

Incidence of Tracheal Stenosis in ICU Hospitalized COVID-19 Patients: Results from a Prospective, Observational, Multicenter Study

 , , , , , , , , , , ,
, , , , , , , , , , ,  , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Design and Setting
2.2. Follow-Up Strategies
2.3. Study Endpoints
2.4. Ethical Review of the Study
2.5. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
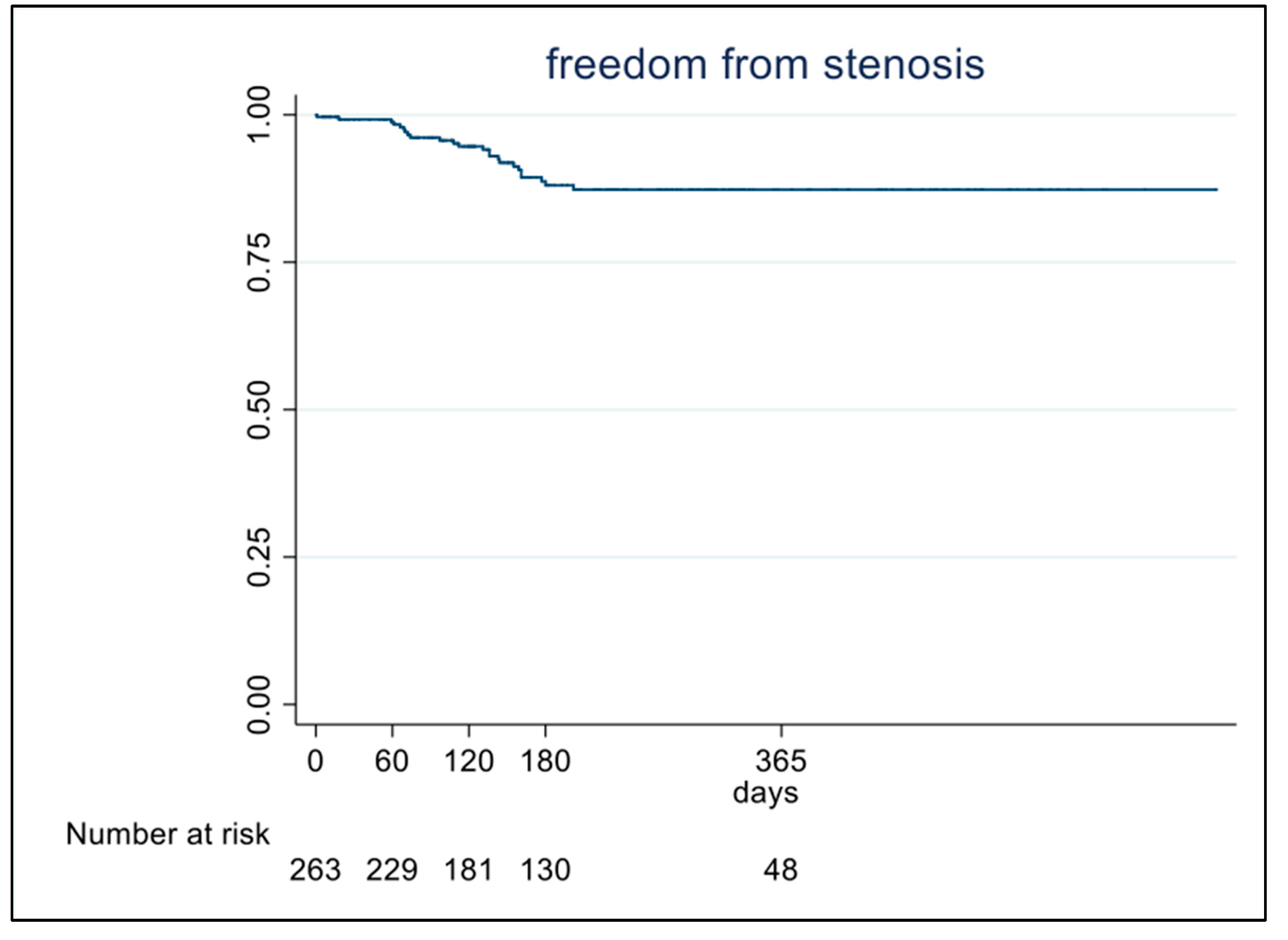
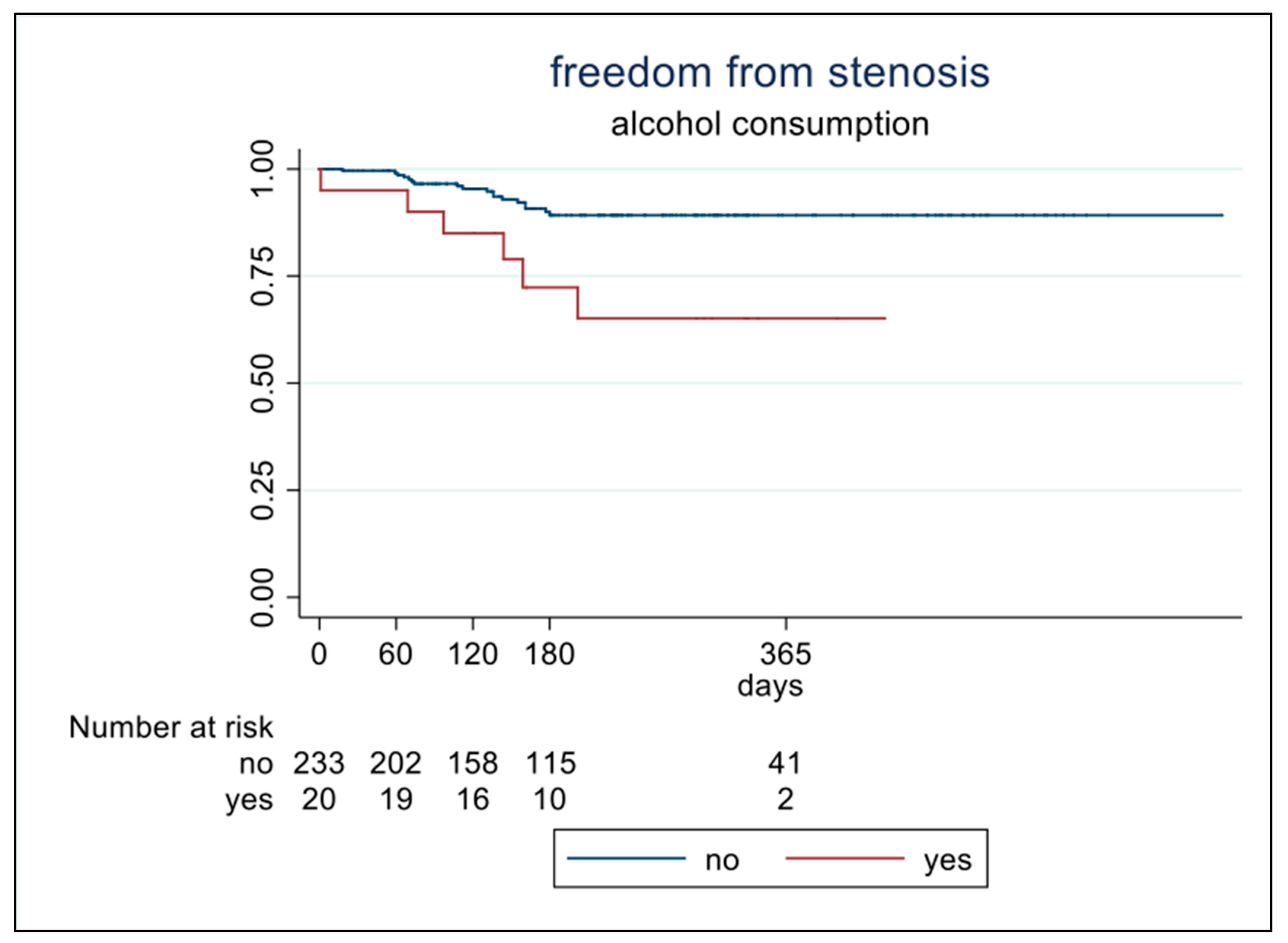
3.2. Follow-Up Period
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ADVS | Airway-Dyspnea-Voice-Swallow |
| CT | computed tomography |
| EDI | expiratory disproportion index |
| FEVI | forced expiratory volume in 1 s |
| ICU | intensive care unit |
| PEFR | peak expiratory flow rate |
| PFT | pulmonary function testing |
References
- Nouraei, S.A.R.; Ma, E.; Patel, A.; Howard, D.J.; Sandhu, G.S. Estimating the population incidence of adult post-intubation laryngotracheal stenosis. Clin. Otolaryngol. 2007, 32, 411–412. [Google Scholar] [CrossRef]
- Piazza, C.; Filauro, M.; Dikkers, F.G.; Nouraei, S.A.R.; Sandu, K.; Sittel, C.; Amin, M.R.; Campos, G.; Eckel, H.E.; Peretti, G. Long-term intubation and high rate of tracheostomy in COVID-19 patients might determine an unprecedented increase of airway stenoses: A call to action from the European Laryngological Society. Eur. Arch. Oto-Rhino-Laryngol. 2020, 278, 1–7. [Google Scholar] [CrossRef]
