
Soluble Transferrin Receptor as Iron Deficiency Biomarker: Impact on Exercise Capacity in Heart Failure Patients
 , , , , , , , , ,
, , , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Baseline Patient Characteristics
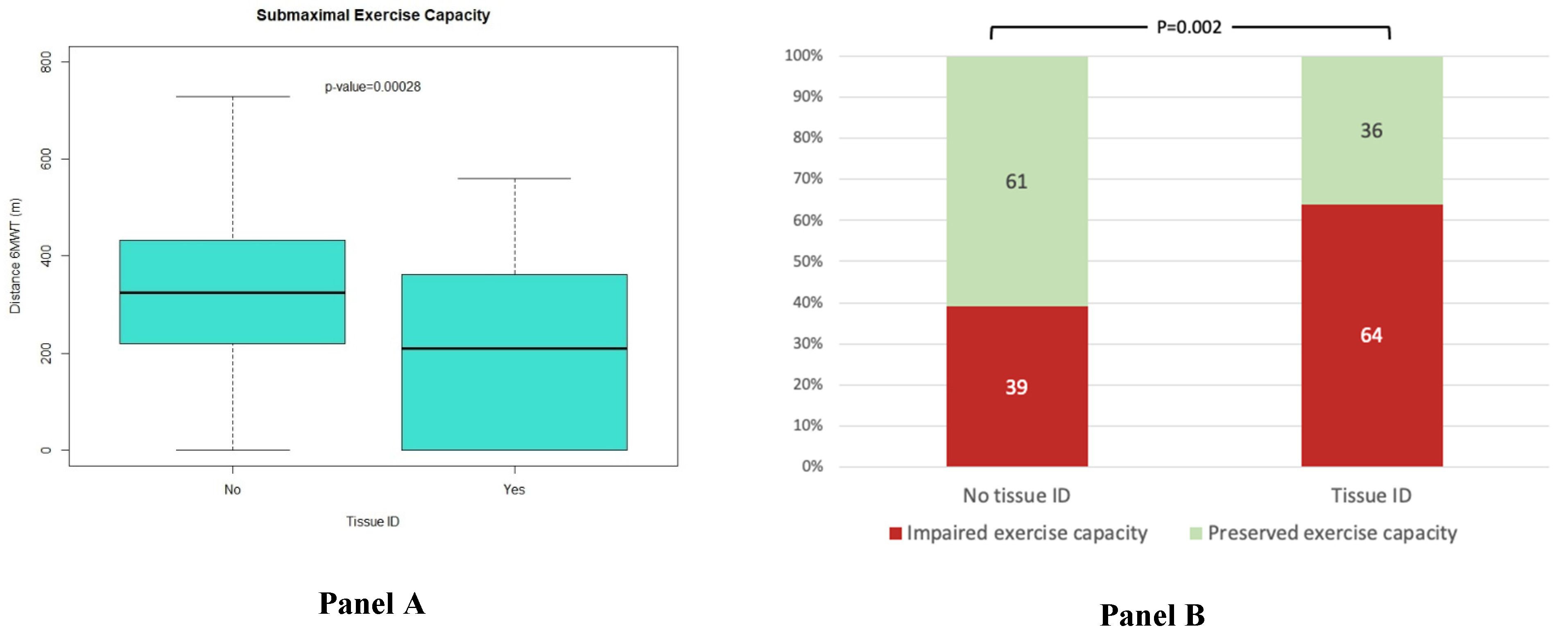
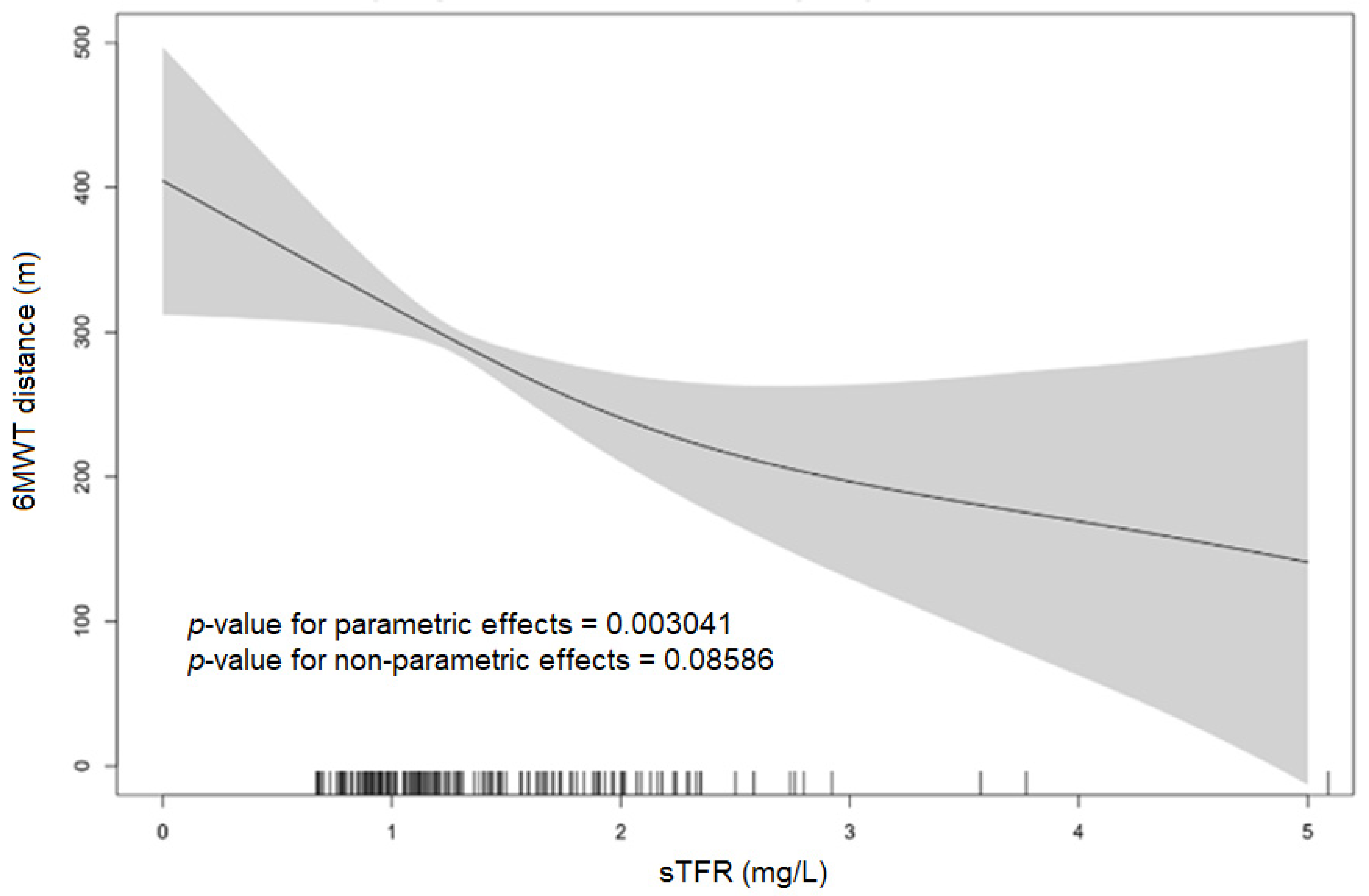
3.2. Association of sTfR with Exercise Capacity and NYHA Class
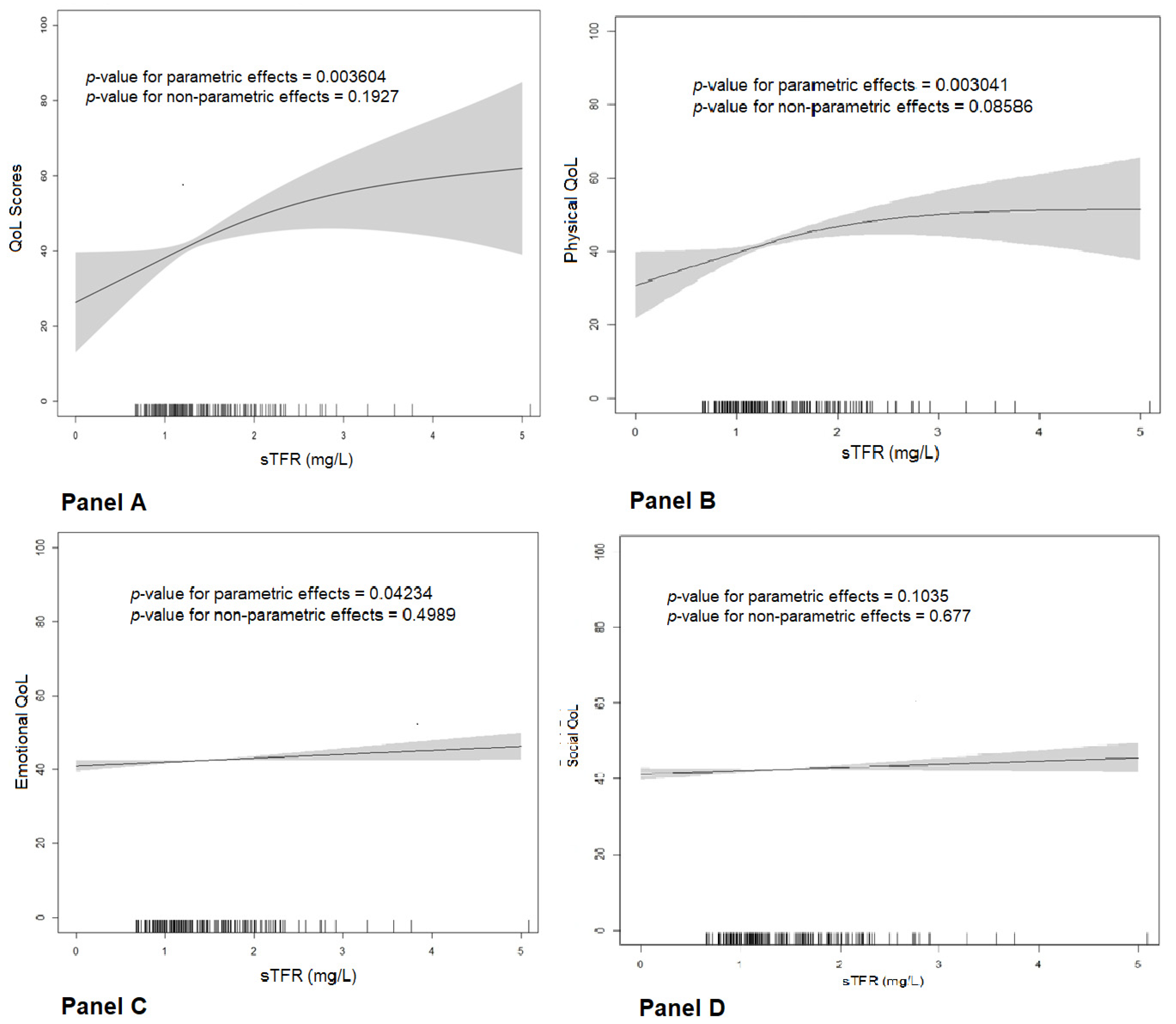
3.3. Association of sTfR with Quality of Life
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cainzos-Achirica, M.; Capdevila, C.; Vela, E.; Cleries, M.; Bilal, U.; Garcia-Altes, A.; Enjuanes, C.; Garay, A.; Yun, S.; Farre, N.; et al. Individual income, mortality and healthcare resource use in patients with chronic heart failure living in a universal healthcare system: A population-based study in Catalonia, Spain. Int. J. Cardiol. 2019, 277, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Farré, N.; Vela, E.; Clèries, M.; Bustins, M.; Cainzos-Achirica, M.; Enjuanes, C.; Moliner, P.; Ruiz, S.; Verdú-Rotellar, J.M.; Comín-Colet, J. Medical resource use and expenditure in patients with chronic heart failure: A population-based analysis of 88 195 patients. Eur. J. Heart Fail. 2016, 18, 1132–1140. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2022, 24, 4–131. [Google Scholar] [CrossRef] [PubMed]
- Ingle, L.; Cleland, J.G.; Clark, A.L. The relation between repeated 6-minute walk test performance and outcome in patients with chronic heart failure. Ann. Phys. Rehabil. Med. 2014, 57, 244–253. [Google Scholar] [CrossRef] [PubMed]
- Johansson, I.; Joseph, P.; Balasubramanian, K.; McMurray, J.J.V.; Lund, L.H.; Ezekowitz, J.A.; Kamath, D.; Alhabib, K.; Bayes-Genis, A.; Budaj, A.; et al. Health-Related Quality of Life and Mortality in Heart Failure: The Global Congestive Heart Failure Study of 23 000 Patients From 40 Countries. Circulation 2021, 143, 2129–2142. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.; Olazo, K.; Sierra, M.; Tarver, M.E.; Caldwell, B.; Saha, A.; Lisker, S.; Lyles, C.; Sarkar, U. Do patient-reported outcome measures measure up? A qualitative study to examine perceptions and experiences with heart failure proms among diverse, low-income patients. J. Patient Rep. Outcomes 2022, 6, 6. [Google Scholar] [CrossRef] [PubMed]
- von Haehling, S.; Arzt, M.; Doehner, W.; Edelmann, F.; Evertz, R.; Ebner, N.; Herrmann-Lingen, C.; Garfias Macedo, T.; Koziolek, M.; Noutsias, M.; et al. Improving exercise capacity and quality of life using non-invasive heart failure treatments: Evidence from clinical trials. Eur. J. Heart Fail. 2021, 23, 92–113. [Google Scholar] [CrossRef]
- Anker, S.D.; Comin Colet, J.; Filippatos, G.; Willenheimer, R.; Dickstein, K.; Drexler, H.; Lüscher, T.F.; Bart, B.; Banasiak, W.; Niegowska, J.; et al. Ferric carboxymaltose in patients with heart failure and iron deficiency. N. Engl. J. Med. 2009, 361, 2436–2448. [Google Scholar] [CrossRef]
