
Investigation of the Expression of Inflammatory Markers in Oral Biofilm Samples in Patients with Systemic Scleroderma and the Association with Clinical Periodontal Parameters—A Preliminary Study

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setup
- Smoking;
- Diabetes type I and II;
- Already diagnosed periodontitis or already undergone periodontitis treatment;
- Poor general health that does not permit a detailed dental examination;
- Toothlessness;
- Prior antibiotic treatment (neither systemic nor local administration for at least 4 weeks).
2.2. Data Extraction and Examination
2.3. Clinical Examination
- Bleeding on probing (BOP) in %
- Mombelli Plaque Index (mPI) graded from 0–3 (grade 0: no plaque detected by inspection and probing; grade 1: accumulation of plaque visible only by probing in the sulcus with a probe but not by eye; grade 2: visible plaque accumulation; grade 3: massive plaque accumulation)
- CAL in mm/% (distance from the cementoenamel junction to the bottom of the pocket/sulcus)
- PD -pocket depth at 6 sites using a PCP-12 probe (Hu-Friedy, Chicago, IL, USA) in %
- DMFT index
- Gingival recessions in mm/%
- Mouth opening in mm (maximum direction between the incisors of the lower and upper jaw); microstomia was defined at a value < 40 mm [22]
- Number of cervical tooth defects
- -
- 0 = normal skin; no folds; no fibrosis
- -
- 1 = mild fibrosis of the skin; fold is formed easily, fine folds are accepted
- -
- 2 = moderate fibrosis of the skin; no fine folds
- -
- 3 = severe fibrosis of the skin; no possibility to form folds
2.4. Examination of the Parameters in the Laboratory
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. Clinical Parameters
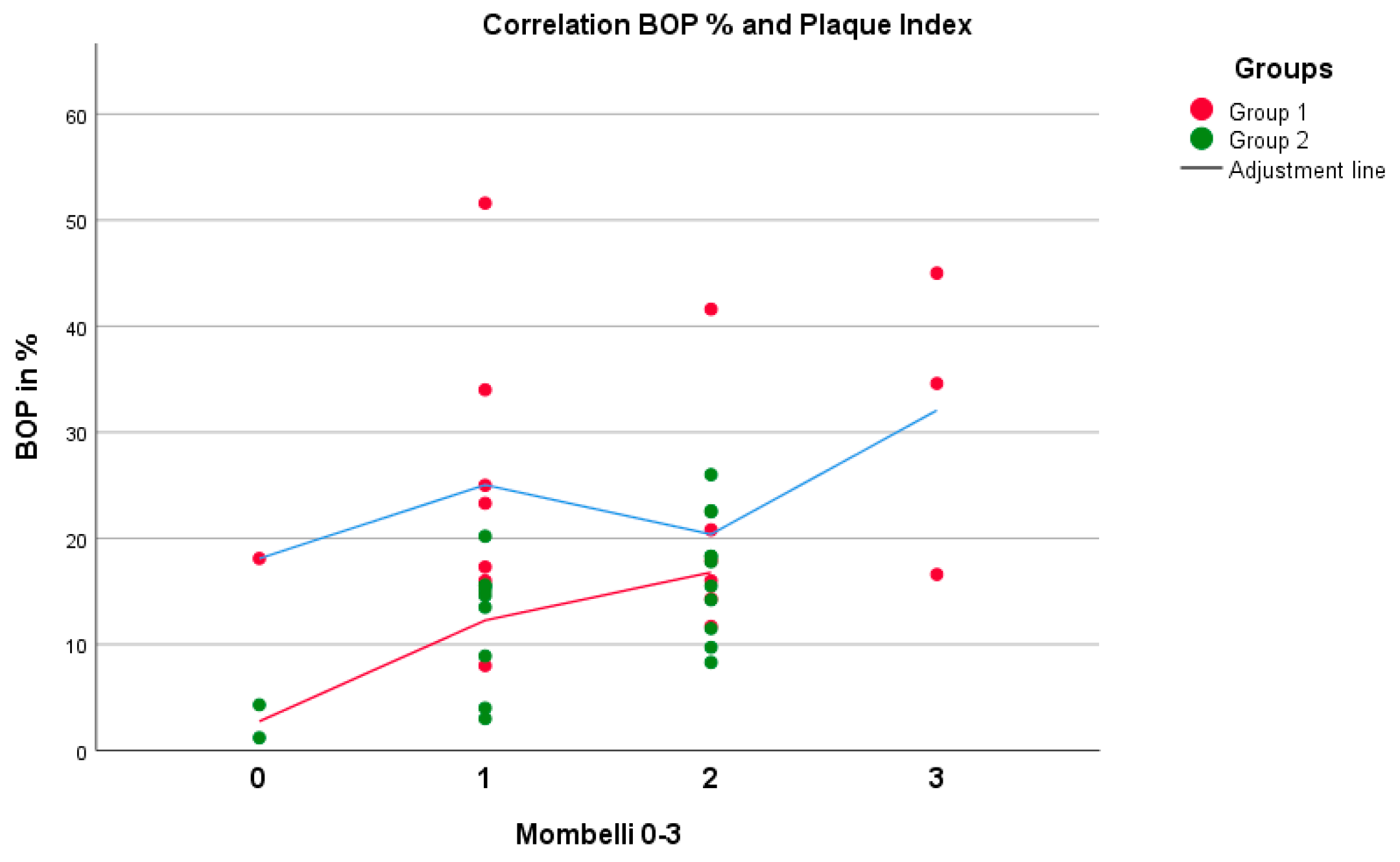
3.2.1. Bleeding on Probing (BOP) and Mombelli Plaque Index (mPI)
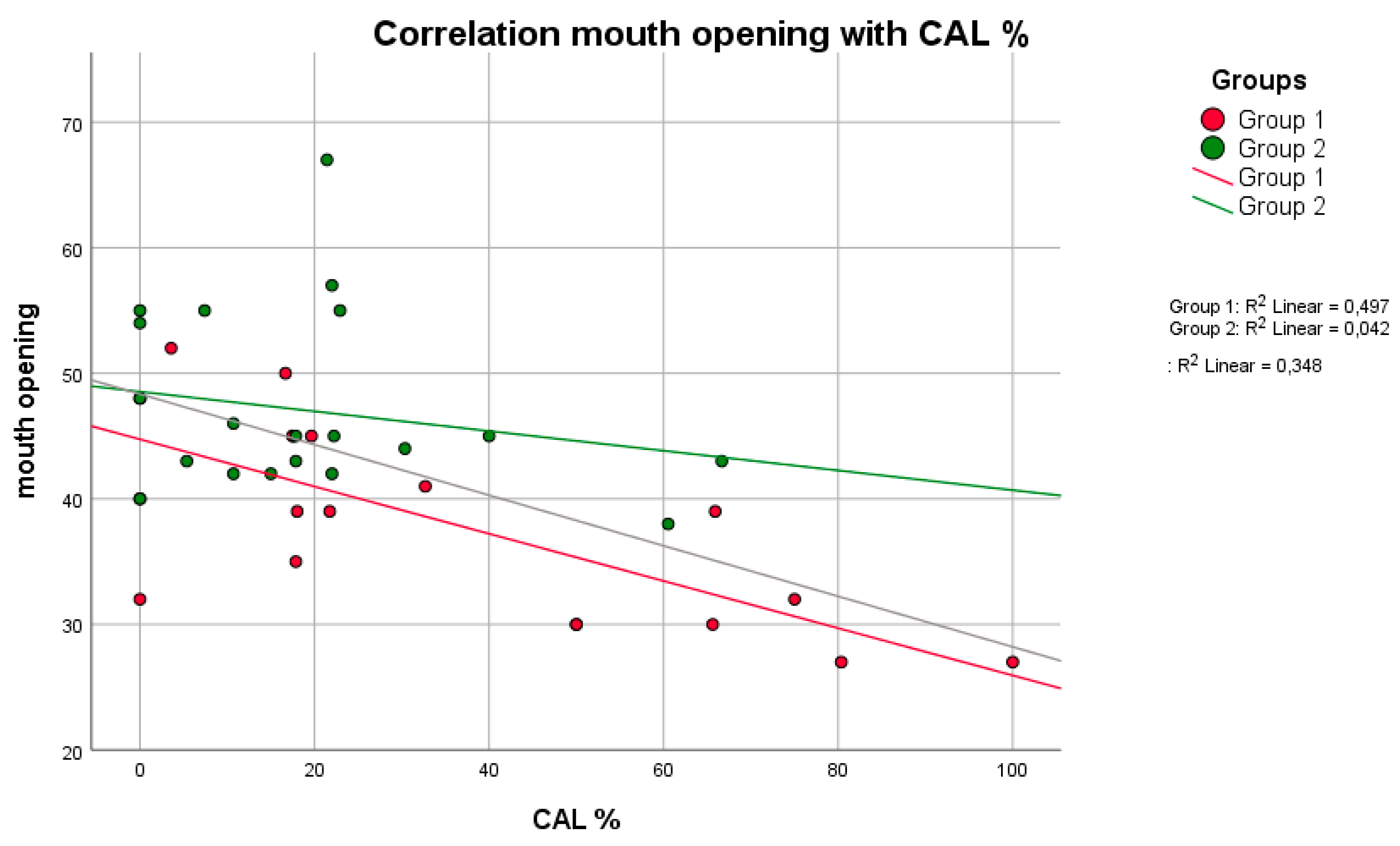
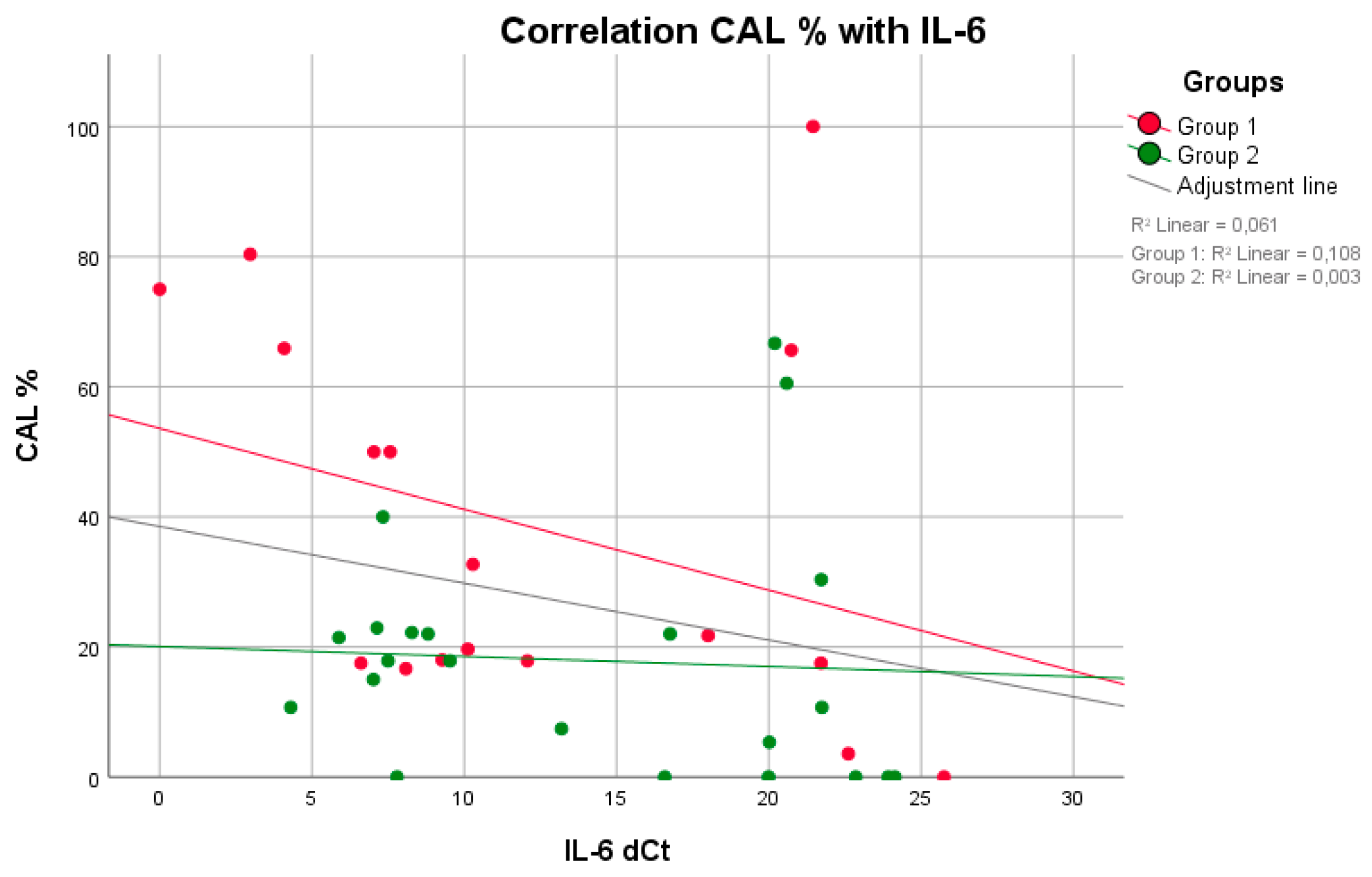
3.2.2. Clinical Attachment Loss (CAL)
3.2.3. DMFT Index and PD
3.2.4. Gingival Recession
3.2.5. Mouth Opening
3.2.6. Cervical Tooth Defects
3.2.7. Cervical Extern Resorptions/Radiological Findings
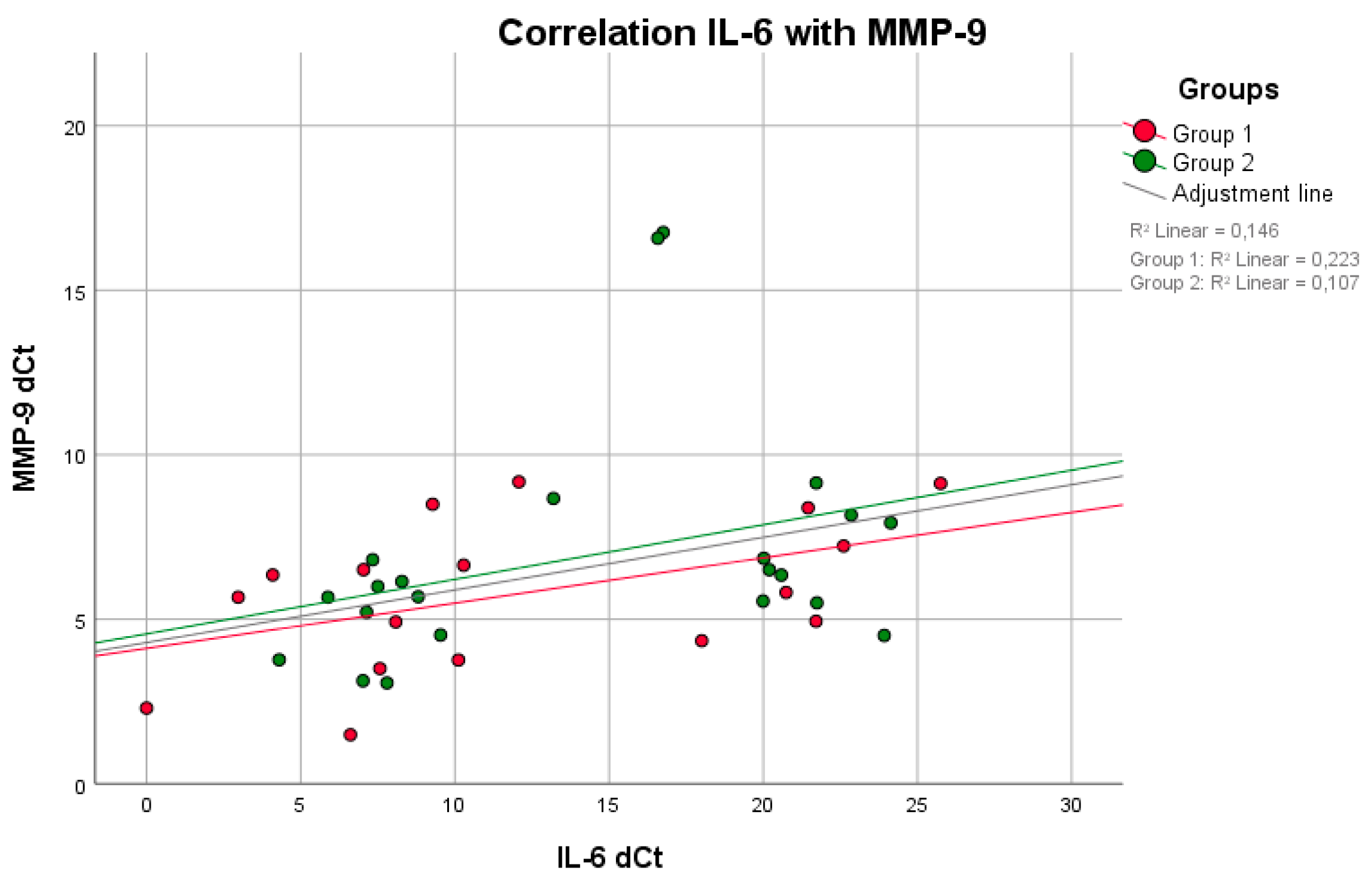
3.3. Cytokine Expressions
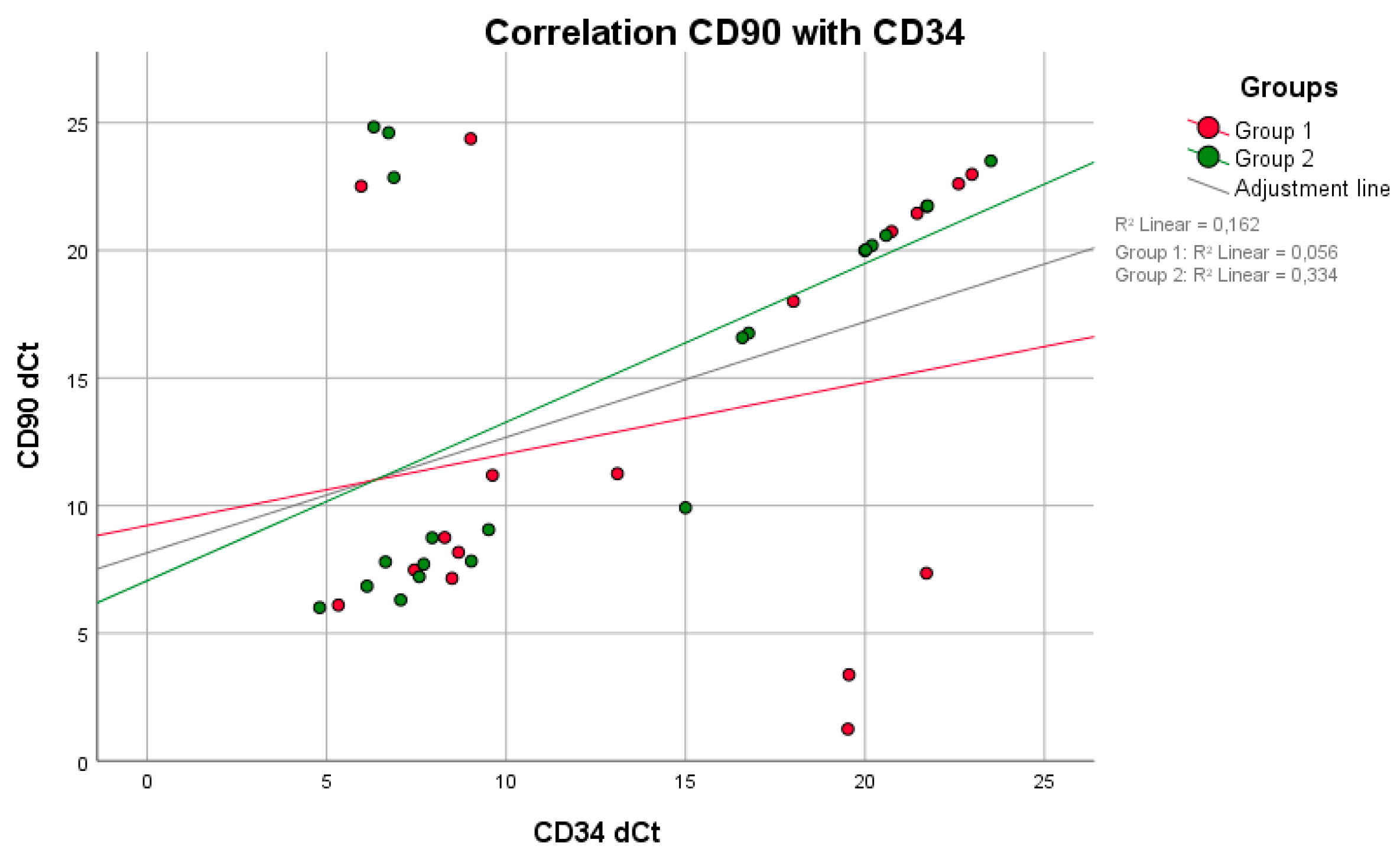
