
Using Real-Time PCR Fluorescence Reaction Values to Improve SARS-CoV-2 Virus Detection and Benefit Clinical Decision-Making
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Equipment
2.3. RNA Extraction
2.3.1. BD MAX™ SARS-CoV-2 Assay
2.3.2. Cepheid Xpert® Xpress SARS-CoV-2 Assay
2.3.3. LabTurbo AIO COVID-19 RNA
2.4. Interpretation of Patient Specimen Results
2.4.1. BD MAX™ SARS-CoV-2 Assay
2.4.2. Cepheid Xpert® Xpress SARS-CoV-2 Assay
2.4.3. LabTurbo AIO COVID-19 RNA
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Kruger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Zuo, Y.Y.; Uspal, W.E.; Wei, T. Airborne Transmission of COVID-19: Aerosol Dispersion, Lung Deposition, and Virus-Receptor Interactions. ACS Nano 2020, 14, 16502–16524. [Google Scholar] [CrossRef] [PubMed]
- Kalinina, O.; Golovkin, A.; Zaikova, E.; Aquino, A.; Bezrukikh, V.; Melnik, O.; Vasilieva, E.; Karonova, T.; Kudryavtsev, I.; Shlyakhto, E. Cytokine Storm Signature in Patients with Moderate and Severe COVID-19. Int. J. Mol. Sci. 2022, 23, 8879. [Google Scholar] [CrossRef] [PubMed]
- Jose, R.J.; Manuel, A. COVID-19 cytokine storm: The interplay between inflammation and coagulation. Lancet Respir. Med. 2020, 8, e46–e47. [Google Scholar] [CrossRef]
- Fernandez-de-Las-Penas, C.; Cuadrado, M.L.; Gomez-Mayordomo, V.; Torres-Macho, J.; Pellicer-Valero, O.J.; Martin-Guerrero, J.D.; Arendt-Nielsen, L. Headache as a COVID-19 onset symptom and post-COVID-19 symptom in hospitalized COVID-19 survivors infected with the Wuhan, Alpha, or Delta SARS-CoV-2 variants. Headache 2022, 62, 1148–1152. [Google Scholar] [CrossRef]
- Chakraborty, C.; Sharma, A.R.; Bhattacharya, M.; Sharma, G.; Lee, S.S.; Agoramoorthy, G. COVID-19: Consider IL-6 receptor antagonist for the therapy of cytokine storm syndrome in SARS-CoV-2 infected patients. J. Med. Virol. 2020, 92, 2260–2262. [Google Scholar] [CrossRef]