- Scholfield, D.W.; Warner, E.; Ahmed, J.; Ghufoor, K. Subglottic and tracheal stenosis associated with coronavirus disease 2019. J. Laryngol. Otol. 2021, 135, 656–658. [Google Scholar] [CrossRef] [PubMed]
- Bradley, B.T.; Maioli, H.; Johnston, R.; Chaudhry, I.; Fink, S.L.; Xu, H.; Najafian, B.; Deutsch, G.; Lacy, J.M.; Williams, T.; et al. Histopathology and ultrastructural findings of fatal COVID-19 infections in Washington State: A case series. Lancet 2020, 396, 320–332. [Google Scholar] [CrossRef] [PubMed]
- Magro, C.; Mulvey, J.J.; Berlin, D.; Nuovo, G.; Salvatore, S.; Harp, J.; Baxter-Stoltzfus, A.; Laurence, J. Complement associated microvascular injury and thrombosis in the pathogenesis of severe COVID-19 infection: A report of five cases. Transl. Res. 2020, 220, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Wright, F.L.; Vogler, T.O.; Moore, E.E.; Moore, H.B.; Wohlauer, M.V.; Urban, S.; Nydam, T.L.; Moore, P.K.; McIntyre, R.C. Fibrinolysis Shutdown Correlation with Thromboembolic Events in Severe COVID-19 Infection. J. Am. Coll. Surg. 2020, 231, 193–203.e1. [Google Scholar] [CrossRef] [PubMed]
- Minonishi, T.; Kinoshita, H.; Hirayama, M.; Kawahito, S.; Azma, T.; Hatakeyama, N.; Fujiwara, Y. The supine-to-prone position change induces modification of endotracheal tube cuff pressure accompanied by tube displacement. J. Clin. Anesth. 2013, 25, 28–31. [Google Scholar] [CrossRef]
