


An Exercise Prescription for Patients with Stroke and Sarcopenia Based on the Modified Delphi Study
 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
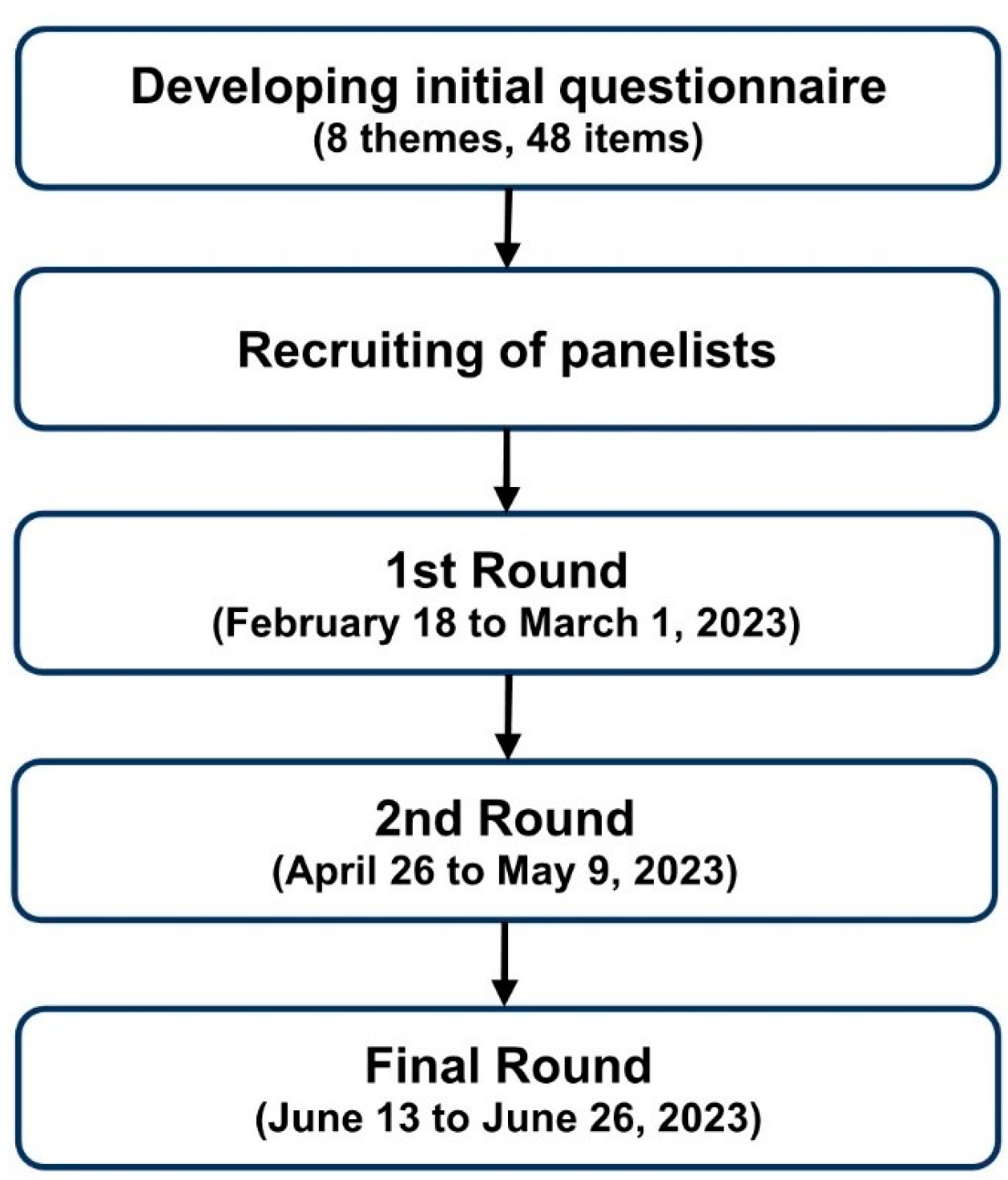
2.1. Study Design
2.2. Participants
2.3. Sample Size
2.4. Delphi Process
2.5. Round 1
2.6. Round 2
2.7. Round 3
2.8. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Consensus
3.2.1. Need for Exercise
3.2.2. Priority of Exercise
3.3. Percentage of Strong Agreement
3.4. Kendall’s Coefficient of Concordance
4. Discussion
4.1. General Theme
4.2. Dosage Theme
4.3. Type Theme
4.4. Additional Exercise Theme
4.5. Evaluation Theme
4.6. Overload Themes
4.7. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rosenberg, I.H. Sarcopenia: Origins and clinical relevance. J. Nutr. 1997, 127, 990S–991S. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 601. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e302. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Landi, F.; Schneider, S.M.; Zuniga, C.; Arai, H.; Boirie, Y.; Chen, L.K.; Fielding, R.A.; Martin, F.C.; Michel, J.P.; et al. Prevalence of and interventions for sarcopenia in ageing adults: A systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing 2014, 43, 748–759. [Google Scholar] [CrossRef] [PubMed]
- Makizako, H.; Nakai, Y.; Tomioka, K.; Taniguchi, Y. Prevalence of sarcopenia defined using the Asia Working Group for Sarcopenia criteria in Japanese community-dwelling older adults: A systematic review and meta-analysis. Phys. Ther. Res. 2019, 22, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Muscaritoli, M.; Anker, S.D.; Argiles, J.; Aversa, Z.; Bauer, J.M.; Biolo, G.; Boirie, Y.; Bosaeus, I.; Cederholm, T.; Costelli, P.; et al. Consensus definition of sarcopenia, cachexia and pre-cachexia: Joint document elaborated by Special Interest Groups (SIG) “cachexia-anorexia in chronic wasting diseases” and “nutrition in geriatrics”. Clin. Nutr. 2010, 29, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Fielding, R.A.; Vellas, B.; Evans, W.J.; Bhasin, S.; Morley, J.E.; Newman, A.B.; Abellan van Kan, G.; Andrieu, S.; Bauer, J.; Breuille, D.; et al. Sarcopenia: An undiagnosed condition in older adults. Current consensus definition: Prevalence, etiology, and consequences. International working group on sarcopenia. J. Am. Med. Dir. Assoc. 2011, 12, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Scherbakov, N.; von Haehling, S.; Anker, S.D.; Dirnagl, U.; Doehner, W. Stroke induced Sarcopenia: Muscle wasting and disability after stroke. Int. J. Cardiol. 2013, 170, 89–94. [Google Scholar] [CrossRef]
- Shefflette, A.; Patel, N.; Caruso, J. Mitigating Sarcopenia with Diet and Exercise. Int. J. Environ. Res. Public. Health 2023, 20, 6652. [Google Scholar] [CrossRef]