Correlation between Clinical and/or Laboratory Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alhendi, F.J.; Werth, V.P.; Sollecito, T.P.; Stoopler, E.T. Systemic Sclerosis: Update for Oral Health Care Providers. Spec. Care Dentist. 2020, 40, 418–430. [Google Scholar] [CrossRef]
- Bossini-Castillo, L.; Lopez-Isac, E.; Mayes, M.D.; Martin, J. Genetics of Systemic Sclerosis. Semin. Immunopathol. 2015, 37, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Sticherling, M. Systemic Sclerosis-Dermatological Aspects. Part 1: Pathogenesis, Epidemiology, Clinical Findings. J. Dtsch. Dermatol. Ges. 2012, 10, 705–718. [Google Scholar] [CrossRef] [Green Version]
- Ranque, B.; Mouthon, L. Geoepidemiology of Systemic Sclerosis. Autoimmun. Rev. 2010, 9, A311–A318. [Google Scholar] [CrossRef] [PubMed]
- Nihtyanova, S.I.; Tang, E.C.; Coghlan, J.G.; Wells, A.U.; Black, C.M.; Denton, C.P. Improved Survival in Systemic Sclerosis Is Associated with Better Ascertainment of Internal Organ Disease: A Retrospective Cohort Study. QJM Int. J. Med. 2010, 103, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Almeida, C.; Almeida, I.; Vasconcelos, C. Quality of Life in Systemic Sclerosis. Autoimmun. Rev. 2015, 14, 1087–1096. [Google Scholar] [CrossRef]
- Jordan, S.; Maurer, B.; Toniolo, M.; Michel, B.; Distler, O. Performance of the New Acr/Eular Classification Criteria for Systemic Sclerosis in Clinical Practice. Rheumatology 2015, 54, 1454–1458. [Google Scholar] [CrossRef] [Green Version]
- Matarese, G.; Isola, G.; Anastasi, G.P.; Favaloro, A.; Milardi, D.; Vermiglio, G.; Vita, G.; Cordasco, G.; Cutroneo, G. Immunohistochemical Analysis of Tgf-Beta1 and Vegf in Gingival and Periodontal Tissues: A Role of These Biomarkers in the Pathogenesis of Scleroderma and Periodontal Disease. Int. J. Mol. Med. 2012, 30, 502–508. [Google Scholar] [CrossRef] [Green Version]
- Balbir-Gurman, A.; Braun-Moscovici, Y. Scleroderma-New Aspects in Pathogenesis and Treatment. Best Pract. Res. Clin. Rheumatol. 2012, 26, 13–24. [Google Scholar] [CrossRef]
