
Biochemical and Microbiological Aspects of the Oral Cavity of Children and Young People with Neurological Impairment and Oropharyngeal Dysphagia

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Type and Ethical Considerations
2.2. Setting
2.3. Participant Selection
Inclusion and Exclusion Criteria
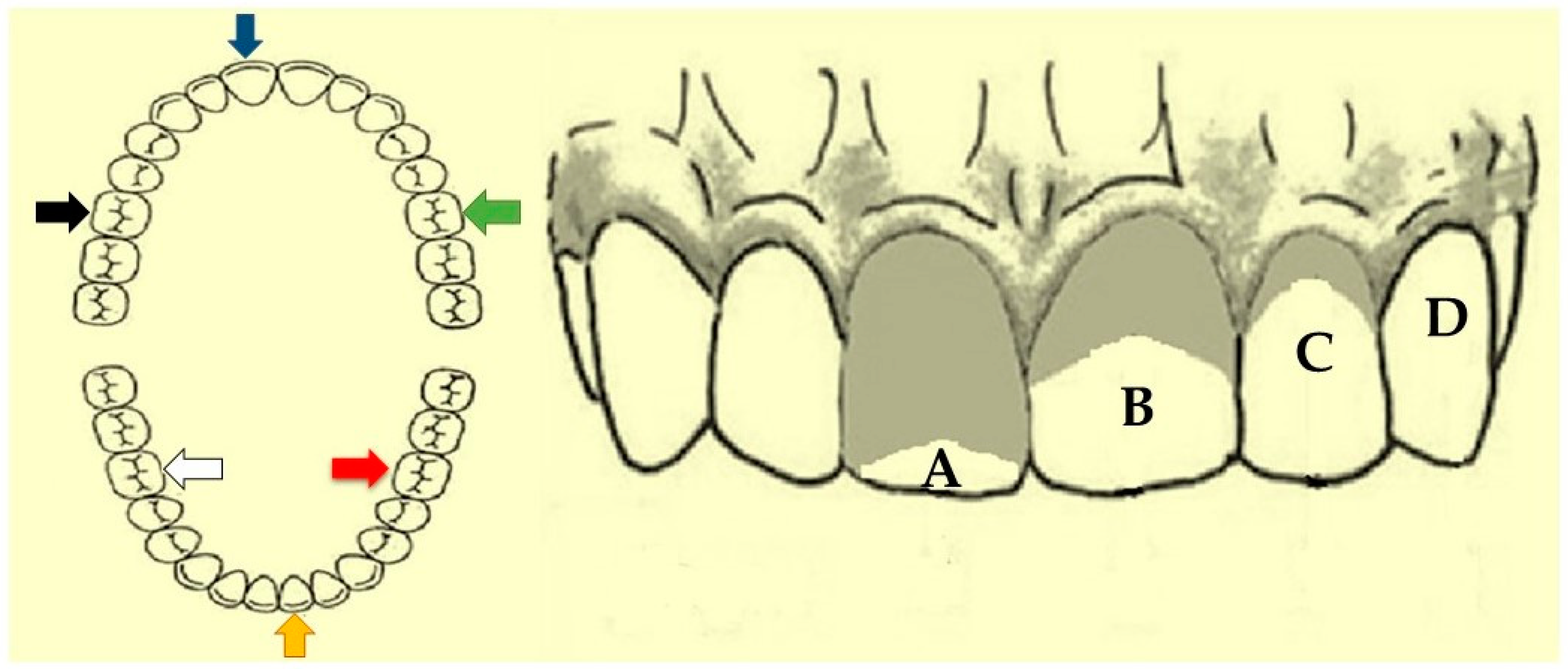
2.4. Oral Hygiene Index—Simplified (OHI-S)
2.5. Salivary pH
2.6. Salivary Flow
2.7. Saliva Collection
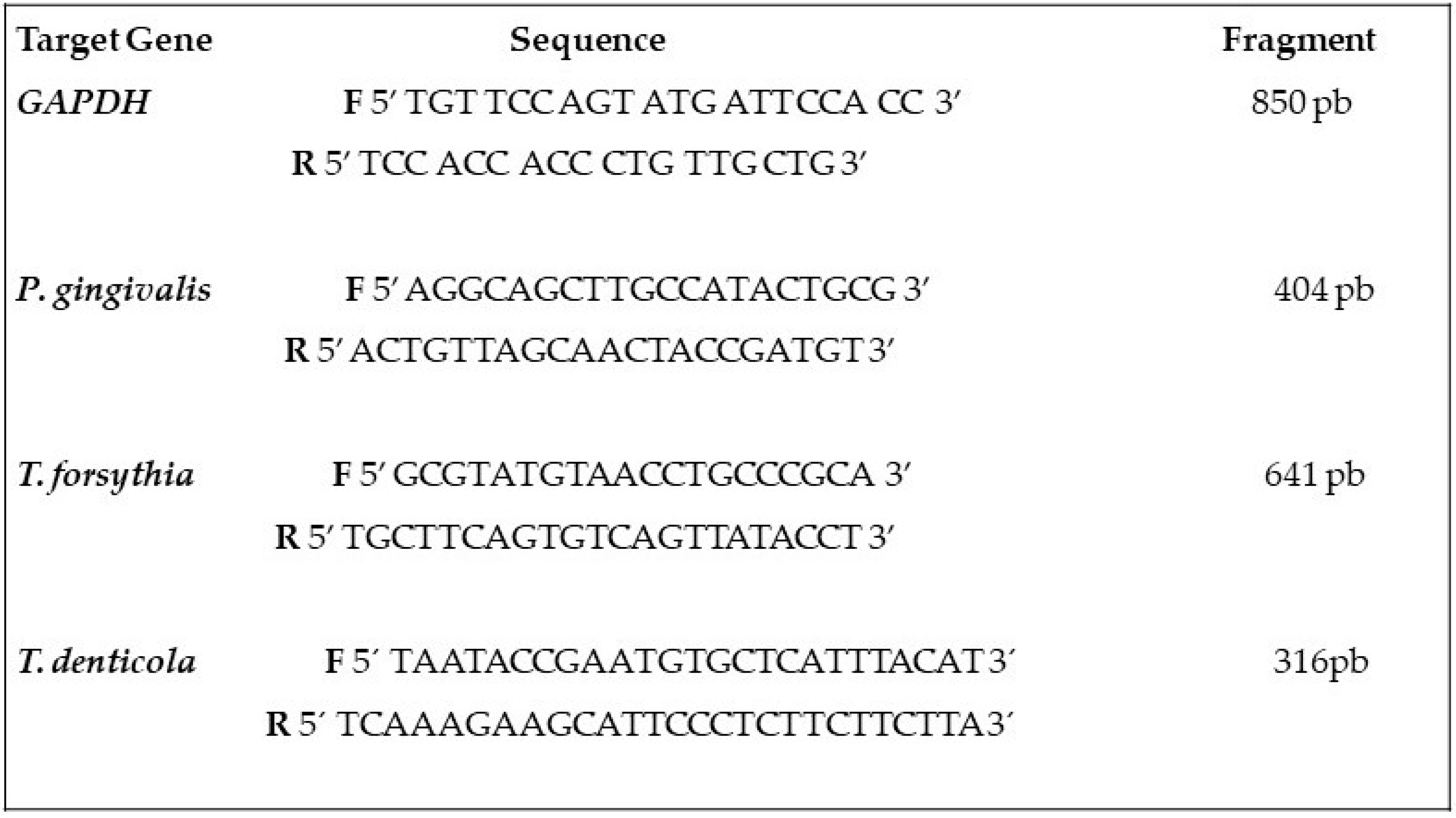
2.8. Bacterial Analysis
2.9. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rosenbaum, P.; Paneth, N.; Leviton, A.; Goldstein, M.; Bax, M.; Damiano, D.; Dan, B.; Jacobsson, B. A report: The definition and classification of cerebral palsy. Dev. Med. Child. Neurol. 2007, 109, 8–14. [Google Scholar]
- Pinto, V.V.; Alves, L.A.C.; Mendes, F.M.; Ciamponi, A.L. The nutritional state of children and adolescents with cerebral palsy is associated with oral motor dysfunction and social conditions: A cross sectional study. BMC Neurol. 2016, 16, 55. [Google Scholar] [CrossRef] [Green Version]
- Gauderer, M.W. Percutaneous endoscopic gastrostomy and the evolution of contemporary long-term enteral access. Clin. Nutr. 2002, 21, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, S.M.; Burgos, M.G.; Santos, E.M.; Prado, L.V.; Petribú, M.M.; Bomfim, F.M. Gastrointestinal complications and protein-calorie adequacy in intensive care unit enteral nutrition patients. Rev. Bras. Ter. Intensiv. 2010, 22, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Dougherty, N.J. A review of cerebral palsy for the oral health professional. Dent. Clin. N. Am. 2009, 53, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Novak, I.; Hines, M.; Goldsmith, S.; Barclay, R. Clinical prognostic messages from a systematic review on cerebral palsy. Pediatrics 2012, 130, e1285–e1312. [Google Scholar] [CrossRef] [Green Version]
- Reid, S.M.; McCutcheon, J.; Reddihough, D.S.; Johnson, H. Prevalence and predictors of drooling in 7- to 14-year-old children with cerebral palsy: A population study. Dev. Med. Child. Neurol. 2012, 54, 1032–1036. [Google Scholar] [CrossRef]
- Arvedson, J.C. Feeding children with cerebral palsy and swallowing difficulties. Eur. J. Clin. Nutr. 2013, 67, S9–S12. [Google Scholar] [CrossRef] [Green Version]
- Fregatto, L.F.; Costa, I.B.; De Bortoli Teixeira, D.; Duarte, J.C.M.; Mascarin, A.M.N.; da Silveira Junior, S.B.; Serva, B.E.B.M.; da Silvam, R.G.; Junior, F.A.; Cola, P.C. Oral hygiene and oral microbiota in children and young people with neurological impairment and oropharyngeal dysphagia. Sci. Rep. 2021, 11, 18090. [Google Scholar] [CrossRef]