- Cannataro, R.; Cione, E.; Bonilla, D.A.; Cerullo, G.; Angelini, F.; D’Antona, G. Strength training in elderly: An useful tool against sarcopenia. Front. Sports Act. Living 2022, 4, 950949. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Marzetti, E.; Martone, A.M.; Bernabei, R.; Onder, G. Exercise as a remedy for sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 25–31. [Google Scholar] [CrossRef]
- Feigin, V.L.; Forouzanfar, M.H.; Krishnamurthi, R.; Mensah, G.A.; Connor, M.; Bennett, D.A.; Moran, A.E.; Sacco, R.L.; Anderson, L.; Truelsen, T.; et al. Global and regional burden of stroke during 1990-2010: Findings from the Global Burden of Disease Study 2010. Lancet 2014, 383, 245–254. [Google Scholar] [CrossRef]
- Yoshimura, Y.; Wakabayashi, H.; Bise, T.; Tanoue, M. Prevalence of sarcopenia and its association with activities of daily living and dysphagia in convalescent rehabilitation ward inpatients. Clin. Nutr. 2018, 37, 2022–2028. [Google Scholar] [CrossRef]
- Matsushita, T.; Nishioka, S.; Taguchi, S.; Yamanouchi, A. Sarcopenia as a predictor of activities of daily living capability in stroke patients undergoing rehabilitation. Geriatr. Gerontol. Int. 2019, 19, 1124–1128. [Google Scholar] [CrossRef]
- Scherbakov, N.; Sandek, A.; Doehner, W. Stroke-related sarcopenia: Specific characteristics. J. Am. Med. Dir. Assoc. 2015, 16, 272–276. [Google Scholar] [CrossRef]
- Nozoe, M.; Kanai, M.; Kubo, H.; Yamamoto, M.; Shimada, S.; Mase, K. Prestroke sarcopenia and functional outcomes in elderly patients who have had an acute stroke: A prospective cohort study. Nutrition 2019, 66, 44–47. [Google Scholar] [CrossRef]
- Nozoe, M.; Kanai, M.; Kubo, H.; Yamamoto, M.; Shimada, S.; Mase, K. Prestroke Sarcopenia and Stroke Severity in Elderly Patients with Acute Stroke. J. Stroke Cerebrovasc. Dis. 2019, 28, 2228–2231. [Google Scholar] [CrossRef]
- Li, W.; Yue, T.; Liu, Y. New understanding of the pathogenesis and treatment of stroke-related sarcopenia. Biomed. Pharmacother. 2020, 131, 110721. [Google Scholar] [CrossRef]
- Mas, M.F.; Gonzalez, J.; Frontera, W.R. Stroke and sarcopenia. Curr. Phys. Med. Rehabil. Rep. 2020, 8, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Nagano, F.; Yoshimura, Y.; Bise, T.; Shimazu, S.; Shiraishi, A. Muscle mass gain is positively associated with functional recovery in patients with sarcopenia after stroke. J. Stroke Cerebrovasc. Dis. 2020, 29, 105017. [Google Scholar] [CrossRef]
- Papadatou, M.C. Sarcopenia in Hemiplegia. J. Frailty Sarcopenia Falls 2020, 5, 38–41. [Google Scholar] [CrossRef]
- Honma, K.; Honda, Y.; Nagase, M.; Nakao, Y.; Harada, T.; Sasanuma, N.; Uchiyama, Y.; Kodama, N.; Domen, K. Impact of skeletal muscle mass on functional prognosis in acute stroke: A cohort study. J. Clin. Neurosci. 2023, 112, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo, M.; Merchant, R.A.; Morley, J.E.; Anker, S.D.; Aprahamian, I.; Arai, H.; Aubertin-Leheudre, M.; Bernabei, R.; Cadore, E.L.; Cesari, M.; et al. International Exercise Recommendations in Older Adults (ICFSR): Expert Consensus Guidelines. J. Nutr. Health Aging 2021, 25, 824–853. [Google Scholar] [CrossRef]
