
Pain Reduction during Rapid Palatal Expansion Due to LED Photobiomodulation Irradiation: A Randomized Clinical Trial

 , , , ,
, , , ,
Abstract
:1. Introduction
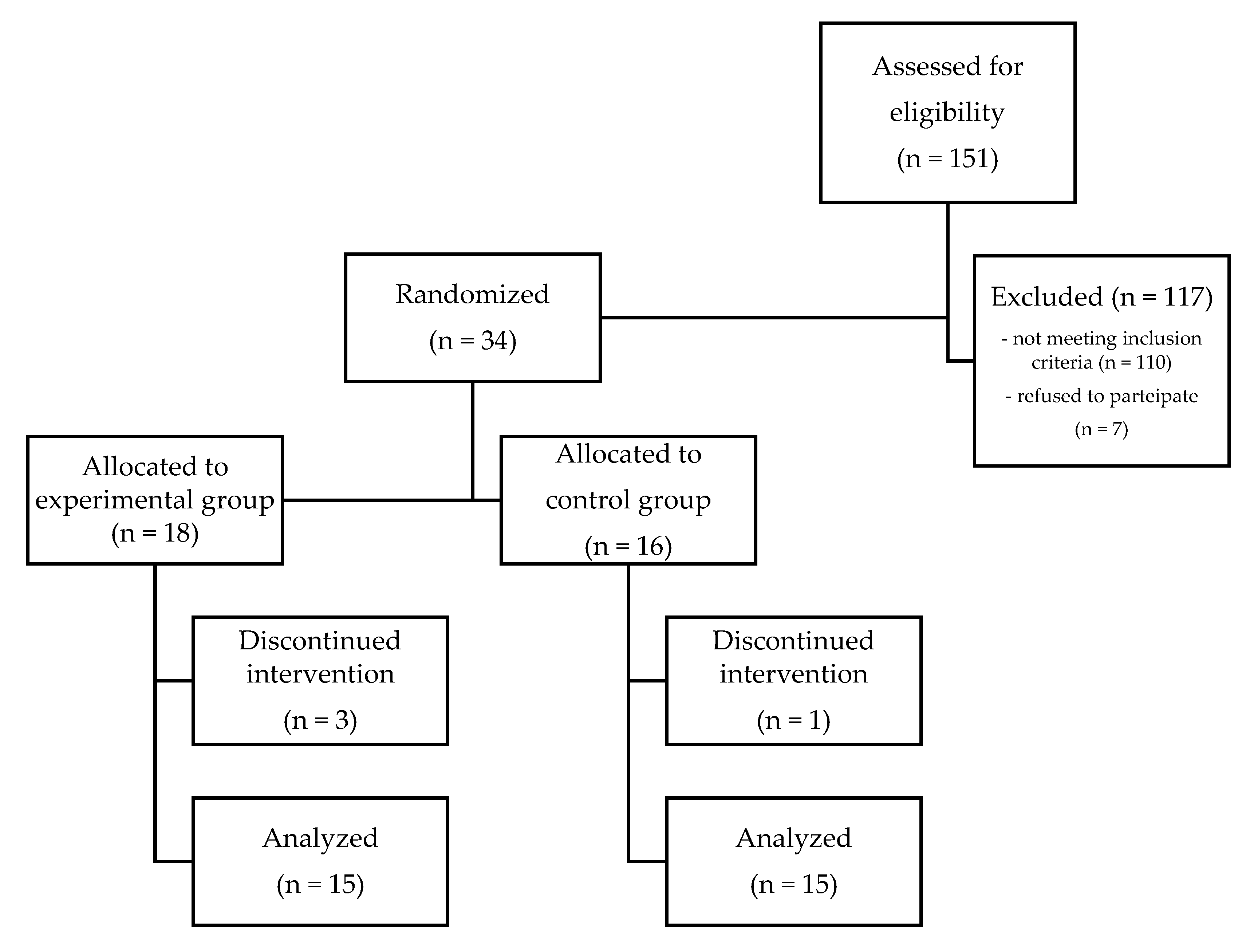
2. Materials and Methods
Statistical Analysis
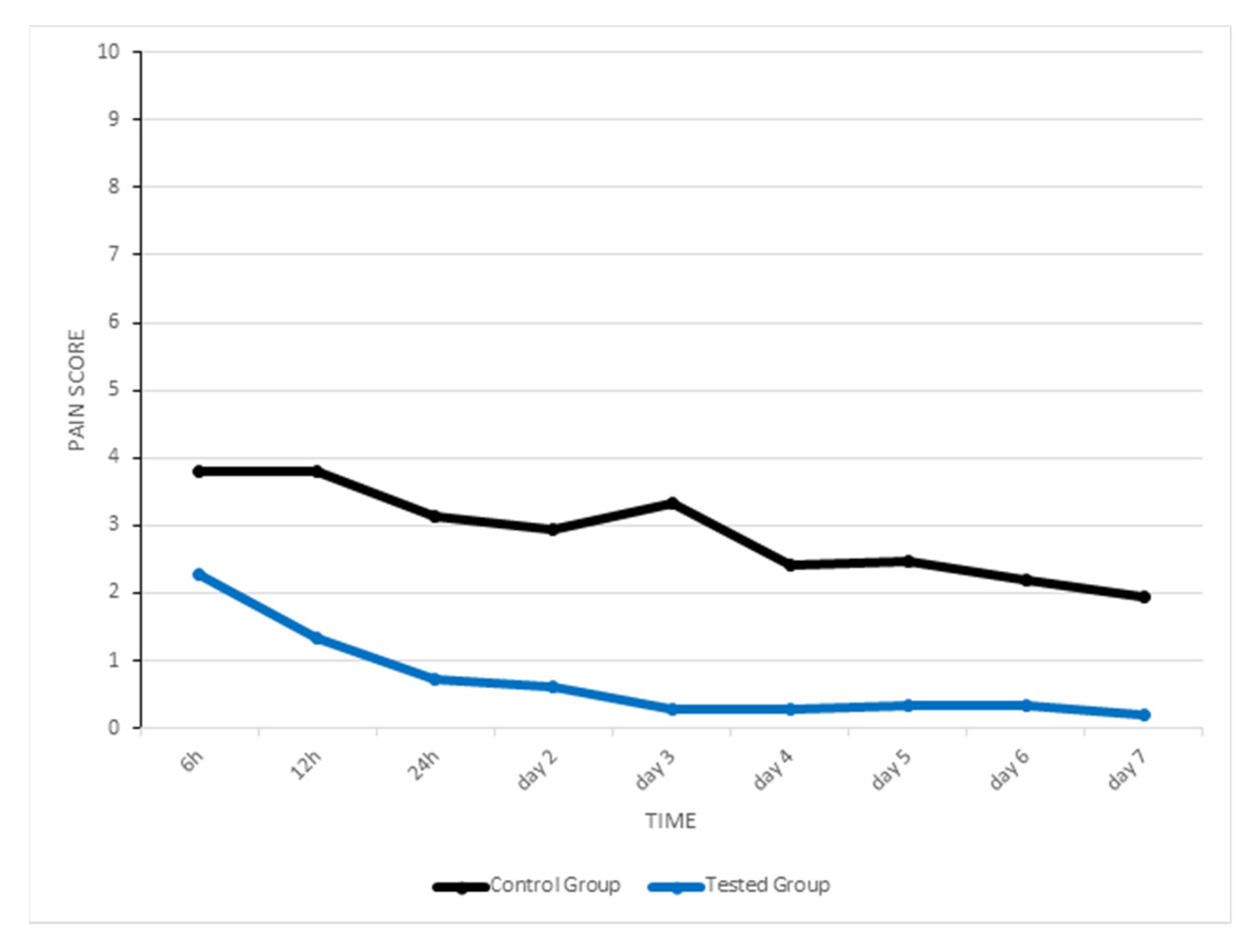
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lo Giudice, A.; Spinuzza, P.; Rustico, L.; Messina, G.; Nucera, R. Short-term treatment effects produced by rapid maxillary expansion evaluated with computer tomography: A systematic review with meta-analysis. Korean J. Orthod. 2020, 50, 314–323. [Google Scholar] [CrossRef]
- Bucci, R.; D’Antò, V.; Rongo, R.; Valletta, R.; Martina, R.; Michelotti, A. Dental and skeletal effects of palatal expansion techniques: A systematic review of the current evidence from systematic reviews and meta-analyses. J. Oral Rehabil. 2016, 43, 543–564. [Google Scholar] [CrossRef] [Green Version]
- Yildirim, M.; Akin, M. Comparison of root resorption after bone-borne and tooth-borne rapid maxillary expansion evaluated with the use of microtomography. Am. J. Orthod. Dentofac. Orthop. 2019, 155, 182–190. [Google Scholar] [CrossRef]
- Lo Giudice, A.; Fastuca, R.; Portelli, M.; Militi, A.; Bellocchio, M.; Spinuzza, P.; Briguglio, F.; Caprioglio, A.; Nucera, R. Effects of rapid vs. slow maxillary expansion on nasal cavity dimensions in growing subjects: A methodological and reproducibility study. Eur. J. Paediatr. Dent. 2017, 18, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Canan, S.; Şenışık, N.E. Comparison of the treatment effects of different rapid maxillary expansion devices on the maxilla and the mandible. Part 1: Evaluation of dentoalveolar changes. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 1125–1138. [Google Scholar] [CrossRef]
- Leonardi, R.; Lo Giudice, A.; Rugeri, M.; Muraglie, S.; Cordasco, G.; Barbato, E. Three-dimensional evaluation on digital casts of maxillary palatal size and morphology in patients with functional posterior crossbite. Eur. J. Orthod. 2018, 40, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Long, H.; Ye, N.; Xue, J.; Yang, X.; Liao, L.; Lai, W. The effectiveness of non-surgical maxillary expansion: A meta-analysis. Eur. J. Orthod. 