
Unlocking the Potential of Mesenchymal Stem Cells in Gynecology: Where Are We Now?


 ,
,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Mesenchymal (Stromal) Stem Cells
2.1. Differential Phenotype Pattern of Mesenchymal Stem Cells in Male and Female Patients
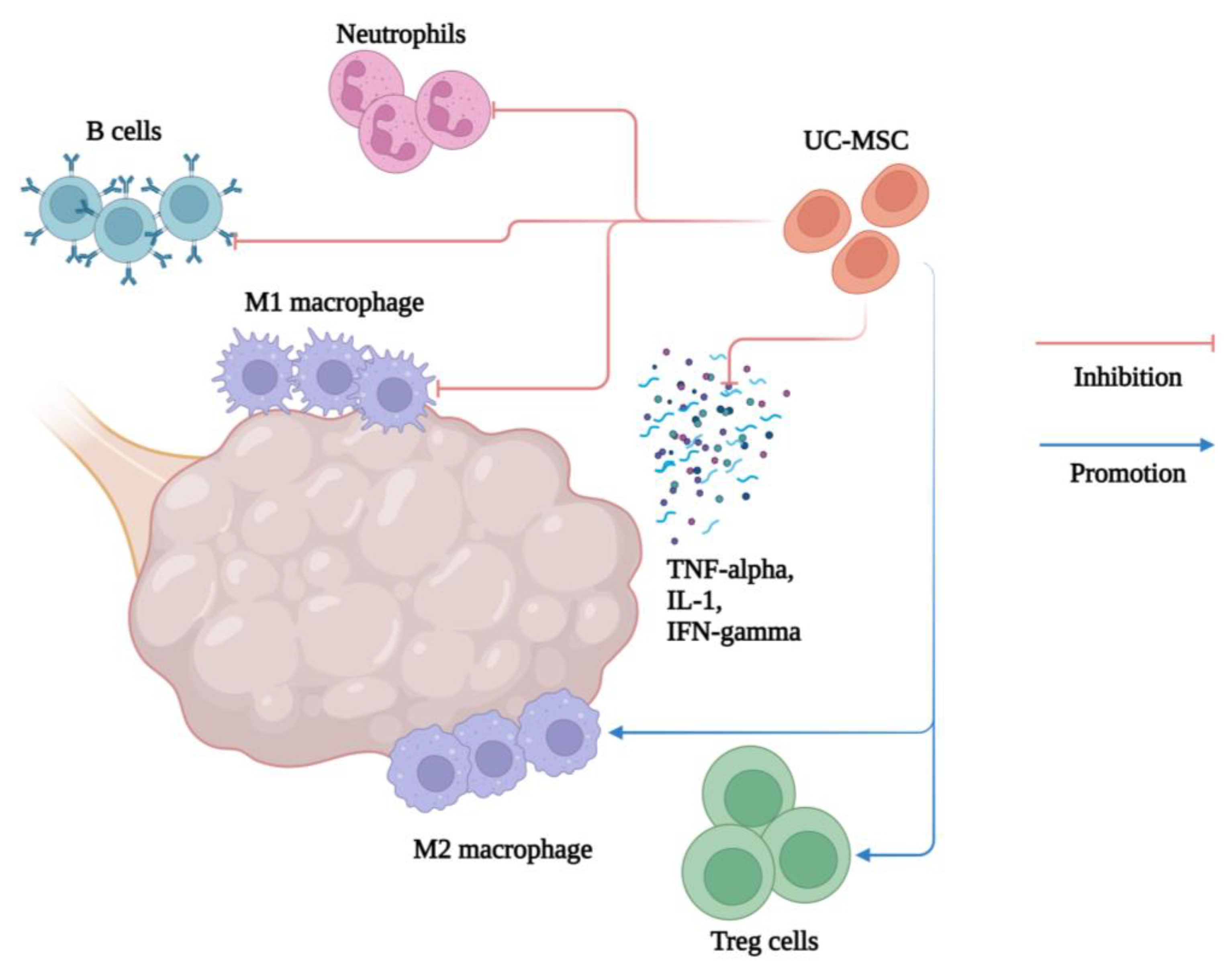
2.2. Regenerative, Immunomodulatory, Anti-Inflammatory, and Antimicrobial Effect of Mesenchymal Stem Cells
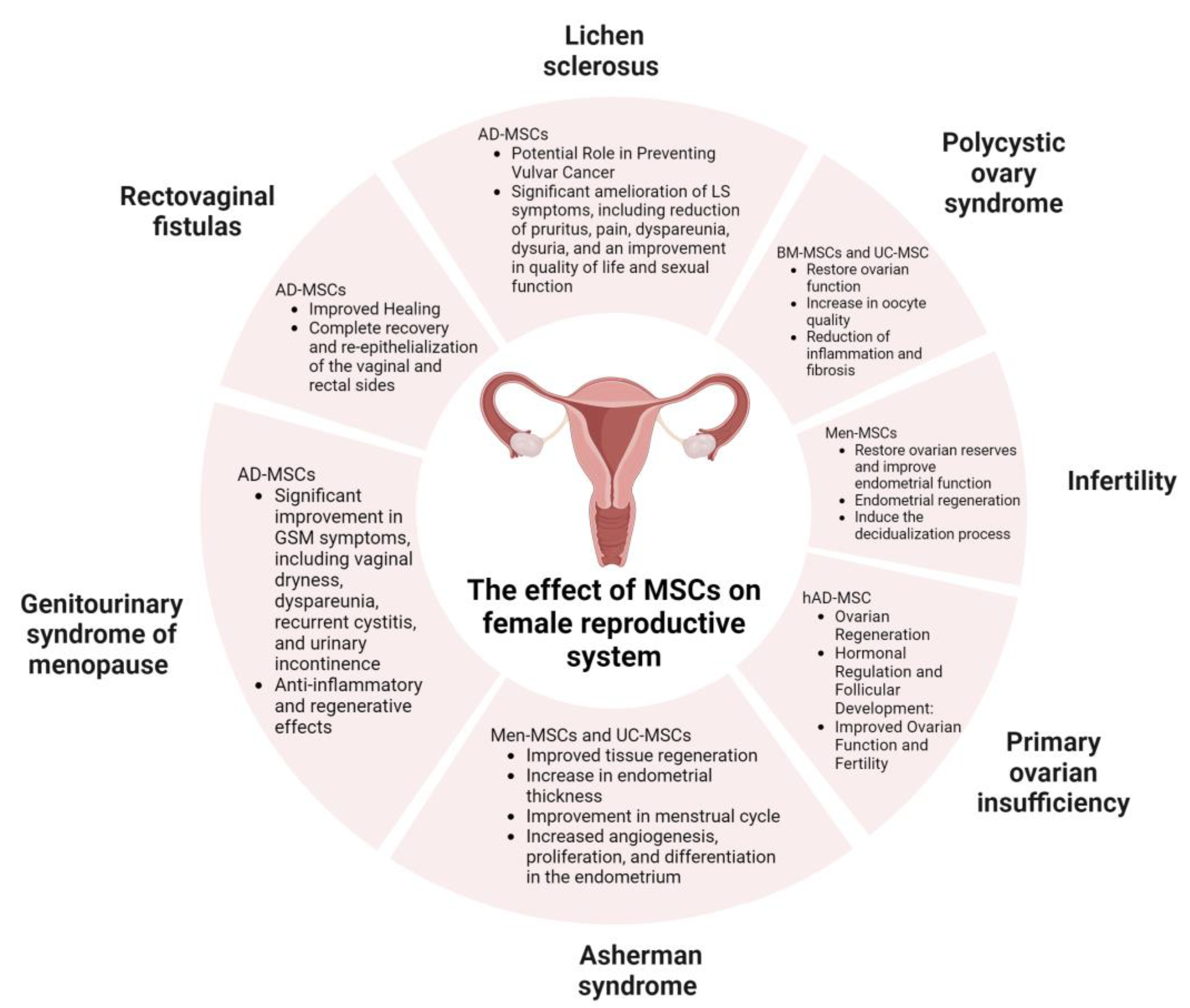
3. Application of Mesenchymal Stem Cells in Gynecological Disorders
3.1. Infertility
3.2. Asherman Syndrome (AS)
3.3. Polycystic Ovary Syndrome (PCOS)
3.4. Primary Ovarian Insufficiency (POI)
3.5. Genitourinary Syndrome of Menopause (GSM)
3.6. Lichen Sclerosus (LS)
3.7. Rectovaginal Fistulas
4. Oogonial Stem Cells
5. Epithelial–Mesenchymal Transition in the Context of Mesenchymal Stem Cells
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bianconi, E.; Piovesan, A.; Facchin, F.; Beraudi, A.; Casadei, R.; Frabetti, F.; Vitale, L.; Pelleri, M.C.; Tassani, S.; Piva, F.; et al. An estimation of the number of cells in the human body. Ann. Hum. Biol. 2013, 40, 463–471. [Google Scholar] [CrossRef]