- Cui, H.; Wang, Z.; Wu, J.; Liu, Y.; Zheng, J.; Xiao, W.; He, P.; Zhou, Y.; Wang, J.; Yu, P.; et al. Chinese expert consensus on prevention and intervention for elderly with sarcopenia (2023). Aging Med. 2023, 6, 104–115. [Google Scholar] [CrossRef]
- Wiangkham, T.; Duda, J.; Haque, M.S.; Rushton, A. Development of an active behavioural physiotherapy intervention (ABPI) for acute whiplash-associated disorder (WAD) II management: A modified Delphi study. BMJ Open 2016, 6, e011764. [Google Scholar] [CrossRef]
- Gracia-Sanchez, A.; Lopez-Pineda, A.; Chicharro-Luna, E.; Gil-Guillen, V.F. A Delphi Study Protocol to Identify Recommendations on Physical Activity and Exercise in Patients with Diabetes and Risk of Foot Ulcerations. Int. J. Environ. Res. Public Health 2021, 18, 10988. [Google Scholar] [CrossRef] [PubMed]
- Labib, M.; Bohm, C.; MacRae, J.M.; Bennett, P.N.; Wilund, K.R.; McAdams-DeMarco, M.; Jhamb, M.; Mustata, S.; Thompson, S.; Global Renal, E.N. An International Delphi Survey on Exercise Priorities in CKD. Kidney Int. Rep. 2021, 6, 657–668. [Google Scholar] [CrossRef]
- Price, J.; Rushton, A.; Tyros, V.; Heneghan, N.R. Expert consensus on the important chronic non-specific neck pain motor control and segmental exercise and dosage variables: An international e-Delphi study. PLoS ONE 2021, 16, e0253523. [Google Scholar] [CrossRef]
- Hanssen, H.; Boardman, H.; Deiseroth, A.; Moholdt, T.; Simonenko, M.; Krankel, N.; Niebauer, J.; Tiberi, M.; Abreu, A.; Solberg, E.E.; et al. Personalized exercise prescription in the prevention and treatment of arterial hypertension: A Consensus Document from the European Association of Preventive Cardiology (EAPC) and the ESC Council on Hypertension. Eur. J. Prev. Cardiol. 2022, 29, 205–215. [Google Scholar] [CrossRef]
- McKenna, H.P. The Delphi technique: A worthwhile research approach for nursing? J. Adv. Nurs. 1994, 19, 1221–1225. [Google Scholar] [CrossRef] [PubMed]
- Hasson, F.; Keeney, S.; McKenna, H. Research guidelines for the Delphi survey technique. J. Adv. Nurs. 2000, 32, 1008–1015. [Google Scholar] [CrossRef] [PubMed]
- Diamond, I.R.; Grant, R.C.; Feldman, B.M.; Pencharz, P.B.; Ling, S.C.; Moore, A.M.; Wales, P.W. Defining consensus: A systematic review recommends methodologic criteria for reporting of Delphi studies. J. Clin. Epidemiol. 2014, 67, 401–409. [Google Scholar] [CrossRef]
- Junger, S.; Payne, S.A.; Brine, J.; Radbruch, L.; Brearley, S.G. Guidance on Conducting and REporting DElphi Studies (CREDES) in palliative care: Recommendations based on a methodological systematic review. Palliat. Med. 2017, 31, 684–706. [Google Scholar] [CrossRef] [PubMed]
- Niederberger, M.; Spranger, J. Delphi Technique in Health Sciences: A Map. Front. Public. Health 2020, 8, 457. [Google Scholar] [CrossRef] [PubMed]
