
A Novel Sensor-Based Application for Home-Based Rehabilitation Can Objectively Measure Postoperative Outcomes following Anterior Cruciate Ligament Reconstruction
 , and
, and
Abstract
:1. Introduction
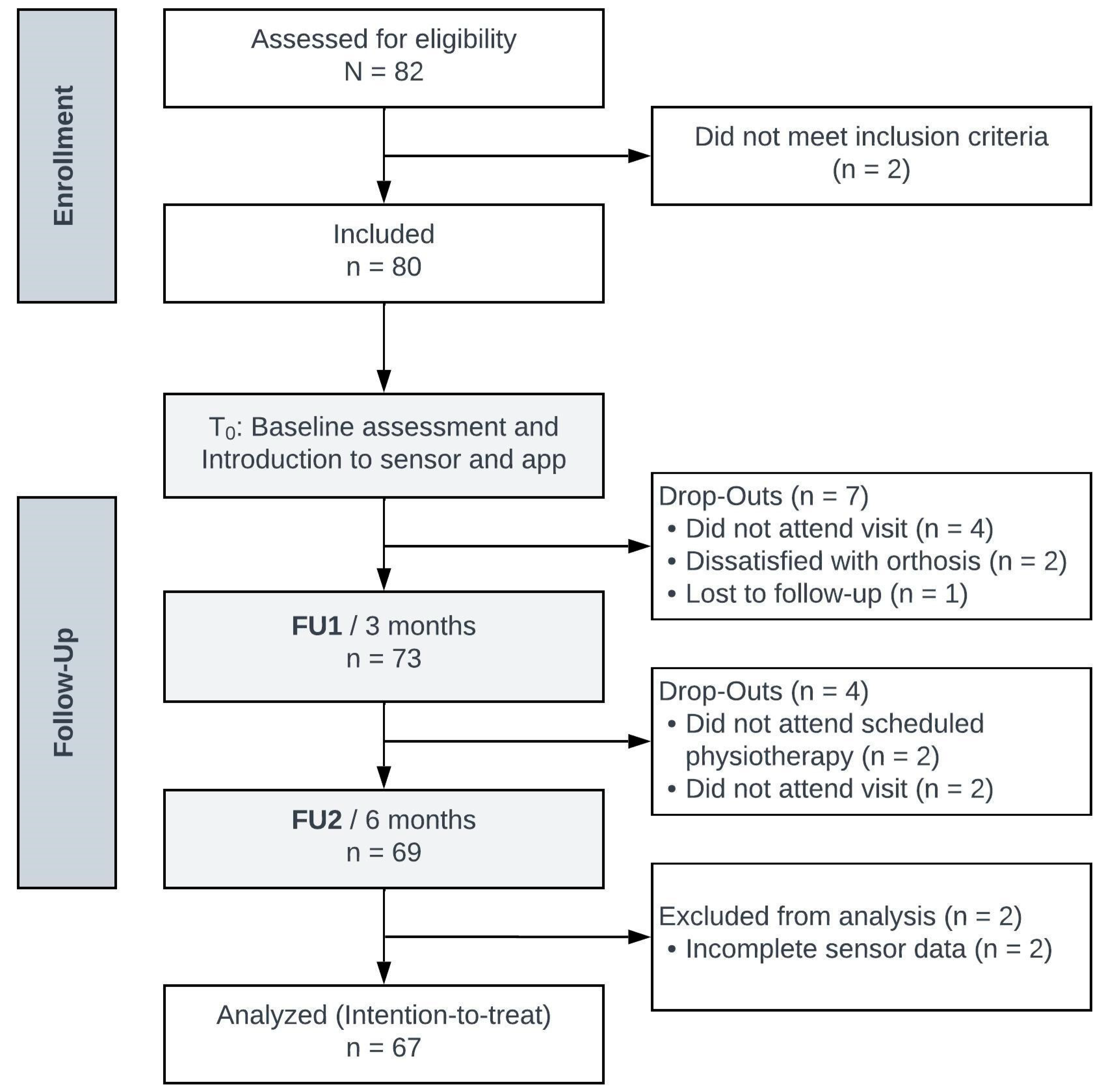
2. Materials and Methods
3. Results
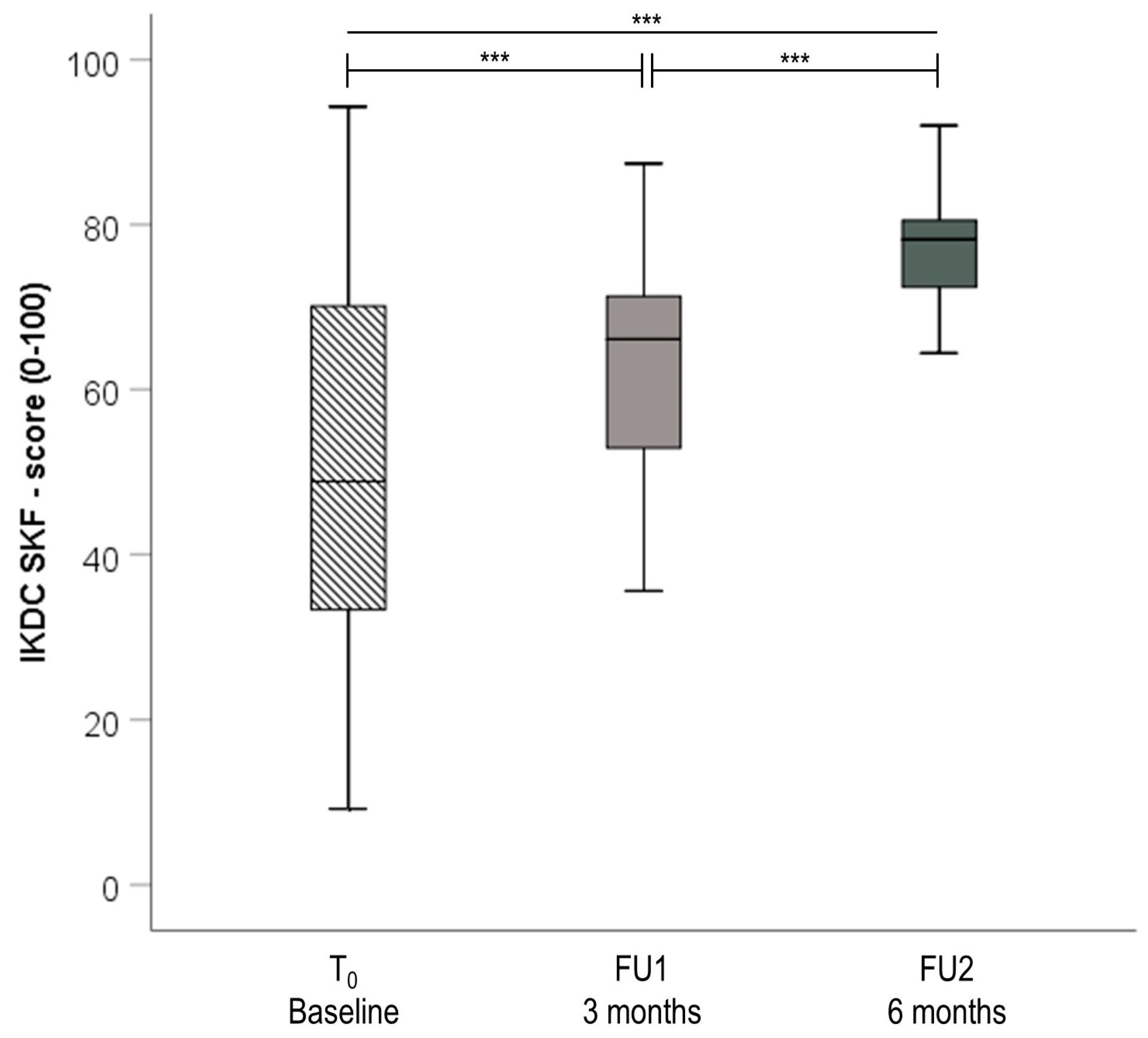
3.1. Patient-Reported Outcome Measures and Functional Assessment
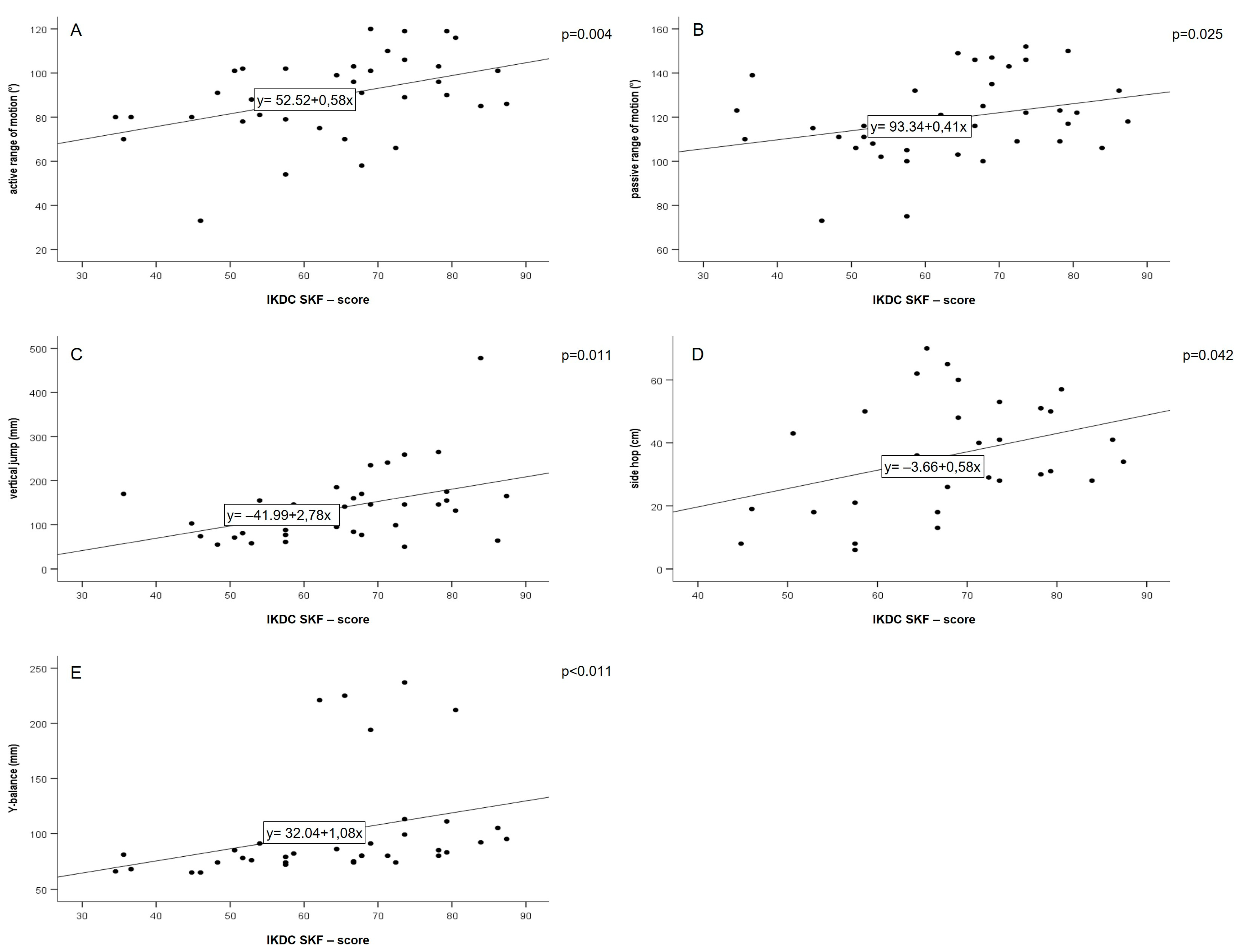
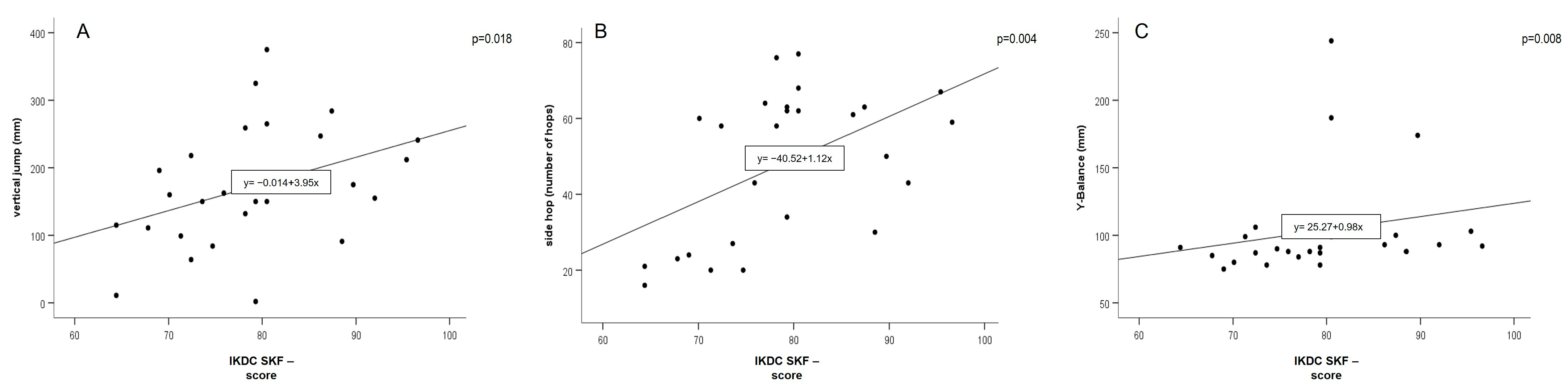
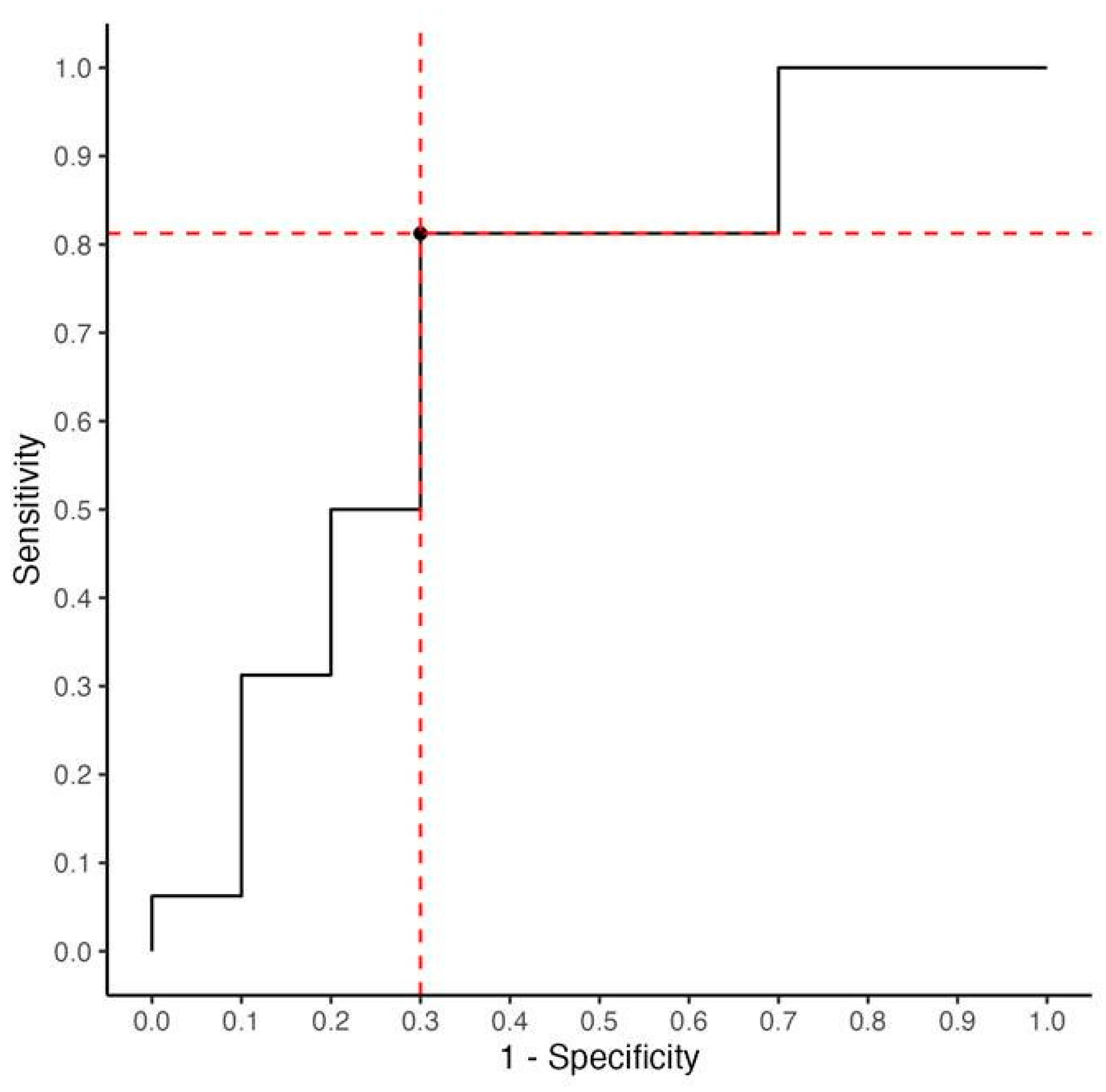
3.2. Explorative Correlation Analysis between DMD Tests TAS and Lysholm Score at Three and Six Months
3.3. Adverse Events and Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barber-Westin, S.D.; Noyes, F.R. Objective criteria for return to athletics after anterior cruciate ligament reconstruction and subsequent reinjury rates: A systematic review. Phys. Sportsmed. 2011, 39, 100–110. [Google Scholar] [CrossRef] [PubMed]
- Schneider, O.; Scharf, H.P.; Stein, T.; Knapstein, S.; Hermann, C.; Flechtenmacher, J. Incidence of knee injuries: Numbers for outpatient and inpatient care in Germany. Orthopade 2016, 45, 1015–1026. [Google Scholar] [CrossRef] [PubMed]
- Bodkin, S.; Goetschius, J.; Hertel, J.; Hart, J. Relationships of Muscle Function and Subjective Knee Function in Patients After ACL Reconstruction. Orthop. J. Sports Med. 2017, 5, 2325967117719041. [Google Scholar] [CrossRef] [PubMed]
- Groot, J.A.; Jonkers, F.J.; Kievit, A.J.; Kuijer, P.P.; Hoozemans, M.J. Beneficial and limiting factors for return to work following anterior cruciate ligament reconstruction: A retrospective cohort study. Arch. Orthop. Trauma Surg. 2017, 137, 155–166. [Google Scholar] [CrossRef]
