
Real-Life Effects of Omalizumab on Chronic Rhinosinusitis with Nasal Polyposis
 ,
,  , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Definition of Criteria for Enrollment of Patients to Be Treated with Omalizumab
2.2. Nasal Polyps Score (NPS)
2.3. Sino-Nasal Outcome Test (SNOT-22)
2.4. Nasal Congestion Score (NCS)
2.5. Numeric Rating Scale (NRS)
2.6. Statistical Analysis
3. Results
3.1. Gender and Age Distribution in Patients with CRSwNP
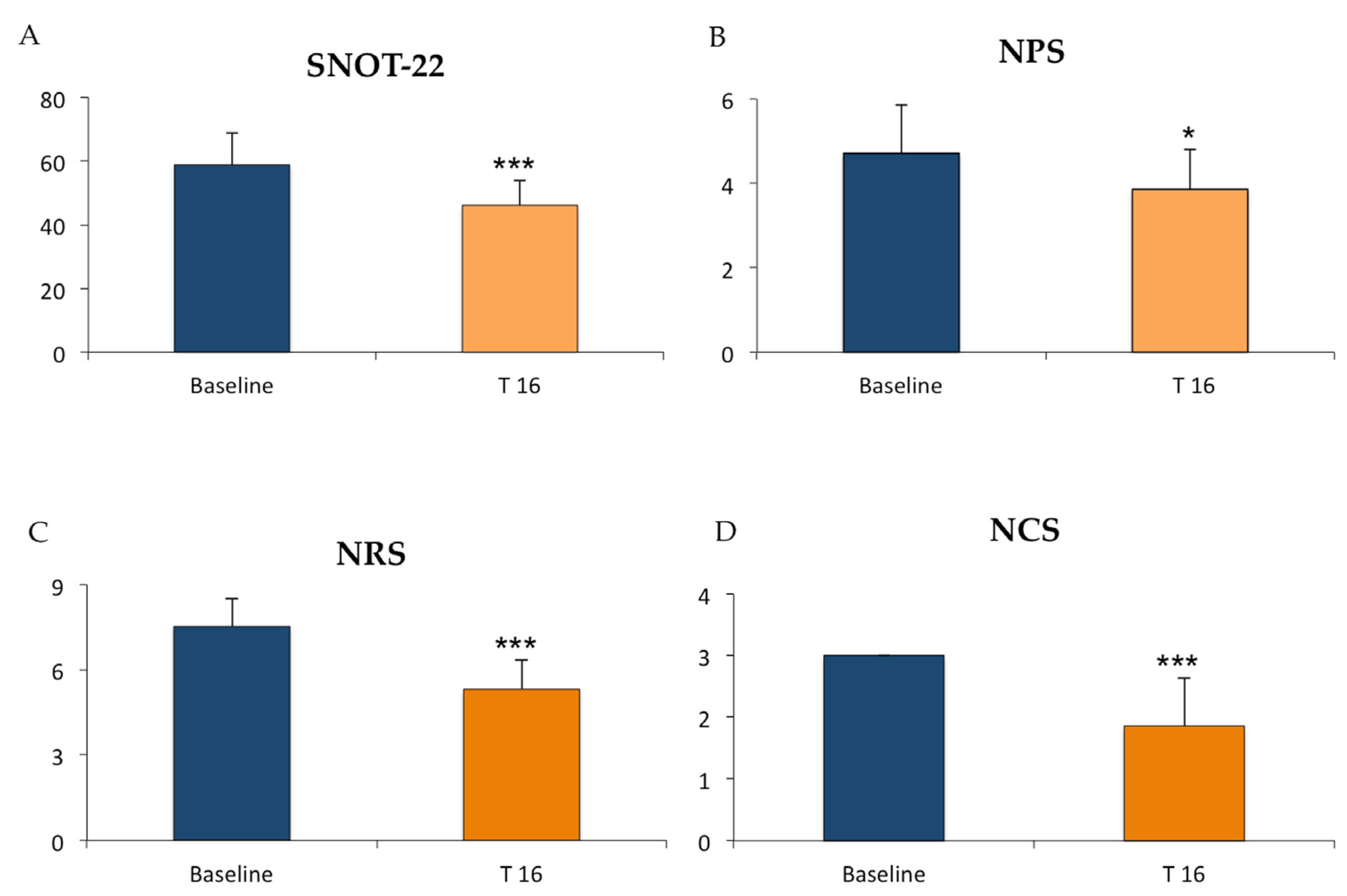
3.2. Omalizumab Improved the SNOT-22, NPS, NRS, and NCS Parameters in Patients with CRSwNP
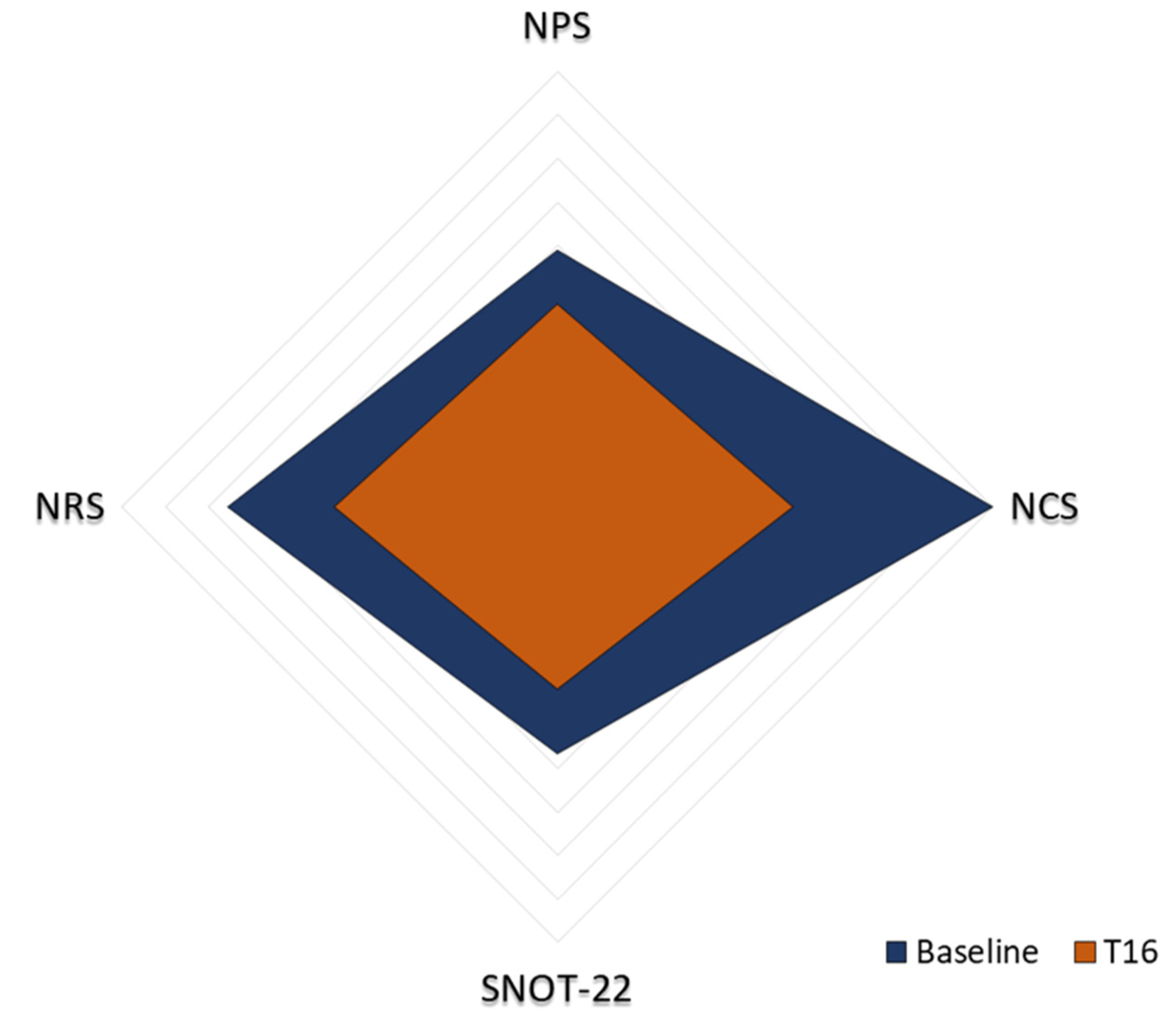
3.3. Radar Graph Representation of the SNOT-22, NPS, NRS, and NCS Parameters in Patients with CRSwNP
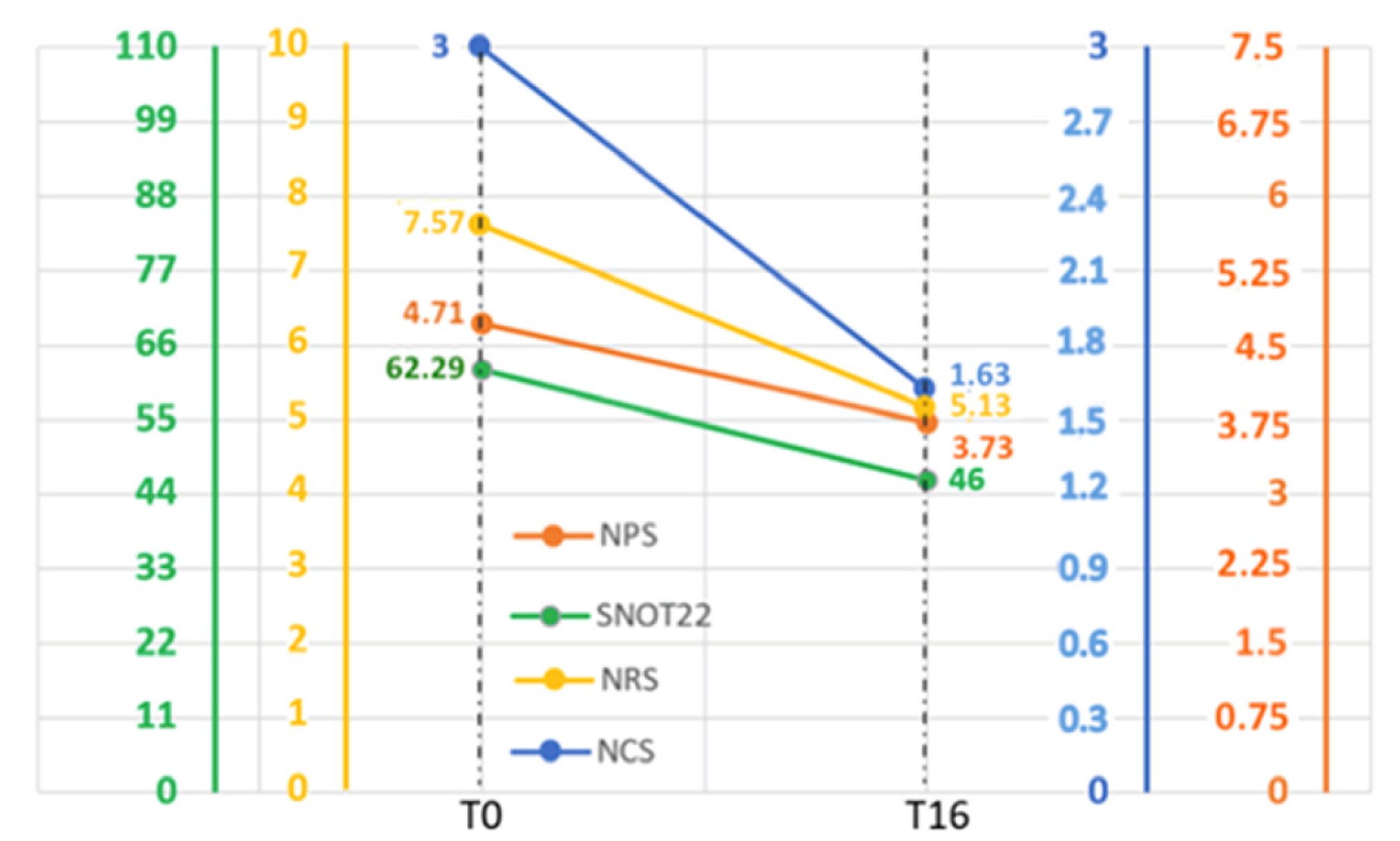
3.4. Analysis of the SNOT-22, NPS, NRS, and NCS Parameters’ Variations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CRSwNP | CRS with nasal polyps |
| CRSsNP | CRS without nasal polyps |
| EPOS | European Position Paper on Rhinosinusitis and Nasal Polyps |
| ENT | Ear, nose, and throat |
| NPS | Nasal polyp score |
| SNOT-22 | Sino-Nasal Outcome Test |
| NRS | Numeric Rating Scale |
| NCS | Nasal congestion score |
| CRS | Chronic rhinosinusitis |
| EMT | Epithelial-to-mesenchymal transition |
| CT | Computed tomography |
| AERD | Aspirin-exacerbated respiratory disease |
| FESS | Functional endoscopic sinus surgery |
| QoL | Quality of life |
| CDRs | Complementarity-determining regions |
| NSAIDs | Nonsteroidal anti-inflammatory drugs |
| VAS | Visual analogue scale |
| ESS | Endoscopic sinus surgery |
References
- Giunta, G.; Pirola, F.; Giombi, F.; Muci, G.; Pace, G.M.; Heffler, E.; Paoletti, G.; Puggioni, F.; Cerasuolo, M.; Ferreli, F.; et al. Care for Patients with Type-2 Chronic Rhinosinusitis. J. Pers. Med. 2023, 13, 618. [Google Scholar] [CrossRef] [PubMed]
