
Fasting GLP-1 Levels and Albuminuria Are Negatively Associated in Patients with Type 2 Diabetes Mellitus
 , , ,
, , ,
Abstract
:
1. Introduction
2. Methods
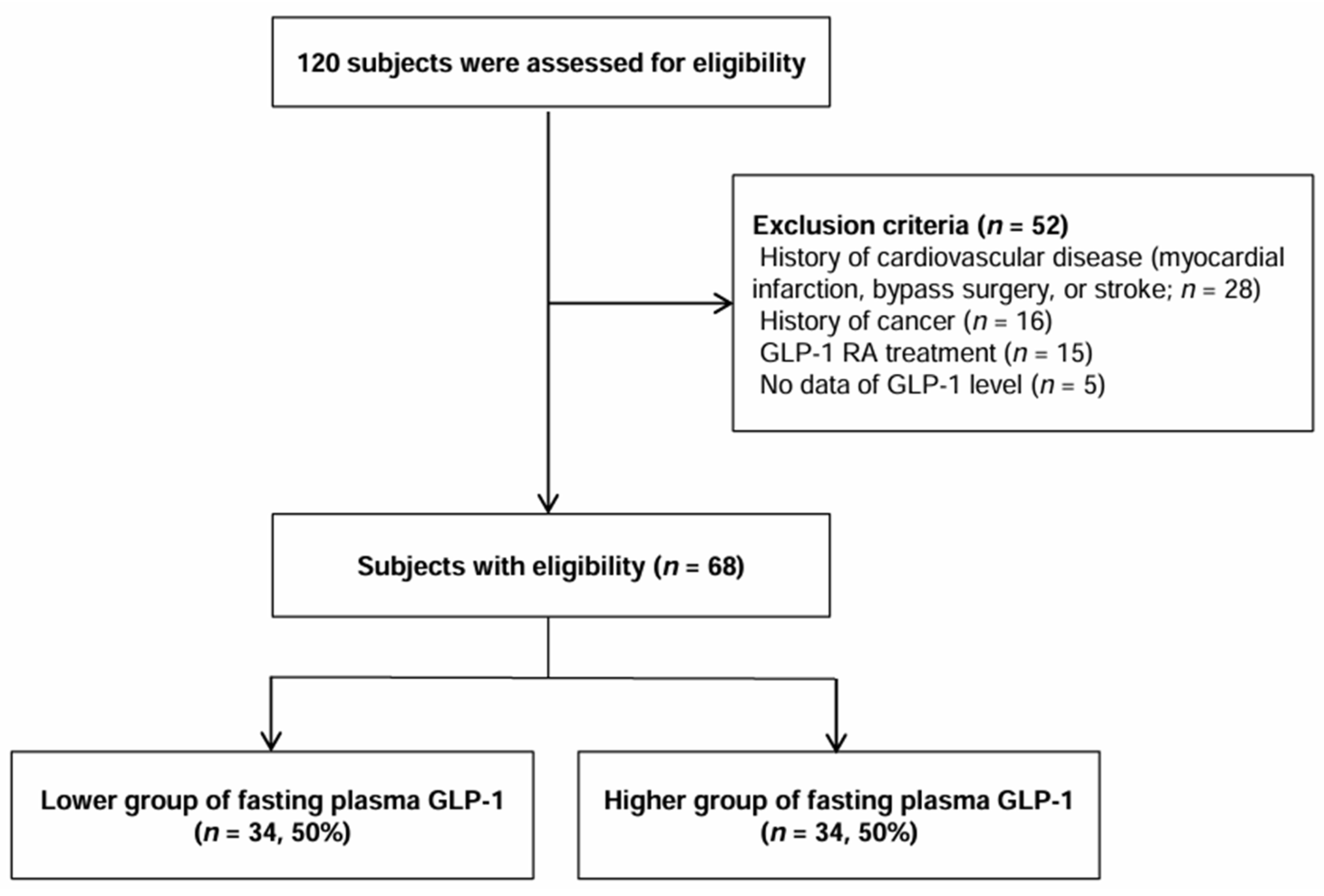
2.1. Study Population and Design
2.2. Measurement
2.3. Statistics Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bae, J.H.; Han, K.-D.; Ko, S.-H.; Yang, Y.S.; Choi, J.H.; Choi, K.M.; Kwon, H.-S.; Won, K.C.; on Behalf of the Committee of Media-Public Relation of the Korean Diabetes Association. Diabetes Fact Sheet in Korea 2021. Diabetes Metab. J. 2022, 46, 417–426. [Google Scholar] [CrossRef]
- Jin, D.C.; Han, J.S. Renal replacement therapy in Korea, 2012. Kidney Res. Clin. Pract. 2014, 33, 9–18. [Google Scholar] [CrossRef]
- Hong, Y.A.; Ban, T.H.; Kang, C.-Y.; Hwang, S.D.; Choi, S.R.; Lee, H.; Jung, H.-Y.; Kim, K.; Kwon, Y.E.; Kim, S.H.; et al. Trends in epidemiologic characteristics of end-stage renal disease from 2019 Korean Renal Data System (KORDS). Kidney Res. Clin. Pract. 2021, 40, 52–61. [Google Scholar] [CrossRef]
- Li, S.; Wang, J.; Zhang, B.; Li, X.; Liu, Y. Diabetes Mellitus and Cause-Specific Mortality: A Population-Based Study. Diabetes Metab. J. 2019, 43, 319–341. [Google Scholar] [CrossRef]
- Fox, C.S. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes: A meta-analysis (vol 380, pg 1662, 2012). Lancet 2013, 381, 374. [Google Scholar]
- Parving, H.-H. Diabetic nephropathy: Prevention and treatment. Kidney Int. 2001, 60, 2041–2055. [Google Scholar] [CrossRef]
- Wada, T.; Shimizu, M.; Toyama, T.; Hara, A.; Kaneko, S.; Furuichi, K. Clinical impact of albuminuria in diabetic nephropathy. Clin. Exp. Nephrol. 2012, 16, 96–101. [Google Scholar] [CrossRef]
- Benzing, T.; Salant, D. Insights into Glomerular Filtration and Albuminuria. N. Engl. J. Med. 2021, 384, 1437–1446. [Google Scholar] [CrossRef]
- Holst, J.J. The Physiology of Glucagon-like Peptide 1. Physiol. Rev. 2007, 87, 1409–1439. [Google Scholar] [CrossRef]
- Elliott, R.M.; Morgan, L.M.; Tredger, J.A.; Deacon, S.; Wright, J.; Marks, V. Glucagon-like peptide-1(7–36)amide and glucose-dependent insulinotropic polypeptide secretion in response to nutrient ingestion in man: Acute post-prandial and 24-h secretion patterns. J. Endocrinol. 1993, 138, 159–166. [Google Scholar] [CrossRef]
- Roberge, J.N.; Brubaker, P.L. Regulation of intestinal proglucagon-derived peptide secretion by glucose-dependent insulinotropic peptide in a novel enteroendocrine loop. Endocrinology 1993, 133, 233–240. [Google Scholar] [CrossRef]