- Dantas, A.T.; Almeida, A.R.; Sampaio, M.; Cordeiro, M.F.; Oliveira, P.S.S.; Mariz, H.A.; Pereira, M.C.; Rego, M.; Pitta, I.D.R.; Duarte, A.; et al. Different Profile of Cytokine Production in Patients with Systemic Sclerosis and Association with Clinical Manifestations. Immunol. Lett. 2018, 198, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Desallais, L.; Avouac, J.; Frechet, M.; Elhai, M.; Ratsimandresy, R.; Montes, M.; Mouhsine, H.; Do, H.; Zagury, J.F.; Allanore, Y. Targeting Il-6 by Both Passive or Active Immunization Strategies Prevents Bleomycin-Induced Skin Fibrosis. Arthritis Res. Ther. 2014, 16, R157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, K.; Xu, S.; Nihtyanova, S.; Derrett-Smith, E.; Abraham, D.; Denton, C.P.; Ong, V.H. Clinical and Pathological Significance of Interleukin 6 Overexpression in Systemic Sclerosis. Ann. Rheum. Dis. 2012, 71, 1235–1242. [Google Scholar] [CrossRef] [PubMed]
- Hax, V.; Gasparin, A.A.; Schneider, L.; Monticielo, O.A.; Soares, H.M.F.; Streit, M.D.A.; Pfaffenseller, B.; Xavier, R.M.; Chakr, R. Vitamin D and Cytokine Profiles in Patients with Systemic Sclerosis. J. Clin. Rheumatol. 2020, 26, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Hajishengallis, G. Periodontitis: From Microbial Immune Subversion to Systemic Inflammation. Nat. Rev. Immunol. 2015, 15, 30–44. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Rivas, M.; Royo, C.; Simeon, C.P.; Corbella, X.; Fonollosa, V. Mortality and Survival in Systemic Sclerosis: Systematic Review and Meta-Analysis. Semin. Arthritis Rheum. 2014, 44, 208–219. [Google Scholar] [CrossRef] [PubMed]
- Smirani, R.; Truchetet, M.E.; Poursac, N.; Naveau, A.; Schaeverbeke, T.; Devillard, R. Impact of Systemic Sclerosis Oral Manifestations on Patients’ Health-Related Quality of Life: A Systematic Review. J. Oral Pathol. Med. 2018, 47, 808–815. [Google Scholar] [CrossRef] [PubMed]
- Elimelech, R.; Mayer, Y.; Braun-Moscovici, Y.; Machtei, E.E.; Balbir-Gurman, A. Periodontal Conditions and Tumor Necrosis Factor-Alpha Level in Gingival Crevicular Fluid of Scleroderma Patients. Isr. Med. Assoc. J. 2015, 17, 549–553. [Google Scholar]
- Eley, B.M.; Cox, S.W. Proteolytic and Hydrolytic Enzymes from Putative Periodontal Pathogens: Characterization, Molecular Genetics, Effects on Host Defenses and Tissues and Detection in Gingival Crevice Fluid. Periodontology 2003, 31, 105–124. [Google Scholar] [CrossRef]