- Ponikowski, P.; van Veldhuisen, D.J.; Comin-Colet, J.; Ertl, G.; Komajda, M.; Mareev, V.; McDonagh, T.; Parkhomenko, A.; Tavazzi, L.; Levesque, V.; et al. Beneficial effects of long-term intravenous iron therapy with ferric carboxymaltose in patients with symptomatic heart failure and iron deficiency†. Eur. Heart J. 2015, 36, 657–668. [Google Scholar] [CrossRef]
- Jankowska, E.A.; Kirwan, B.A.; Kosiborod, M.; Butler, J.; Anker, S.D.; McDonagh, T.; Dorobantu, M.; Drozdz, J.; Filippatos, G.; Keren, A.; et al. The effect of intravenous ferric carboxymaltose on health-related quality of life in iron-deficient patients with acute heart failure: The results of the AFFIRM-AHF study. Eur. Heart J. 2021, 42, 3011–3020. [Google Scholar] [CrossRef]
- von Haehling, S.; Ebner, N.; Evertz, R.; Ponikowski, P.; Anker, S.D. Iron Deficiency in Heart Failure: An Overview. JACC Heart Fail. 2019, 7, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Enjuanes, C.; Klip, I.T.; Bruguera, J.; Cladellas, M.; Ponikowski, P.; Banasiak, W.; van Veldhuisen, D.J.; van der Meer, P.; Jankowska, E.A.; Comín-Colet, J. Iron deficiency and health-related quality of life in chronic heart failure: Results from a multicenter European study. Int. J. Cardiol. 2014, 174, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Enjuanes, C.; Bruguera, J.; Grau, M.; Cladellas, M.; Gonzalez, G.; Meroño, O.; Moliner-Borja, P.; Verdú, J.M.; Farré, N.; Comín-Colet, J. Iron Status in Chronic Heart Failure: Impact on Symptoms, Functional Class and Submaximal Exercise Capacity. Rev. Esp. Cardiol. (Engl. Ed.) 2016, 69, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Alcaide-Aldeano, A.; Garay, A.; Alcoberro, L.; Jiménez-Marrero, S.; Yun, S.; Tajes, M.; García-Romero, E.; Díez-López, C.; González-Costello, J.; Mateus-Porta, G.; et al. Iron Deficiency: Impact on Functional Capacity and Quality of Life in Heart Failure with Preserved Ejection Fraction. J. Clin. Med. 2020, 9, 1199. [Google Scholar] [CrossRef] [PubMed]
- Martens, P.; Nijst, P.; Verbrugge, F.H.; Smeets, K.; Dupont, M.; Mullens, W. Impact of iron deficiency on exercise capacity and outcome in heart failure with reduced, mid-range and preserved ejection fraction. Acta Cardiol. 2018, 73, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Wish, J.B. Assessing iron status: Beyond serum ferritin and transferrin saturation. Clin. J. Am. Soc. Nephrol. 2006, 1 (Suppl. 1), S4–S8. [Google Scholar] [CrossRef] [PubMed]
- Brownlie, T., 4th; Utermohlen, V.; Hinton, P.S.; Haas, J.D. Tissue iron deficiency without anemia impairs adaptation in endurance capacity after aerobic training in previously untrained women. Am. J. Clin. Nutr. 2004, 79, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Hirsh, V.; Tongers, J.; Bode, J.; Berliner, D.; Widder, J.; Escher, F.; Mustenko, V.; Chung, B.; Rostami, F.; Guba-Quint, A.; et al. Cardiac iron concentration in relation to systemic iron status and disease severity in non-ischaemic heart failure with reduced ejection fraction. Eur. J. Heart Fail. 2020, 22, 2038–2046. [Google Scholar] [CrossRef]