- Baggio, L.L.; Drucker, D.J. Biology of Incretins: GLP-1 and GIP. Gastroenterology 2007, 132, 2131–2157. [Google Scholar] [CrossRef]
- Drucker, D.J.; Nauck, M.A. The incretin system: Glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes. Lancet 2006, 368, 1696–1705. [Google Scholar] [CrossRef]
- Crajoinas, R.O.; Oricchio, F.T.; Pessoa, T.D.; Pacheco, B.P.M.; Lessa, L.M.A.; Malnic, G.; Girardi, A.C.C. Mechanisms mediating the diuretic and natriuretic actions of the incretin hormone glucagon-like peptide-1. Am. J. Physiol. Physiol. 2011, 301, F355–F363. [Google Scholar] [CrossRef]
- Calanna, S.; Christensen, M.; Holst, J.J.; Laferrère, B.; Gluud, L.L.; Vilsbøll, T.; Knop, F.K. Secretion of glucagon-like peptide-1 in patients with type 2 diabetes mellitus: Systematic review and meta-analyses of clinical studies. Diabetologia 2013, 56, 965–972. [Google Scholar] [CrossRef]
- Mosenzon, O.; Schechter, M.; Leibowitz, G. Kidney Outcomes with Glucagon-Like Peptide-1 Receptor Agonists in Patients with Type 2 Diabetes. Adv. Chronic Kidney Dis. 2021, 28, 347–360. [Google Scholar] [CrossRef]
- Gerstein, H.C.; Colhoun, H.M.; Dagenais, G.R.; Diaz, R.; Lakshmanan, M.; Pais, P.; Probstfield, J.; Botros, F.T.; Riddle, M.C.; Rydén, L.; et al. Dulaglutide and renal outcomes in type 2 diabetes: An exploratory analysis of the REWIND randomised, placebo-controlled trial. Lancet 2019, 394, 131–138. [Google Scholar] [CrossRef]
- Mann, J.F.E.; Orsted, D.D.; Brown-Frandsen, K.; Marso, S.P.; Poulter, N.R.; Rasmussen, S.; Tornøe, K.; Zinman, B.; Buse, J.B.; for the LEADER Steering Committee and Investigators. Liraglutide and Renal Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 839–848. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A More Accurate Method to Estimate Glomerular Filtration Rate from Serum Creatinine: A New Prediction Equation. Modification of Diet in Renal Disease Study Group. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Pfeffer, M.A.; Claggett, B.; Diaz, R.; Dickstein, K.; Gerstein, H.C.; Køber, L.V.; Lawson, F.C.; Ping, L.; Wei, X.; Lewis, E.F.; et al. Lixisenatide in Patients with Type 2 Diabetes and Acute Coronary Syndrome. N. Engl. J. Med. 2015, 373, 2247–2257. [Google Scholar] [CrossRef]