- Cross, V. The Same But Different A Delphi study of clinicians’ and academics’ perceptions of physiotherapy undergraduates. Physiotherapy 1999, 85, 28–39. [Google Scholar] [CrossRef]
- Schmidt, R.C. Managing Delphi Surveys Using Nonparametric Statistical Techniques. Decis. Sci. 2007, 28, 763–774. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Stone, M.; Plisk, S.; Collins, D. Training principles: Evaluation of modes and methods of resistance training—A coaching perspective. Sports Biomech. 2002, 1, 79–103. [Google Scholar] [CrossRef]


{kind=link}
| Participants, n (%) | |
|---|---|
| Age, yrs, mean (range) | 41.3 (28–59) |
| Female sex | 8 (53.3) |
| Profession | |
| Physician—Physiatrist | 3 (20.0) |
| Physician—Neurosurgeon | 1 (6.7) |
| Physician—Neurologist | 1 (6.7) |
| Therapist—Physical | 3 (20.0) |
| Therapist—Occupational | 2 (13.3) |
| Nurse—Clinical | 4 (26.6) |
| Nurse—Research | 1 (6.7) |
| Affiliation | |
| University hospital | 10 (66.7) |
| Rehabilitation hospital | 5 (33.3) |
| Experience period | |
| <10 yrs | 2 (13.3) |
| 10–19 yrs | 8 (53.3) |
| ≥20 yrs | 5 (33.3) |
| Questionnaire about the Need for Exercise | 1st Round | 2nd Round | Final Round | |||||||
| Median | IQR | % of Agreement | Median | IQR | % of Agreement | Median | IQR | % of Agreement | ||
| 1 | Is exercise necessary to treat preexisting sarcopenia with hemiplegic stroke? | 6.00 | 1.00 | 100.00 | 6.00 | 1.00 | 100.00 | 6.00 | 1.00 | 100.00 |
| Questionnaire about Exercise Priorities | 1st Round | 2nd Round | Final Round | |||||||
| Median | IQR | % of Agreement | Median | IQR | % of Agreement | Median | IQR | % of Agreement | ||
| Theme 1—General; Does exercise need to be | ||||||||||
| 1 | Modified to each patient | 6.00 | 2.00 | 93.33 | 6.00 | 1.50 | 100.00 | 6.00 | 1.00 | 100.00 |
| 2 | Simple | 6.00 | 0.50 | 93.33 | 6.00 | 0.50 | 93.33 | 6.00 | 0.50 | 100.00 |
| 3 | Realistic | 6.00 | 1.50 | 93.33 | 6.00 | 0.50 | 93.33 | 6.00 | 0.00 | 93.33 |
| 4 | An achievable challenge | 6.00 | 3.00 | 66.67 | 6.00 | 1.00 | 80.00 | 6.00 | 0.50 | 86.67 |
| 5 | Acceptable to the patient | 7.00 | 1.00 | 100.00 | 6.00 | 1.00 | 100.00 | 6.00 | 1.00 | 100.00 |
| 6 | Appropriately time consuming | 6.00 | 1.00 | 100.00 | 6.00 | 1.00 | 100.00 | 6.00 | 1.00 | 100.00 |
| 7 | Adhered to by the patient | 7.00 | 1.00 | 100.00 | 7.00 | 1.00 | 100.00 | 7.00 | 1.00 | 100.00 |
| 8 | Decided in collaboration with the patient | 5.00 | 1.50 | 73.33 | 5.00 | 1.00 | 80.00 | 5.00 | 1.00 | 93.33 |
| 9 | Decided considering functional status and goals | 7.00 | 1.00 | 100.00 | 7.00 | 0.50 | 100.00 | 7.00 | 0.00 | 100.00 |
| 10 | Decided to affect neuromuscular performance | 6.00 | 1.50 | 93.33 | 6.00 | 1.00 | 93.33 | 6.00 | 0.50 | 100.00 |
| 11 | Decided to improve subjective symptoms | 5.00 | 1.50 | 73.33 | 5.00 | 1.00 | 80.00 | 5.00 | 1.00 | 86.67 |