- Suominen, P.; Punnonen, K.; Rajamäki, A.; Irjala, K. Serum transferrin receptor and transferrin receptor-ferritin index identify healthy subjects with subclinical iron deficits. Blood 1998, 92, 2934–2939. [Google Scholar] [CrossRef]
- Skikne, B.S.; Flowers, C.H.; Cook, J.D. Serum transferrin receptor: A quantitative measure of tissue iron deficiency. Blood 1990, 75, 1870–1876. [Google Scholar] [CrossRef]
- Sierpinski, R.; Josiak, K.; Suchocki, T.; Wojtas-Polc, K.; Mazur, G.; Butrym, A.; Rozentryt, P.; van der Meer, P.; Comin-Colet, J.; von Haehling, S.; et al. High soluble transferrin receptor in patients with heart failure: A measure of iron deficiency and a strong predictor of mortality. Eur. J. Heart Fail. 2021, 23, 919–932, Erratum in Eur. J. Heart Fail. 2022, 24, 591. [Google Scholar] [CrossRef] [PubMed]
- Comín-Colet, J.; Enjuanes, C.; González, G.; Torrens, A.; Cladellas, M.; Meroño, O.; Ribas, N.; Ruiz, S.; Gómez, M.; Verdú, J.M.; et al. Iron deficiency is a key determinant of health-related quality of life in patients with chronic heart failure regardless of anaemia status. Eur. J. Heart Fail. 2013, 15, 1164–1172. [Google Scholar] [CrossRef]
- Calero-Molina, E.; Moliner, P.; Hidalgo, E.; Rosenfeld, L.; Verdú-Rotellar, J.M.; Verdú-Soriano, J.; Yun, S.; Garay, A.; Alcoberro, L.; Jiménez-Marrero, S.; et al. Interplay between psychosocial and heart failure related factors may partially explain limitations in self-efficacy in patients with heart failure: Insights from a real-world cohort of 1,123 patients. Int. J. Nurs. Stud. 2022, 129, 104233. [Google Scholar] [CrossRef] [PubMed]
- Calero-Molina, E.; Hidalgo, E.; Rosenfeld, L.; Verdú-Rotellar, J.M.; Verdú-Soriano, J.; Garay, A.; Alcoberro, L.; Jimenez-Marrero, S.; Garcimartin, P.; Yun, S.; et al. The relationship between self-care, long-term mortality, and heart failure hospitalization: Insights from a real-world cohort study. Eur. J. Cardiovasc. Nurs. 2022, 21, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Farré, N.; Aranyó, J.; Enjuanes, C.; Verdú-Rotellar, J.M.; Ruiz, S.; Gonzalez-Robledo, G.; Meroño, O.; de Ramon, M.; Moliner, P.; Bruguera, J.; et al. Differences in neurohormonal activity partially explain the obesity paradox in patients with heart failure: The role of sympathetic activation. Int. J. Cardiol. 2015, 181, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Gavaldà-Manso, M.; Jimenez-Marrero, S.; Cainzos-Achirica, M.; Garay, A.; Enjuanes, C.; Yun, S.; Diez, C.; Gonzalez-Costello, J.; Tajes, M.; Farre, N.; et al. Reduced levels of vasopressin, an independent mechanism in the obesity paradox in patients with chronic heart failure: Insights from the DAMOCLES study. Int. J. Cardiol. 2019, 276, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Moliner, P.; Enjuanes, C.; Tajes, M.; Cainzos-Achirica, M.; Lupón, J.; Garay, A.; Jimenez-Marrero, S.; Yun, S.; Farré, N.; Cladellas, M.; et al. Association Between Norepinephrine Levels and Abnormal Iron Status in Patients With Chronic Heart Failure: Is Iron Deficiency More Than a Comorbidity? J. Am. Heart Assoc. 2019, 8, e010887. [Google Scholar] [CrossRef]
