Efficacy of Applying Hyaluronic Acid Gels in the Primary Prevention of Intrauterine Adhesion after Hysteroscopic Myomectomy: A Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Study Selection
2.2. Procedures
2.3. Statistical Analysis and Data Synthesis
3. Results
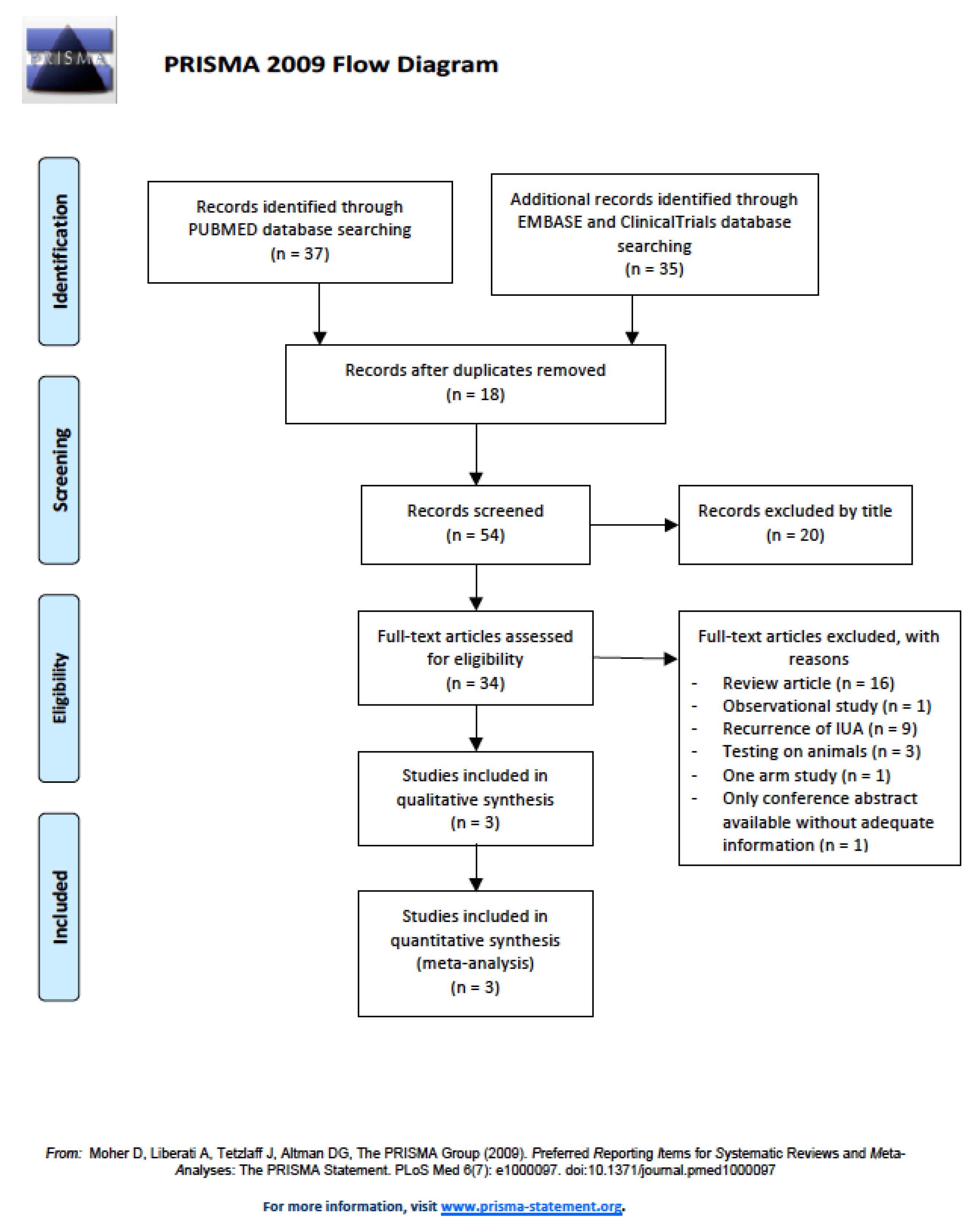
3.1. Strategy to Include Studies in the Current Meta-Analysis
3.2. Characteristics of Included Studies
3.3. Quality of Included Studies
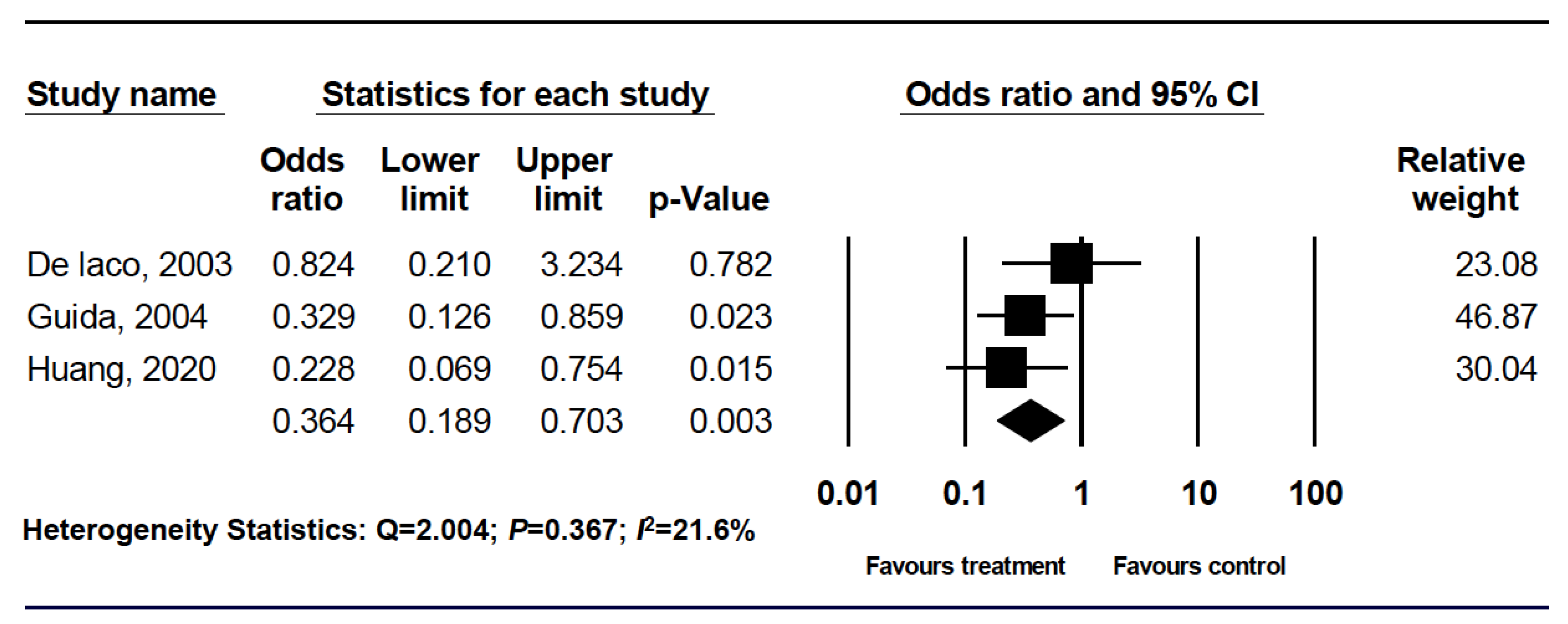
3.4. Effectiveness of Primary Prevention of Developing Intrauterine Adhesion in Patients Undergoing Hysteroscopic Surgery, Including Fibroid, Polyp, and Septum
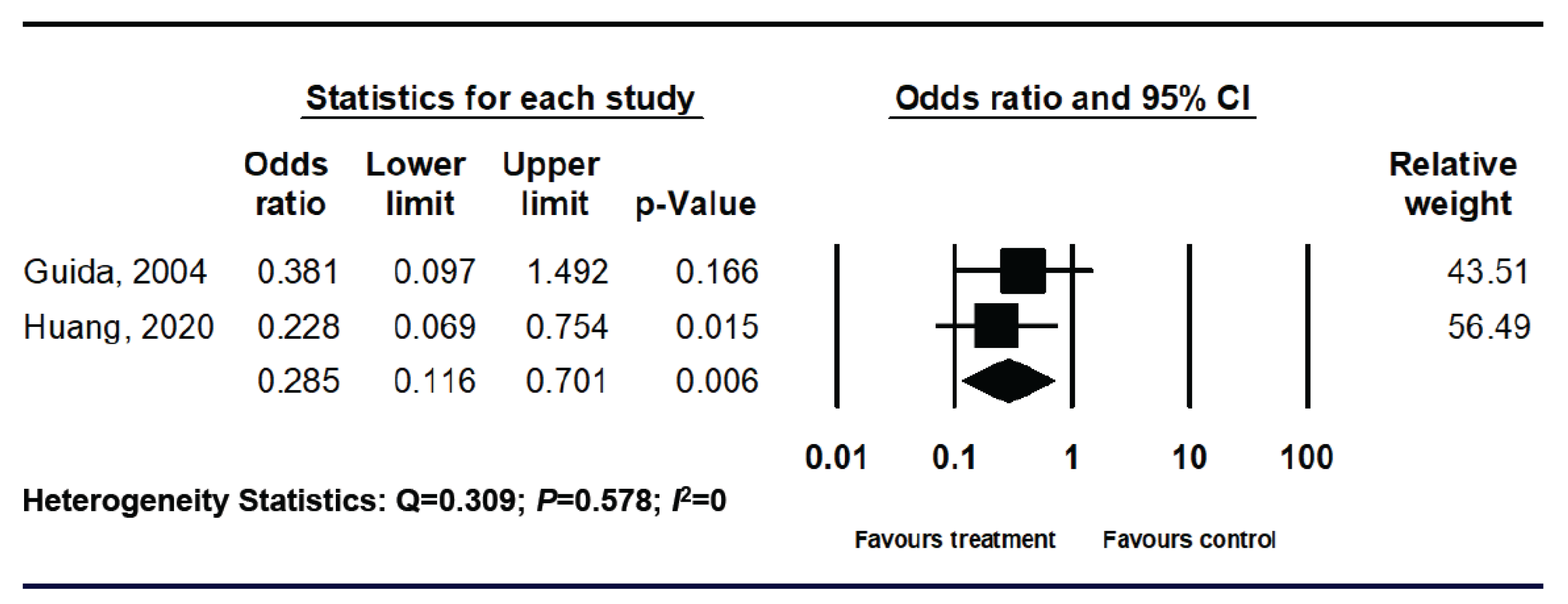
3.5. Significant Reduction of Intrauterine Adhesion Rates in Patients Undergoing Hysteroscopic Myomectomy
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ACHA | auto-crosslinked hyaluronic acid |
| CI | confidence interval |
| D&C | dilation and curettage |
| IUA | intrauterine adhesion or intrauterine adhesions |
| NaCMC | sodium carboxymethylcellulose |
| OR | odds ratio |
| PEO | polyethylene oxide |
| PRISMA | Preferred Reporting Items for Systematic reviews and Meta-analyses |
| RCTs | randomized controlled trials |
| RR | relative risk |
References
- Yu, D.; Wong, Y.M.; Cheong, Y.; Xia, E.; Li, T.C. Asherman syndrome-one century later. Fertil. Steril. 2008, 89, 759–779. [Google Scholar] [CrossRef] [PubMed]
- Deans, R.; Abbott, J. Review of intrauterine adhesions. J. Minim. Invasive Gynecol. 2010, 17, 555–569. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, N.; Smorgick, N.; Ben Ami, I.; Vaknin, Z.; Tovbin, Y.; Halperin, R.; Pansky, M. Intercoat (Oxiplex/AP gel) for preventing intrauterine adhesions after operative hysteroscopy for suspected retained products of conception: Double-blind, prospective, randomized pilot study. J. Minim. Invasive Gynecol. 2014, 21, 126–130. [Google Scholar] [CrossRef] [PubMed]
- Hooker, A.B.; Lemmers, M.; Thurkow, A.L.; Heymans, M.W.; Opmeer, B.C.; Brolmann, H.A.M.; Mol, B.W.; Huirne, J.A.F. Systematic review and meta-analysis of intrauterine adhesions after miscarriage: Prevalence, risk factors and long-term reproductive outcome. Hum. Reprod. Update 2014, 20, 262–278. [Google Scholar] [CrossRef] [Green Version]
- Barel, O.; Krakov, A.; Pansky, M.; Vaknin, Z.; Halperin, R.; Smorgick, N. Intrauterine adhesions after hysteroscopic treatment for retained products of conception: What are the risk factors? Fertil. Steril. 2015, 103, 775–779. [Google Scholar] [CrossRef]