- Wolfe, M.; Hughes, B.; Duong, D.; Chan-Herur, V.; Wigginton, K.R.; White, B.J.; Boehm, A.B. Detection of SARS-CoV-2 Variants Mu, Beta, Gamma, Lambda, Delta, Alpha, and Omicron in Wastewater Settled Solids Using Mutation-Specific Assays Is Associated with Regional Detection of Variants in Clinical Samples. Appl. Environ. Microbiol. 2022, 88, e0004522. [Google Scholar] [CrossRef]
- Gandhi, M.; Yokoe, D.S.; Havlir, D.V. Asymptomatic Transmission, the Achilles’ Heel of Current Strategies to Control COVID-19. N. Engl. J. Med. 2020, 382, 2158–2160. [Google Scholar] [CrossRef]
- Cascella, M.; Rajnik, M.; Aleem, A.; Dulebohn, S.C.; Di Napoli, R. Features, Evaluation, and Treatment of Coronavirus (COVID-19). In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Hu, D. Identification of Shrinking Cities on the Main Island of Taiwan Based on Census Data and Population Registers: A Spatial Analysis. ISPRS Int. J. Geo-Inf. 2021, 10, 694. [Google Scholar] [CrossRef]
- Jerbi, L.; Azrad, M.; Peretz, A. Evaluation of Factors that Affect the Performance of COVID-19 Molecular Assays Including Presence of Symptoms, Number of Detected Genes and RNA Extraction Type. Mol. Diagn. Ther. 2022, 26, 229–238. [Google Scholar] [CrossRef]
- Caruana, G.; Brouillet, R.; Opota, O.; Greub, G. Assessment of SARS-CoV-2 tests costs and reimbursement tariffs readjustments during the COVID-19 pandemic. Swiss Med. Wkly. 2022, 152, w30168. [Google Scholar] [CrossRef] [PubMed]
- Jian, M.J.; Chung, H.Y.; Chang, C.K.; Lin, J.C.; Yeh, K.M.; Chiu, S.K.; Wang, Y.H.; Liao, S.J.; Li, S.Y.; Hsieh, S.S.; et al. Novel automated sample-to-result SARS-CoV-2 laboratory-developed RT-PCR assay for high-throughput testing using LabTurbo AIO 48 system. Clin. Chim. Acta 2021, 514, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Navarathna, D.H.; Sharp, S.; Lukey, J.; Arenas, M.; Villas, H.; Wiley, L.; Englett, I.; Juan, M.R.S.; Jinadatha, C. Understanding false positives and the detection of SARS-CoV-2 using the Cepheid Xpert Xpress SARS-CoV-2 and BD MAX SARS-CoV-2 assays. Diagn. Microbiol. Infect. Dis. 2021, 100, 115334. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration. False Positive Results with BD SARS-CoV-2 Reagents for the BD Max System—Letter to Clinical Laboratory Staff and Health Care Providers; Food and Drug Administration: Montgomery, MD, USA, 2020. [Google Scholar]