- Botta, M.; Tsonas, A.M.; Pillay, J.; Boers, L.S.; Algera, A.G.; Bos, L.D.J.; Dongelmans, D.A.; Hollmann, M.W.; Horn, J.; Vlaar, A.P.J.; et al. Ventilation management and clinical outcomes in invasively ventilated patients with COVID-19 (PRoVENT-COVID): A national, multicentre, observational cohort study. Lancet Respir. Med. 2020, 9, 139–148. [Google Scholar] [CrossRef]
- Rhen, T.; Cidlowski, J.A. Antiinflammatory Action of Glucocorticoids—New Mechanisms for Old Drugs. N. Engl. J. Med. 2005, 353, 1711–1723. [Google Scholar] [CrossRef]
- Vogelhut, M.M.; Downs, J.B. Prolonged endotracheal intubation. Chest 1979, 76, 110–111. [Google Scholar] [CrossRef]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed]
- Calamari, K.; Politano, S.; Matrka, L. Does the Expiratory Disproportion Index Remain Predictive of Airway Stenosis in Obese Patients? Laryngoscope 2021, 131, 606–609. [Google Scholar] [CrossRef] [PubMed]
- Myer, C.M.; O’connor, D.M.; Cotton, R.T. Proposed grading system for subglottic stenosis based on endotracheal tube sizes. Ann. Otol. Rhinol. Laryngol. 1994, 103, 319–323. [Google Scholar] [CrossRef] [PubMed]
- George, S.C.; Hlastala, M.P.; Souders, J.E.; Babb, A.L. Gas exchange in the airways. J. Aerosol Med. Depos. Clear. Eff. Lung 1996, 9, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Forgèt, M.A.; Sisson, J.H.; Spurzem, J.R.; Wyatt, T.A. Ethanol increases phosphodiesterase 4 activity in bovine bronchial epithelial cells. Alcohol 2003, 31, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Rosa, D.F.; Sarandy, M.M.; Novaes, R.D.; Freitas, M.B.; do Carmo Gouveia Pelúzio, M.; Gonçalves, R.V. High-fat diet and alcohol intake promotes inflammation and impairs skin wound healing in Wistar rats. Mediat. Inflamm. 2018, 2018, 4658583. [Google Scholar] [CrossRef] [PubMed]