- Chiarella, E.; Lombardo, N.; Lobello, N.; Aloisio, A.; Aragona, T.; Pelaia, C.; Scicchitano, S.; Bond, H.M.; Mesuraca, M. Nasal Polyposis: Insights in Epithelial-Mesenchymal Transition and Differentiation of Polyp Mesenchymal Stem Cells. Int. J. Mol. Sci. 2020, 21, 6878. [Google Scholar] [CrossRef] [PubMed]
- Chiarella, E.; Lombardo, N.; Lobello, N.; Piazzetta, G.L.; Morrone, H.L.; Mesuraca, M.; Bond, M.B. Deficit in Adipose Differentiation in Mesenchymal Stem Cells Derived from Chronic Rhinosinusitis Nasal Polyps Compared to Nasal Mucosal Tissue. Int. J. Mol. Sci. 2020, 21, 9214. [Google Scholar] [CrossRef] [PubMed]
- Mesuraca, M.; Nisticò, C.; Lombardo, N.; Piazzetta, G.L.; Lobello, N.; Chiarella, E. Cellular and Biochemical Characterization of Mesenchymal Stem Cells from Killian Nasal Polyp. Int. J. Mol. Sci. 2022, 23, 13214. [Google Scholar] [CrossRef] [PubMed]
- Hong, H.; Dan, W.; Kai, S.T.; Rui, Z.; Fenghong, C.; Wenxiang, G.; Haixin, H.; Jianbo, S.; Yunping, F.; Qintai, Y.; et al. Sinus computed tomography predicts clinical response to corticosteroids in chronic rhinosinusitis with nasal polyps. Clin. Transl. Allergy 2018, 8, 24. [Google Scholar] [CrossRef]
- Vennik, J.; Eyles, C.; Thomas, M.; Hopkins, C.; Little, P.; Blackshaw, H.; Schilder, A.; Savage, I.; Philpott, C.M. Chronic rhinosinusitis: A qualitative study of patient views and experiences of current management in primary and secondary care. BMJ Open 2019, 9, e022644. [Google Scholar] [CrossRef]
- Gliklich, R.E.; Metson, R. The health impact of chronic sinusitis in patients seeking otolaryngologic care. Otolaryngol. Head Neck Surg. 1995, 113, 104–109. [Google Scholar] [CrossRef]
- Stevens, W.W.; Schleimer, R.P.; Kern, R.C. Chronic Rhinosinusitis with Nasal Polyps. J. Allergy Clin. Immunol. Pract. 2016, 4, 565–572. [Google Scholar] [CrossRef]
- Macchi, A.; Giorli, A.; Cantone, E.; Pipolo, C.G.; Arnone, F.; Barbone, U.; Bertazzoni, G.; Bianchini, C.; Ciofalo, A.; Cipolla, F.; et al. Sense of smell in chronic rhinosinusitis: A multicentric study on 811 patients. Front. Allergy 2023, 4, 1083964. [Google Scholar] [CrossRef]