- Wilson, M.J.; Sparkes, D.; Myers, C.; Smielewska, A.A.; Husain, M.M.; Smith, C.; Rolfe, K.J.; Zhang, H.; Jalal, H. Streamlining SARS-CoV-2 confirmatory testing to reduce false positive results. J. Clin. Virol. 2021, 136, 104762. [Google Scholar] [CrossRef]
- Lu, X.; Wang, L.; Sakthivel, S.K.; Whitaker, B.; Murray, J.; Kamili, S.; Lynch, B.; Malapati, L.; Burke, S.A.; Harcourt, J.; et al. US CDC Real-Time Reverse Transcription PCR Panel for Detection of Severe Acute Respiratory Syndrome Coronavirus 2. Emerg. Infect. Dis. 2020, 26, 1654–1665. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.Y.; Jian, M.J.; Chang, C.K.; Lin, J.C.; Yeh, K.M.; Chen, C.W.; Yang, Y.S.; Hsieh, S.S.; Chen, E.S.; Yang, M.H.; et al. Multicenter study evaluating novel multi-specimen pooling assay for the detection of SARS-CoV-2: High sensitivity and high throughput testing. J. Microbiol. Immunol. Infect. 2022, 55, 1069–1075. [Google Scholar] [CrossRef]
- Miller, S.; Lee, T.; Merritt, A.; Pryce, T.; Levy, A.; Speers, D. Single-Point Mutations in the N Gene of SARS-CoV-2 Adversely Impact Detection by a Commercial Dual Target Diagnostic Assay. Microbiol. Spectr. 2021, 9, e0149421. [Google Scholar] [CrossRef]
- Falasca, F.; Sciandra, I.; Di Carlo, D.; Gentile, M.; Deales, A.; Antonelli, G.; Turriziani, O. Detection of SARS-COV N2 Gene: Very low amounts of viral RNA or false positive? J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2020, 133, 104660. [Google Scholar] [CrossRef]
- AlBahrani, S.; Alghamdi, M.; Zakary, N.; Jebakumar, A.Z.; AlZahrani, S.J.; ElGezery, M.H.; Abdallah, K.O.; Al-Tawfiq, J.A. Initial viral cycle threshold values in patients with COVID-19 and their clinical significance. Eur. J. Med. Res. 2022, 27, 101. [Google Scholar] [CrossRef]
- Mishra, B.; Ranjan, J.; Purushotham, P.; Kar, P.; Payal, P.; Saha, S.; Deshmukh, V.; Das, S. Comparison of Cycle Threshold and Clinical Status Among Different Age Groups of COVID-19 Cases. Cureus 2022, 14, e24194. [Google Scholar] [CrossRef]