- Kvist, J. Rehabilitation following anterior cruciate ligament injury: Current recommendations for sports participation. Sports Med. 2004, 34, 269–280. [Google Scholar] [CrossRef] [PubMed]
- van Melick, N.; van Cingel, R.E.; Brooijmans, F.; Neeter, C.; van Tienen, T.; Hullegie, W.; Nijhuis-van der Sanden, M.W. Evidence-based clinical practice update: Practice guidelines for anterior cruciate ligament rehabilitation based on a systematic review and multidisciplinary consensus. Br. J. Sports Med. 2016, 50, 1506–1515. [Google Scholar] [CrossRef] [PubMed]
- Barber-Westin, S.D.; Noyes, F.R. Factors used to determine return to unrestricted sports activities after anterior cruciate ligament reconstruction. Arthroscopy 2011, 27, 1697–1705. [Google Scholar] [CrossRef]
- Dingenen, B.; Gokeler, A. Optimization of the Return-to-Sport Paradigm After Anterior Cruciate Ligament Reconstruction: A Critical Step Back to Move Forward. Sports Med. 2017, 47, 1487–1500. [Google Scholar] [CrossRef]
- Irrgang, J.J.; Anderson, A.F.; Boland, A.L.; Harner, C.D.; Kurosaka, M.; Neyret, P.; Richmond, J.C.; Shelborne, K.D. Development and validation of the international knee documentation committee subjective knee form. Am. J. Sports Med. 2001, 29, 600–613. [Google Scholar] [CrossRef]
- Roos, E.M.; Roos, H.P.; Lohmander, L.S.; Ekdahl, C.; Beynnon, B.D. Knee Injury and Osteoarthritis Outcome Score (KOOS)--development of a self-administered outcome measure. J. Orthop. Sports Phys. Ther. 1998, 28, 88–96. [Google Scholar] [CrossRef]