2014, 36, 233–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo Giudice, A.; Leonardi, R.; Ronsivalle, V.; Allegrini, S.; Lagravère, M.; Marzo, G.; Isola, G. Evaluation of pulp cavity/chamber changes after tooth-borne and bone-borne rapid maxillary expansions: A CBCT study using surface-based superimposition and deviation analysis. Clin. Oral Investig. 2021, 25, 2237–2247. [Google Scholar] [CrossRef]
- Babacan, H.; Doruk, C.; Bicakci, A.A. Pulpal blood flow changes due to rapid maxillary expansion. Angle Orthod. 2010, 80, 1136–1140. [Google Scholar] [CrossRef] [PubMed]
- Lo Giudice, A.; Galletti, C.; Gay-Escoda, C.; Leonardi, R. CBCT assessment of radicular volume loss after rapid maxillary expansion: A systematic review. J. Clin. Exp. Dent. 2018, 10, e484–e494. [Google Scholar] [CrossRef]
- Lo Giudice, A.; Barbato, E.; Cosentino, L.; Ferraro, C.M.; Leonardi, R. Alveolar bone changes after rapid maxillary expansion with tooth-born appliances: A systematic review. Eur. J. Orthod. 2017, 40, 296–303. [Google Scholar] [CrossRef]
- Ghoneima, A.; Abdel-Fattah, E.; Hartsfield, J.; El-Bedwehi, A.; Kamel, A.; Kula, K. Effects of rapid maxillary expansion on the cranial and circummaxillary sutures. Am. J. Orthod. Dentofac. Orthop. 2011, 140, 510–519. [Google Scholar] [CrossRef] [Green Version]
- Lo Giudice, A.; Ronsivalle, V.; Lagravere, M.; Leonardi, R.; Martina, S.; Isola, G. Transverse dentoalveolar response of mandibular arch after rapid maxillary expansion (RME) with tooth-borne and bone-borne appliances: A CBCT retrospective study. Angle Orthod. 2020, 90, 680–687. [Google Scholar] [CrossRef]
- Lo Giudice, A.; Rustico, L.; Ronsivalle, V.; Nicotra, C.; Lagravère, M.; Grippaudo, C. Evaluation of the changes of orbital cavity volume and shape after tooth-borne and bone-borne rapid maxillary expansion (RME). Head Face Med. 2020, 16, 1–10. [Google Scholar] [CrossRef]
- De Felippe, N.L.O.; Da Silveira, A.C.; Viana, G.; Smith, B. Influence of palatal expanders on oral comfort, speech, and mastication. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Joviliano, P.; Junqueira, A.; Stabile, A.; A Leite-Panissi, C.R.; Rocha, M.J. Rapid maxillary expansion causes neuronal activation in brain structures of rats. Brain Res. Bull. 2008, 76, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Sousa, M.V.S.; Pinzan, A.; Consolaro, A.; Henriques, J.F.C.; de Freitas, M.R. Systematic Literature Review: Influence of Low-Level Laser on Orthodontic Movement and Pain Control in Humans. Photomed. Laser Surg. 2014, 32, 592–599. [Google Scholar] [CrossRef]