- Coyle, P.V.; Al Molawi, N.H.; Kacem, M.; El Kahlout, R.A.; Al Kuwari, E.; Al Khal, A.; Gillani, I.; Jeremijenko, A.; Saeb, H.; Al Thani, M.; et al. Reporting of RT-PCR cycle threshold (Ct) values during the first wave of COVID-19 in Qatar improved result interpretation in clinical and public health settings. J. Med. Microbiol. 2022, 7, 1499. [Google Scholar] [CrossRef]
- Tok, Y.T.; Kuskucu, M.A.; Erdem, H.; Saribal, D.; Salman Yilmaz, S.; Nohut, O.K.; Karaali, R.; Balkan, I.I.; Mete, B.; Tabak, O.F.; et al. Detection of SARS-CoV-2 RNA in Upper Respiratory Swap Samples by Pooling Method. Balkan. Med. J. 2022, 39, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Contreras, J.; Espinoza, M.A.; Sandoval-Jaime, C.; Cantu-Cuevas, M.A.; Madrid-Gonzalez, D.A.; Baron-Olivares, H.; Ortiz-Orozco, O.D.; Munoz-Rangel, A.V.; Guzman-Rodriguez, C.; Hernandez-de la Cruz, M.; et al. Pooling saliva samples as an excellent option to increase the surveillance for SARS-CoV-2 when re-opening community settings. PLoS ONE 2022, 17, e0263114. [Google Scholar] [CrossRef] [PubMed]
- Watkins, A.E.; Fenichel, E.P.; Weinberger, D.M.; Vogels, C.B.F.; Brackney, D.E.; Casanovas-Massana, A.; Campbell, M.; Fournier, J.; Bermejo, S.; Datta, R.; et al. Pooling saliva to increase SARS-CoV-2 testing capacity. medRxiv 2020, preprint. [Google Scholar] [CrossRef]
- Wang, H.; Hogan, C.A.; Miller, J.A.; Sahoo, M.K.; Huang, C.; Mfuh, K.O.; Sibai, M.; Zehnder, J.; Hickey, B.; Sinnott-Armstrong, N.; et al. Performance of Nucleic Acid Amplification Tests for Detection of Severe Acute Respiratory Syndrome Coronavirus 2 in Prospectively Pooled Specimens. Emerg. Infect. Dis. 2021, 27, 92. [Google Scholar] [CrossRef]
- Handous, I.; Hannachi, N.; Marzouk, M.; Hazgui, O.; Bouafif Ep Ben Alaya, N.; Boukadida, J. Pooling Nasopharyngeal Swab Specimens to Improve Testing Capacity for SARS-CoV-2 by Real-Time RT-PCR. Biol. Proced. Online 2021, 23, 19. [Google Scholar] [CrossRef]