- Coma, M.; González-Moneo, M.J.; Enjuanes, C.; Velázquez, P.P.; Espargaró, D.B.; Pérez, B.A.; Tajes, M.; Garcia-Elias, A.; Farré, N.; Sánchez-Benavides, G.; et al. Effect of Permanent Atrial Fibrillation on Cognitive Function in Patients With Chronic Heart Failure. Am. J. Cardiol. 2016, 117, 233–239. [Google Scholar] [CrossRef]
- González-Moneo, M.J.; Sánchez-Benavides, G.; Verdu-Rotellar, J.M.; Cladellas, M.; Bruguera, J.; Quiñones-Ubeda, S.; Enjuanes, C.; Peña-Casanova, J.; Comín-Colet, J. Ischemic aetiology, self-reported frailty, and gender with respect to cognitive impairment in chronic heart failure patients. BMC Cardiovasc. Disord. 2016, 16, 163. [Google Scholar] [CrossRef]
- Tapia, J.; Basalo, M.; Enjuanes, C.; Calero, E.; José, N.; Ruíz, M.; Calvo, E.; Garcimartín, P.; Moliner, P.; Hidalgo, E.; et al. Psychosocial factors partially explain gender differences in health-related quality of life in heart failure patients. ESC Heart Fail. 2023, 10, 1090–1102. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117, Erratum in Am. J. Respir. Crit. Care Med. 2016, 193, 1185. [Google Scholar] [CrossRef]
- Bittner, V.; Weiner, D.H.; Yusuf, S.; Rogers, W.J.; McIntyre, K.M.; Bangdiwala, S.I.; Kronenberg, M.W.; Kostis, J.B.; Kohn, R.M.; Guillotte, M.; et al. Prediction of mortality and morbidity with a 6-minute walk test in patients with left ventricular dysfunction. SOLVD Investigators. JAMA 1993, 270, 1702–1707. [Google Scholar] [CrossRef] [PubMed]
- Arslan, S.; Erol, M.K.; Gundogdu, F.; Sevimli, S.; Aksakal, E.; Senocak, H.; Alp, N. Prognostic value of 6-minute walk test in stable outpatients with heart failure. Tex. Heart Inst. J. 2007, 34, 166–169. [Google Scholar] [PubMed]
- Garin, O.; Soriano, N.; Ribera, A.; Ferrer, M.; Pont, A.; Alonso, J.; Permanyer, G.; Grupo IC-QoL. Validación de la versión española del Minnesota Living with Heart Failure Questionnaire [Validation of the Spanish version of the Minnesota Living with Heart Failure Questionnaire]. Rev. Esp. Cardiol. 2008, 61, 251–259. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Jankowska, E.A.; Rozentryt, P.; Witkowska, A.; Nowak, J.; Hartmann, O.; Ponikowska, B.; Borodulin-Nadzieja, L.; von Haehling, S.; Doehner, W.; Banasiak, W.; et al. Iron deficiency predicts impaired exercise capacity in patients with systolic chronic heart failure. J. Card. Fail. 2011, 17, 899–906. [Google Scholar] [CrossRef] [PubMed]
- Jankowska, E.A.; Rozentryt, P.; Witkowska, A.; Nowak, J.; Hartmann, O.; Ponikowska, B.; Borodulin-Nadzieja, L.; Banasiak, W.; Polonski, L.; Filippatos, G.; et al. Iron deficiency: An ominous sign in patients with systolic chronic heart failure. Eur. Heart J. 2010, 31, 1872–1880, Erratum in Eur. Heart J. 2011, 32, 1054. [Google Scholar] [CrossRef] [PubMed]
