
Association between Obstructive Sleep Apnea and Chronic Kidney Disease According to Sex, Long Working Hours: The Korean National Health and Nutrition Examination Survey (2019–2020)

Abstract
:1. Introduction
2. Materials and Methods
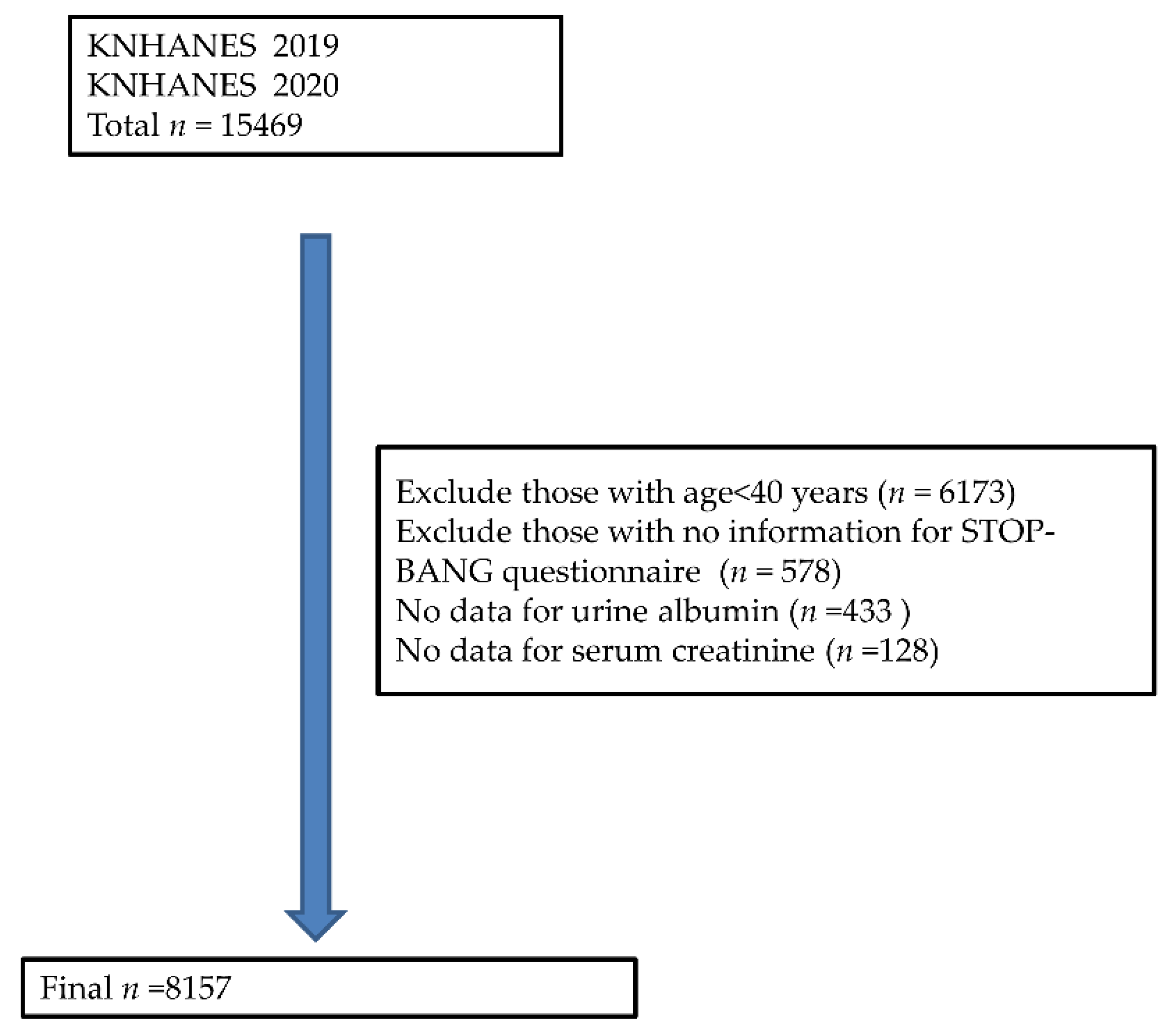
2.1. Study Design
2.2. STOP-BANG Score
2.3. Assessment of Estimated Glomerular Filtration Rate (eGFR), Albuminuria, and Chronic Kidney Disease
2.4. Working Hours
2.5. Covariates
2.6. Statistical Analyses