- Hooker, A.B.; de Leeuw, R.; van de Ven, P.M.; Bakkum, E.A.; Thurkow, A.L.; Vogel, N.E.A.; van Vliet, H.A.A.M.; Bongers, M.Y.; Emanuel, M.H.; Verdonkschot, A.E.M.; et al. Prevalence of intrauterine adhesions after the application of hyaluronic acid gel after dilatation and curettage in women with at least one previous curettage: Short-term outcomes of a multicenter, prospective randomized controlled trial. Fertil. Steril. 2017, 107, 1223–1231. [Google Scholar] [CrossRef] [Green Version]
- Salazar, C.A.; Isaacson, K.; Morris, S. A comprehensive review of Asherman’s syndrome: Causes, symptoms and treatment options. Curr. Opin. Obstet. Gynecol. 2017, 29, 249–256. [Google Scholar] [CrossRef]
- Dreisler, E.; Kjer, J.J. Asherman’s syndrome: Current perspectives on diagnosis and management. Int. J. Womens Health 2019, 11, 191–198. [Google Scholar] [CrossRef]
- Dawood, A.; Al-Talib, A.; Tulandi, T. Predisposing factors and treatment outcome of different stages of intrauterine adhesions. J. Obstet. Gynaecol. Can. 2010, 32, 767–770. [Google Scholar] [CrossRef]
- Jiang, D.; Rinkevich, Y. Scars or regeneration?—Dermal fibroblasts as drivers of diverse skin wound responses. Int. J. Mol. Sci. 2020, 21, 617. [Google Scholar] [CrossRef] [Green Version]
- El Ayadi, A.; Jay, J.W.; Prasai, A. Current approaches targeting the wound healing phases to attenuate fibrosis and scarring. Int. J. Mol. Sci. 2020, 21, 1105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akita, S. Wound repair and regeneration: Mechanisms, signaling. Int. J. Mol. Sci. 2019, 20, 6328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogawa, R. Recent advances in scar biology. Int. J. Mol. Sci. 2018, 19, 1749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, P.H.; Huang, B.S.; Horng, H.C.; Yeh, C.C.; Chen, Y.J. Wound healing. J. Chin. Med. Assoc. 2018, 81, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Horng, H.C.; Chang, W.H.; Yeh, C.C.; Huang, B.S.; Chang, C.P.; Chen, Y.J.; Tsui, K.H.; Wang, P.H. Estrogen effects on wound healing. Int. J. Mol. Sci. 2017, 18, 2325. [Google Scholar] [CrossRef]
- Owusu-Akyaw, A.; Krishnamoorthy, K.; Goldsmith, L.T.; Morelli, S.S. The role of mesenchymal-epithelial transition in endometrial function. Hum. Reprod. Update 2019, 25, 114–133. [Google Scholar] [CrossRef]
- Wei, C.; Pan, Y.; Zhang, Y.; Dai, Y.; Jiang, L.; Shi, L.; Yang, W.; Xu, S.; Zhang, Y.; Xu, W.; et al. Overactivated sonic hedgehog signaling aggravates intrauterine adhesion via inhibiting autophagy in endometrial stromal cells. Cell. Death. Dis. 2020, 11, 755. [Google Scholar] [CrossRef]
- Liu, F.; Hu, S.; Wang, S.; Cheng, K. Cell and biomaterial-based approaches to uterus regeneration. Regen. Biomater. 2019, 6, 141–148. [Google Scholar] [CrossRef]