- Subbarao, K.C.; Nattuthurai, G.S.; Sundararajan, S.K.; Sujith, I.; Joseph, J.; Syedshah, Y.P. Gingival Crevicular Fluid: An Overview. J. Pharm. Bioallied Sci. 2019, 11, S135–S139. [Google Scholar] [CrossRef]
- Zijnge, V.; van Leeuwen, M.B.; Degener, J.E.; Abbas, F.; Thurnheer, T.; Gmur, R.; Harmsen, H.J. Oral Biofilm Architecture on Natural Teeth. PLoS ONE 2010, 5, e9321. [Google Scholar] [CrossRef] [Green Version]
- Buchbender, M.; Fehlhofer, J.; Proff, P.; Most, T.; Ries, J.; Hannig, M.; Neurath, M.F.; Gund, M.; Atreya, R.; Kesting, M. Expression of Inflammatory Mediators in Biofilm Samples and Clinical Association in Inflammatory Bowel Disease Patients-a Preliminary Study. Clin. Oral Investig. 2021. open access. [Google Scholar] [CrossRef] [PubMed]
- Aliko, A.; Ciancaglini, R.; Alushi, A.; Tafaj, A.; Ruci, D. Temporomandibular Joint Involvement in Rheumatoid Arthritis, Systemic Lupus Erythematosus and Systemic Sclerosis. Int. J. Oral Maxillofac. Surg. 2011, 40, 704–709. [Google Scholar] [CrossRef]
- Khanna, D.; Furst, D.E.; Clements, P.J.; Allanore, Y.; Baron, M.; Czirjak, L.; Distler, O.; Foeldvari, I.; Kuwana, M.; Matucci-Cerinic, M.; et al. Standardization of the Modified Rodnan Skin Score for Use in Clinical Trials of Systemic Sclerosis. J. Scleroderma Relat. Disord. 2017, 2, 11–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cieplik, F.; Zaura, E.; Brandt, B.W.; Buijs, M.J.; Buchalla, W.; Crielaard, W.; Laine, M.L.; Deng, D.M.; Exterkate, R.A.M. Microcosm Biofilms Cultured from Different Oral Niches in Periodontitis Patients. J. Oral Microbiol. 2019, 11, 1551596. [Google Scholar] [CrossRef]
- Detert, J.; Pischon, N.; Burmester, G.R.; Buttgereit, F. Pathogenesis of Parodontitis in Rheumatic Diseases. Z. Fur. Rheumatol. 2010, 69, 109–112. [Google Scholar] [CrossRef]
- Isola, G.; Williams, R.C.; Gullo, A.L.; Ramaglia, L.; Matarese, M.; Iorio-Siciliano, V.; Cosio, C.; Matarese, G. Risk Association between Scleroderma Disease Characteristics, Periodontitis, and Tooth Loss. Clin. Rheumatol. 2017, 36, 2733–2741. [Google Scholar] [CrossRef] [PubMed]