- Marso, S.P.; Daniels, G.H.; Brown-Frandsen, K.; Kristensen, P.; Mann, J.F.; Nauck, M.A.; Nissen, S.E.; Pocock, S.; Poulter, N.R.; Ravn, L.S.; et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 311–322. [Google Scholar] [CrossRef]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jodar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 1834–1844. [Google Scholar] [CrossRef]
- Holman, R.R.; Bethel, M.A.; Mentz, R.J.; Thompson, V.P.; Lokhnygina, Y.; Buse, J.B.; Chan, J.C.; Choi, J.; Gustavson, S.M.; Iqbal, N.; et al. Effects of Once-Weekly Exenatide on Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 1228–1239. [Google Scholar] [CrossRef]
- Hernandez, A.F.; Green, J.B.; Janmohamed, S.; D’Agostino, R.B.; Granger, C.B.; Jones, N.P.; Leiter, L.A.; Rosenberg, A.E.; Sigmon, K.N.; Somerville, M.C.; et al. Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes): A double-blind, randomised placebo-controlled trial. Lancet 2018, 392, 1519–1529. [Google Scholar] [CrossRef]
- Gerstein, H.C.; Colhoun, H.M.; Dagenais, G.R.; Diaz, R.; Lakshmanan, M.; Pais, P.; Probstfield, J.; Riesmeyer, J.S.; Riddle, M.C.; Rydén, L.; et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): A double-blind, randomised placebo-controlled trial. Lancet 2019, 394, 121–130. [Google Scholar] [CrossRef]
- Husain, M.; Birkenfeld, A.L.; Donsmark, M.; Dungan, K.; Eliaschewitz, F.G.; Franco, D.R.; Jeppesen, O.K.; Lingvay, I.; Mosenzon, O.; Pedersen, S.D.; et al. Oral Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2019, 381, 841–851. [Google Scholar] [CrossRef]
- Kristensen, S.L.; Rørth, R.; Jhund, P.S.; Docherty, K.F.; Sattar, N.; Preiss, D.; Køber, L.; Petrie, M.C.; McMurray, J.J.V. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: A systematic review and meta-analysis of cardiovascular outcome trials. Lancet Diabetes Endocrinol. 2019, 7, 776–785. [Google Scholar] [CrossRef]
- Zelniker, T.A.; Wiviott, S.D.; Raz, I.; Im, K.; Goodrich, E.L.; Furtado, R.H.M.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; et al. Comparison of the Effects of Glucagon-Like Peptide Receptor Agonists and Sodium-Glucose Cotransporter 2 Inhibitors for Prevention of Major Adverse Cardiovascular and Renal Outcomes in Type 2 Diabetes Mellitus. Circulation 2019, 139, 2022–2031. [Google Scholar] [CrossRef]
- Perkovic, V.; Jardine, M.J.; Neal, B.; Bompoint, S.; Heerspink, H.J.L.; Charytan, D.M.; Edwards, R.; Agarwal, R.; Bakris, G.; Bull, S.; et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N. Engl. J. Med. 2019, 380, 2295–2306. [Google Scholar] [CrossRef]