- Lysholm, J.; Gillquist, J. Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am. J. Sports Med. 1982, 10, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Undheim, M.B.; Cosgrave, C.; King, E.; Strike, S.; Marshall, B.; Falvey, É.; Franklyn-Miller, A. Isokinetic muscle strength and readiness to return to sport following anterior cruciate ligament reconstruction: Is there an association? A systematic review and a protocol recommendation. Br. J. Sports Med. 2015, 49, 1305–1310. [Google Scholar] [CrossRef] [PubMed]
- Buckthorpe, M.; Tamisari, A.; Villa, F.D. A Ten Task-Based Progression in Rehabilitation after Acl Reconstruction: From Post-Surgery to Return to Play-a Clinical Commentary. Int. J. Sports Phys. Ther. 2020, 15, 611–623. [Google Scholar] [CrossRef] [PubMed]
- Kotsifaki, A.; Van Rossom, S.; Whiteley, R.; Korakakis, V.; Bahr, R.; Sideris, V.; Jonkers, I. Single leg vertical jump performance identifies knee function deficits at return to sport after ACL reconstruction in male athletes. Br. J. Sports Med. 2022, 56, 490–498. [Google Scholar] [CrossRef]
- Mitternacht, J.; Hermann, A.; Carqueville, P. Acquisition of Lower-Limb Motion Characteristics with a Single Inertial Measurement Unit-Validation for Use in Physiotherapy. Diagnostics 2022, 12, 1640. [Google Scholar] [CrossRef]
- Hoher, J.; Lischke, B.; Petersen, W.; Mengis, N.; Niederer, D.; Stein, T.; Stoffels, T.; Prill, R.; Schmidt-Lucke, C. Sensor-based telerehabilitation system increases patient adherence after knee surgery. PLoS Digit. Health 2023, 2, e0000175. [Google Scholar] [CrossRef]