- Parat, K.; Radic, M.; Perkovic, D.; Lukenda, D.B.; Kaliterna, D.M. Reduced Salivary Flow and Caries Status Are Correlated with Disease Activity and Severity in Patients with Diffuse Cutaneous Systemic Sclerosis. J. Int. Med. Res. 2020, 48, 300060520941375. [Google Scholar] [CrossRef]
- Pischon, N.; Hoedke, D.; Kurth, S.; Lee, P.; Dommisch, H.; Steinbrecher, A.; Pischon, T.; Burmester, G.R.; Buttgereit, F.; Detert, J.; et al. Increased Periodontal Attachment Loss in Patients with Systemic Sclerosis. J. Periodontol. 2016, 87, 763–771. [Google Scholar] [CrossRef] [Green Version]
- Leung, W.K.; Chu, C.H.; Mok, M.Y.; Yeung, K.W.; Ng, S.K. Periodontal Status of Adults with Systemic Sclerosis: Case-Control Study. J. Periodontol. 2011, 82, 1097–1219. [Google Scholar] [CrossRef]
- Miranda, T.S.; Figueiredo, N.F.; Figueiredo, L.C.; Silva, H.; Rocha, F.R.G.; Duarte, P.M. Cytokine Profiles of Healthy and Diseased Sites in Individuals with Periodontitis. Arch. Oral Biol. 2020, 120, 104957. [Google Scholar] [CrossRef]
- Miranda, T.S.; Heluy, S.L.; Cruz, D.F.; da Silva, H.D.P.; Feres, M.; Figueiredo, L.C.; Duarte, P.M. The Ratios of Pro-Inflammatory to Anti-Inflammatory Cytokines in the Serum of Chronic Periodontitis Patients with and without Type 2 Diabetes and/or Smoking Habit. Clin. Oral Investig. 2019, 23, 641–650. [Google Scholar] [CrossRef] [PubMed]
- Bunaes, D.F.; Mustafa, M.; Mohamed, H.G.; Lie, S.A.; Leknes, K.N. The Effect of Smoking on Inflammatory and Bone Remodeling Markers in Gingival Crevicular Fluid and Subgingival Microbiota Following Periodontal Therapy. J. Periodontal. Res. 2017, 52, 713–724. [Google Scholar] [CrossRef] [PubMed]
- Kawamoto, D.; Amado, P.P.L.; Albuquerque-Souza, E.; Bueno, M.R.; Vale, G.C.; Saraiva, L.; Mayer, M.P.A. Chemokines and Cytokines Profile in Whole Saliva of Patients with Periodontitis. Cytokine 2020, 135, 155197. [Google Scholar] [CrossRef] [PubMed]
- Ebersole, J.L.; Kirakodu, S.; Novak, M.J.; Stromberg, A.J.; Shen, S.; Orraca, L.; Gonzalez-Martinez, J.; Burgos, A.; Gonzalez, O.A. Cytokine Gene Expression Profiles During Initiation, Progression and Resolution of Periodontitis. J. Clin. Periodontol. 2014, 41, 853–861. [Google Scholar] [CrossRef] [PubMed]