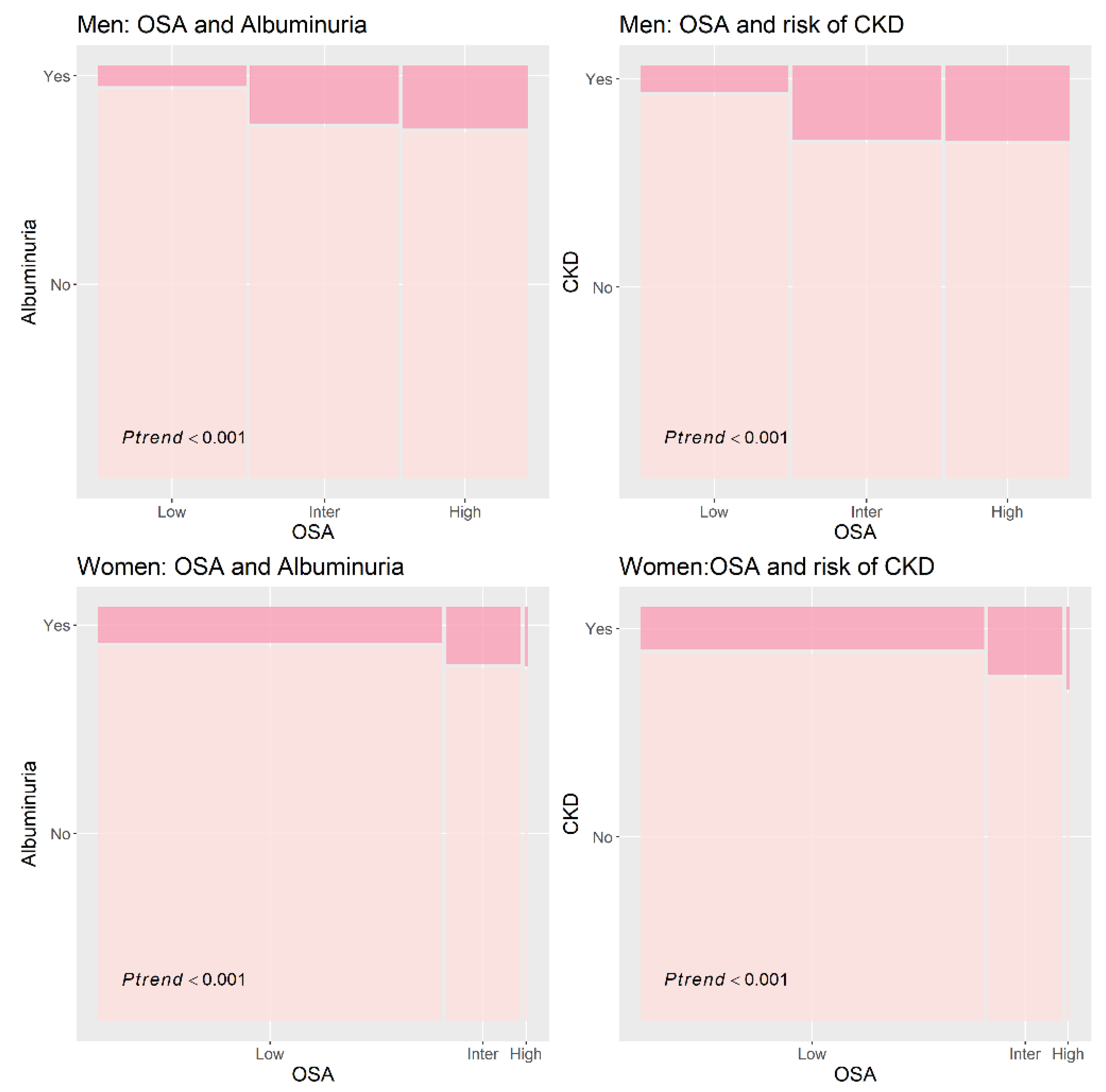
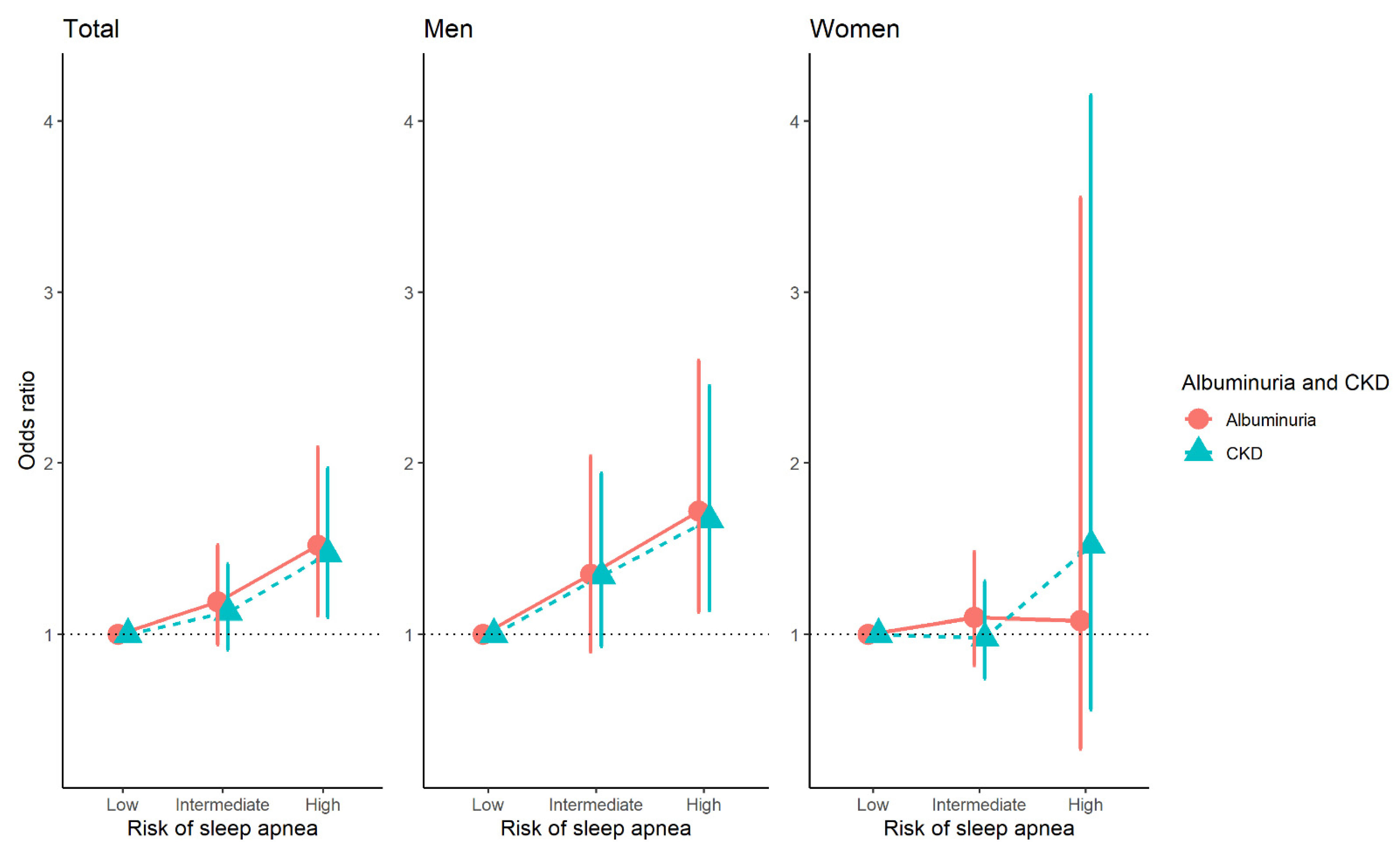
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Obstructive Sleep Apnea. Available online: https://www.ncbi.nlm.nih.gov/books/NBK459252/ (accessed on 19 January 2023).