- Caccianiga, G.; Crestale, C.; Cozzani, M.; Piras, A.; Mutinelli, S.; Lo Giudeice, A.; Cordasco, G. Low-level laser theraphy and invisible aligners. J. Biol. Regul. Homeost. Agents 2016, 30, 107–113. [Google Scholar]
- Mizutani, K.; Musya, Y.; Wakae, K.; Kobayashi, T.; Tobe, M.; Taira, K.; Harada, T. A Clinical Study on Serum Prostaglandin E2 with Low-Level Laser Therapy. Photomed. Laser Surg. 2004, 22, 537–539. [Google Scholar] [CrossRef] [PubMed]
- Bicakci, A.A.; Kocoglu-Altan, B.; Toker, H.; Mutaf, I.; Sumer, Z. Efficiency of Low-Level Laser Therapy in Reducing Pain Induced by Orthodontic Forces. Photomed. Laser Surg. 2012, 30, 460–465. [Google Scholar] [CrossRef]
- Nicotra, C.; Polizzi, A.; Zappalà, G.; Leonida, A.; Indelicato, F.; Caccianiga, G. A Comparative Assessment of Pain Caused by the Placement of Banded Orthodontic Appliances with and without Low-Level Laser Therapy: A Randomized Controlled Prospective Study. Dent. J. 2020, 8, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancini, G.E.; Carinci, F.; Zollino, I.; Avantaggiato, A.; Puglisi, P.; Caccianiga, G.; Brunelli, G. Effectiveness of self-ligating orthodontic treatment. Eur. J. Inflamm. 2011, 9, 53–58. [Google Scholar]
- Caccianiga, G.; Perillo, L.; Portelli, M.; Baldoni, M.; Galletti, C.; Gay-Escoda, C. Evaluation of effectiveness of photobiostimulation in alleviating side effects after dental implant surgery. A randomized clinical trial. Med. Oral Patol. Oral Cir. Bucal. 2020, 25, e277–e282. [Google Scholar] [CrossRef]
- Lo Giudice, A.; Nucera, R.; Perillo, L.; Paiusco, A.; Caccianiga, G. Is low-level laser therapy an effective method to alleviate pain induced by active orthodontic alignment archwire? A randomized clinical trial. J. Evid. Based Dent. Pract. 2019, 19, 71–78. [Google Scholar] [CrossRef]
- Esper, M.; Ângela, L.R.; Nicolau, R.A.; Arisawa, E.; Ângela, L.S. The effect of two phototherapy protocols on pain control in orthodontic procedure—a preliminary clinical study. Lasers Med. Sci. 2011, 26, 657–663. [Google Scholar] [CrossRef]