| 12 | Monitored by the patient | 6.00 | 1.50 | 80.00 | 6.00 | 0.50 | 100.00 | 6.00 | 0.00 | 100.00 |
| 13 | Adapted to rehabilitation stage | 6.00 | 1.00 | 100.00 | 6.00 | 1.00 | 100.00 | 6.00 | 0.50 | 100.00 |
| 14 | Taught to the patient in advance | 6.00 | 2.00 | 100.00 | 6.00 | 1.00 | 100.00 | 6.00 | 0.50 | 100.00 |
| 15 | Decided considering equipment availability | 6.00 | 0.00 | 100.00 | 6.00 | 0.00 | 100.00 | 6.00 | 0.00 | 100.00 |
| Theme 2—Exercise dosage | ||||||||||
| 1 | Frequency | 6.00 | 1.00 | 100.00 | 6.00 | 1.00 | 100.00 | 6.00 | 1.00 | 100.00 |
| 2 | Intensity of patient’s effort | 6.00 | 0.50 | 93.33 | 6.00 | 1.00 | 100.00 | 6.00 | 0.00 | 100.00 |
| 3 | Load of objective weight | 6.00 | 1.00 | 93.33 | 6.00 | 1.00 | 100.00 | 6.00 | 1.00 | 100.00 |
| 4 | Repetitions per set | 6.00 | 1.00 | 100.00 | 6.00 | 0.50 | 100.00 | 6.00 | 0.00 | 100.00 |
| 5 | Number of Sets | 6.00 | 0.50 | 100.00 | 6.00 | 0.50 | 93.33 | 6.00 | 0.00 | 93.33 |
| 6 | Exercise duration | 6.00 | 1.00 | 100.00 | 6.00 | 1.00 | 100.00 | 6.00 | 0.50 | 100.00 |
| Theme 3—Exercise type | ||||||||||
| 1 | Exercise sequence (e.g., stretching→strengthening) | 6.00 | 1.50 | 93.33 | 6.00 | 1.50 | 100.00 | 6.00 | 1.50 | 93.33 |
| 2 | Exercise position (e.g., supine, prone, sitting) | 6.00 | 0.50 | 93.33 | 6.00 | 0.00 | 100.00 | 6.00 | 0.00 | 100.00 |
| 3 | Target muscle | 6.00 | 1.00 | 100.00 | 6.00 | 1.00 | 100.00 | 6.00 | 1.00 | 100.00 |
| 4 | Range of movement | 6.00 | 1.00 | 93.33 | 6.00 | 0.00 | 100.00 | 6.00 | 0.00 | 100.00 |
| 5 | Direction of resistance | 6.00 | 0.50 | 93.33 | 6.00 | 0.00 | 100.00 | 6.00 | 0.00 | 100.00 |
| 6 | Use of equipment | 6.00 | 1.00 | 93.33 | 6.00 | 1.00 | 93.33 | 6.00 | 1.00 | 86.67 |
| 7 | Use of weight equipment (e.g., ankle weights) | 5.00 | 1.00 | 93.33 | 5.00 | 1.00 | 86.67 | 5.00 | 0.50 | 80.00 |
| 8 | Use of elastic equipment (e.g., Thera band) | 5.00 | 1.00 | 93.33 | 5.00 | 1.00 | 86.67 | 5.00 | 0.50 | 86.67 |
| 9 | Use of balancing equipment (e.g., wall or cane) | 6.00 | 1.00 | 80.00 | 6.00 | 1.00 | 86.67 | 6.00 | 1.00 | 80.00 |
| Theme 4—Additional to extremity strengthening exercise | ||||||||||
| 1 | Aerobic exercise | 6.00 | 1.00 | 93.33 | 6.00 | 1.00 | 100.00 | 6.00 | 0.50 | 100.00 |
| 2 | Stretching exercise | 6.00 | 1.00 | 93.33 | 6.00 | 1.00 | 100.00 | 6.00 | 1.00 | 100.00 |
| 3 | Flexibility exercise (e.g., yoga) | 5.00 | 1.50 | 73.33 | 5.00 | 1.00 | 80.00 | 5.00 | 1.00 | 80.00 |
| 4 | Core muscles exercise (e.g., pilates) | 6.00 | 1.00 | 86.67 | 6.00 | 1.00 | 93.33 | 6.00 | 1.00 | 100.00 |
| Theme 5—Evaluation of exercise | ||||||||||
| 1 | Technique complexity | 6.00 | 1.50 | 73.33 | 5.00 | 1.00 | 100.00 | 5.00 | 1.00 | 93.33 |
| 2 | Patient effort | 6.00 | 0.00 | 100.00 | 6.00 | 0.00 | 100.00 | 6.00 | 0.00 | 100.00 |
| 3 | Patient compliance | 6.00 | 0.50 | 100.00 | 6.00 | 0.50 | 100.00 | 6.00 | 0.00 | 100.00 |