- Kato, A.; Peters, A.T.; Stevens, W.W.; Schleimer, R.P.; Tan, B.K.; Kern, R.C. Endotypes of chronic rhinosinusitis: Relationships to disease phenotypes, pathogenesis, clinical findings, and treatment approaches. Allergy 2022, 77, 812–826. [Google Scholar] [CrossRef]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology 2020, 58 (Suppl. S29), 1–464. [Google Scholar] [CrossRef] [PubMed]
- Stevens, W.W.; Peters, A.T.; Suh, L.; Norton, E.J.; Kern, R.C.; Conley, D.B.; Chandra, R.K.; Tan, B.K.; Grammer, L.C.; Harris, K.E.; et al. A retrospective, cross-sectional study reveals that women with CRSwNP have more severe disease than men. Immun. Inflamm. Dis. 2020, 3, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.K.; Chandra, R.K.; Pollak, J.; Kato, A.; Conley, D.B.; Peters, A.T.; Grammer, L.C.; Avila, P.C.; Kern, R.C.; Stewart, W.F.; et al. Incidence and associated premorbid diagnoses of patients with chronic rhinosinusitis. J. Allergy Clin. Immunol. 2013, 131, 1350–1360. [Google Scholar] [CrossRef] [PubMed]
- Promsopa, C.; Kansara, S.; Citardi, M.J.; Fakhri, S.; Porter, P.; Luong, A. Prevalence of confirmed asthma varies in chronic rhinosinusitis subtypes. Int. Forum Allergy Rhinol. 2016, 6, 373–377. [Google Scholar] [CrossRef] [PubMed]
- Walters, B.K.; Hagan, J.B.; Divekar, R.D.; Willson, T.J.; Stokken, J.K.; Pinheiro-Neto, C.D.; O’Brien, E.K.; Choby, G. Aspirin-Exacerbated Respiratory Disease and the Unified Airway: A Contemporary Review. Otolaryngol. Clin. North Am. 2023, 56, 107–124. [Google Scholar] [CrossRef] [PubMed]
- Peters, A.T.; Spector, S.; Hsu, J.; Hamilos, D.L.; Baroody, F.M.; Chandra, R.K.; Grammer, L.C.; Kennedy, D.W.; Cohen, N.A.; Kaliner, M.A.; et al. Diagnosis and management of rhinosinusitis: A practice parameter update. Ann. Allergy Asthma Immunol. 2014, 113, 347–385. [Google Scholar] [CrossRef] [PubMed]
- Blaiss, M.S. Chronic rhinosinusitis with nasal polyps management in the age of biologics. Allergy Asthma Proc. 2020, 41, 413–419. [Google Scholar] [CrossRef]