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; Heinzer, R.; Ip, M.S.M.; Morrell, M.J.; Nunez, C.M.; Patel, S.R.; Penzel, T.; Pépin, J.L.; et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. Lancet Respir. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peppard, P.E.; Young, T.; Barnet, J.H.; Palta, M.; Hagen, E.W.; Hla, K.M. Increased prevalence of sleep-disordered breathing in adults. Am. J. Epidemiol. 2013, 177, 1006–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santilli, M.; Manciocchi, E.; D’Addazio, G.; Di Maria, E.; D’Attilio, M.; Femminella, B.; Sinjari, B. Prevalence of Obstructive Sleep Apnea Syndrome: A Single-Center Retrospective Study. Int. J. Environ. Res. Public Health 2021, 18, 10277. [Google Scholar] [CrossRef] [PubMed]
- Su, X.; Li, J.H.; Gao, Y.; Chen, K.; Gao, Y.; Guo, J.J.; Shi, M.; Zou, X.; Xu, W.; Zhao, L.B.; et al. Impact of obstructive sleep apnea complicated with type 2 diabetes on long-term cardiovascular risks and all-cause mortality in elderly patients. BMC Geriatr. 2021, 21, 508. [Google Scholar] [CrossRef]
- Hwang, M.; Zhang, K.; Nagappa, M.; Saripella, A.; Englesakis, M.; Chung, F. Validation of the STOP-Bang questionnaire as a screening tool for obstructive sleep apnoea in patients with cardiovascular risk factors: A systematic review and meta-analysis. BMJ Open Respir. Res. 2021, 8, e000848. [Google Scholar] [CrossRef]
- Chung, F.; Yegneswaran, B.; Liao, P.; Chung, S.A.; Vairavanathan, S.; Islam, S.; Khajehdehi, A.; Shapiro, C.M. STOP questionnaire: A tool to screen patients for obstructive sleep apnea. Anesthesiology 2008, 108, 812–821. [Google Scholar] [CrossRef] [Green Version]
- GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.H.; Perger, E.; Lyons, O.D. Obstructive sleep apnea and chronic kidney disease. Curr. Opin. Pulm. Med. 2018, 24, 549–554. [Google Scholar] [CrossRef]
- Hwu, D.-W.; Lin, K.-D.; Lin, K.-C.; Lee, Y.-J.; Chang, Y.-H. The association of obstructive sleep apnea and renal outcomes—A systematic review and meta-analysis. BMC Nephrol. 2017, 18, 313. [Google Scholar] [CrossRef] [Green Version]
- Umbro, I.; Fabiani, V.; Fabiani, M.; Angelico, F.; Del Ben, M. A systematic review on the association between obstructive sleep apnea and chronic kidney disease. Sleep Med. Rev. 2020, 53, 101337. [Google Scholar] [CrossRef]
- Fu, Y.; Lin, J.; Chen, L.; Chen, X.; Chen, Q. Meta-analysis of the effects of CPAP therapy on estimated glomerular filtration rate in patients with obstructive sleep apnea. Sleep Breath. 2023. [Google Scholar] [CrossRef]
- O’Connor, C.; Thornley, K.S.; Hanly, P.J. Gender differences in the polysomnographic features of obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 2000, 161, 1465–1472. [Google Scholar] [CrossRef]
- Ricardo, A.C.; Yang, W.; Sha, D.; Appel, L.J.; Chen, J.; Krousel-Wood, M.; Manoharan, A.; Steigerwalt, S.; Wright, J.; Rahman, M.; et al. Sex-Related Disparities in CKD Progression. J. Am. Soc. Nephrol. 2019, 30, 137–146. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.; Seo, E.; Mun, E.; Lee, W. A longitudinal study of working hours and chronic kidney disease in healthy workers: The Kangbuk Samsung Health Study. J. Occup. Health 2021, 63, e12266. [Google Scholar] [CrossRef]
- Kim, K.D.; Jang, S.Y. Association Between Long Working Hours and Chronic Kidney Disease According to Diabetic Status: A Nationwide Study (Korean National Health and Nutrition Examination Survey 2010–2017). J. Occup. Environ. Med. 2022, 64, 190–196. [Google Scholar] [CrossRef]
- Oh, K.; Kim, Y.; Kweon, S.; Kim, S.; Yun, S.; Park, S.; Lee, Y.K.; Kim, Y.; Park, O.; Jeong, E.K. Korea National Health and Nutrition Examination Survey, 20th anniversary: Accomplishments and future directions. Epidemiol. Health 2021, 43, e2021025. [Google Scholar] [CrossRef]
- STOP-Bang Questionnaire. Available online: http://www.stopbang.ca/patient/screening.php (accessed on 11 November 2022).