- Belancic, A.; Kresovic, A.; Troskot Dijan, M. Glucagon-like peptide-1 receptor agonists in the era of COVID-19: Friend or foe? Clin. Obes. 2021, 11, e12439. [Google Scholar] [CrossRef]
- Reppo, I.; Jakobson, M.; Volke, V. Effects of Semaglutide and Empagliflozin on Inflammatory Markers in Patients with Type 2 Diabetes. Int. J. Mol. Sci. 2023, 24, 5714. [Google Scholar] [CrossRef]
- Astrup, A.; Rössner, S.; Van Gaal, L.; Rissanen, A.; Niskanen, L.; Al Hakim, M.; Madsen, J.; Rasmussen, M.F.; Lean, M.E. Effects of liraglutide in the treatment of obesity: A randomised, double-blind, placebo-controlled study. Lancet 2009, 374, 1606–1616. [Google Scholar] [CrossRef]
- Viby, N.-E.; Isidor, M.S.; Buggeskov, K.B.; Poulsen, S.S.; Hansen, J.B.; Kissow, H. Glucagon-Like Peptide-1 (GLP-1) Reduces Mortality and Improves Lung Function in a Model of Experimental Obstructive Lung Disease in Female Mice. Endocrinology 2013, 154, 4503–4511. [Google Scholar] [CrossRef]
- Zhao, L.; Chen, Y.; Xia, F.; Abudukerimu, B.; Zhang, W.; Guo, Y.; Wang, N.; Lu, Y. A Glucagon-Like Peptide-1 Receptor Agonist Lowers Weight by Modulating the Structure of Gut Microbiota. Front. Endocrinol. 2018, 9, 233. [Google Scholar] [CrossRef]
- Yip, K.P.; Tse, C.M.; McDonough, A.A.; Marsh, D.J. Redistribution of Na+/H+ exchanger isoform NHE3 in proximal tubules induced by acute and chronic hypertension. Am. J. Physiol. 1998, 275, F565–F575. [Google Scholar] [CrossRef]
- Yu, J.H.; Park, S.Y.; Lee, D.Y.; Kim, N.H.; Seo, J.A. GLP-1 receptor agonists in diabetic kidney disease: Current evidence and future directions. Kidney Res. Clin. Pract. 2022, 41, 136–149. [Google Scholar] [CrossRef]
- Tanaka, T.; Higashijima, Y.; Wada, T.; Nangaku, M. The potential for renoprotection with incretin-based drugs. Kidney Int. 2014, 86, 701–711. [Google Scholar] [CrossRef]
- Hendarto, H.; Inoguchi, T.; Maeda, Y.; Ikeda, N.; Zheng, J.; Takei, R.; Yokomizo, H.; Hirata, E.; Sonoda, N.; Takayanagi, R. GLP-1 analog liraglutide protects against oxidative stress and albuminuria in streptozotocin-induced diabetic rats via protein kinase A-mediated inhibition of renal NAD(P)H oxidases. Metabolism 2012, 61, 1422–1434. [Google Scholar] [CrossRef]
- Cai, X.; She, M.; Xu, M.; Chen, H.; Li, J.; Chen, X.; Zheng, D.; Liu, J.; Chen, S.; Zhu, J.; et al. GLP-1 treatment protects endothelial cells from oxidative stress-induced autophagy and endothelial dysfunction. Int. J. Biol. Sci. 2018, 14, 1696–1708. [Google Scholar] [CrossRef]