- Selvarajah, J.; Saim, A.B.; Bt Hj Idrus, R.; Lokanathan, Y. Current and Alternative Therapies for Nasal Mucosa Injury: A Review. Int. J. Mol. Sci. 2020, 21, 480. [Google Scholar] [CrossRef]
- Orlandi, R.R.; Kingdom, T.T.; Smith, T.L.; Bleier, B.; DeConde, A.; Luong, A.U.; Poetker, D.M.; Soler, Z.; Welch, K.C.; Wise, S.K.; et al. International Consensus Statement on Allergy and Rhinology: Rhinosinusitis. Int. Forum Allergy Rhinol. 2021, 11, 213–739. [Google Scholar] [CrossRef]
- Weber, R.K. Comprehensive review on endonasal endoscopic sinus surgery. Laryngo-Rhino-Otologie 2015, 94, S64–S142. [Google Scholar] [CrossRef]
- De Corso, E.; Bellocchi, G.; De Benedetto, M.; Lombardo, N.; Macchi, A.; Malvezzi, L.; Motta, G.; Pagella, F.; Vicini, C.; Passali, D. Biologics for severe uncontrolled chronic rhinosinusitis with nasal polyps: A change management approach. Consensus of the Joint Committee of Italian Society of Otorhinolaryngology on biologics in rhinology. Acta Otorhinolaryngol. Ital. 2022, 42, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Patel, G.B.; Peters, A.T. The Role of Biologics in Chronic Rhinosinusitis with Nasal Polyps. Ear. Nose Throat J. 2021, 100, 44–47. [Google Scholar] [CrossRef] [PubMed]
- De Corso, E.; Pipolo, C.; Cantone, E.; Ottaviano, G.; Gallo, S.; Trimarchi, M.; Torretta, S.; Cavaliere, C.; Lucidi, D.; Seccia, V.; et al. Practical recommendations for managing severe chronic rhinosinusitis with nasal polyps in the era of biologics. Acta Otorhinolaryngol. Ital. 2023, 43, 324–340. [Google Scholar] [CrossRef] [PubMed]
- Bachert, C.; Desrosiers, C.M.Y.; Hellings, P.W.; Laidlaw, T.M. The Role of Biologics in Chronic Rhinosinusitis with Nasal Polyps. J. Allergy Clin. Immunol. Pract. 2020, 9, 1099–1106. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Kim, T.H. Fundamental role of dendritic cells in inducing Th2 responses. Korean J. Intern. Med. 2018, 33, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Bachert, C.; Bhattacharyya, N.; Desrosiers, M.; Khan, A.H. Burden of Disease in Chronic Rhinosinusitis with Nasal Polyps. J. Asthma Allergy 2021, 14, 127–134. [Google Scholar] [CrossRef]