- Zhou, Q.; Wu, X.; Hu, J.; Yuan, R. Abnormal expression of fibrosis markers, estrogen receptor α and stromal derived factor-1/chemokine (C-X-C motif) receptor-4 axis in intrauterine adhesions. Int. J. Mol. Med. 2018, 42, 81–90. [Google Scholar] [CrossRef]
- Foix, A.; Bruno, R.O.; Davison, T.; Lema, B. The pathology of postcurettage adhesions. Am. J. Obstet. Gynecol. 1966, 96, 1027–1033. [Google Scholar] [CrossRef]
- Yaffe, H.; Ron, M.; Polishuk, W. Amenorrhoea, hypomenorrhoea and uterine fibrosis. Am. J. Obstet. Gynecol. 1978, 130, 599–601. [Google Scholar] [CrossRef]
- Han, Q.; Du, Y. Advances in the application of biomimetic endometrium interfaces for uterine bioengineering in female infertility. Front. Bioeng. Biotechnol. 2020, 8, 153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, Y.; Xu, D. The Effect of adjuvant treatment to prevent and treat intrauterine adhesions: A network meta-analysis of randomized controlled trials. J. Minim. Invasive Gynecol. 2018, 25, 589–599. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.Y.; Tsai, C.C.; Kung, F.T.; Lan, K.C.; Ou, Y.C. Association between hysteroscopic findings of previous cesarean delivery scar defects and abnormal uterine bleeding. Taiwan J. Obstet. Gynecol. 2019, 58, 541–544. [Google Scholar] [CrossRef] [PubMed]
- Doroftei, B.; Dabuleanu, A.M.; Ilie, O.D.; Maftei, R.; Anton, E.; Simionescu, G.; Matei, T.; Armeanu, T. Mini-review of the new therapeutic possibilities in Asherman syndrome—Where are we after one hundred and twenty-six years? Diagnostics 2020, 10, 706. [Google Scholar] [CrossRef] [PubMed]
- Valle, R.F.; Sciarra, J.J. Intrauterine adhesions: Hysteroscopic diagnosis, classification, treatment, and reproductive outcome. Am. J. Obstet. Gynecol. 1988, 158, 1459–1470. [Google Scholar] [CrossRef]
- Menzies, D. Postoperative adhesions: Their treatment and relevance in clinical practice. Ann. R. Coll. Surg. Engl. 1993, 75, 147–153. [Google Scholar]
- Schenker, J.G. Etiology of and therapeutic approach to synechia uteri. Eur. J. Obstet. Gynecol. Reprod. Biol. 1996, 65, 109–113. [Google Scholar] [CrossRef]
- Healy, M.W.; Schexnayder, B.; Connell, M.T.; Terry, N.; DeCherney, A.H.; Csokmay, J.M.; Yauger, B.J.; Hill, M.J. Intrauterine adhesion prevention after hysteroscopy: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2016, 215, 267–275. [Google Scholar] [CrossRef]
- Bosteels, J.; Weyers, S.; D’Hooghe, T.M.; Torrance, H.; Broekmans, F.J.; Chua, S.J.; Mol, B.W.J. Anti-adhesion therapy following operative hysteroscopy for treatment of female subfertility. Cochrane. Database Syst. Rev. 2017, 11, CD011110. [Google Scholar] [CrossRef] [Green Version]