- Littleton, N.W.; Kakehashi, S.; Fitzgerald, F.J. Study of differences in the occurrence of dental caries in Caucasian and Negro children. J. Dent. Res. 1970, 49, 742–751. [Google Scholar] [CrossRef]
- Klein, F.K.; Dicks, J.L. Evaluation of accumulation of calculus in tube-fed mentally handicapped patients. J. Am. Dent. Assoc. 1984, 108, 352–354. [Google Scholar] [CrossRef]
- Dicks, J.L.; Banning, J.S. Evaluation of calculus accumulation in tube-fed, mentally handicapped patients: The effects of oral hygiene status. Spec. Care Dentist. 1991, 11, 104–106. [Google Scholar] [CrossRef]
- Jawadi, A.H.; Casamassimo, P.S.; Griffen, A.; Enrile, B.; Marcone, M. Comparison of oral findings in special needs children with and without gastrostomy. Pediatr. Dent. 2004, 26, 283–288. [Google Scholar]
- Ayars, G.H.; Altman, L.C.; Fretwell, M.D. Effect of decreased salivation and pH on the adherence of Klebsiella species to human buccal epithelial cells. Infect. Immun. 1982, 38, 179–182. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues Santos, M.T.; Siqueira, W.L.; Nicolau, J. Amylase and peroxidase activities and sialic acid concentration in saliva of adolescents with cerebral palsy. Quintessence Int. 2007, 38, 467–472. [Google Scholar]
- Santos, M.T.; Batista, R.; Guaré, R.O.; Leite, M.F.; Ferreira, M.C.; Durão, M.S.; Nascimento, O.A.; Jardim, J.R. Salivary osmolality and hydration status in children with cerebral palsy. J. Oral Pathol. Med. 2011, 40, 582–586. [Google Scholar] [CrossRef]
- Faveri, M.; Figueiredo, L.C.; Duarte, P.M.; Mestnik, M.J.; Mayer, M.P.; Feres, M. Microbiological profile of untreated subjects with localized aggressive periodontitis. J. Clin. Periodontol. 2009, 36, 739–749. [Google Scholar] [CrossRef] [PubMed]
- Ramseier, C.A.; Kinney, J.S.; Herr, A.E.; Braun, T.; Sugai, J.V.; Shelburne, C.A.; Rayburn, L.A.; Tran, H.M.; Singh, A.K.; Giannobile, W.V. Identification of pathogen and host-response markers correlated with periodontal disease. J. Periodontol. 2009, 80, 436–446. [Google Scholar] [CrossRef] [PubMed]
- Wara-aswapati, N.; Pitiphat, W.; Chanchaimongkon, L.; Taweechaisupapong, S.; Boch, J.A.; Ishikawa, I. Red bacterial complex is associated with the severity of chronic periodontitis in a Thai population. Oral Dis. 2009, 15, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Kebschull, M.; Papapanou, P.N. Periodontal microbial complexes associated with specific cell and tissue responses. J. Clin. Periodontol. 2011, 38, 17–27. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. BMJ Clin. Res. Ed. 2007, 335, 806–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greene, J.C.; Vermillion, J.R. The simplified oral hygiene index. J. Am. Dent. Assoc. 1964, 68, 7–13. [Google Scholar] [CrossRef]
