Hoffmann, P.; Benharouga, M.; Salomon, A.; Schaal, J.-P.; Feige, J.-J.; et al. Borg5 Is Required for Angiogenesis by Regulating Persistent Directional Migration of the Cardiac Microvascular Endothelial Cells. Mol. Biol. Cell 2014, 25, 841–851. [Google Scholar] [CrossRef]
- Vita, J.A. Endothelial Function. Circulation 2011, 124, e906–e912. [Google Scholar] [CrossRef]
- McClintic, B.R.; McClintic, J.I.; Bisognano, J.D.; Block, R.C. The Relationship between Retinal Microvascular Abnormalities and Coronary Heart Disease: A Review. Am. J. Med. 2010, 123, 374.e1–374.e7. [Google Scholar] [CrossRef]
- McGeechan, K.; McGeechan, M.K.; Liew, M.G.; Macaskill, P.; Irwig, M.L.; Klein, R.; Klein, B.E.; Wang, M.J.J.; Mitchell, P.; Vingerling, J.R.; et al. Meta-analysis: Retinal Vessel Caliber and Risk for Coronary Heart Disease. Ann. Intern. Med. 2009, 151, 404. [Google Scholar] [CrossRef]
- Wang, S.B.; Mitchell, P.; Liew, G.; Wong, T.Y.; Phan, K.; Thiagalingam, A.; Joachim, N.; Burlutsky, G.; Gopinath, B. A Spectrum of Retinal Vasculature Measures and Coronary Artery Disease. Atherosclerosis 2018, 268, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Aschauer, J.; Aschauer, S.; Pollreisz, A.; Datlinger, F.; Gatterer, C.; Mylonas, G.; Egner, B.; Hofer, D.; Steiner, I.; Hengstenberg, C.; et al. Identification of Subclinical Microvascular Biomarkers in Coronary Heart Disease in Retinal Imaging. Transl. Vis. Sci. Technol. 2021, 10, 24. [Google Scholar] [CrossRef] [PubMed]
- Arnould, L.; Guenancia, C.; Azemar, A.; Alan, G.; Pitois, S.; Bichat, F.; Zeller, M.; Gabrielle, P.-H.; Bron, A.M.; Creuzot-Garcher, C.; et al. The EYE-MI pilot study: A prospective acute coronary syndrome cohort evaluated with retinal optical coherence tomography angiography. Investig. Opthalmology Vis. Sci. 2018, 59, 4299–4306. [Google Scholar] [CrossRef] [PubMed]
- Altinkaynak, H.; Kara, N.; Sayın, N.; Güneş, H.; Avşar, S.; Yazıcı, A.T. Subfoveal Choroidal Thickness in Patients with Chronic Heart Failure Analyzed by Spectral-Domain Optical Coherence Tomography. Curr. Eye Res. 2014, 39, 1123–1128. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.; Yusufu, M.; Wang, Y.; He, M.; Shi, D.; Wang, R. Association of retinal microvascular density and complexity with incident coronary heart disease. Atherosclerosis 2023, 380, 117196. [Google Scholar] [CrossRef] [PubMed]
- Boyraz, B.; Peker, T. Comparison of SYNTAX and Gensini Scores in the Decision of Surgery or Percutaneous Revascularization in Patients With Multivessel Coronary Artery Disease. Cureus 2022, 14, e22482. [Google Scholar] [CrossRef]
- Chakraborty, R.; Read, S.A.; Collins, M.J. Diurnal Variations in Axial Length, Choroidal Thickness, Intraocular Pressure, and Ocular Biometrics. Investig. Opthalmol. Vis. Sci. 2011, 52, 5121–5129. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criteria | Ahmad M et al. (2017) [13] | Neoh YL et al. (2018) [14] | Wang J et al. (2019) [15] | Kocamaz M et al. (2021) [16] | Zhong P et al. (2022) [11] | Agca FV et al. (2023) [17] | Ay İE et al. (2023) [18] | Matulevičiūtė et al. (2023) [19] | Ren Y et al. (2023) [20] | Sideri AM et al. (2023) [21] | Zhou T et al. (2023) [22] |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Selection | |||||||||||
| Is the case definition adequate? | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ |
| Representativeness of the cases | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ |
| Selection of controls | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ |
| Definition of controls | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ |
| Comparability | |||||||||||
| Comparability of cases and controls on the basis of the design or analysis | ★★ | ★ | ★★ | ★ | ★★ | ★★ | ★★ | ★★ | ★★ | ★★ | ★ |
| Exposure | |||||||||||
| Ascertainment of exposure | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ |
| Same method of ascertainment for cases and controls | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ |
| Non-response rate | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ |
| Total score | 8 | 7 | 8 | 7 | 8 | 8 | 8 | 8 | 8 | 8 | 7 |