- Wacharapluesadee, S.; Kaewpom, T.; Ampoot, W.; Ghai, S.; Khamhang, W.; Worachotsueptrakun, K.; Wanthong, P.; Nopvichai, C.; Supharatpariyakorn, T.; Putcharoen, O.; et al. Evaluating the efficiency of specimen pooling for PCR-based detection of COVID-19. J. Med. Virol. 2020, 92, 2193–2199. [Google Scholar] [CrossRef]
- Praharaj, I.; Jain, A.; Singh, M.; Balakrishnan, A.; Dhodapkar, R.; Borkakoty, B.; Ashok, M.; Das, P.; Biswas, D.; Kalawat, U.; et al. Pooled testing for COVID-19 diagnosis by real-time RT-PCR: A multi-site comparative evaluation of 5- & 10-sample pooling. Indian J. Med. Res. 2020, 152, 88–94. [Google Scholar] [CrossRef]
- Healy, B.; Khan, A.; Metezai, H.; Blyth, I.; Asad, H. The impact of false positive COVID-19 results in an area of low prevalence. Clin. Med. 2021, 21, e54–e56. [Google Scholar] [CrossRef]
- Lin, L.; Carlquist, J.; Sinclair, W.; Hall, T.; Lopansri, B.K.; Bennett, S.T. Experience with False-Positive Test Results on the TaqPath Real-Time Reverse Transcription-Polymerase Chain Reaction Coronavirus Disease 2019 (COVID-19) Testing Platform. Arch. Pathol. Lab. Med. 2021, 145, 259–261. [Google Scholar] [CrossRef]
- Fenaux, H.; Ghelfenstein-Ferreira, T.; Salmona, M.; Mahjoub, N.; Feghoul, L.; Maylin, S.; Chaix, M.L.; Minier, M.; Gabassi, A.; Goff, J.L.; et al. Interpretation of single target positivity among SARS-CoV-2 RT-PCR result tests. J. Clin. Virol. Plus 2021, 1, 100021. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Equipment | Target Gene | Primers and Probe | Oligonucleotide Sequence (5′ to 3′) | Reference |
|---|---|---|---|---|
| BD MAX™ | N1 | Forward primer | GACCCCAAAATCAGCGAAAT | [17] |
| Reverse primer | TCTGGTTACTGCCAGTTGAATCTG | |||
| Probe | FAM–ACCCCGCATTACGTTTGGTGGACC–BHQ1 | |||
| N2 | Forward primer | TTACAAACATTGGCCGCAAA | ||
| Reverse primer | GCGCGACATTCCGAAGAA | |||
| Probe | FAM–ACAATTTGCCCCCAGCGCTTCAG–BHQ1 | |||
| RNase P | Forward primer | AGATTTGGACCTGCGAGCG | ||
| Reverse primer | GAGCGGCTGTCTCCACAAGT | |||
| Probe | FAM–TTCTGACCTGAAGGCTCTGCGCG–BHQ1 | |||
| LabTurbo™ | E | Forward primer | ACAGGTACGTTAATAGTTAATAGCGT | [18] |