- Montalvo, A.M.; Schneider, D.K.; Webster, K.E.; Yut, L.; Galloway, M.T.; Heidt, R.S., Jr.; Kaeding, C.C.; Kremcheck, T.E.; Magnussen, R.A.; Parikh, S.N.; et al. Anterior Cruciate Ligament Injury Risk in Sport: A Systematic Review and Meta-Analysis of Injury Incidence by Sex and Sport Classification. J. Athl. Train. 2019, 54, 472–482. [Google Scholar] [CrossRef]
- Buckthorpe, M. Recommendations for Movement Re-training After ACL Reconstruction. Sports Med. 2021, 51, 1601–1618. [Google Scholar] [CrossRef]
- Noyes, F.R.; Barber, S.D.; Mangine, R.E. Abnormal lower limb symmetry determined by function hop tests after anterior cruciate ligament rupture. Am. J. Sports Med. 1991, 19, 513–518. [Google Scholar] [CrossRef]
- Hoher, J.L.B.; Ohde, J.; Streich, N.; Herbort, M.; Schmidt-Lucke, C. The digitally measured single-leg vertical jump is a valid tool for documenting early rehabilitation progress after knee joint surgery. In Proceedings of the 11. Jahreskongress der Deutschen Kniegesellschaft, München, Germany, 18–19 November 2022. [Google Scholar]
- Hoher, J.S.N.; Allers, U.; Steinkamp, R.; Schraplau, A.; Ostner, I.; Suprizio, H.; Tenfelde, O.; Schmidt-Lucke, C. Single leg vertical hop test—Validation of a sensor-based medical device in early rehabilitation after reconstruction of the anterior cruciate ligament (ACL). In Proceedings of the OT Digital 2022, Berlin, Germany, 2–3 December 2022. [Google Scholar]
- Huang, H.; Nagao, M.; Arita, H.; Nishio, H.; Kaneko, H.; Saita, Y.; Ishijima, M.; Takazawa, Y.; Ikeda, H.; Kaneko, K. Validation and defining the minimal clinically important difference of the Japanese version of the IKDC Subjective Knee Form. J. Orthop. Sci. 2021, 26, 149–155. [Google Scholar] [CrossRef]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Logerstedt, D.; Di