- De Corso, E.; Settimi, S.; Montuori, C.; Cantiani, A.; Corbò, M.; Di Bella, G.A.; Sovardi, F.; Pagella, F.; Rigante, M.; Passali, G.C.; et al. How to manage recurrences after surgery in CRSwNP patients in the biologic era: A narrative review. Acta Otorhinolaryngol. Ital. 2023, 43, S3–S13. [Google Scholar] [CrossRef]
- Kim, S.D.; Cho, K.S. Treatment Strategy of Uncontrolled Chronic Rhinosinusitis with Nasal Polyps: A Review of Recent Evidence. Int. J. Mol. Sci. 2023, 24, 5015. [Google Scholar] [CrossRef]
- Liu, P.; Pan, Z.; Gu, C.; Cao, X.; Liu, X.; Zhang, J.; Xiao, Z.; Wang, X.; Guo, H.; Ju, D.; et al. An Omalizumab Biobetter Antibody with Improved Stability and Efficacy for the Treatment of Allergic Diseases. Front. Immunol. 2020, 11, 596908. [Google Scholar] [CrossRef]
- Lowe, P.J.; Renard, D. Omalizumab decreases IgE production in patients with allergic (IgE-mediated) asthma; PKPD analysis of a biomarker, total IgE. Br. J. Clin. Pharmacol. 2011, 72, 306–320. [Google Scholar] [CrossRef]
- Kumar, C.; Zito, P.M. Omalizumab. In StatPearls; StatPearls Publishing: St. Petersburg, FL, USA, 2023. [Google Scholar]
- Serrano-Candelas, E.; Martinez-Aranguren, R.; Valero, A.; Bartra, J.; Gastaminza, G.; Goikoetxea, M.J.; Martín, M.; Ferrer, M. Comparable actions of Omalizumab on mast cells and basophils. Clin. Exp. Allergy 2016, 46, 92–102. [Google Scholar] [CrossRef] [PubMed]
- Kariyawasam, H.H.; James, L.K. Chronic Rhinosinusitis with Nasal Polyps: Targeting IgE with Anti-IgE Omalizumab Therapy. Drug Des. Dev. Ther. 2020, 14, 5483–5494. [Google Scholar] [CrossRef] [PubMed]