- Denton, C.P.; Ong, V.H.; Xu, S.; Chen-Harris, H.; Modrusan, Z.; Lafyatis, R.; Khanna, D.; Jahreis, A.; Siegel, J.; Sornasse, T. Therapeutic Interleukin-6 Blockade Reverses Transforming Growth Factor-Beta Pathway Activation in Dermal Fibroblasts: Insights from the Fasscinate Clinical Trial in Systemic Sclerosis. Ann. Rheum. Dis. 2018, 77, 1362–1371. [Google Scholar] [CrossRef]
- Meng, C.; Chen, X.; Li, J.; Wu, Y.; Liu, H. Expression of Mmp-9 and Timp-1 in Lesions of Systemic Sclerosis and Its Implications. J. Huazhong Univ. Sci. Technolog. Med. Sci. 2008, 28, 480–482. [Google Scholar] [CrossRef] [PubMed]
- Giannelli, G.; Iannone, F.; Marinosci, F.; Lapadula, G.; Antonaci, S. The Effect of Bosentan on Matrix Metalloproteinase-9 Levels in Patients with Systemic Sclerosis-Induced Pulmonary Hypertension. Curr. Med. Res. Opin. 2005, 21, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, K.; Kubo, M.; Hoashi, T.; Tamaki, K. Decreased Mmp-9 Activity in the Serum of Patients with Diffuse Cutaneous Systemic Sclerosis. Clin. Exp. Dermatol. 2002, 27, 301–305. [Google Scholar] [CrossRef]
- Kim, H.D.; Kim, S.; Jeon, S.; Kim, S.J.; Cho, H.J.; Choi, Y.N. Diagnostic and Prognostic Ability of Salivary Mmp-9 and S100a8 for Periodontitis. J. Clin. Periodontol. 2020, 47, 1191–1200. [Google Scholar] [CrossRef]
- Seguier, S.; Gogly, B.; Bodineau, A.; Godeau, G.; Brousse, N. Is Collagen Breakdown During Periodontitis Linked to Inflammatory Cells and Expression of Matrix Metalloproteinases and Tissue Inhibitors of Metalloproteinases in Human Gingival Tissue? J. Periodontol. 2001, 72, 1398–1406. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Gu, B.; Zhao, L.; Shi, Q.; Xu, J.; Wen, N. Meta-Analysis of the Association between Serum and Gingival Crevicular Fluid Matrix Metalloproteinase-9 and Periodontitis. J. Am. Dent. Assoc. 2019, 150, 34–41. [Google Scholar] [CrossRef] [PubMed]