| Reverse primer | ATATTGCAGCAGTACGCACACA | |||
| Probe | FAM-ACACTAGCCATCCTTACTGCGCTTCG-BBQ | |||
| N1 | Forward primer | GACCCCAAAATCAGCGAAAT | ||
| Reverse primer | TCTGGTTACTGCCAGTTGAATCTG | |||
| Probe | /56FAM/ACCCCGCAT/ZEN/TACGTTTGGTGGACC/3IABkFQ/FAM/ACCCCGCAT/ZEN/TACGTTTGGTGGACC/3IABkFQ/ | |||
| GeneXpert | RNase P | Forward primer | AGATTTGGACCTGCGAGCG | [19] |
| Reverse primer | GAGCGGCTGTCTCCACAAGT | |||
| Probe | /5Cy5/TTCTGACCT/TAO/GAAGGCTCTGCGCG/3IAbRQSp/ | |||
| N2 | Forward primer | TTACAAACATTGGCCGCAAA | ||
| Reverse primer | CGCGCTGTAAGGCTTCTT | |||
| Probe | CACAATTTGCCCCCAGCGCTTC | |||
| E | Forward primer | Confidential issue | ||
| Reverse primer | Confidential issue | |||
| Probe | Confidential issue |
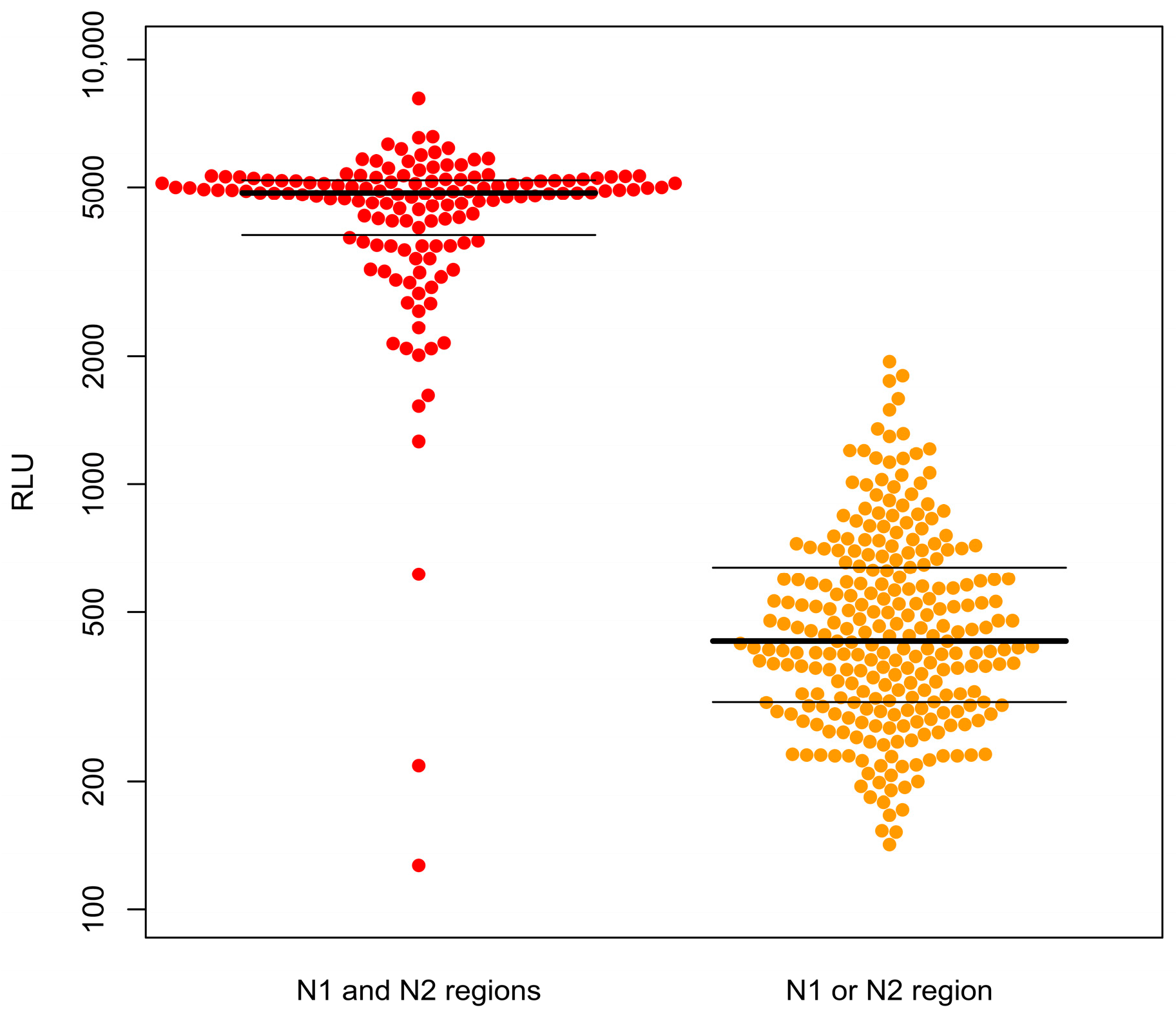
| Confirmed Negative | Confirmed Positive | Total | |
|---|---|---|---|
| N1 and N2 regions | 5 | 135 | 140 |
| N1 or N2 region | 258 | 2 | 260 |
| Total | 263 | 137 | 400 |
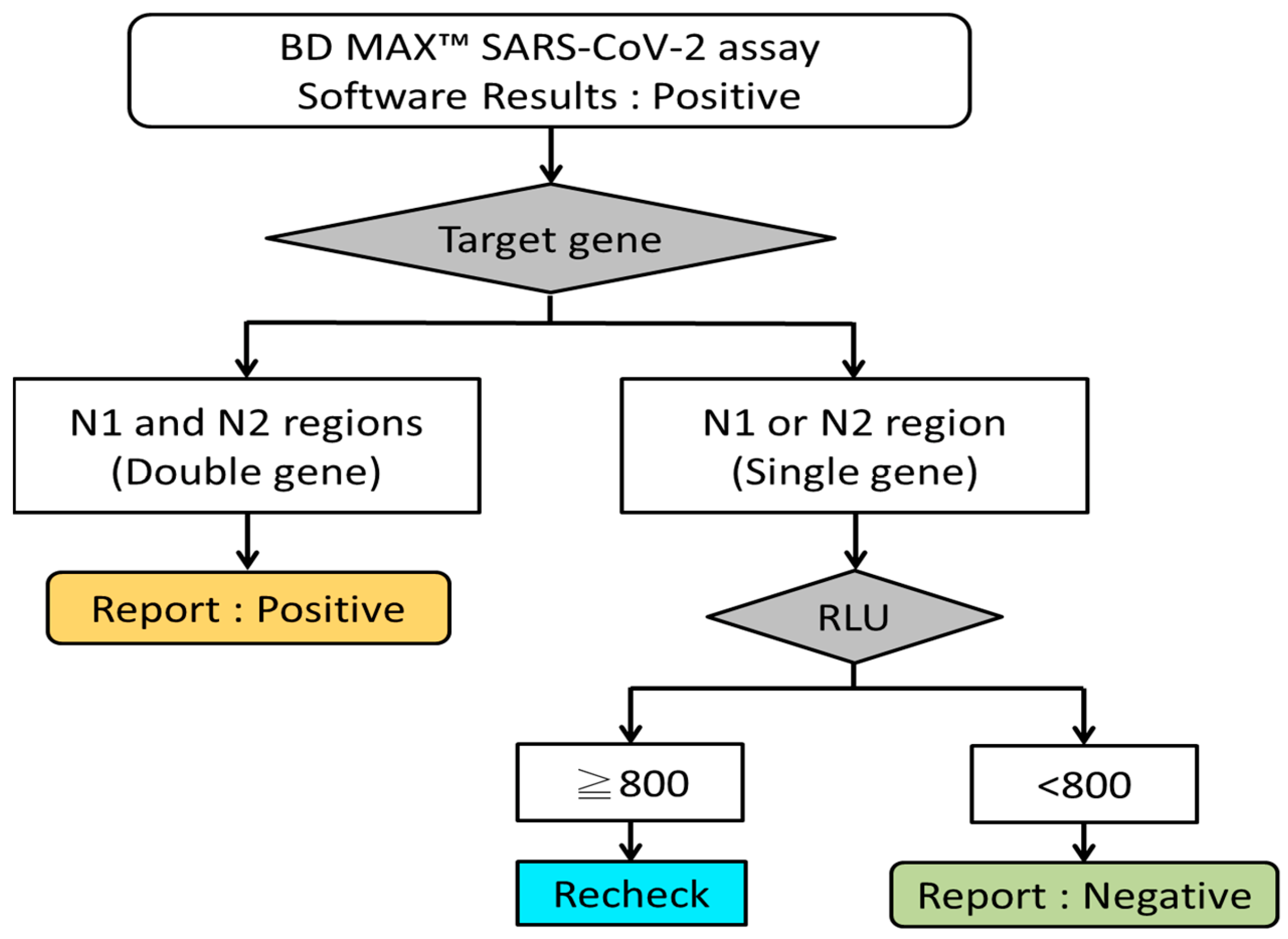
| Gene | RLU | Confirmed Negative | Confirmed Positive | Total |
|---|---|---|---|---|
| N1 or N2 region | RLU ≥ 800 | 34 | 2 | 36 |
| RLU < 800 | 224 | 0 | 224 | |
| Total | 258 | 2 | 260 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, W.-W.; Hsu, C.-W.; Chan, Y.-J.; Su, S.-B.; Feng, I.-J.; Hou, C.-Y.; Huang, C.-Y. Using Real-Time PCR Fluorescence Reaction Values to Improve SARS-CoV-2 Virus Detection and Benefit Clinical Decision-Making. Life 2023, 13, 683. https://doi.org/10.3390/life13030683
Yang W-W, Hsu C-W, Chan Y-J, Su S-B, Feng I-J, Hou C-Y, Huang C-Y. Using Real-Time PCR Fluorescence Reaction Values to Improve SARS-CoV-2 Virus Detection and Benefit Clinical Decision-Making. Life. 2023; 13(3):683. https://doi.org/10.3390/life13030683
Chicago/Turabian StyleYang, Wan-Wen, Chin-Wen Hsu, Yu-Ju Chan, Shih-Bin Su, I-Jung Feng, Chia-Yi Hou, and Chien-Yuan Huang. 2023. "Using Real-Time PCR Fluorescence Reaction Values to Improve SARS-CoV-2 Virus Detection and Benefit Clinical Decision-Making" Life 13, no. 3: 683. https://doi.org/10.3390/life13030683