- Tandon, M.; Singh, A.; Saluja, V.; Dhankhar, M.; Pandey, C.K.; Jain, P. Validation of a New “Objective Pain Score” vs. “Numeric Rating Scale” for the Evaluation of Acute Pain: A Comparative Study. Anesthesiol. Pain Med. 2016, 6, e32101. [Google Scholar] [CrossRef] [PubMed]
- Godse, K.; Mehta, A.; Patil, S.; Gautam, M.; Nadkarni, N. Omalizumab—A Review. Indian J. Dermatol. 2015, 60, 381–384. [Google Scholar] [CrossRef]
- Shiung, Y.Y.; Chiang, C.Y.; Chen, J.B.; Wu, P.C.; Alfur Fu-Hsin Hung, A.F.H.; Donic Chien-Sheng Lu, D.C.S.; Pan, R.L.; Chang, T.W. An anti-IgE monoclonal antibody that binds to IgE on CD23 but not on high-affinity IgE. Fc receptors. Immunobiology 2012, 217, 676–863. [Google Scholar] [CrossRef]
- Shen, Y.; Zhang, N.; Yang, Y.; Hong, S.; Bachert, C. Local Immunoglobulin E in nasal polyps: Role and modulation. Front. Immunol. 2022, 13, 961503. [Google Scholar] [CrossRef]
- Sponsor Hoffmann-La Roche. An Extension Study of Omalizumab in Participants with Chronic Rhinosinusitis with Nasal Polyps; ID NCT03478930; Hoffmann-La Roche: Basel, Switzerland, 2022. [Google Scholar]
- Ellen Dutta, M.D. Subcutaneous Omalizumab for Treatment of Chronic Rhinosinusitis with Nasal Polyposis; ID NCT01066104; Massachusetts General Hospital: Boston, MA, USA, 2017. [Google Scholar]
- Sponsor Hoffmann-La Roche. A Clinical Trial of Omalizumab in Participants with Chronic Rhinosinusitis with Nasal Polyps (POLYP 1); ID NCT03280550; Hoffmann-La Roche: Basel, Switzerland, 2020. [Google Scholar]
- Gevaert, P.; A Omachi, T.; Corren, J.; Mullol, J.; Han, J.; Lee, S.E.; Kaufman, D.; Ligueros-Saylan, M.; Howard, M.; Zhu, R.; et al. Efficacy and safety of Omalizumab in nasal polyposis: 2 randomized phase 3 trials. J. Allergy Clin. Immunol. 2020, 146, 595–605. [Google Scholar] [CrossRef]
- Damask, C.; Chen, M.; Holweg, C.T.J.; Yoo, B.; A Millette, L.; Franzese, C. Defining the Efficacy of Omalizumab in Nasal Polyposis: A POLYP 1 and POLYP 2 Subgroup Analysis. Am. J. Rhinol. Allergy 2022, 36, 135–141. [Google Scholar] [CrossRef]