- Comin-Colet, J.; Lainscak, M.; Dickstein, K.; Filippatos, G.S.; Johnson, P.; Lüscher, T.F.; Mori, C.; Willenheimer, R.; Ponikowski, P.; Anker, S.D. The effect of intravenous ferric carboxymaltose on health-related quality of life in patients with chronic heart failure and iron deficiency: A subanalysis of the FAIR-HF study. Eur. Heart J. 2013, 34, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Kirwan, B.A.; Anker, S.D.; McDonagh, T.; Dorobantu, M.; Drozdz, J.; Fabien, V.; Filippatos, G.; Göhring, U.M.; Keren, A.; et al. Ferric carboxymaltose for iron deficiency at discharge after acute heart failure: A multicentre, double-blind, randomised, controlled trial. Lancet 2020, 396, 1895–1904, Erratum in Lancet 2021, 398, 1964. [Google Scholar] [CrossRef]
- Graham, F.J.; Pellicori, P.; Ford, I.; Petrie, M.C.; Kalra, P.R.; Cleland, J.G.F. Intravenous iron for heart failure with evidence of iron deficiency: A meta-analysis of randomised trials. Clin. Res. Cardiol. 2021, 110, 1299–1307. [Google Scholar] [CrossRef]
- González-Costello, J.; Cainzos-Achirica, M.; Lupón, J.; Farré, N.; Moliner-Borja, P.; Enjuanes, C.; Antonio, M.; Fuentes, L.; Díez-López, C.; Bayés-Genis, A.; et al. Use of intravenous iron in patiens with iron deficiency and chronic heart failure: Real-world evidence. Eur. J. Intern. Med. 2020, 80, 91–98. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032, Erratum in Circulation 2022, 146, e185. Erratum in Circulation 2023, 147, e674. [Google Scholar] [CrossRef] [PubMed]
- Campodonico, J.; Nicoli, F.; Motta, I.; Migone De Amicis, M.; Bonomi, A.; Cappellini, M.; Agostoni, P. Prognostic role of transferrin saturation in heart failure patients. Eur. J. Prev. Cardiol. 2021, 28, 1639–1646. [Google Scholar] [CrossRef] [PubMed]
- Grote Beverborg, N.; Klip, I.T.; Meijers, W.C.; Voors, A.A.; Vegter, E.L.; van der Wal, H.H.; Swinkels, D.W.; van Pelt, J.; Mulder, A.B.; Bulstra, S.K.; et al. Definition of Iron Deficiency Based on the Gold Standard of Bone Marrow Iron Staining in Heart Failure Patients. Circ. Heart Fail. 2018, 11, e004519. [Google Scholar] [CrossRef] [PubMed]
- Martens, P.; Grote Beverborg, N.; van der Meer, P. Iron deficiency in heart failure-time to redefine. Eur. J. Prev. Cardiol. 2021, 28, 1647–1649. [Google Scholar] [CrossRef] [PubMed]
- National Kidney Foundation. IV. NKF-K/DOQI Clinical Practice Guidelines for Anemia of Chronic Kidney Disease: Update 2000. Am. J. Kidney Dis. 2001, 37 (Suppl. 1), S182–S238, Erratum in Am. J. Kidney Dis. 2001, 38, 442. [Google Scholar] [CrossRef]
- González-Costello, J.; Comin-Colet, J.; Lupón, J.; Enjuanes, C.; Antonio, M.; Fuentes, L.; Moliner-Borja, P.; Farré, N.; Zamora, E.; Manito, N.; et al. Importance of iron deficiency in patients with chronic heart failure as a predictor of mortality and hospitalizations: Insights from an observational cohort study. BMC Cardiovasc. Disord. 2018, 18, 206. [Google Scholar] [CrossRef] [PubMed]
- Koulaouzidis, A.; Said, E.; Cottier, R.; Saeed, A.A. Soluble transferrin receptors and iron deficiency, a step beyond ferritin. A systematic review. J. Gastrointestin Liver Dis. 2009, 18, 345–352. [Google Scholar] [PubMed]
- Skikne, B.S. Serum transferrin receptor. Am. J. Hematol. 2008, 83, 872–875. [Google Scholar] [CrossRef]