- Di Spiezio Sardo, A.; Spinelli, M.; Bramante, S.; Scognamiglio, M.; Greco, E.; Guida, M.; Cela, V.; Nappi, C. Efficacy of a polyethylene oxide-sodium carboxymethylcellulose gel in prevention of intrauterine adhesions after hysteroscopic surgery. J. Minim. Invasive Gynecol. 2011, 18, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Bosteels, J.; Weyers, S.; Mol, B.W.; D’Hooghe, T. Anti-adhesion barrier gels following operative hysteroscopy for treating female infertility: A systematic review and meta-analysis. Gynecol. Surg. 2014, 11, 113–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, F.; Xin, X.; He, F.; Liu, J.; Cui, Y. Meta-analysis on the use of hyaluronic acid gel to prevent intrauterine adhesion after intrauterine operations. Exp. Ther. Med. 2020, 19, 2672–2678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsubara, S. A novel uterine stent for preventing intrauterine adhesion: Not only gynecologic but also obstetric significance. Ann. Transl. Med. 2020, 8, 614. [Google Scholar] [CrossRef]
- Lee, D.Y.; Lee, S.R.; Kim, S.K.; Joo, J.K.; Lee, W.S.; Shin, J.H.; Cho, S.; Park, J.C.; Kim, S.H. A new thermo-responsive hyaluronic acid sol-gel to prevent intrauterine adhesions after hysteroscopic surgery: A randomized, non-inferiority trial. Yonsei Med. J. 2020, 61, 868–874. [Google Scholar] [CrossRef] [PubMed]
- Ducarme, G.; Davitian, C.; Zarrouk, S.; Uzan, M.; Poncelet, C. Interest of auto-crosslinked hyaluronic acid gel in the prevention of intrauterine adhesions after hysteroscopic surgery: A case-control study. J. Gynecol. Obstet. Biol. Reprod. 2006, 35, 691–695. [Google Scholar] [CrossRef]
- Huang, H.; Xu, B.; Cheng, C.; Xu, D. A novel intrauterine stent for prevention of intrauterine adhesions. Ann. Transl. Med. 2020, 8, 61. [Google Scholar] [CrossRef]
- Mettler, L.; Schollmeyer, T.; Tinelli, A.; Malvasi, A.; Alkatout, I. Complications of uterine fibroids and their management, surgical management of fibroids, laparoscopy and hysteroscopy versus hysterectomy, haemorrhage, adhesions, and complications. Obstet. Gynecol. Int. 2012, 2012, 791248. [Google Scholar] [CrossRef] [Green Version]
- Capmas, P.; Levaillant, J.M.; Fernandez, H. Surgical techniques and outcome in the management of submucous fibroids. Curr. Opin. Obst. Gyn. 2013, 25, 332–338. [Google Scholar] [CrossRef]
- Mazzon, I.; Favilli, A.; Cocco, P.; Grasso, M.; Horvath, S.; Bini, V.; Di Renzo, G.C.; Gerli, S. Does cold loop hysteroscopic myomectomy reduce intrauterine adhesions? A retrospective study. Fertil. Steril. 2014, 101, 294–298. [Google Scholar] [CrossRef]