- Maza-Solano, J.; Callejon-Leblic, A.; Martin-Jimenez, D.; Moreno-Luna, R.; Gonzalez-Garcia, J.; Cuvillo, A.; Sanchez-Gomez, S. Omalizumab Treatment in Uncontrolled Asthma and CRSwNP Patients, with Previous Endoscopic Sinus Surgery, to Improve Quality of Life and Endoscopic Outcomes: A Two-Year Real-Life Study. Curr. Allergy Asthma Rep. 2023, 23, 555–566. [Google Scholar] [CrossRef]
- Tat, T.S. Omalizumab is effective in nasal polyposis with or without asthma, a real-life study. World Allergy Organ. J. 2022, 15, 100670. [Google Scholar] [CrossRef]
- Piazzetta, G.L.; Lobello, N.; Chiarella, E.; Rizzuti, A.; Pelaia, C.; Pelaia, G.; Lombardo, N. Targeting IL-4 and IL-13 Receptors on Eosinophils in CRSwNP Patients: The Clinical Efficacy of Dupilumab. J. Pers. Med. 2023, 13, 1404. [Google Scholar] [CrossRef] [PubMed]
- Pelaia, C.; Lombardo, N.; Busceti, M.T.; Piazzetta, G.L.; Crimi, C.; Calabrese, C.; Vatrella, A.; Pelaia, G. Short-Term Evaluation of Dupilumab Effects in Patients with Severe Asthma and Nasal Polyposis. J. Asthma Allergy 2021, 14, 1165–1172. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lombardo, N.; Piazzetta, G.L.; Lobello, N.; Cicala, G.; Patafi, M.; Benincasa, A.T.; Pelaia, C.; Chiarella, E.; Pelaia, G. Real-Life Effects of Omalizumab on Chronic Rhinosinusitis with Nasal Polyposis. J. Pers. Med. 2024, 14, 3. https://doi.org/10.3390/jpm14010003
Lombardo N, Piazzetta GL, Lobello N, Cicala G, Patafi M, Benincasa AT, Pelaia C, Chiarella E, Pelaia G. Real-Life Effects of Omalizumab on Chronic Rhinosinusitis with Nasal Polyposis. Journal of Personalized Medicine. 2024; 14(1):3. https://doi.org/10.3390/jpm14010003
Chicago/Turabian StyleLombardo, Nicola, Giovanna Lucia Piazzetta, Nadia Lobello, Giuseppe Cicala, Maria Patafi, Anna Teresa Benincasa, Corrado Pelaia, Emanuela Chiarella, and Girolamo Pelaia. 2024. "Real-Life Effects of Omalizumab on Chronic Rhinosinusitis with Nasal Polyposis" Journal of Personalized Medicine 14, no. 1: 3. https://doi.org/10.3390/jpm14010003