- Serratine, A.C.P.; Silva, M.R.M. Validação de um método simplificado de avaliação do pH salivar em crianças. Pesq. Bras. Odontoped. Clin. Integr. 2009, 9, 217–221. [Google Scholar] [CrossRef]
- Chaves Neto, A.H.; Sassaki, K.T.; Nakamune, A.C.M.S. Protein phosphatase activities in the serum and saliva of healthy children. RPG Rev. Pos. Grad. 2011, 18, 90–95. [Google Scholar]
- Dalpke, A.; Frank, J.; Peter, M.; Heeg, K. Activation of Toll-Like Receptor 9 by DNA from Different Bacterial Species. Infect. Immun. 2006, 74, 940–946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Carvalho, R.B.; Mendes, R.F.; Prado, R.R., Jr.; Moita Neto, J.M. Oral health and oral motor function in children with cerebral palsy. Spec. Care Dentist. 2011, 31, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Morales-Chávez, M.; Rada-Berroteran, A.; Arcila-Ramos, L. Periodontal status of mentally handicapped school children in Caracas, Venezuela. A cross-sectional study. J. Oral Res. 2014, 3, 156–161. [Google Scholar] [CrossRef] [Green Version]
- El Ashiry, E.A.; Alaki, S.M.; Nouri, S.M. Oral Health Quality of Life in Children with Cerebral Palsy: Parental Perceptions. J. Clin. Pediatr. Dent. 2016, 40, 375–387. [Google Scholar] [CrossRef]
- Wyne, A.H.; Al-Hammad, N.S.; Splieth, C.H. Dental caries and related risk factors in Saudi cerebral palsy children. Neurosciences 2017, 22, 282–286. [Google Scholar] [CrossRef] [Green Version]
- Makkar, H.; Reynolds, M.A.; Wadhawan, A.; Dagdag, A.; Merchant, A.T.; Postolache, T.T. Periodontal, metabolic, and cardiovascular disease: Exploring the role of inflammation and mental health. Pteridines 2018, 29, 124–163. [Google Scholar] [CrossRef]
- Hoshino, T.; Kawaguchi, M.; Shimizu, N.; Hoshino, N.; Ooshima, T.; Fujiwara, T. PCR detection and identification of oral streptococci in saliva samples using gtf genes. Diagn. Microbiol. Infect. Dis. 2004, 48, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Lima, E.D.A.; Facundo, A.G.L.F.; Carvalho, A.C.L.C.; Silva, E.B.; Gomes, C.F.; Cabral, G.M. Saliva e Hidratação. Importância da quantidade e da qualidade da saliva para manutenção da condição bucal satisfatória em pacientes com paralisia cerebral. Rev. Campo Do Saber 2017, 3, 101–119. [Google Scholar]
- Previtali, E.F.; Santos, M.T.B.R. Cárie Dentária e Higiene Bucal em Crianças com Paralisia Cerebral Tetraparesia Espástica com Alimentação por Vias Oral e Gastrostomia. Pesq. Bras. Odontoped. Clin. Integr. 2009, 9, 43–47. [Google Scholar] [CrossRef]