- Farias, R.D.; Closs, L.Q.; Miguens, S.A.Q. Evaluation of the use of low-level laser therapy in pain control in orthodontic patients: A randomized split-mouth clinical trial. Angle Orthod. 2015, 86, 193–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figueira, I.Z.; Sousa, A.P.C.; Machado, A.W.; Habib, F.A.L.; Soares, L.G.P.; Pinheiro, A.L.B. Clinical study on the efficacy of LED phototherapy for pain control in an orthodontic procedure. Lasers Med. Sci. 2019, 34, 479–485. [Google Scholar] [CrossRef]
- Tortamano, A.; Lenzi, D.C.; Haddad, A.C.; Bottino, M.C.; Dominguez, G.C.; Vigorito, J.W. Low-level laser therapy for pain caused by placement of the first orthodontic archwire: A randomized clinical trial. Am. J. Orthod. Dentofac. Orthop. 2009, 136, 662–667. [Google Scholar] [CrossRef] [PubMed]
- Caccianiga, G.; Rey, G.; Baldoni, M.; Caccianiga, P.; Baldoni, A.; Ceraulo, S. Periodontal Decontamination Induced by Light and Not by Heat: Comparison between Oxygen High Level Laser Therapy (OHLLT) and LANAP. Appl. Sci. 2021, 11, 4629. [Google Scholar] [CrossRef]
- Caccianiga, G.; Rey, G.; Caccianiga, P.; Leonida, A.; Baldoni, M.; Baldoni, A.; Ceraulo, S. Rough Dental Implant Surfaces and Peri-Implantitis: Role of Phase-Contrast Microscopy, Laser Protocols, and Modified Home Oral Hygiene in Maintenance. A 10-Year Retrospective Study. Appl. Sci. 2021, 11, 4985. [Google Scholar] [CrossRef]
- Caccianiga, G.; Rey, G.; Caccianiga, P.; Leonida, A.; Baldoni, M.; Baldoni, A.; Ceraulo, S. Peri-Implantitis Management: Surgical versus Non-Surgical Approach Using Photodynamic Therapy Combined with Hydrogen Peroxide (OHLLT—Oxygen High Level Laser Therapy): A Retrospective Controlled Study. Appl. Sci. 2021, 11, 5073. [Google Scholar] [CrossRef]
- Caccianiga, G.; Rey, G.; Caccianiga, P.; Leonida, A.; Baldoni, M.; Baldoni, A.; Ceraulo, S. Laser Management of Peri-Implantitis: A Comparison between Photodynamic Therapy Combined with Hydrogen Peroxide (OHLLT) and OHLLT + Er:YAG Laser. A Retrospective Controlled Study. Appl. Sci. 2021, 11, 6771. [Google Scholar] [CrossRef]