- Skov, J.; Dejgaard, A.; Frokiaer, J.; Holst, J.J.; Jonassen, T.; Rittig, S.; Christiansen, J.S. Glucagon-like peptide-1 (GLP-1): Effect on kidney hemodynamics and renin-angiotensin-aldosterone system in healthy men. J. Clin. Endocrinol. Metab. 2013, 98, E664–E671. [Google Scholar] [CrossRef]
- Song, L.-L.; Wang, N.; Zhang, J.-P.; Yu, L.-P.; Chen, X.-P.; Zhang, B.; Yang, W.-Y. Postprandial glucagon-like peptide 1 secretion is associated with urinary albumin excretion in newly diagnosed type 2 diabetes patients. World J. Diabetes 2023, 14, 279–289. [Google Scholar] [CrossRef]
- Basolo, A.; Heinitz, S.; Stinson, E.J.; Begaye, B.; Hohenadel, M.; Piaggi, P.; Krakoff, J.; Votruba, S.B. Fasting glucagon-like peptide 1 concentration is associated with lower carbohydrate intake and increases with overeating. J. Endocrinol. Investig. 2019, 42, 557–566. [Google Scholar] [CrossRef]
- McIntosh, C.H.; Demuth, H.U.; Pospisilik, J.A.; Pederson, R. Dipeptidyl peptidase IV inhibitors: How do they work as new antidiabetic agents? Regul. Pept. 2005, 128, 159–165. [Google Scholar] [CrossRef]
- Madsbad, S. Exenatide and liraglutide: Different approaches to develop GLP-1 receptor agonists (incretin mimetics)—Preclinical and clinical results. Best Pract. Res. Clin. Endocrinol. Metab. 2009, 23, 463–477. [Google Scholar] [CrossRef]
- Gerich, J. DPP-4 inhibitors: What may be the clinical differentiators? Diabetes Res. Clin. Pract. 2010, 90, 131–140. [Google Scholar] [CrossRef]
- Gilbert, M.P.; Pratley, R.E. GLP-1 Analogs and DPP-4 Inhibitors in Type 2 Diabetes Therapy: Review of Head-to-Head Clinical Trials. Front. Endocrinol. 2020, 11, 178. [Google Scholar] [CrossRef]
- Chu, C.D.; Powe, N.R.; McCulloch, C.E.; Banerjee, T.; Crews, D.C.; Saran, R.; Bragg-Gresham, J.; Morgenstern, H.; Pavkov, M.E.; Saydah, S.H.; et al. Angiotensin-Converting Enzyme Inhibitor or Angiotensin Receptor Blocker Use Among Hypertensive US Adults with Albuminuria. Hypertension 2021, 77, 94–102. [Google Scholar] [CrossRef]
- Robles, N.; Romero, B.; de Vinuesa, E.G.; Sánchez-Casado, E.; Cubero, J. Treatment of Proteinuria with Lercanidipine Associated with Renin-Angiotensin Axis-Blocking Drugs. Ren. Fail. 2010, 32, 192–197. [Google Scholar] [CrossRef]
- Loutradis, C.; Papadopoulou, E.; Angeloudi, E.; Karagiannis, A.; Sarafidis, P. The Beneficial Hemodynamic Actions of SGLT-2 Inhibitors beyond the Management of Hyperglycemia. Curr. Med. Chem. 2020, 27, 6682–6702. [Google Scholar] [CrossRef] [PubMed]