- Inker, L.A.; Eneanya, N.D.; Coresh, J.; Tighiouart, H.; Wang, D.; Sang, Y.; Crews, D.C.; Doria, A.; Estrella, M.M.; Froissart, M.; et al. New Creatinine- and Cystatin C-Based Equations to Estimate GFR without Race. N. Engl. J. Med. 2021, 385, 1737–1749. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes Diabetes Work Group. KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int. 2022, 102, S1–S127. [Google Scholar] [CrossRef]
- Messenger, J. Working Time and the Future of Work; International Labour Organization: Geneva, Switzerland, 2018; Volume 6, p. 44. [Google Scholar]
- Flack, J.M.; Adekola, B. Blood pressure and the new ACC/AHA hypertension guidelines. Trends Cardiovasc. Med. 2020, 30, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Strange, C.; Richard, C.L.; Shan, S.; Phillips, B.A.; Kanotra, S.; Drummond, M.B.; Megenhardt, L.; Lal, C.; Pleasants, R.A. A population-based estimate of the health care burden of obstructive sleep apnea using a STOP-BAG questionnaire in South Carolina. J. Clin. Sleep Med. 2021, 17, 367–374. [Google Scholar] [CrossRef]
- Lee, M.R.; Jung, S.M. Obstructive sleep apnea related to mental health, health-related quality of life and multimorbidity: A nationwide survey of a representative sample in Republic of Korea. PLoS ONE 2023, 18, e0287182. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Anton, A.; D’Ambrosio, C.M. Sex Differences in Obstructive Sleep Apnea. Clin. Chest Med. 2021, 42, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Fietze, I.; Laharnar, N.; Obst, A.; Ewert, R.; Felix, S.B.; Garcia, C.; Gläser, S.; Glos, M.; Schmidt, C.O.; Stubbe, B.; et al. Prevalence and association analysis of obstructive sleep apnea with gender and age differences—Results of SHIP-Trend. J. Sleep Res. 2019, 28, e12770. [Google Scholar] [CrossRef]
- Dewan, N.A.; Nieto, F.J.; Somers, V.K. Intermittent hypoxemia and OSA: Implications for comorbidities. Chest 2015, 147, 266–274. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.H.; Lurie, R.C.; Lyons, O.D. Sleep Apnea and Chronic Kidney Disease: A State-of-the-Art Review. Chest 2020, 157, 673–685. [Google Scholar] [CrossRef]
- Abuyassin, B.; Badran, M.; Ayas, N.T.; Laher, I. Intermittent hypoxia causes histological kidney damage and increases growth factor expression in a mouse model of obstructive sleep apnea. PLoS ONE 2018, 13, e0192084. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.; Heizhati, M.; Li, N.; Lin, M.; Gan, L.; Zhu, Q.; Cai, L.; Yuan, Y.; Yao, L.; Li, M.; et al. The relationship between obstructive sleep apnea and risk of renal impairment in patients with hypertension, a longitudinal study. Sleep Med. 2023, 109, 18–24. [Google Scholar] [CrossRef]
- Kim, T.; Kang, J. Relationship between obstructive sleep apnea, insulin resistance, and metabolic syndrome: A nationwide population-based survey. Endocr. J. 2023, 70, 107–119. [Google Scholar] [CrossRef]