- Ponikowska, B.; Suchocki, T.; Paleczny, B.; Olesinska, M.; Powierza, S.; Borodulin-Nadzieja, L.; Reczuch, K.; von Haehling, S.; Doehner, W.; Anker, S.D.; et al. Iron status and survival in diabetic patients with coronary artery disease. Diabetes Care 2013, 36, 4147–4156. [Google Scholar] [CrossRef]
- Weidmann, H.; Bannasch, J.H.; Waldeyer, C.; Shrivastava, A.; Appelbaum, S.; Ojeda-Echevarria, F.M.; Schnabel, R.; Lackner, K.J.; Blankenberg, S.; Zeller, T.; et al. Iron Metabolism Contributes to Prognosis in Coronary Artery Disease: Prognostic Value of the Soluble Transferrin Receptor Within the AtheroGene Study. J. Am. Heart Assoc. 2020, 9, e015480. [Google Scholar] [CrossRef]
- Tajes, M.; Díez-López, C.; Enjuanes, C.; Moliner, P.; Ferreiro, J.L.; Garay, A.; Jiménez-Marrero, S.; Yun, S.; Sosa, S.G.; Alcoberro, L.; et al. Neurohormonal activation induces intracellular iron deficiency and mitochondrial dysfunction in cardiac cells. Cell Biosci. 2021, 11, 89. [Google Scholar] [CrossRef] [PubMed]
- Alnuwaysir, R.I.S.; Hoes, M.F.; van Veldhuisen, D.J.; van der Meer, P.; Grote Beverborg, N. Iron Deficiency in Heart Failure: Mechanisms and Pathophysiology. J. Clin. Med. 2021, 11, 125. [Google Scholar] [CrossRef] [PubMed]
- Jankowska, E.A.; von Haehling, S.; Anker, S.D.; Macdougall, I.C.; Ponikowski, P. Iron deficiency and heart failure: Diagnostic dilemmas and therapeutic perspectives. Eur. Heart J. 2013, 34, 816–829. [Google Scholar] [CrossRef] [PubMed]
- Kobak, K.A.; Radwańska, M.; Dzięgała, M.; Kasztura, M.; Josiak, K.; Banasiak, W.; Ponikowski, P.; Jankowska, E.A. Structural and functional abnormalities in iron-depleted heart. Heart Fail. Rev. 2019, 24, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Hoes, M.F.; Grote Beverborg, N.; Kijlstra, J.D.; Kuipers, J.; Swinkels, D.W.; Giepmans, B.N.G.; Rodenburg, R.J.; van Veldhuisen, D.J.; de Boer, R.A.; van der Meer, P. Iron deficiency impairs contractility of human cardiomyocytes through decreased mitochondrial function. Eur. J. Heart Fail. 2018, 20, 910–919. [Google Scholar] [CrossRef]
- Leszek, P.; Sochanowicz, B.; Szperl, M.; Kolsut, P.; Brzóska, K.; Piotrowski, W.; Rywik, T.M.; Danko, B.; Polkowska-Motrenko, H.; Różański, J.M.; et al. Myocardial iron homeostasis in advanced chronic heart failure patients. Int. J. Cardiol. 2012, 159, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Díez-López, C.; Tajes Orduña, M.; Enjuanes Grau, C.; Moliner Borja, P.; González-Costello, J.; García-Romero, E.; Francesch Manzano, J.; Yun Viladomat, S.; Jiménez-Marrero, S.; Ramos-Polo, R.; et al. Blood Differential Gene Expression in Patients with Chronic Heart Failure and Systemic Iron Deficiency: Pathways Involved in Pathophysiology and Impact on Clinical Outcomes. J. Clin. Med. 2021, 10, 4937. [Google Scholar] [CrossRef]
- Giannitsi, S.; Bougiakli, M.; Bechlioulis, A.; Kotsia, A.; Michalis, L.K.; Naka, K.K. 6-minute walking test: A useful tool in the management of heart failure patients. Ther. Adv. Cardiovasc. Dis. 2019, 13, 1753944719870084. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Soluble Transferrin Receptor (sTfR) Levels, Divided into Tertiles | |||||