- Škrtić, M.; Cherney, D.Z. Sodium–glucose cotransporter-2 inhibition and the potential for renal protection in diabetic nephropathy. Curr. Opin. Nephrol. Hypertens. 2015, 24, 96–103. [Google Scholar] [CrossRef]
- Gerard, A.O.; Laurain, A.; Favre, G.; Drici, M.D.; Esnault, V.L.M. Activation of the Tubulo-Glomerular Feedback by SGLT2 Inhibitors in Patients with Type 2 Diabetes and Advanced Chronic Kidney Disease: Toward the End of a Myth? Diabetes Care 2022, 45, e148–e149. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variable | Fasting Plasma GLP-1 (pmol/L) | p-Value | ||
|---|---|---|---|---|
| Group L (<1.83) n = 34 | Group H (1.83–3.32) n = 34 | Total n = 68 | ||
| Age (years) | 59.3 ± 9.8 | 56.7 ± 10.0 | 58.8 ± 9.9 | 0.291 |
| Men, n (%) | 26 (76.5) | 17 (50.0) | 43 (63.2) | 0.044 |
| Systolic BP (mmHg) | 131.3 ± 15.9 | 127.8 ± 11.9 | 129.5 ± 14.0 | 0.326 |
| Diastolic BP (mmHg) | 74.5 ± 11.2 | 76.4 ± 10.9 | 75.4 ± 11.0 | 0.493 |
| Body mass index (kg/m2) | 26.0 ± 3.4 | 25.2 ± 5.3 | 25.6 ± 4.4 | 0.505 |
| Waist circumference (cm) | 92.0 ± 8.6 | 93.0 ± 10.4 | 92.5 ± 9.4 | 0.754 |
| Total cholesterol (mg/dL) | 156.0 ± 31.3 | 169.6 ± 34.3 | 162.8 ± 33.3 | 0.093 |
| HDL cholesterol (mg/dL) | 46.9 ± 8.0 | 47.9 ± 10.7 | 47.4 ± 9.4 | 0.656 |
| LDL cholesterol (mg/dL) | 75.6 ± 17.7 | 82.7 ± 18.4 | 79.2 ± 18.3 | 0.109 |
| Triglycerides (mg/dL) | 148.5 (110.0–198.0) | 160.0 (110.0–217.0) | 155.0 (110.0–212.0) | 0.840 |
| Duration of diabetes (months) | 121.9 ± 91.2 | 84.4 ± 79.4 | 102.9 ± 86.8 | 0.086 |
| HbA1c (%) | 8.3 ± 2.1 | 7.7 ± 1.5 | 8.0 ± 1.9 | 0.132 |
| Fasting plasma glucose (mg/dL) | 200.1 ± 78.5 | 177.0 ± 79.5 | 188.5 ± 79.3 | 0.231 |
| Fasting insulin (uIU/mL) | 12.9 (5.9–22.2) | 20.0 (8.1–32.9) | 14.5 (7.5–29.8) | 0.130 |
| HOMA-IR | 5.4 (2.8–13.5) | 10.9 (3.3–17.0) | 6.7 (3.0–14.3) | 0.275 |
| HOMA-β (%) | 27.4 (16.6–68.7) | 41.9 (17.0–85.1) | 32.7 (17.0–84.7) | 0.448 |
| Estimated GFR (mL/min/1.73 m2) | 90.9 ± 27.9 | 103.6 ± 27.2 | 97.3 ± 28.1 | 0.079 |
| Creatinine (mg/dL) | 0.9 ± 0.4 | 0.7 ± 0.3 | 0.8 ± 0.3 | 0.040 |
| hs-CRP (mg/dL) | 0.4 (0.2–1.1) | 0.9 (0.3–1.7) | 0.5 (0.2–1.4) | 0.067 |
| GLP-1 (pmol/L) | 1.4 ± 0.3 | 2.5 ± 0.5 | 2.0 ± 0.6 | <0.001 |
| UACR (mg/g) | 55.0 (0.0–470.0) | 10.0 (0.0–60.0) | 10.0 (0.0–195.0) | 0.036 |
| Albuminuria, n (%) | 20 (58.8) | 11 (32.4) | 31 (45.6) | 0.051 |