- Pappal, R.B.; Burruss, C.P.; Witt, M.A.; Harryman, C.; Ali, S.Z.; Bush, M.L.; Fritz, M.A. Risk factors for developing subglottic and tracheal stenosis from the medical intensive care unit. Laryngoscope Investig. Otolaryngol. 2023, 8, 699–707. [Google Scholar] [CrossRef] [PubMed]
- Sun, K.; Zhang, H.; Zhang, W.; Cheng, Y.; Wang, G. Long-term prognostic factors of clinical success after interventional bronchoscopy in patients with scarring central airway stenosis. BMC Pulm. Med. 2021, 21, 73. [Google Scholar] [CrossRef]
- Kanlikama, M.; Celenk, F.; Gonuldas, B.; Gulsen, S. Cervical Tracheal Resection and Anastomosis for Postintubation Tracheal Stenosis. J. Craniofac. Surg. 2018, 29, e578–e582. [Google Scholar] [CrossRef]
- Mangiameli, G.; Perroni, G.; Costantino, A.; De Virgilio, A.; Malvezzi, L.; Mercante, G.; Giudici, V.M.; Ferraroli, G.M.; Voulaz, E.; Giannitto, C.; et al. Analysis of Risk Factors for Tracheal Stenosis Managed during COVID-19 Pandemic: A Retrospective, Case-Control Study from Two European Referral Centre. J. Pers. Med. 2023, 13, 729. [Google Scholar] [CrossRef]
- Sarper, A.; Ayten, A.; Eser, I.; Ozbudak, O.; Demircan, A. Tracheal stenosis after tracheostomy or intubation: Review with special regard to cause and management. Texas Hear. Inst. J. 2005, 32, 154–158. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1163461/ (accessed on 5 January 2023).