|---|---|---|---|---|---|
| Lower Tertile | Middle Tertile | Upper Tertile | |||
| Whole Cohort (n = 215) | sTfR < 1.11 mg/L (n = 73) | sTfR 1.1–1.46 mg/L (n = 71) | sTfR ≥ 1.46 mg/L (n = 71) | p-Value | |
| Demographic and Clinical Factors | |||||
| Age, years | 70 (12) | 68 (13) | 70 (11) | 72 (11) | 0.113 |
| Sex (female), n (%) | 62 (29%) | 23 (32%) | 14 (20%) | 25 (35%) | 0.104 |
| Systolic blood pressure, mmHg | 125 (24) | 124 (23) | 127 (23) | 124 (26) | 0.807 |
| Heart rate, bpm | 73 (14) | 71 (14) | 72 (14) | 77 (11) | 0.020 |
| NYHA Functional Class, n (%) | 0.033 | ||||
| I | 44 (21%) | 22 (31%) | 15 (21%) | 7 (10%) | |
| II | 112 (53%) | 36 (50%) | 36 (51%) | 40 (57%) | |
| III | 46 (22%) | 12 (18%) | 18 (25%) | 16 (23%) | |
| IV | 11 (5%) | 2 (3%) | 2 (3%) | 7 (10%) | |
| Impaired submaximal exercise capacity, n (%) | 91 (45%) | 25 (35%) | 30 (46%) | 36 (55%) | 0.061 |
| HF hospitalization in previous year, n (%) | 172 (80%) | 51 (71%) | 63 (89%) | 58 (82%) | 0.025 |
| LVEF, % | 43 (15) | 42 (15) | 45 (14) | 42 (15) | 0.470 |
| Ischemic etiology of HF, n (%) | 64 (30%) | 16 (22%) | 23 (32%) | 25 (35%) | 0.183 |
| Comorbidities | |||||
| Hypertension, n (%) | 156 (73%) | 50 (69%) | 51 (72%) | 55 (78%) | 0.476 |
| Diabetes mellitus, n (%) | 68 (32%) | 19 (26%) | 28 (39%) | 21 (29%) | 0.202 |
| Obesity (%) | 58 (27%) | 17 (23%) | 21 (30%) | 20 (28%) | 0.671 |
| Previous MI, n (%) | 35 (16%) | 8 (11%) | 11 (16%) | 16 (23%) | 0.166 |
| CKD, n (%) | 90 (42%) | 26 (36%) | 31 (45%) | 33 (47%) | 0.361 |
| Treatments (%) | |||||
| ACEI or ARBs | 185 (86%) | 64 (88%) | 61 (86%) | 60 (85%) | 0.869 |
| Beta-blockers | 191 (89%) | 64 (88%) | 63 (89%) | 64 (90%) | 0.895 |
| MRA | 90 (42%) | 34 (47%) | 25 (35%) | 31 (44%) | 0.359 |
| Diuretics | 195 (91%) | 62 (85%) | 63 (89%) | 70 (99%) | 0.015 |
| Antiplatelet or anticoagulant therapy | 168 (78%) | 50 (69%) | 59 (83%) | 59 (83%) | 0.049 |
| Laboratory | |||||
| Hemoglobin, g/dL | 14.2 (1.4) | 14.1 (1.3) | 14.1 (1.4) | 14.1 (1.5) | 0.978 |
| Creatinine, mg/dL | 1.2 (0.4) | 1.1 (0.3) | 1.2 (0.3) | 1.3 (0.4) | 0.024 |
| NT-proBNP, pg/mL (median, IQR) | 1125 (587–2668) | 1123 (505–2548) | 966 (489–2144) | 1660 (757–3871) | 0.122 |
| Serum proteins, g/dL | 6.9 (0.7) | 7.0 (0.8) | 6.8 (0.7) | 6.7 (0.7) | 0.196 |
| Serum albumin, g/dL | 4.0 (0.6) | 4.2 (0.5) | 3.9 (0.5) | 3.9 (0.7) | 0.030 |
| Dependent Variable: Distance Walked in the 6 MWT (Submaximal Exercise Capacity) in Meters | ||||
| Univariate Linear Regression Models | Multivariate Linear Regression Models | |||
| Measures of Tissue ID | Standardized β Coefficient | p-Value | Standardized β Coefficient | p-Value |
| Log sTfR (mg/L) | −0.249 | <0.001 | −0.135 | 0.010 |
| sTfR > 75th percentile (1.63 mg/L) | −0.278 | <0.001 | −0.176 | 0.001 |
| Dependent variable: Advanced NYHA Functional Class (NYHA ≥ III or IV) | ||||
| Univariate Binary Logistic Regression Models | Multivariate Binary Logistic Regression Models | |||