| 4 | Patient pain during exercise | 6.00 | 1.00 | 100.00 | 6.00 | 0.50 | 100.00 | 6.00 | 0.00 | 100.00 |
| 5 | Patient pain after exercise | 7.00 | 1.00 | 100.00 | 6.00 | 1.00 | 100.00 | 6.00 | 0.50 | 100.00 |
| 6 | Patient fatigue during exercise | 6.00 | 1.00 | 100.00 | 6.00 | 0.50 | 100.00 | 6.00 | 0.00 | 100.00 |
| 7 | Patient fatigue after exercise | 6.00 | 1.00 | 100.00 | 6.00 | 1.00 | 100.00 | 6.00 | 0.00 | 100.00 |
| Theme 6—Progressive overload | ||||||||||
| 1 | Does the patient need progressive overload exercise? | 7.00 | 1.00 | 93.33 | 7.00 | 1.00 | 100.00 | 7.00 | 1.00 | 100.00 |
| Theme 7—When to overload | ||||||||||
| 1 | When the patient no longer feels exercise is difficult | 6.00 | 0.50 | 93.33 | 6.00 | 0.50 | 100.00 | 6.00 | 0.00 | 100.00 |
| 2 | When the patient is not fatigued | 6.00 | 0.00 | 93.33 | 6.00 | 0.00 | 100.00 | 6.00 | 0.00 | 100.00 |
| 3 | When the patient feels ready | 6.00 | 1.00 | 80.00 | 6.00 | 0.50 | 93.33 | 6.00 | 0.00 | 93.33 |
| 4 | When the patient achieves functional goals | 6.00 | 1.50 | 93.33 | 6.00 | 1.00 | 100.00 | 6.00 | 0.50 | 100.00 |
| 5 | When the patient gains improvement of neuromuscular performance | 6.00 | 0.50 | 86.67 | 6.00 | 0.00 | 93.33 | 6.00 | 0.00 | 100.00 |
| 6 | When symptoms decrease | 5.00 | 1.00 | 80.00 | 5.00 | 1.00 | 86.67 | 5.00 | 1.00 | 93.33 |
| Theme 8—How to overload | ||||||||||
| 1 | Considering patient’s functional activity | 7.00 | 1.00 | 100.00 | 7.00 | 0.50 | 100.00 | 7.00 | 0.00 | 100.00 |
| 2 | Frequency | 6.00 | 1.00 | 93.33 | 6.00 | 0.50 | 100.00 | 6.00 | 0.50 | 100.00 |
| 3 | Intensity of patient’s effort | 6.00 | 1.50 | 93.33 | 6.00 | 1.00 | 100.00 | 6.00 | 1.00 | 100.00 |
| 4 | Load of objective weight | 6.00 | 1.00 | 93.33 | 6.00 | 0.00 | 100.00 | 6.00 | 0.00 | 100.00 |
| 5 | Repetitions per set | 6.00 | 1.00 | 93.33 | 6.00 | 0.50 | 93.33 | 6.00 | 0.00 | 93.33 |
| 6 | Number of sets | 6.00 | 0.50 | 93.33 | 6.00 | 1.00 | 86.67 | 6.00 | 0.50 | 93.33 |
| 7 | Change of exercise position | 6.00 | 1.00 | 93.33 | 6.00 | 1.00 | 100.00 | 6.00 | 0.50 | 100.00 |
| 8 | Change of range of movement | 6.00 | 1.00 | 100.00 | 6.00 | 0.50 | 100.00 | 6.00 | 0.00 | 100.00 |
| 9 | Addition of exercise equipment | 5.00 | 1.00 | 86.67 | 5.00 | 1.00 | 100.00 | 5.00 | 1.00 | 100.00 |
| 1st Round | 2nd Round | Final Round | ||||
|---|---|---|---|---|---|---|
| % of Agreement | % of Strong Agreement | % of Agreement | % of Strong Agreement | % of Agreement | % of Strong Agreement | |
| Theme 1 | ||||||
| 1 | 93.33 | 66.67 | 100.00 | 73.33 | 100.00 | 80.00 |
| 2 | 93.33 | 73.33 | 93.33 | 73.33 | 100.00 | 73.33 |
| 3 | 93.33 | 66.67 | 93.33 | 73.33 | 93.33 | 80.00 |
| 4 | 66.67 | 66.67 | 80.00 | 66.67 | 86.67 | 73.33 |
| 5 | 100.00 | 93.33 | 100.00 | 93.33 | 100.00 | 86.67 |
| 6 | 100.00 | 93.33 | 100.00 | 93.33 | 100.00 | 93.33 |
| 7 | 100.00 | 80.00 | 100.00 | 86.67 | 100.00 | 93.33 |
| 8 | 73.33 | 33.33 | 80.00 | 46.67 | 93.33 | 46.67 |