Stasi, S.; Grindem, H.; Lynch, A.; Eitzen, I.; Engebretsen, L.; Risberg, M.A.; Axe, M.J.; Snyder-Mackler, L. Self-reported knee function can identify athletes who fail return-to-activity criteria up to 1 year after anterior cruciate ligament reconstruction: A delaware-oslo ACL cohort study. J. Orthop. Sports Phys. Ther. 2014, 44, 914–923. [Google Scholar] [CrossRef] [PubMed]
- Ra, H.J.; Kim, H.S.; Choi, J.Y.; Ha, J.K.; Kim, J.Y.; Kim, J.G. Comparison of the ceiling effect in the Lysholm score and the IKDC subjective score for assessing functional outcome after ACL reconstruction. Knee 2014, 21, 906–910. [Google Scholar] [CrossRef]
- Briggs, K.K.; Lysholm, J.; Tegner, Y.; Rodkey, W.G.; Kocher, M.S.; Steadman, J.R. The reliability, validity, and responsiveness of the Lysholm score and Tegner activity scale for anterior cruciate ligament injuries of the knee: 25 years later. Am. J. Sports Med. 2009, 37, 890–897. [Google Scholar] [CrossRef] [PubMed]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Webster, K.E. Fifty-five per cent return to competitive sport following anterior cruciate ligament reconstruction surgery: An updated systematic review and meta-analysis including aspects of physical functioning and contextual factors. Br. J. Sports Med. 2014, 48, 1543–1552. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Lee, J.W.; Kim, S.G.; Cho, H.W.; Bae, J.H. Low Rate of Return to Preinjury Tegner Activity Level Among Recreational Athletes: Results at 1 Year After Primary ACL Reconstruction. Orthop. J. Sports Med. 2021, 9, 2325967120975751. [Google Scholar] [CrossRef]