| Measures of Tissue ID | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| Log sTfR 1 (mg/L) | 5.59 (0.852–36.671) | 0.073 | 0.915 (0.079–10.594) | 0.943 |
| sTfR > 75th percentile (1.63 mg/L) | 1.73 (0.887–3.368) | 0.108 | 0.849 (0.364–1.980) | 0.704 |
| MLHFQ Overall Summary Scores | |||||
| Univariate Linear Regression Models | Multivariate Linear Regression Models | ||||
| Measures of Tissue ID | Standardized β Coefficient | p-Value | Standardized β Coefficient | p-Value | R Model |
| sTfR (mg/L) | 0.201 | 0.004 | 0.183 | 0.008 | 0.280 |
| sTfR > 75th percentile (1.63 mg/L) | 0.191 | 0.006 | 0.164 | 0.019 | 0.267 |
| MLHFQ Physical Dimension Scores | |||||
| Univariate Linear Regression Models | Multivariate Linear Regression Models | ||||
| Measures of Tissue ID | Standardized β coefficient | p-Value | Standardized β coefficient | p-value | R model |
| sTfR (mg/L) | 0.204 | 0.003 | 0.176 | 0.012 | 0.310 |
| sTfR > 75th percentile (1.63 mg/L) | 0.213 | 0.002 | 0.151 | 0.029 | 0.377 |
| MLHFQ Emotional Dimension Scores | |||||
| Univariate Linear Regression Models | Multivariate Linear Regression Models | ||||
| Measures of Tissue ID | Standardized β Coefficient | p-Value | Standardized β Coefficient | p-Value | R Model |
| sTfR, 1 mg/L | 0.142 | 0.042 | 0.132 | 0.057 | 0.258 |
| sTfR > 75th percentile (1.63 mg/L) | 0.161 | 0.021 | 0.148 | 0.034 | 0.258 |
| MLHFQ Social Dimension Scores | |||||
| Univariate Linear Regression Models | Multivariate Linear Regression Models | ||||
| Measures of Tissue ID | Standardized β Coefficient | p-Value | Standardized β Coefficient | p-Value | R Model |
| sTfR, 1 mg/L | 0.114 | 0.102 | 0.132 | 0.052 | 0.305 |
| sTfR > 75th percentile (1.63 mg/L) | 0.061 | 0.384 | 0.096 | 0.162 | 0.305 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ras-Jiménez, M.d.M.; Ramos-Polo, R.; Francesch Manzano, J.; Corbella Santano, M.; Morillas Climent, H.; Jose-Bazán, N.; Jiménez-Marrero, S.; Garcimartin Cerezo, P.; Yun Viladomat, S.; Moliner Borja, P.; et al. Soluble Transferrin Receptor as Iron Deficiency Biomarker: Impact on Exercise Capacity in Heart Failure Patients. J. Pers. Med. 2023, 13, 1282. https://doi.org/10.3390/jpm13081282
Ras-Jiménez MdM, Ramos-Polo R, Francesch Manzano J, Corbella Santano M, Morillas Climent H, Jose-Bazán N, Jiménez-Marrero S, Garcimartin Cerezo P, Yun Viladomat S, Moliner Borja P, et al. Soluble Transferrin Receptor as Iron Deficiency Biomarker: Impact on Exercise Capacity in Heart Failure Patients. Journal of Personalized Medicine. 2023; 13(8):1282. https://doi.org/10.3390/jpm13081282
Chicago/Turabian StyleRas-Jiménez, Maria del Mar, Raúl Ramos-Polo, Josep Francesch Manzano, Miriam Corbella Santano, Herminio Morillas Climent, Núria Jose-Bazán, Santiago Jiménez-Marrero, Paloma Garcimartin Cerezo, Sergi Yun Viladomat, Pedro Moliner Borja, and et al. 2023. "Soluble Transferrin Receptor as Iron Deficiency Biomarker: Impact on Exercise Capacity in Heart Failure Patients" Journal of Personalized Medicine 13, no. 8: 1282. https://doi.org/10.3390/jpm13081282