| Univariate Model | Fasting Plasma GLP-1 (pmol/L) | ||
|---|---|---|---|
| r | r2 | p-Value | |
| Age (years) | −0.161 | 0.026 | 0.190 |
| Men [n (%)] | 0.154 | 0.024 | 0.210 |
| Body mass index (kg/m2) | −0.039 | 0.002 | 0.749 |
| Waist circumference (cm) | −0.051 | 0.003 | 0.740 |
| Systolic BP (mmHg) | −0.173 | 0.030 | 0.172 |
| Estimated GFR (ml/min/1.73 m2) | 0.275 | 0.076 | 0.034 |
| hs-CRP (mg/L) | −0.089 | 0.008 | 0.472 |
| Total cholesterol (mg/dL) | 0.126 | 0.016 | 0.307 |
| Triglyceride (mg/dL) | 0.099 | 0.010 | 0.422 |
| LDL cholesterol (mg/dL) | 0.075 | 0.006 | 0.543 |
| HDL cholesterol (mg/dL) | −0.090 | 0.008 | 0.465 |
| Fasting plasma glucose (mg/dL) | −0.060 | 0.004 | 0.626 |
| Fasting plasma insulin (μU/mL) | 0.162 | 0.026 | 0.197 |
| HOMA-IR | 0.109 | 0.012 | 0.388 |
| HOMA- β (%) | −0.015 | 0.000 | 0.920 |
| HbA1c (%) | −0.089 | 0.008 | 0.472 |
| UACR (mg/g) | −0.252 | 0.064 | 0.038 |
| Multivariate Model | Fasting Plasma GLP-1 (pmol/L) | ||
| β | 95% CI | p-Value | |
| Fasting plasma glucose (mg/dL) | −0.002 ± 0.001 | −0.004–0.000 | 0.047 |
| UACR (mg/g) | −0.305 ± 0.133 | −0.571–0.038 | 0.026 |
| Fasting Plasma GLP-1 (pmol/L) | |||||
|---|---|---|---|---|---|
| Group L (<1.83) n = 34 | Group H * (1.83–3.32) n = 34 | p-Value | Decline of 1 pmol/L as a Continuous Variable | p-Value | |
| Model 1 | 2.987 (1.108–8.049) | 1 | 0.031 | 1.556 (1.003–1.802) | 0.049 |
| Model 2 | 3.121 (1.133–8.603) | 1 | 0.028 | 1.622 (1.091–1.843) | 0.030 |
| Model 3 | 3.410 (1.160–10.023) | 1 | 0.026 | 1.673 (1.173–1.870) | 0.018 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, C.-W.; Yu, T.Y.; Jeong, J.W.; Ha, S.E.; Singh, R.; Lee, M.Y.; Ro, S. Fasting GLP-1 Levels and Albuminuria Are Negatively Associated in Patients with Type 2 Diabetes Mellitus. J. Pers. Med. 2024, 14, 280. https://doi.org/10.3390/jpm14030280
Jang C-W, Yu TY, Jeong JW, Ha SE, Singh R, Lee MY, Ro S. Fasting GLP-1 Levels and Albuminuria Are Negatively Associated in Patients with Type 2 Diabetes Mellitus. Journal of Personalized Medicine. 2024; 14(3):280. https://doi.org/10.3390/jpm14030280
Chicago/Turabian StyleJang, Cheol-Won, Tae Yang Yu, Jin Woo Jeong, Se Eun Ha, Rajan Singh, Moon Young Lee, and Seungil Ro. 2024. "Fasting GLP-1 Levels and Albuminuria Are Negatively Associated in Patients with Type 2 Diabetes Mellitus" Journal of Personalized Medicine 14, no. 3: 280. https://doi.org/10.3390/jpm14030280