- Lin, C.M.; Davidson, T.M.; Ancoli-Israel, S. Gender differences in obstructive sleep apnea and treatment implications. Sleep Med. Rev. 2008, 12, 481–496. [Google Scholar] [CrossRef] [Green Version]
- Votteler, S.; Knaack, L.; Janicki, J.; Fink, G.R.; Burghaus, L. Sex differences in polysomnographic findings in patients with obstructive sleep apnea. Sleep Med. 2023, 101, 429–436. [Google Scholar] [CrossRef]
- Bublitz, M.; Adra, N.; Hijazi, L.; Shaib, F.; Attarian, H.; Bourjeily, G. A Narrative Review of Sex and Gender Differences in Sleep Disordered Breathing: Gaps and Opportunities. Life 2022, 12, 2003. [Google Scholar] [CrossRef]
- Dosman, J.A.; Karunanayake, C.P.; Fenton, M.; Ramsden, V.R.; Seeseequasis, J.; Mike, D.; Seesequasis, W.; Neubuhr, M.; Skomro, R.; Kirychuk, S.; et al. STOP-Bang Score and Prediction of Severity of Obstructive Sleep Apnea in a First Nation Community in Saskatchewan, Canada. Clocks Sleep 2022, 4, 535–548. [Google Scholar] [CrossRef]
- Jung, F.U.; Bodendieck, E.; Bleckwenn, M.; Hussenoeder, F.S.; Luppa, M.; Riedel-Heller, S.G. Burnout, work engagement and work hours—How physicians’ decision to work less is associated with work-related factors. BMC Health Serv. Res. 2023, 23, 157. [Google Scholar] [CrossRef] [PubMed]
- Rapa, S.F.; Di Iorio, B.R.; Campiglia, P.; Heidland, A.; Marzocco, S. Inflammation and Oxidative Stress in Chronic Kidney Disease-Potential Therapeutic Role of Minerals, Vitamins and Plant-Derived Metabolites. Int. J. Mol. Sci. 2019, 21, 263. [Google Scholar] [CrossRef] [Green Version]
- Min, J.; Lee, D.W.; Kang, M.Y.; Myong, J.P.; Kim, H.R.; Lee, J. Working for Long Hours Is Associated with Dietary Fiber Insufficiency. Front. Nutr. 2022, 9, 786569. [Google Scholar] [CrossRef]
- Du, Y.; Duan, X.; Zheng, M.; Zhao, W.; Huang, J.; Lao, L.; Weng, F.; Lin, D.E.; Yang, Z.; Li, H.; et al. Association Between Eating Habits and Risk of Obstructive Sleep Apnea: A Population-Based Study. Nat. Sci. Sleep 2021, 13, 1783–1795. [Google Scholar] [CrossRef]
- Asghari, G.; Momenan, M.; Yuzbashian, E.; Mirmiran, P.; Azizi, F. Dietary pattern and incidence of chronic kidney disease among adults: A population-based study. Nutr. Metab. 2018, 15, 88. [Google Scholar] [CrossRef]
- Hui, L.; Benca, R. The Bidirectional Relationship Between Obstructive Sleep Apnea and Chronic Kidney Disease. J. Stroke Cerebrovasc. Dis. 2021, 30, 105652. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Men (n = 3575) | Women (n = 4582) | Total (n = 8157) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Low | Intermediate | High | p Value | Low | Intermediate | High | p Value | Low | Intermediate | High | p Value | |
| n | 1254 | 1260 | 1061 | 3740 | 807 | 35 | 4994 | 2067 | 1096 | |||
| Age, y | 56.0 ± 12.1 | 64.6 ± 10.0 | 59.1 ± 11.1 | <0.001 | 58.9 ± 11.9 | 65.5 ± 9.0 | 63.6 ± 9.6 | <0.001 | 58.2 ± 12.0 | 65.0 ± 9.6 | 59.2 ± 11.1 | <0.001 |
| Education | ||||||||||||