- Ferreira, A.D.S.P.; Silva, H.A.B.; Buzalaf, M.A.R.; Kato, M.T.; Marta, S.N. Alterações salivares em pacientes submetidos à gastrostomia. Arch. Health Investig. 2016, 5, 92. [Google Scholar]
- Hidas, A.; Cohen, J.; Beeri, M.; Shapira, J.; Steinberg, D.; Moskovitz, M. Salivary bacteria and oral health status in children with disabilities fed through gastrostomy. Int. J. Paediatr. Dent. 2010, 20, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Aframian, D.J.; Davidowitz, T.; Benoliel, R. The distribution of oral mucosal pH values in healthy saliva secretors. Oral Dis. 2006, 12, 420–423. [Google Scholar] [CrossRef]
- Zero, D.T.; Brennan, M.T.; Daniels, T.E.; Papas, A.; Stewart, C.; Pinto, A.; Al-Hashimi, I.; Navazesh, M.; Rhodus, N.; Sciubba, J.; et al. Clinical practice guidelines for oral management of Sjögren disease: Dental caries prevention. J. Am. Dent. Assoc. 2016, 147, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Kakodkar, K.; Schroeder, J.W., Jr. Pediatric dysphagia. Pediatr. Clin. N. Am. 2013, 60, 969–977. [Google Scholar] [CrossRef]
- Erasmus, C.E.; Van Hulst, K.; Rotteveel, L.J.; Jongerius, P.H.; Van Den Hoogen, F.J.; Roeleveld, N.; Rotteveel, J.J. Drooling in cerebral palsy: Hypersalivation or dysfunctional oral motor control? Dev. Med. Child. Neurol. 2009, 51, 454–459. [Google Scholar] [CrossRef]
- Hegde, A.M.; Pani, S.C. Drooling of saliva in children with cerebral palsy-etiology, prevalence, and relationship to salivary flow rate in an Indian population. Spec. Care Dentist. 2009, 29, 163–168. [Google Scholar] [CrossRef]
- Dias, B.L.; Fernandes, A.R.; Maia Filho, H.S. Sialorrhea in children with cerebral palsy. J. Pediatr. 2016, 92, 549–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Subramaniam, P.; Babu, K.L.; Rodriguez, A. Relation of salivary risk factors to dental caries in children with cerebral palsy. J. Clin. Pediatr. Dent. 2010, 34, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Papaioannou, W.; Gizani, S.; Haffajee, A.D.; Quirynen, M.; Mamai-Homata, E.; Papagiannoulis, L. The microbiota on different oral surfaces in healthy children. Oral Microbiol. Immunol. 2009, 24, 183–189. [Google Scholar] [CrossRef]
- Faria Carrada, C.; Almeida Ribeiro Scalioni, F.; Evangelista Cesar, D.; Lopes Devito, K.; Ribeiro, L.C.; Almeida Ribeiro, R. Salivary Periodontopathic Bacteria in Children and Adolescents with Down Syndrome. PLoS ONE 2016, 11, e0162988. [Google Scholar] [CrossRef] [PubMed]
- Bodet, C.; Chandad, F.; Grenier, D. Pathogenic potential of Porphyromonas gingivalis, Treponema denticola and Tannerella forsythia, the red bacterial complex associated with periodontitis. Pathol. Biol. 2007, 55, 154–162. [Google Scholar] [CrossRef]