- Nammour, S.; El Mobadder, M.; Maalouf, E.; Namour, M.; Namour, A.; Rey, G.; Matamba, P.; Matys, J.; Zeinoun, T.; Grzech-Leśniak, K. Clinical Evaluation of Diode (980 nm) Laser-Assisted Nonsurgical Periodontal Pocket Therapy: A Randomized Comparative Clinical Trial and Bacteriological Study. Photobiomodulation Photomed. Laser Surg. 2021, 39, 10–22. [Google Scholar] [CrossRef]
- Caccianiga, G.; Cambini, A.; Donzelli, E.; Baldoni, M.; Rey, G.; Paiusco, A. Effects of laser biostimulation on the epithelial tissue for keratinized layer differentiation: An in vitro study. J. Boil. Regul. Homeost. Agents 2016, 30, 27469555. [Google Scholar]
- Caccianiga, G.; Rey, G.; Baldoni, M.; Paiusco, A. Clinical, Radiographic and Microbiological Evaluation of High Level Laser Therapy, a New Photodynamic Therapy Protocol, in Peri-Implantitis Treatment; a Pilot Experience. BioMed Res. Int. 2016, 2016, 6321906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turhani, D.; Scheriau, M.; Kapral, D.; Benesch, T.; Jonke, E.; Bantleon, H.P. Pain relief by single low-level laser irradiation in orthodontic patients undergoing fixed appliance therapy. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 371–377. [Google Scholar] [CrossRef]
- Deana, N.F.; Zaror, C.; Sandoval, P.; Alves, N. Effectiveness of Low-Level Laser Therapy in Reducing Orthodontic Pain: A Systematic Review and Meta-Analysis. Pain Res. Manag. 2017, 2017, 8560652. [Google Scholar] [CrossRef]
- Mancini, G.; Carinci, F.; Zollino, I.; Avantaggiato, A.; Puglisi, P.; Caccianiga, G.; Brunelli, G. Simplicity Et Reliability of Invisalign System. Eur. J. Inflamm. 2011, 9, 43–47. [Google Scholar]
- Mingardi, M.; Fumagalli, T.; Cambini, A.; Giacomello, M.; Caccianiga, G. Management Missing Later Incisor in Monozygotic Twins: Two Case Reports. Eur. J. Inflamm. 2012, 10, 61–64. [Google Scholar] [CrossRef] [Green Version]
- Caccianiga, G.; Stanizzi, A.; Zorzella, P.; Crestale, C.; Denotti, D.; Squarzoni, N. Laser Biostimulation and Self Ligating Appliances in Orthodontics: Periodontal Remodeling. Eur. J. Inflamm. 2012, 10, 55–59. [Google Scholar] [CrossRef]
- Caccianiga, G.; Giudice, A.L.; Longoni, S.; Ceraulo, S.; Baldoni, M.; Leonida, A. Low-level laser therapy protocols in dental movement acceleration and in pain management during orthodontic treatment. J. Biol. Regul. Homeost. Agents 2019, 33, 59–68. [Google Scholar]