- Putensen, C.; Theuerkauf, N.; Guenther, U.; Vargas, M.; Pelosi, P. Percutaneous and surgical tracheostomy in critically ill adult patients: A meta-analysis. Crit. Care 2014, 18, 544. [Google Scholar] [CrossRef] [PubMed]
- Brascia, D.; De Palma, A.; Cantatore, M.G.; Pizzuto, O.; Signore, F.; Sampietro, D.; Valentini, M.; Genualdo, M.; Marulli, G. Not only acute respiratory failure: COVID-19 and the post-intubation/tracheostomy upper airways lesions. Front Surg. 2023, 10, 1150254. [Google Scholar] [CrossRef] [PubMed]
- Bacchin, D.; Aprile, V.; Lenzini, A.; Korasidis, S.; Mastromarino, M.G.; Picchi, A.; Fanucchi, O.; Ribechini, A.; Ambrogi, M.C.; Lucchi, M. Surgical treatment of tracheal stenosis during COVID-19 era: A single-center experience and lessons learnt on the field. Updates Surg. 2023, 75, 1681–1690. [Google Scholar] [CrossRef] [PubMed]
- Conforti, S.; Licchetta, G.; Reda, M.; Astaneh, A.; Pogliani, L.; Fieschi, S.; Rinaldo, A.; Torre, M. Management of COVID-19-related post-intubation tracheal stenosis. Front. Surg. 2023, 10, 1129803. [Google Scholar] [CrossRef] [PubMed]
- Orlandi, R.; Raveglia, F.; Calderoni, M.; Cassina, E.M.; Cioffi, U.; Guttadauro, A.; Libretti, L.; Pirondini, E.; Rimessi, A.; Tuoro, A.; et al. Management of COVID-19 related tracheal stenosis: The state of art. Front. Surg. 2023, 10, 1118477. [Google Scholar] [CrossRef] [PubMed]
- Beyoglu, M.A.; Sahin, M.F.; Turkkan, S.; Yazicioglu, A.; Yekeler, E. Complex Post-intubation Tracheal Stenosis in COVID-19 Patients. Indian J. Surg. 2022, 84, 805–813. [Google Scholar] [CrossRef]
- Piazza, C.; Lancini, D.; Filauro, M.; Sampieri, C.; Bosio, P.; Zigliani, G.; Ioppi, A.; Vallin, A.; Deganello, A.; Peretti, G. Post-COVID-19 airway stenosis treated by tracheal resection and anastomosis: A bicentric experience. Acta Otorhinolaryngol. Ital. 2022, 42, 99–105. [Google Scholar] [CrossRef]
- Nouraei, S.A.; Nouraei, S.M.; Patel, A.; Murphy, K.; Giussani, D.A.; Koury, E.F.; Brown, J.M.; George, P.J.; Cummins, A.C.; Sandhu, G.S. Diagnosis of laryngotracheal stenosis from routine pulmonary physiology using the expiratory disproportion index. Laryngoscope 2013, 123, 3099–3104. [Google Scholar] [CrossRef]
- Schuering, J.H.C.; Halperin, I.J.Y.; Ninaber, M.K.; Willems, L.N.A.; van Benthem, P.P.G.; Sjögren, E.V.; Langeveld, A.P.M. The diagnostic accuracy of spirometry as screening tool for adult patients with a benign subglottic stenosis. BMC Pulm. Med. 2023, 23, 314. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patients (n = 281) | ||
|---|---|---|
| Age, Years | 61 (±10) | |
| Gender (Male), n (%) | 225 (80%) | |
| Smoking status, n (%) | Never | 176 (63%) |
| Former | 65 (23%) | |
| Current | 28 (10%) | |
| N/A | 12 (4.3%) | |
| Alcohol use, n (%) | No | 245 (87%) |
| Yes | 21 (7.5%) | |
| N/A | 15 (5.5%) | |
| GERD, n (%) | 21 (7.5%) | |
| Diabetes, n (%) | No | 161 (57%) |
| Type I | 62 (22%) | |
| Type II | 56 (20%) | |
| N/A | 2 (0.7%) | |
| COPD/Asthma, n (%) | 44 (16%) | |