- Mengis, N.; Zimmermann, F.; Schemel, L.; Rippke, J.N.; Milinkovic, D.D.; Balcarek, P. Return to Sports and Patients’ Rehabilitation Continuum After Deepening Trochleoplasty and Concomitant Patellar-Stabilizing Procedures: A Case Series of 111 Patients at 2 to 4 Years of Follow-up. Am. J. Sports Med. 2022, 50, 674–680. [Google Scholar] [CrossRef]
- Rushdi, I.; Sharifudin, S.; Shukur, A. Arthrofibrosis Following Anterior Cruciate Ligament Reconstruction. Malays. Orthop. J. 2019, 13, 34–38. [Google Scholar] [CrossRef]
- Rothrauff, B.B.; Kondo, E.; Siebold, R.; Wang, J.H.; Yoon, K.H.; Fu, F.H. Anterior cruciate ligament reconstruction with remnant preservation: Current concepts. J. ISAKOS 2020, 5, 128–133. [Google Scholar] [CrossRef]
- Wilk, K.E.; Romaniello, W.T.; Soscia, S.M.; Arrigo, C.A.; Andrews, J.R. The relationship between subjective knee scores, isokinetic testing, and functional testing in the ACL-reconstructed knee. J. Orthop. Sports Phys. Ther. 1994, 20, 60–73. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics (n = 67) | n (%) |
|---|---|
| Sex | |
| Male | 47 (70.1%) |
| Female | 20 (29.9%) |
| Median [Q1–Q3] | |
| Age [years] 1 | 25.3 [21.9–32.0] |
| Height [cm] | 177.0 [169.0–183.0] |
| Weight [kg] | 75.5 [67.3–85.0] |
| BMI [kg/m2] | 23.9 [22.5–26.3] |
| Tegner Activity Scale, T0 | 6.0 [4.0–7.0] |
| Lysholm Score, T0 | 56.5 [42.3–72.3] |
| IKDC-SKF Score, T0 | 47.1 [30.5–59.8] |
| n (%) | |
| Injured Leg | |
| Right | 27 (41%) |
| Left | 40 (59%) |
| n (%) | |
| Diagnosis for acute co-injuries | |
| ACL rupture—ACL reconstruction (Semitendinosus/Gracilis) | 67 (100%) |
| Lateral meniscus tear, repair | 10 (15%) |