- Farrar, J.T.; Young, J.P., Jr.; LaMoreaux, L.; Werth, J.L.; Poole, R.M. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 2001, 94, 149–158. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Sample Characteristics | Total Sample | EG (n = 15) | CG (n = 15) | Significance |
|---|---|---|---|---|
| Gender: male/female | 14/16 | 7/8 | 7/8 | NS |
| Age, y, mean (SD) | 7.8 (1.2) | 7.6 (1.1) | 8 (1.2) | NS |
| Time Schedule | Median CG (min-max) IC 95% | Median EG (min-max) IC 95% | Significance |
|---|---|---|---|
| 6 h | 4 (1–7), IC 95%: 2.75–4.85 | 2 (1–4), IC 95%: 1.73–2.80 | <0.05 |
| 12 h | 3 (2–7), IC 95%: 2.93–4.67 | 1 (0–3), IC 95%: 0.84–1.83 | <0.001 |
| 24 h | 3 (1–6), IC 95%: 2.30–3.97 | 1 (0–2), IC 95%: 0.29–1.18 | <0.001 |
| 2 d | 3 (0–5), IC 95%: 2.03–3.83 | 0 (0–2), IC 95%: 0.19–1.01 | <0.001 |
| 3 d | 4 (1–7), IC 95%: 2.45–4.21 | 0 (0–1), IC 95%: 0.01–0.52 | <0.001 |
| 4 d | 2 (0–5), IC 95%: 1.68–3.12 | 0 (0–1), IC 95%: 0.01–0.52 | <0.001 |
| 5 d | 3 (0–6), IC 95%: 1.53–3.40 | 0 (0–1), IC 95%: 0.06–0.60 | <0.001 |
| 6 d | 2 (0–6), IC 95%: 1.24–3.16 | 0 (0–1), IC 95%: 0.06–0.60 | <0.05 |
| 7 d | 1 (0–6), IC 95%: 0.88–2.99 | 0 (0–1), IC 95%: 0.03–043 | <0.05 |
| Dependent Variable | Predictor Variable | R | R-Square | Standard Error | Significance |
|---|---|---|---|---|---|
| Pain CG | Time | 0.933 | 0.852 | 0.262 | p < 0.001 |
| Pain TG | Time | 0.750 | 0.563 | 0.485 | p < 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caccianiga, G.; Caccianiga, P.; Baldoni, M.; Lo Giudice, A.; Perillo, L.; Moretti, N.; Ceraulo, S. Pain Reduction during Rapid Palatal Expansion Due to LED Photobiomodulation Irradiation: A Randomized Clinical Trial. Life 2022, 12, 37. https://doi.org/10.3390/life12010037
Caccianiga G, Caccianiga P, Baldoni M, Lo Giudice A, Perillo L, Moretti N, Ceraulo S. Pain Reduction during Rapid Palatal Expansion Due to LED Photobiomodulation Irradiation: A Randomized Clinical Trial. Life. 2022; 12(1):37. https://doi.org/10.3390/life12010037
Chicago/Turabian StyleCaccianiga, Gianluigi, Paolo Caccianiga, Marco Baldoni, Antonino Lo Giudice, Letizia Perillo, Nicolò Moretti, and Saverio Ceraulo. 2022. "Pain Reduction during Rapid Palatal Expansion Due to LED Photobiomodulation Irradiation: A Randomized Clinical Trial" Life 12, no. 1: 37. https://doi.org/10.3390/life12010037