- da Silva, K.D.; Coelho, L.V.; Couto, A.M.d.; de Aguiar, M.C.F.; Tarquinio, S.B.C.; Gomes, A.P.N.; Mendonca, E.F.; Batista, A.C.; Nonaka, C.F.W.; de Sena, L.S.B.; et al. Clinicopathological and Immunohistochemical Features of the Oral Lymphoepithelial Cyst: A Multicenter Study. J. Oral Pathol. Med. 2020, 49, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Park, H.S.; Yoon, H.S.; Chung, J.H.; Cho, S. Cd34 Stromal Expression Is Inversely Proportional to Smooth Muscle Actin Expression and Extent of Morphea. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 2208–2216. [Google Scholar] [CrossRef]
- Nazari, B.; Rice, L.M.; Stifano, G.; Barron, A.M.; Wang, Y.M.; Korndorf, T.; Lee, J.; Bhawan, J.; Lafyatis, R.; Browning, J.L. Altered Dermal Fibroblasts in Systemic Sclerosis Display Podoplanin and Cd90. Am. J. Pathol. 2016, 186, 2650–2664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, Y.Y.; Lagares, D.; Tager, A.M.; Kapoor, M. Fibrosis--a Lethal Component of Systemic Sclerosis. Nat. Rev. Rheumatol. 2014, 10, 390–402. [Google Scholar] [CrossRef] [PubMed]
- Goncalves, P.G.P.; Lourenco, S.I.M.; de Vasconcelos Gurgel, B.C. Immunohistochemical Study of Cd34 and Podoplanin in Periodontal Disease. J. Periodontal Res. 2019, 54, 349–355. [Google Scholar] [CrossRef]
- Sato, S.; Hasegawa, M.; Takehara, K. Serum Levels of Interleukin-6 and Interleukin-10 Correlate with Total Skin Thickness Score in Patients with Systemic Sclerosis. J. Dermatol. Sci. 2001, 27, 140–146. [Google Scholar] [CrossRef]
- Arroyo-Bote, S.; Bucchi, C.; Manzanares, M.C. External Cervical Resorption: A New Oral Manifestation of Systemic Sclerosis. J. Endod. 2017, 43, 1740–1743. [Google Scholar] [CrossRef] [PubMed]
- Baron, M.; Hudson, M.; Dagenais, M.; Macdonald, D.; Gyger, G.; el Sayegh, T.; Pope, J.; Fontaine, A.; Masetto, A.; Matthews, D.; et al. Relationship between Disease Characteristics and Oral Radiologic Findings in Systemic Sclerosis: Results from a Canadian Oral Health Study. Arthritis Care Res. 2016, 68, 673–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Parameter | lcSSc (n = 11) | dcSSc (n = 6) |
|---|---|---|
| Raynaud Syndrome | 10 | 6 |
| Sicca Symptomatic | 6 | 5 |
| Xerostomia | 3 | 3 |
| Esophageal motility disorder | 8 | 6 |
| Restricted lung function | 5 | 5 |
| Digital ulcers | 2 | 3 |
| Sklerodaktyy | 7 | 3 |
| mRSS (Ø) | 4.9 | 11.6 |
| Group 1 (n = 17) (SD) | Group 2 (n = 22) (SD) | p-Value | RQ | |
|---|---|---|---|---|
| CT IL-2 | 23.00 (2.43) | 21.98 (4.76) | 0.679 | 0.49# |