| Reference | Country | OCT/OCTA Type | Study Type | Methods | Parameters | Patients | CAD Patients (Mean Age ± SD, % of Female Patients) | No CAD Patients (Mean Age ± SD, % of Female Patients) |
|---|---|---|---|---|---|---|---|---|
| Ahmad M et al. (2017) [13] | USA | - | Cross-sectional | EDI SD-OCT | Subfoveal CTh and CTh 2000 µm superiorly, inferiorly, nasally, and temporally to the fovea. | 62 (single eye) | 34 (61.1 ± 6.8, 44.1%) | 28 (60.1 ± 5.3, 60.8%) |
| Neoh YL et al. (2018) [14] | Malaysia | Cirrus | Cross-sectional | Humphrey visual field analysis, OCT | Axial length, ONH disc area, ONH rim area, RNFL thickness, vCDR. | 119 (single eye) | 59 (59.1 ± 9, 18.6%) | 60 (54.1 ± 10.9, 66.7%) |
| Wang J et al. (2019) [15] | China | Optovue | Cross-sectional | OCTA | Mean retinal thickness, SCP and DCP vessel density, flow area. | 316 (both eyes) | 158 (66.3 ± 8.4, 54.43%) | 158 (64.4 ± 9.2, 55.69%) |
| Kocamaz M et al. (2021) [16] | Turkey | Heidelberg Spectralis | Cross-sectional | EDI SD-OCT | RNFL thickness, subfoveal CTh and CTh nasally and temporally to the fovea. | 85 (both eyes) | 53 (61.36 ± 10.57, 18.9%) | 32 (57.84 ± 7.52, 18.8%) |
| Zhong P et al. (2022) [11] | China | Optovue | Cross-sectional | OCTA | RNFL thickness, RPC density, SCP and DCP vascular density, GC-IPL thickness. | 410 (single eye) | 270 (59.1 ± 9.1, 21.9%) | 140 (59.3 ± 6.9, 24.3%) |
| Agca FV et al. (2023) [17] | Turkey | Optovue | Cross-sectional | OCTA | SCP vessel density whole, DCP vessel density whole, RPC density whole, FAZ area. | 185 (single eye) | 123 (55.85 ± 7.19, 26.83%) | 62 (54.39 ± 6.45, 26%) |
| Ay İE et al. (2023) [18] | Turkey | Optovue | Cross-sectional | OCTA | SCP vascular density whole, DCP vascular density whole, FAZ area, RNFL thickness. | 104 (single eye) | 69 (61.5 ± 9, 24.64%) | 37 (60 ± 7, 32.43%) |
| Matulevičiūtė I et al. (2023) [19] | Lithuania | - | Cross-sectional | OCT, OCTA | RNFL thickness, CTh, SCP and DCP vascular density, FAZ area, GC-IPL thickness, retina thickness. | 165 (single eye) | 92 (59.96 ± 8.44, 36.96%) | 73 (59.22 ± 6.95, 45.2%) |
| Ren Y et al. (2023) [20] | China | Optovue | Cross-sectional | OCTA | RNFL, RPC density, SCP and DCP vessel density. | 185 (single eye) | 127 (61.57 ± 8.32, 41.73%) | 58 (61.91 ± 8.53, 53.4%) |
| Sideri AM et al. (2023) [21] | Greece | Topcon | Cross-sectional | OCTA | FAZ area, SCP and DCP vascular density, choriocapillaris layer thickness. | 330 (both eyes) | 88 (55.9 ± 13.7, 6%) | 77 (56.6 ± 13.05, 17%) |
| Zhou T et al. (2023) [22] | China | - | Cross-sectional | OCTA | Choroid thickness. | 637 (single eye) | 200 (53.43 ± 5.26, 31.12%) | 437 (51.41 ± 5.45, 38.5%) |
| Criteria (Studies Reporting Criteria) | CAD | No-CAD | p |
|---|---|---|---|
| Age (weighted mean ± SD) (10 studies) | 58.69 ± 9.72 | 57.73 ± 9.27 | 0.016 |
| Female patients (no., %) (10 studies) | 480 (31.83%) | 363 (39.24%) | 0.0001 |
| Arterial hypertension (no., %) (11 studies) | 874 (56.90%) | 220 (48.78%) | 0.0023 |
| Hyperlipidemia (no., %) (4 studies) | 208 (57.62%) | 69 (27.06%) | <0.001 |
| Diabetes mellitus (no., %) (8 studies) | 428 (34.91%) | 76 (20.11%) | <0.001 |
| Smoking (no., %) (4 studies) | 243 (49.89%) | 43 (35.83%) | 0.0057 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rusu, A.C.; Horvath, K.U.; Tinica, G.; Chistol, R.O.; Bulgaru-Iliescu, A.-I.; Todosia, E.T.; Brînzaniuc, K. Retinal Structural and Vascular Changes in Patients with Coronary Artery Disease: A Systematic Review and Meta-Analysis. Life 2024, 14, 448. https://doi.org/10.3390/life14040448
Rusu AC, Horvath KU, Tinica G, Chistol RO, Bulgaru-Iliescu A-I, Todosia ET, Brînzaniuc K. Retinal Structural and Vascular Changes in Patients with Coronary Artery Disease: A Systematic Review and Meta-Analysis. Life. 2024; 14(4):448. https://doi.org/10.3390/life14040448
Chicago/Turabian StyleRusu, Alexandra Cristina, Karin Ursula Horvath, Grigore Tinica, Raluca Ozana Chistol, Andra-Irina Bulgaru-Iliescu, Ecaterina Tomaziu Todosia, and Klara Brînzaniuc. 2024. "Retinal Structural and Vascular Changes in Patients with Coronary Artery Disease: A Systematic Review and Meta-Analysis" Life 14, no. 4: 448. https://doi.org/10.3390/life14040448