| Low | 198 (12.2) | 401 (28.9) | 266 (18.2) | <0.001 | 1229 (29.4) | 483 (55.1) | 20 (46.2) | <0.001 | 1427 (24.2) | 884 (38.5) | 286 (19.0) | <0.001 |
| Medium | 372 (35.4) | 392 (36.1) | 345 (33.2) | 1120 (35.8) | 215 (29.5) | 10 (36.4) | 1492 (35.7) | 607 (33.7) | 355 (33.3) | |||
| High | 569 (52.5) | 344 (35.0) | 447 (48.6) | 1089 (34.8) | 107 (15.4) | 5 (17.4) | 1658 (40.2) | 451 (27.8) | 452 (47.7) | |||
| Not response | 115 | 123 | 3 | 302 | 2 | 0 | 417 | 125 | 3 | |||
| Smoking | ||||||||||||
| non smoker | 251 (20.5) | 254 (19.6) | 173 (16.5) | 0.001 | 3368 (91.0) | 725 (90.1) | 33 (94.4) | 0.562 | 3619 (69.3) | 979 (44.1) | 206 (18.7) | <0.001 |
| Former smoker | 574 (44.6) | 674 (52.6) | 555 (50.3) | 200 (5.2) | 40 (5.0) | 2 (5.6) | 774 (17.3) | 714 (36.1) | 557 (49.1) | |||
| Current smoker | 418 (34.9) | 314 (27.8) | 331 (33.2) | 135 (3.8) | 39 (4.9) | 0 (0) | 553 (13.3) | 353 (19.9) | 331 (32.3) | |||
| Not response | 11 | 18 | 2 | 37 | 3 | 0 | 48 | 21 | 2 | |||
| Alcohol consumption | ||||||||||||
| Non-drinker | 436 (33.1) | 421 (31.3) | 311 (28.3) | 0.098 | 2449 (63.9) | 577 (70.7) | 26 (75.5) | 0.004 | 2885 (54.4) | 998 (45.0) | 337 (29.6) | <0.001 |
| Alcohol drinker | 808 (66.9) | 824 (68.7) | 748 (71.7) | 1259 (36.1) | 228 (29.3) | 9 (24.5) | 2067 (45.6) | 1052 (55.0) | 757 (70.4) | |||
| Not response | 10 | 15 | 2 | 32 | 2 | 0 | 42 | 17 | 2 | |||
| Physical activity | ||||||||||||
| No | 660 (56.5) | 652 (56.3) | 608 (59.3) | 0.378 | 2116 (61.2) | 549 (67.4) | 22 (68.6) | 0.027 | 2776 (59.7) | 1201 (60.3) | 630 (59.6) | 0.920 |
| Yes | 480 (43.5) | 484 (43.7) | 448 (40.7) | 1319 (38.8) | 255 (32.6) | 13 (31.4) | 1799 (40.3) | 739 (39.7) | 461 (40.4) | |||
| Not response | 114 | 124 | 5 | 305 | 3 | 0 | 419 | 127 | 5 | |||
| BMI | ||||||||||||
| <25 | 901 (70.3) | 677 (50.2) | 481 (43.8) | <0.001 | 2615 (71.0) | 409 (50.3) | 10 (21.5) | <0.001 | 3516 (70.8) | 1086 (50.3) | 491 (43.2) | <0.001 |
| ≥25 | 353 (29.7) | 583 (49.8) | 580 (56.2) | 1125 (29.0) | 398 (49.7) | 25 (78.5) | 1478 (29.2) | 981 (49.7) | 605 (56.8) | |||
| HOMA-IR | 2.1 ± 2.0 | 2.7 ± 3.2 | 3.0 ± 3.4 | <0.001 | 2.2 ± 2.1 | 3.1 ± 4.0 | 3.9 ± 2.9 | <0.001 | 2.2 ± 2.1 | 2.9 ± 3.5 | 3.1 ± 3.4 | <0.001 |
| Hypercholesterolemia | 232 (19.3) | 384 (32.2) | 352 (35.0) | <0.001 | 1183 (30.4) | 412 (51.4) | 16 (52.3) | <0.001 | 1415 (27.0) | 796 (38.8) | 368 (35.4) | <0.001 |
| Not response | 107 | 3 | 1 | 144 | 62 | 34 | ||||||
| High blood pressure | 543 (44.8) | 998 (78.3) | 893 (82.7) | <0.001 | 1834 (45.8) | 711 (87.5) | 35 (100) | <0.001 | 2377 (45.5) | 1709 (81.5) | 928 (83.2) | <0.001 |
| Albuminuria (uACR) | ||||||||||||
| <30 | 1191 (94.8) | 1082 (87.0) | 898 (86.2) | <0.001 | 3417 (92.0) | 695 (85.0) | 30 (83.7) | <0.001 | 4608 (92.9) | 1777 (86.3) | 928 (86.1) | <0.001 |
| ≥30 | 63 (5.2) | 178 (13.0) | 163 (13.8) | 323 (8.0) | 112 (15.0) | 5 (16.3) | 386 (7.1) | 290 (13.7) | 168 (13.9) | |||
| eGFR | ||||||||||||