| Stenosis, n (%) | 24 (8.5%) | |
| Stenosis grade, n (%) | I | 17 (71%) |
| II | 4 (17%) | |
| III | 1 (4%) | |
| IV | 2 (8%) | |
| Stenosis (n = 24) | No Stenosis (n = 257) | OR (95%CI) | p-Value | |
|---|---|---|---|---|
| Male sex, n (%) | 18 (75%) | 207 (81%) | 0.72 (0.27–1.9) | 0.53 |
| Age (mean, SD) | 61 ± 9.7 | 62 ± 11 | 1.01 (0.97–1.1) | 0.67 |
| BMI (mean, SD) | 27.7 ± 5.1 | 29.7 ± 6.1 | 1.07 (0.99–1.1) | 0.074 |
| Smoking status (n = 245) | ||||
| Never, n (%) | 16 (67%) | 160 (65%) | 1 | |
| Former, n (%) | 7 (29%) | 58 (24%) | 1.2 (0.47–3.1) | 0.69 |
| Current, n (%) | 1 (4.2%) | 27 (11%) | 0.37 (0.05–2.9) | 0.35 |
| Alcohol consumer, n (%) | 6 (25%) | 14 (5.8%) | 5.4 (1.9–16) | 0.002 |
| Alcohol units (mean, SD) | 0.75 ± 1.7 | 0.10 ± 0.57 | 1.7 (1.2–2.5) | 0.005 |
| GERD, n (%) | 1 (4.2%) | 20/255 (7.9%) | 0.51 (0.07–4.0) | 0.52 |
| Diabetes (n = 255) | ||||
| No, n (%) | 12 (50%) | 149 (58%) | 1 | |
| Type I, n (%) | 3 (13%) | 59 (23%) | 0.63 (0.17–2.3) | 0.49 |
| Type II, n (%) | 9 (38%) | 47 (18%) | 2.4 (0.94–6.0) | 0.066 |
| COPD, n (%) | 2 (8.3%) | 22/255 (8.6%) | 0.96 (0.21–4.4) | 0.96 |
| Asthma, n (%) | 2 (8.3%) | 18/255 (7.1%) | 1.2 (0.26–5.5) | 0.82 |
| Stenosis (n = 24) | No Stenosis (n = 257) | p-Value | |
|---|---|---|---|
| Days from admission to intubation (median, range) | 2 (0–9) | 2 (0–366) | 0.689 |
| Days of intubation (median, range) | 24 ± 16 | 23 ± 17 | 0.527 |
| Tracheostomy performed (count, percentage) | 18 (75%) | 134 (52%) | 0.034 |
| Days of tracheostomy (median, range) | 34 (5–168) | 29 (4–126) | 0.125 |
| Stenosis (n = 24) | No Stenosis (n = 257) | p-Value | |
|---|---|---|---|
| EDI | 45 ± 13 (n = 18) | 39 ± 9.9 (n = 142) | 0.025 |
| Dyspnea | 18/31 (58%) | 107/377 (28%) | 0.001 |
| Voice change | 9/30 (30%) | 38/377 (10%) | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perroni, G.; Radovanovic, D.; Mondoni, M.; Mangiameli, G.; Giudici, V.M.; Crepaldi, A.; Giatti, V.; Morenghi, E.; Stella, G.M.; Pavesi, S.; et al. Incidence of Tracheal Stenosis in ICU Hospitalized COVID-19 Patients: Results from a Prospective, Observational, Multicenter Study. J. Pers. Med. 2024, 14, 39. https://doi.org/10.3390/jpm14010039
Perroni G, Radovanovic D, Mondoni M, Mangiameli G, Giudici VM, Crepaldi A, Giatti V, Morenghi E, Stella GM, Pavesi S, et al. Incidence of Tracheal Stenosis in ICU Hospitalized COVID-19 Patients: Results from a Prospective, Observational, Multicenter Study. Journal of Personalized Medicine. 2024; 14(1):39. https://doi.org/10.3390/jpm14010039
Chicago/Turabian StylePerroni, Gianluca, Dejan Radovanovic, Michele Mondoni, Giuseppe Mangiameli, Veronica Maria Giudici, Alessandro Crepaldi, Valentina Giatti, Emanuela Morenghi, Giulia Maria Stella, Stefano Pavesi, and et al. 2024. "Incidence of Tracheal Stenosis in ICU Hospitalized COVID-19 Patients: Results from a Prospective, Observational, Multicenter Study" Journal of Personalized Medicine 14, no. 1: 39. https://doi.org/10.3390/jpm14010039