- Naka, S.; Yamana, A.; Nakano, K.; Okawa, R.; Fujita, K.; Kojima, A.; Nemoto, H.; Nomura, R.; Matsumoto, M.; Ooshima, T. Distribution of periodontopathic bacterial species in Japanese children with developmental disabilities. BMC Oral Health 2009, 9, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mineoka, T.; Awano, S.; Rikimaru, T.; Kurata, H.; Yoshida, A.; Ansai, T.; Takehara, T. Site-specific development of periodontal disease is associated with increased levels of Porphyromonas gingivalis, Treponema denticola, and Tannerella forsythia in subgingival plaque. J. Periodontol. 2008, 79, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Mättö, J.; Saarela, M.; Alaluusua, S.; Oja, V.; Jousimies-Somer, H.; Asikainen, S. Detection of Porphyromonas gingivalis from saliva by PCR by using a simple sample-processing method. J. Clin. Microbiol. 1998, 36, 157–160. [Google Scholar] [CrossRef] [Green Version]
- Brodeur, C.; Belley, É.; Deschênes, L.-M.; Enriquez-Rosas, A.; Hubert, M.; Guimond, A.; Bilodeau, J.; Soucy, J.-P.; Macoir, J. Primary and Secondary Progressive Aphasia in Posterior Cortical Atrophy. Life 2022, 12, 662. [Google Scholar] [CrossRef]
- Bensi, C.; Costacurta, M.; Docimo, R. Oral health in children with cerebral palsy: A systematic review and meta-analysis. Spec. Care Dentist. 2020, 40, 401–411. [Google Scholar] [CrossRef]
- Sakellari, D.; Belibasakis, G.; Chadjipadelis, T.; Arapostathis, K.; Konstantinidis, A. Supragingival and subgingival microbiota of adult patients with Down’s syndrome. Changes after periodontal treatment. Oral Microbiol. Immunol. 2001, 16, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Martinez, R.E.; Loyola-Rodriguez, J.P.; Bonilla-Garro, S.E.; Patiño-Marin, N.; Haubek, D.; Amano, A.; Poulsen, K. Characterization of periodontal biofilm in Down syndrome patients: A comparative study. J. Clin. Pediatr. Dent. 2013, 37, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Monte, M.A.; Veroux, M.; Rodolico, M.S.; Losi, V.; Di Pino, L.; Bella, R.; Lanza, G.; Monte, I.P. Fabry’s Disease: The Utility of a Multidisciplinary Screening Approach. Life 2022, 12, 623. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group I | Group II | Total | p-Value * | |
|---|---|---|---|---|
| Median (Interquartile) | Median (Interquartile) | Median (Interquartile) | ||
| Oral Hygiene (level) | 4.00 (1.68) | 2.00 (0.93) | 2.50 (2.4) | 0.0003 |
| Plaque | 2.10 (1.08) | 1.80 (0.5) | 2.00 (0.7) | 0.2939 |
| Calculus | 2.00 (0.85) | 0.00 (0.08) | 0.50 (2) | 0.0000 |
| Group I | Group II | Total | p-Value * | |
|---|---|---|---|---|
| Median (Interquartile) | Median (Interquartile) | Median (Interquartile) | ||