| <60 | 1234 (99.1) | 1179 (94.9) | 1012 (96.5) | <0.001 | 3641 (97.7) | 766 (95.2) | 33 (91.4) | 0.004 | 4875 (98.1) | 1945 (95.0) | 1045 (96.3) | <0.001 |
| ≥60 | 20 (0.9) | 81 (5.1) | 49 (3.5) | 99 (2.3) | 41 (4.8) | 2 (8.6) | 119 (1.9) | 122 (5.0) | 51 (3.7) | |||
| High risk of CKD | ||||||||||||
| No | 1173 (94.0) | 1033 (83.7) | 867 (84.0) | <0.001 | 3354 (90.5) | 675 (83.0) | 28 (75.1) | <0.001 | 4527 (91.5) | 1708 (83.5) | 895 (83.8) | <0.001 |
| Yes | 81 (6.0) | 227 (16.3) | 194 (16.0) | 386 (9.5) | 132 (17.0) | 7 (24.9) | 467 (8.5) | 359 (16.5) | 201 (16.2) | |||
| Cardiovascular disease | ||||||||||||
| No | 1110 (98.0) | 1075 (95.4) | 1000 (95.4) | <0.001 | 3388 (98.4) | 768 (96.0) | 34 (97.5) | <0.001 | 4498 (98.3) | 1843 (95.6) | 1034 (95.5) | <0.001 |
| Yes | 34 (2.0) | 64 (4.6) | 59 (4.6) | 67 (1.6) | 39 (4.0) | 1 (2.5) | 101 (1.7) | 103 (4.4) | 60 (4.5) | |||
| Not response | 110 | 121 | 2 | 285 | 0 | 0 | 395 | 121 | 2 | |||
| Working hours | ||||||||||||
| ≤40 | 787 (58.4) | 890 (64.8) | 657 (56.6) | 0.003 | 3166 (84.3) | 700 (86.4) | 30 (78.6) | 0.423 | 3953 (76.3) | 1059 (72.2) | 687 (57.2) | <0.001 |
| >40 | 467 (41.6) | 370 (35.2) | 404 (43.4) | 574 (15.7) | 107 (13.6) | 5 (21.4) | 1041 (23.7) | 477 (27.8) | 409 (42.8) | |||
| OSA | Albuminuria | CKD | |
|---|---|---|---|
| Odds Ratio (95% CI) | Odds Ratio (95% CI) | ||
| Men | |||
| Working hours > 40 h | Low | 1 (Reference) | 1 (Reference) |
| Intermediate | 1.37 (0.67–2.81) | 1.28 (0.68–2.41) | |
| High | 2.09 (1.05–4.15) | 2.04 (1.08–3.86) | |
| Working hours ≤ 40 h | Low | 1 (Reference) | 1 (Reference) |
| Intermediate | 1.35 (0.81–2.24) | 1.39 (0.88–2.20) | |
| High | 1.54 (0.90–2.64) | 1.51 (0.93–2.47) | |
| Women | |||
| Working hours > 40 h | Low | 1 (Reference) | 1 (Reference) |
| Intermediate | 1.02 (0.33–3.11) | 0.98 (0.32–2.95) | |
| High | 1.17 (0.18–7.80) | 6.22 (0.88–44.10) | |
| Working hours ≤ 40 h | Low | 1 (Reference) | 1 (Reference) |
| Intermediate | 1.10 (0.81–1.50) | 0.97 (0.73–1.30) | |
| High | 0.84 (0.23–3.09) | 0.77 (0.25–2.37) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, S.-M.; Lee, M.-R. Association between Obstructive Sleep Apnea and Chronic Kidney Disease According to Sex, Long Working Hours: The Korean National Health and Nutrition Examination Survey (2019–2020). Life 2023, 13, 1625. https://doi.org/10.3390/life13081625
Jung S-M, Lee M-R. Association between Obstructive Sleep Apnea and Chronic Kidney Disease According to Sex, Long Working Hours: The Korean National Health and Nutrition Examination Survey (2019–2020). Life. 2023; 13(8):1625. https://doi.org/10.3390/life13081625
Chicago/Turabian StyleJung, Sung-Min, and Mee-Ri Lee. 2023. "Association between Obstructive Sleep Apnea and Chronic Kidney Disease According to Sex, Long Working Hours: The Korean National Health and Nutrition Examination Survey (2019–2020)" Life 13, no. 8: 1625. https://doi.org/10.3390/life13081625