| 9 | 100.00 | 86.67 | 100.00 | 100.00 | 100.00 | 100.00 |
| 10 | 93.33 | 73.33 | 93.33 | 73.33 | 100.00 | 80.00 |
| 11 | 73.33 | 46.67 | 80.00 | 40.00 | 86.67 | 46.67 |
| 12 | 80.00 | 66.67 | 100.00 | 73.33 | 100.00 | 86.67 |
| 13 | 100.00 | 93.33 | 100.00 | 93.33 | 100.00 | 93.33 |
| 14 | 100.00 | 66.67 | 100.00 | 86.67 | 100.00 | 93.33 |
| 15 | 100.00 | 80.00 | 100.00 | 86.67 | 100.00 | 93.33 |
| Theme 2 | ||||||
| 1 | 100.00 | 93.33 | 100.00 | 100.00 | 100.00 | 100.00 |
| 2 | 93.33 | 80.00 | 100.00 | 73.33 | 100.00 | 80.00 |
| 3 | 93.33 | 66.67 | 100.00 | 66.67 | 100.00 | 66.67 |
| 4 | 100.00 | 80.00 | 100.00 | 86.67 | 100.00 | 86.67 |
| 5 | 100.00 | 73.33 | 93.33 | 73.33 | 93.33 | 80.00 |
| 6 | 100.00 | 73.33 | 100.00 | 73.33 | 100.00 | 73.33 |
| Theme 3 | ||||||
| 1 | 93.33 | 66.67 | 100.00 | 66.67 | 93.33 | 60.00 |
| 2 | 93.33 | 80.00 | 100.00 | 86.67 | 100.00 | 93.33 |
| 3 | 100.00 | 86.67 | 100.00 | 93.33 | 100.00 | 86.67 |
| 4 | 93.33 | 93.33 | 100.00 | 93.33 | 100.00 | 93.33 |
| 5 | 93.33 | 86.67 | 100.00 | 86.67 | 100.00 | 86.67 |
| 6 | 93.33 | 53.33 | 93.33 | 60.00 | 86.67 | 60.00 |
| 7 | 93.33 | 33.33 | 86.67 | 40.00 | 80.00 | 26.67 |
| 8 | 93.33 | 40.00 | 86.67 | 40.00 | 86.67 | 26.67 |
| 9 | 80.00 | 60.00 | 86.67 | 66.67 | 80.00 | 60.00 |
| Theme 4 | ||||||
| 1 | 93.33 | 60.00 | 100.00 | 66.67 | 100.00 | 73.33 |
| 2 | 93.33 | 80.00 | 100.00 | 93.33 | 100.00 | 86.67 |
| 3 | 73.33 | 40.00 | 80.00 | 40.00 | 80.00 | 33.33 |
| 4 | 86.67 | 60.00 | 93.33 | 66.67 | 100.00 | 66.67 |
| Theme 5 | ||||||
| 1 | 73.33 | 53.33 | 100.00 | 40.00 | 93.33 | 40.00 |
| 2 | 100.00 | 86.67 | 100.00 | 93.33 | 100.00 | 93.33 |
| 3 | 100.00 | 93.33 | 100.00 | 93.33 | 100.00 | 93.33 |
| 4 | 100.00 | 86.67 | 100.00 | 100.00 | 100.00 | 93.33 |
| 5 | 100.00 | 80.00 | 100.00 | 93.33 | 100.00 | 86.67 |
| 6 | 100.00 | 93.33 | 100.00 | 93.33 | 100.00 | 86.67 |
| 7 | 100.00 | 93.33 | 100.00 | 93.33 | 100.00 | 86.67 |
| Theme 6 | ||||||
| 1 | 93.33 | 93.33 | 100.00 | 100.00 | 100.00 | 93.33 |
| Theme 7 | ||||||
| 1 | 93.33 | 80.00 | 100.00 | 86.67 | 100.00 | 93.33 |
| 2 | 93.33 | 80.00 | 100.00 | 86.67 | 100.00 | 86.67 |
| 3 | 80.00 | 53.33 | 93.33 | 73.33 | 93.33 | 86.67 |
| 4 | 93.33 | 73.33 | 100.00 | 86.67 | 100.00 | 86.67 |
| 5 | 86.67 | 80.00 | 93.33 | 86.67 | 100.00 | 93.33 |
| 6 | 80.00 | 40.00 | 86.67 | 33.33 | 93.33 | 33.33 |
| Theme 8 | ||||||
| 1 | 100.00 | 80.00 | 100.00 | 100.00 | 100.00 | 100.00 |
| 2 | 93.33 | 53.33 | 100.00 | 73.33 | 100.00 | 80.00 |
| 3 | 93.33 | 66.67 | 100.00 | 80.00 | 100.00 | 80.00 |
| 4 | 93.33 | 66.67 | 100.00 | 80.00 | 100.00 | 80.00 |
| 5 | 93.33 | 80.00 | 93.33 | 86.67 | 93.33 | 93.33 |
| 6 | 93.33 | 73.33 | 86.67 | 66.67 | 93.33 | 73.33 |
| 7 | 93.33 | 60.00 | 100.00 | 66.67 | 100.00 | 73.33 |
| 8 | 100.00 | 60.00 | 100.00 | 73.33 | 100.00 | 86.67 |
| 9 | 86.67 | 40.00 | 100.00 | 40.00 | 100.00 | 33.33 |
| Final Round | |||||