| Salivary pH | 7.50 (1.0) | 6.00 (0.62) | 6.70 (1.5) | 0.0000 |
| Salivary flow | 0.80 (0.5) | 0.70 (0.72) | 0.70 (0.7) | 0.1168 |
| Porphyromonas gingivalis | Tannerella forsythia | Treponema denticola | ||||
|---|---|---|---|---|---|---|
| No | Yes | No | Yes | No | Yes | |
| Group I (%) | 5 (26.3) | 14 (73.7) | 5 (26.3) | 14 (73.7) | 9 (47.4) | 10 (52.6) |
| Group II (%) | 10 (50) | 10 (50) | 10 (50) | 10 (50) | 11 (55) | 9 (45) |
| Total (%) | 15 (38.5) | 24 (61.5) | 15 (38.5) | 24 (61.5) | 20 (51.3) | 19 (48.7) |
| p-value * | 0.2339 | 0.2339 | 0.8759 | |||
| Variables | Β | 95% CI | p-Value * | Model | |||
|---|---|---|---|---|---|---|---|
| Dependent | Independent | Lower Bound | Upper Bound | p-Value | R2 | ||
| Oral Hygiene | Gastrostomy (1 = yes; 2 = no) | −1.540 | −2.353 | −0.727 | <0.001 | <0.001 | 0.382 |
| Age (years) | 0.042 | −0.035 | 0.120 | 0.277 | |||
| Calculus | Gastrostomy (1 = yes; 2 = no) | −1.579 | −2.049 | −1.109 | <0.001 | <0.001 | 0.604 |
| Age (years) | 0.005 | −0.040 | 0.050 | 0.818 | |||
| Salivary pH | Gastrostomy (1 = yes; 2 = no) | −1.197 | −1.656 | −0.737 | <0.001 | <0.001 | 0.492 |
| Gender (1 = male; 2 = female) | −0.392 | −0.854 | 0.070 | 0.094 | |||
| Salivary flow | Gastrostomy (1 = yes; 2 = no) | −0.064 | −0.334 | 0.205 | 0.630 | 0.092 | 0.124 |
| Gender (1 = male; 2 = female) | −0.277 | −0.547 | −0.007 | 0.044 * | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duarte, J.C.M.; Costa, I.B.; Teixeira, D.d.B.; Fregatto, L.F.; Mendes, C.G.; Mascarin, A.M.N.; da Silveira Junior, S.B.; Serva, B.E.B.M.; Comar, L.P.; da Silva, R.G.; et al. Biochemical and Microbiological Aspects of the Oral Cavity of Children and Young People with Neurological Impairment and Oropharyngeal Dysphagia. Life 2023, 13, 1342. https://doi.org/10.3390/life13061342
Duarte JCM, Costa IB, Teixeira DdB, Fregatto LF, Mendes CG, Mascarin AMN, da Silveira Junior SB, Serva BEBM, Comar LP, da Silva RG, et al. Biochemical and Microbiological Aspects of the Oral Cavity of Children and Young People with Neurological Impairment and Oropharyngeal Dysphagia. Life. 2023; 13(6):1342. https://doi.org/10.3390/life13061342
Chicago/Turabian StyleDuarte, Janaina Costa Marangon, Isabela Bazzo Costa, Daniel de Bortoli Teixeira, Luiz Fernando Fregatto, Claudemir Gregorio Mendes, Aline Maria Noli Mascarin, Salum Bueno da Silveira Junior, Bianca Eduarda Baptistella Mesquita Serva, Livia Picchi Comar, Roberta Gonçalves da Silva, and et al. 2023. "Biochemical and Microbiological Aspects of the Oral Cavity of Children and Young People with Neurological Impairment and Oropharyngeal Dysphagia" Life 13, no. 6: 1342. https://doi.org/10.3390/life13061342