- Litta, P.; Leggieri, C.; Conte, L.; Dalla Toffola, A.; Multinu, F.; Angioni, S. Monopolar versus bipolar device: Safety, feasibility, limits and perioperative complications in performing hysteroscopic myomectomy. Clin. Exp. Obstet. Gynecol. 2014, 41, 335–338. [Google Scholar] [PubMed]
- Haber, K.; Hawkins, E.; Levie, M.; Chudnoff, S. Hysteroscopic morcellation: Review of the manufacturer and user facility device experience (MAUDE) database. J. Minim. Invasive Gynecol. 2015, 22, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Ciebiera, M.; Łoziński, T.; Wojtyła, C.; Rawski, W.; Jakiel, G. Complications in modern hysteroscopic myomectomy. Ginekol. Pol. 2018, 89, 398–404. [Google Scholar] [CrossRef] [Green Version]
- Friedman, J.A.; Wong, J.M.K.; Chaudhari, A.; Tsai, S.; Milad, M.P. Hysteroscopic myomectomy: A comparison of techniques and review of current evidence in the management of abnormal uterine bleeding. Curr. Opin. Obstet. Gynecol. 2018, 30, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Chiu, C.S.; Hwu, Y.M.; Lee, R.K.; Lin, M.H. Intrauterine adhesion prevention with Malecot catheter after hysteroscopic myomectomy: A novel approach. Taiwan J. Obstet. Gynecol. 2020, 59, 56–60. [Google Scholar] [CrossRef]
- March, C.M. Management of Asherman’s syndrome. Rerpod. BioMed. Online. 2011, 23, 63–76. [Google Scholar] [CrossRef] [Green Version]
- Santamaria, X.; Isaacson, K.; Simón, C. Asherman’s Syndrome: It may not be all our fault. Hum. Reprod. 2018, 33, 1374–1380. [Google Scholar] [CrossRef]
- Yang, J.H.; Chen, M.J.; Chen, C.D.; Chen, S.U.; Ho, H.N.; Yang, Y.S. Optimal waiting period for subsequent fertility treatment after various hysteroscopic surgeries. Fertil. Steril. 2013, 99, 2092–2096. [Google Scholar] [CrossRef]
- Yang, J.H.; Chen, M.J.; Wu, M.Y.; Chao, K.H.; Ho, H.N.; Yang, Y.S. Office hysteroscopic early lysis of intrauterine adhesion after transcervical resection of multiple apposing submucous myomas. Fertil. Steril. 2008, 89, 1254–1259. [Google Scholar] [CrossRef]
- Liao, W.L.; Ying, T.H.; Shen, H.P.; Wu, P.J. Combined treatment for big submucosal myoma with High Intensity Focused Ultrasound and hysteroscopic resection. Taiwan J. Obstet. Gynecol. 2019, 58, 888–890. [Google Scholar] [CrossRef]
- Zhang, L.P.; Wang, M.; Shang, X.; Zhang, Q.; Yang, B.J.; Xu, Y.; Li, J.H.; Feng, L.M. The incidence if placeta related diseases after the hysteroscopic adhesiolysis in patients with intrauterine adhesions. Taiwan J. Obstet. Gynecol. 2020, 59, 575–579. [Google Scholar] [CrossRef] [PubMed]