| Lateral meniscus tear, partial meniscectomy | 5 (8%) |
| Medial meniscus tear, repair | 12 (18%) |
| Medial meniscus tear, partial meniscectomy | 2 (3%) |
| Cartilage damage (CM2°), chondroplasty | 4 (6%) |
| Partial medial collateral ligament tear, non-operative | 7 (10%) |
| Adhesions arthrolysis | 4 (6%) |
| Hematoma flushing | 1 (1%) |
| Lateral collateral ligament strain, non-operative | 1 (1%) |
| Category | Test | Outcome Parameter | Optimal and Earliest Timepoint for Assessment Postoperatively * |
|---|---|---|---|
| Range of Motion | Angle measurement passive | Flexion (degrees), extension (degrees) | 3–5 days |
| Angle measurement active | Flexion (degrees), extension (degrees) | 3–5 days | |
| Extension deficit | Extension deficit (degrees) | 3–5 days | |
| Coordination | One leg squat | Knee displacement (degrees) | 1–1.5 months |
| Angle reproduction | Deviation from predefined angle (degrees) | 1–2 weeks | |
| Y-Balance | Dynamic Balance Composite Score (mm) | 1–1.5 months post | |
| One leg stance (Functional stability) | Knee displacement (mm) | 2–3 weeks | |
| Strength/Speed | Vertical jump | Jump height (mm) | 1–1.5 months |
| Distance jump | Jumping distance (cm) | 1.5–2 months | |
| Side hop | Number of hops performed within 30 s | 2–3 months | |
| Drop jump | Knee displacement (degrees) | 2–3 months | |
| Speedy jump | Time (s) to complete small obstacle course | 2–3 months |
| IKDC-SKF Score | Lysholm Score | Tegner Activity Scale | |
|---|---|---|---|
| T0 | 47.1 [30.5–59.8] | 56.5 [42.3–72.3] | 6.0 [4.0–7.0] |
| FU1 | 64.4 [51.7–73.6] *** | 79.0 [63.5–85.5] *** | 4.0 [3.0–4.0] *** |