| CT IL-6 | 13.02 (7.42) | 14.33 (6.99) | 0.479 | 2.48# |
| CT IL-10 | 10.81 (7.22) | 11.29 (6.11) | 0.590 | 1.40 |
| CT MMP9 | 5.80 (2.28) | 6.93 (3.54) | 0.590 | 2.19# |
| CT CD90 | 13.22 (7.86) | 15.03 (7.13) | 0.552 | 3.52# |
| CT CD34 | 14.26 (6.66) | 12.83 (6.62) | 0.396 | 0.37# |
| CT CD11a | 6.11 (4.34) | 9.12 (6.68) | 0.193 | 8.07# |
| BOP (in %) | 24.22 (12.59) | 13.66 (6.72) | 0.006 * | - |
| mPI (grade 0–3) | 1.65 (0.86) | 1.41 (0.66) | 0.451 | |
| CAL (%) | 38.35 (29.78) | 17.86 (18.55) | 0.035 * | - |
| CAL Ø (mm) | 1.95 (1.73) | 0.76 (0.95) | 0.009 * | - |
| PD ≥ 4 mm (%) | 14.83 (9.24) | 11.58 (8.99) | 0.178 | - |
| DMFT | 20.53 (5.23) | 18.00 (6.36) | 0.150 | - |
| Gingival recession (%) | 38.14 (29.71) | 16.90 (18.11) | 0.020 * | - |
| Gingival recession Ø (mm) | 1.14 (1.10) | 0.43 (0.56) | 0.020 * | - |
| Maximum mouth opening (mm) | 37.53 (7.95) | 47.14 (7.12) | 0.001 * | - |
| Cervical tooth defects (n) | 5.82 (5.11) | 2.36 (2.64) | 0.011 * | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buchbender, M.; Lugenbühl, A.; Fehlhofer, J.; Kirschneck, C.; Ries, J.; Lutz, R.; Sticherling, M.; Kesting, M.R. Investigation of the Expression of Inflammatory Markers in Oral Biofilm Samples in Patients with Systemic Scleroderma and the Association with Clinical Periodontal Parameters—A Preliminary Study. Life 2021, 11, 1145. https://doi.org/10.3390/life11111145
Buchbender M, Lugenbühl A, Fehlhofer J, Kirschneck C, Ries J, Lutz R, Sticherling M, Kesting MR. Investigation of the Expression of Inflammatory Markers in Oral Biofilm Samples in Patients with Systemic Scleroderma and the Association with Clinical Periodontal Parameters—A Preliminary Study. Life. 2021; 11(11):1145. https://doi.org/10.3390/life11111145
Chicago/Turabian StyleBuchbender, Mayte, Amelie Lugenbühl, Jakob Fehlhofer, Christian Kirschneck, Jutta Ries, Rainer Lutz, Michael Sticherling, and Marco Rainer Kesting. 2021. "Investigation of the Expression of Inflammatory Markers in Oral Biofilm Samples in Patients with Systemic Scleroderma and the Association with Clinical Periodontal Parameters—A Preliminary Study" Life 11, no. 11: 1145. https://doi.org/10.3390/life11111145