- Dogan, O.; Pulatoglu, C.; Yassa, M. A new facilitating technique for postpartum hysterectomy at full dilatation: Cervical clamp. J. Chin. Med. Assoc. 2018, 81, 366–369. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, N.; Takeuchi, R.; Izuchi, D.; Yuge, N.; Miyazaki, M.; Yasunaga, M.; Egashira, K.; Ueoka, Y.; Inoue, Y. Hysteroscopic adhesiolysis for patients with Asherman’s syndrome: Menstrual and fertility outcomes. Reprod. Med. Biol. 2013, 12, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Di Guardo, F.; Della Corte, L.; Vilos, G.A.; Carugno, J.; Török, P.; Giampaolino, P.; Manchanda, R.; Vitale, S.G. Evaluation and treatment of infertile women with Asherman syndrome: An updated review focusing on the role of hysteroscopy. Reprod. Biomed. Online 2020, 41, 55–61. [Google Scholar] [CrossRef]
- Donnez, J.; Nisolle, M. Hysteroscopic lysis of intrauterine adhesions (Asherman syndrome). In Atlas of Laser Operative Laparoscopy and Hysteroscopy; Donnez, J., Ed.; Parthenon: New York, NY, USA, 1994; pp. 305–322. [Google Scholar]
- Zhou, Q.; Shi, X.; Saravelos, S.; Huang, X.; Zhao, Y.; Huang, R.; Xia, E.; Li, T.C. Auto-cross-linked hyaluronic acid gel for prevention of intrauterine adhesions after hysteroscopic adhesiolysis: A randomized controlled trial. J. Minim. Invasive Gynecol. 2020. [Google Scholar] [CrossRef]
- Lin, X.; Wei, M.; Li, T.C.; Huang, Q.; Huang, D.; Zhou, F.; Zhang, S. A comparison of intrauterine balloon, intrauterine contraceptive device and hyaluronic acid gel in the prevention of adhesion reformation following hysteroscopic surgery for asherman syndrome: A cohort study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 170, 512–516. [Google Scholar] [CrossRef]
- Salma, U.; Xue, M.; Md Sayed, A.S.; Xu, D. Efficacy of intrauterine device in the treatment of intrauterine adhesions. Biomed. Res. Int. 2014, 2014, 589296. [Google Scholar] [CrossRef] [Green Version]
- Azumaguchi, A.; Henmi, H.; Saito, T. Efficacy of silicone sheet as a personalized barrier for preventing adhesion reformation after hysteroscopic adhesiolysis of intrauterine adhesions. Reprod. Med. Biol. 2019, 18, 378–383. [Google Scholar] [CrossRef]
- Zhu, R.; Duan, H.; Gan, L.; Wang, S. Comparison of intrauterine suitable balloon and Foley balloon in the prevention of adhesion after hysteroscopic adhesiolysis. Biomed. Res. Int. 2018, 2018, 9494101. [Google Scholar] [CrossRef] [Green Version]
- Thubert, T.; Dussaux, C.; Demoulin, G.; Rivain, A.L.; Trichot, C.; Deffieux, X. Influence of auto-cross-linked hyaluronic acid gel on pregnancy rate and hysteroscopic outcomes following surgical removal of intra-uterine adhesions. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 193, 65–69. [Google Scholar] [CrossRef]