| FU2 | 78.2 [71.9–83.4] *** | 87.0 [80.0–90.0] ** | 5.0 [4.0–5.0] ** |
| Type of Event | Description | Total (n = 67) |
|---|---|---|
| Serious adverse event | ||
| knee joint infection with surgical irrigation, ACL preserved | 1 | |
| Adverse event | ||
| patellofemoral pain syndrome | 1 | |
| ACL plastic partial rupture, no surgery required | 1 | |
| Arthrofibrosis with indication for oral cortisone therapy | 2 | |
| Arthrofibrosis after infection | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mengis, N.; Schmidt, S.; Ellermann, A.; Sobau, C.; Egloff, C.; Kreher, M.M.; Ksoll, K.; Schmidt-Lucke, C.; Rippke, J.-N. A Novel Sensor-Based Application for Home-Based Rehabilitation Can Objectively Measure Postoperative Outcomes following Anterior Cruciate Ligament Reconstruction. J. Pers. Med. 2023, 13, 1398. https://doi.org/10.3390/jpm13091398
Mengis N, Schmidt S, Ellermann A, Sobau C, Egloff C, Kreher MM, Ksoll K, Schmidt-Lucke C, Rippke J-N. A Novel Sensor-Based Application for Home-Based Rehabilitation Can Objectively Measure Postoperative Outcomes following Anterior Cruciate Ligament Reconstruction. Journal of Personalized Medicine. 2023; 13(9):1398. https://doi.org/10.3390/jpm13091398
Chicago/Turabian StyleMengis, Natalie, Sebastian Schmidt, Andree Ellermann, Christian Sobau, Christian Egloff, Mahli Megan Kreher, Korbinian Ksoll, Caroline Schmidt-Lucke, and Jules-Nikolaus Rippke. 2023. "A Novel Sensor-Based Application for Home-Based Rehabilitation Can Objectively Measure Postoperative Outcomes following Anterior Cruciate Ligament Reconstruction" Journal of Personalized Medicine 13, no. 9: 1398. https://doi.org/10.3390/jpm13091398