|---|---|---|---|---|---|
| N | Kendall W | χ2 | df | p | |
| All items in all themes | 15 | 0.319 | 268.094 | 56 | <0.00 1* |
| Theme 1—General | 15 | 0.303 | 63.679 | 14 | <0.001 * |
| Theme 2—Exercise dosage | 15 | 0.228 | 17.073 | 5 | 0.004 * |
| Theme 3—Exercise type | 15 | 0.379 | 45.456 | 8 | <0.001 * |
| Theme 4—Additional exercise | 15 | 0.378 | 17.012 | 3 | 0.001 * |
| Theme 5—Evaluation of exercise | 15 | 0.394 | 35.486 | 6 | <0.001 * |
| Theme 6—Progressive overload | 15 | NA | NA | NA | NA |
| Theme 7—When to overload | 15 | 0.311 | 23.296 | 5 | <0.001 * |
| Theme 8—How to overload | 15 | 0.391 | 46.860 | 8 | <0.001 * |
| Category | Priority |
|---|---|
| General | Modification/Simplicity/Reality/Achievable challenge/Acceptability/Proper time/Adherence/Collaboration with the patient/Functional status and goals of the patients/Effect on neuromuscular performance of the patient/Improvement of patient symptoms/Patient monitoring/Adaptation of rehabilitation stage/Education about exercise for the patient/Equipment availability |
| Dosage | Frequency/Intensity/Load/Repetitions per set/Number of sets/Exercise duration |
| Type | Sequence/Position/Target muscle/Range of movement/Direction of resistance/Use of equipment/Use of weight equipment/Use of elastic equipment/Use of balancing equipment |
| Additional exercise | Aerobic/Stretching/Flexibility/Core muscle exercise |
| Evaluation | Complexity/Effort/Compliance/Pain during exercise/after exercise/Fatigue during exercise/after exercise |
| Progressive overload | Need |
| When to overload | When the patient feels exercise is not difficult/When the patient is not fatigued/when the patient feels ready/When the patient achieves goals/When the patient gains improved neuromuscular performance/When the patient’s symptoms decrease |
| How to overload | Consideration of patient’s function/Frequency/Intensity/Load/Repetitions per set/Number of sets/Change position/Change range of movement/Additional equipment |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, J.W.; Park, G.-Y.; Park, H.-Y.; Yoo, Y.J.; Yoon, M.-J.; Song, S.; Park, K.H.; Lee, H.; Choi, S.; Im, S.; et al. An Exercise Prescription for Patients with Stroke and Sarcopenia Based on the Modified Delphi Study. Life 2024, 14, 332. https://doi.org/10.3390/life14030332
Yoo JW, Park G-Y, Park H-Y, Yoo YJ, Yoon M-J, Song S, Park KH, Lee H, Choi S, Im S, et al. An Exercise Prescription for Patients with Stroke and Sarcopenia Based on the Modified Delphi Study. Life. 2024; 14(3):332. https://doi.org/10.3390/life14030332
Chicago/Turabian StyleYoo, Jae Wan, Geun-Young Park, Hae-Yeon Park, Yeun Jie Yoo, Mi-Jeong Yoon, SeungYup Song, Kyung Hyun Park, Hooman Lee, Sangui Choi, Sun Im, and et al. 2024. "An Exercise Prescription for Patients with Stroke and Sarcopenia Based on the Modified Delphi Study" Life 14, no. 3: 332. https://doi.org/10.3390/life14030332