- Passos, I.M.P.E.; Britto, R.L. Diagnosis and treatment of müllerian malformations. Taiwan. J. Obstet. Gynecol. 2020, 59, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Fei, Z.; Bin, Z.; Xin, X.; Fei, H.; Yuechong, C. Meta-analysis on the use of hyaluronic acid gel to prevent recurrence of intrauterine adhesion after hysteroscopic adhesiolysis. Taiwan. J. Obstet. Gynecol. 2019, 58, 731–736. [Google Scholar] [CrossRef] [PubMed]
- Krajcovicova, R.; Hudeck, R.; Ventruba, P.; Surgentova, K. The role of hyaluronan in Asherman’s syndrome therapy. J. Gynecol. Surg. 2015, 31, 250–254. [Google Scholar] [CrossRef]
- Diamond, M.P.; Daniell, J.F.; Feste, J.; Surrey, M.W.; McLaughlin, D.S.; Friedman, S.; Vaughn, W.K.; Martin, D.C. Adhesion reformation and de novo adhesion formation after reproductive pelvic surgery. Fertil. Steril. 1987, 47, 864–866. [Google Scholar] [CrossRef]
- Guida, M.; Acunzo, G.; Di Spiezio Sardo, A.; Bifulco, G.; Piccoli, R.; Pellicano, M.; Cerrota, G.; Cirillo, D.; Nappi, C. Effectiveness of auto-crosslinked hyaluronic acid gel in the prevention of intrauterine adhesions after hysteroscopic surgery: A prospective, randomized, controlled study. Hum. Reprod. 2004, 19, 1461–1464. [Google Scholar] [CrossRef] [Green Version]
- Mensitieri, M.; Ambrosio, L.; Nicolais, L.; Bellini, D.; O’Regan, M. Viscoelastic properties modulation of a novel autocrosslinked hyaluronic acid polymer. J. Mater. Sci. Mater. Med. 1996, 7, 695–698. [Google Scholar] [CrossRef]
- Lee, H.H.; Huang, B.S.; Cheng, M.; Yeh, C.C.; Lin, I.C.; Horng, H.C.; Huang, H.Y.; Lee, W.L.; Wang, P.H. Intracervical Foley catheter plus intravaginal misoprostol vs intravaginal misoprostol alone for cervical ripening: A meta-analysis. Int. J. Environ. Res. Health 2020, 17, 1825. [Google Scholar] [CrossRef] [Green Version]
- De Iaco, P.A.; Muzzupapa, G.; Bigon, E.; Pressato, D.; Dona, M.; Pavesio, A.; Bovicelli, L. Efficacy of a hyaluronan derivative gel in postsurgical adhesion prevention in the presence of inadequate hemostasis. Surgery 2001, 130, 60–64. [Google Scholar] [CrossRef]
- Huang, C.Y.; Chang, W.H.; Cheng, M.; Huang, H.Y.; Horng, H.C.; Chen, Y.J.; Lee, W.L.; Wang, P.H. Crosslinked hyaluronic acid gels for the prevention of intrauterine adhesions after a hysteroscopic myomectomy in women with submucosal myomas: A prospective, randomized, controlled trial. Life 2020, 10, 67. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Taskin, O.; Sadik, S.; Onoglu, A.; Gokdeniz, R.; Erturan, E.; Burak, F.; Wheeler, J.M. Role of endometrial suppression on the frequency of intrauterine adhesions after resectoscopic surgery. J. Am. Assoc. Gynecol. Laparosc. 2000, 7, 351–354. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study [Ref.] | n | Age (y) | Indication | Exclusion Criteria | Tools | Intervention | Follow-up Evaluation | DR |
|---|---|---|---|---|---|---|---|---|
| De Iaco, 2003 [69] | 40 | 18–65 | Fibroid Polyp Septum | Not stated | MR | HA/NaCMC, 10.5 ± 5.5 mL | 9 weeks | Not stated |
| Guida, 2004 [67] | 132 | <50 | Fibroid (n = 49) Polyp (n = 67) Septum (n = 16) | Postmenopause Pregnancy Prolapse Current illness Age > 50 y BW > 100 kg Other intrauterine lesions | BR | ACHA, 10 mL | 3 months | 4.3% |
| Huang, 2020 [70] | 70 | 20–65 | Fibroid (n = 70) |
| BR | 3 or 4% ACHA, 10 mL | 12 weeks | 1.4% |
| Study [Ref.] | Bias Due to Randomization Process | Bias Due to Deviation from Intended Intervention | Bias Due to Missing Data | Bias Due to Outcome Measurement | Bias Due to Selection of Reported Results | Overall Risk of Bias |
|---|---|---|---|---|---|---|
| De Iaco, 2003 [69] | No information | No information | No information | No information | Some concerns | High |
| Guida, 2004 [67] | Low | Some concerns | Some concerns | Low | Low | Some concerns |
| Huang, 2020 [70] | Low | Low | Low | Low | Low | Low |
| Study [Reference] | Intervention | Control | p-Value | ||
|---|---|---|---|---|---|
| n | Adhesion rate | n | Adhesion rate | ||
| De Iaco, 2003 [69] | 18 | 27.8% | 22 | 31.8% | 0.78 |
| Guida, 2004 [67] | 67 | 10.4% | 65 | 26.2% | <0.05 |
| Huang, 2020 [70] | 47 | 12.8% | 23 | 39.1% | 0.012 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, M.; Chang, W.-H.; Yang, S.-T.; Huang, H.-Y.; Tsui, K.-H.; Chang, C.-P.; Lee, W.-L.; Wang, P.-H. Efficacy of Applying Hyaluronic Acid Gels in the Primary Prevention of Intrauterine Adhesion after Hysteroscopic Myomectomy: A Meta-Analysis of Randomized Controlled Trials. Life 2020, 10, 285. https://doi.org/10.3390/life10110285
Cheng M, Chang W-H, Yang S-T, Huang H-Y, Tsui K-H, Chang C-P, Lee W-L, Wang P-H. Efficacy of Applying Hyaluronic Acid Gels in the Primary Prevention of Intrauterine Adhesion after Hysteroscopic Myomectomy: A Meta-Analysis of Randomized Controlled Trials. Life. 2020; 10(11):285. https://doi.org/10.3390/life10110285
Chicago/Turabian StyleCheng, Min, Wen-Hsun Chang, Szu-Ting Yang, Hsin-Yi Huang, Kuan-Hao Tsui, Chia-Pei Chang, Wen-Ling Lee, and Peng-Hui Wang. 2020. "Efficacy of Applying Hyaluronic Acid Gels in the Primary Prevention of Intrauterine Adhesion after Hysteroscopic Myomectomy: A Meta-Analysis of Randomized Controlled Trials" Life 10, no. 11: 285. https://doi.org/10.3390/life10110285