- Hu, Y.; Yang, Y.; Tan, P.; Zhang, Y.; Han, M.; Yu, J.; Zhang, X.; Jia, Z.; Wang, D.; Yao, K.; et al. Induction of mouse totipotent stem cells by a defined chemical cocktail. Nature 2023, 617, 792–797. [Google Scholar] [CrossRef]
- Reardon, S. Third patient free of HIV after receiving virus-resistant cells. Nature 2023, 615, 13–14. [Google Scholar] [CrossRef]
- Danielyan, L.; Beer-Hammer, S.; Stolzing, A.; Schafer, R.; Siegel, G.; Fabian, C.; Kahle, P.; Biedermann, T.; Lourhmati, A.; Buadze, M.; et al. Intranasal delivery of bone marrow-derived mesenchymal stem cells, macrophages, and microglia to the brain in mouse models of Alzheimer’s and Parkinson’s disease. Cell Transplant. 2014, 23 (Suppl 1), S123–S139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, L.; Liu, J.W.; Shi, H.Y.; Ma, Y.M. Neural stem cell therapy for brain disease. World J. Stem Cells 2021, 13, 1278–1292. [Google Scholar] [CrossRef]
- Dulak, J.; Szade, K.; Szade, A.; Nowak, W.; Jozkowicz, A. Adult stem cells: Hopes and hypes of regenerative medicine. Acta Biochim. Pol. 2015, 62, 329–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamanaka, S. Pluripotent Stem Cell-Based Cell Therapy-Promise and Challenges. Cell Stem Cell 2020, 27, 523–531. [Google Scholar] [CrossRef]
- Lv, F.J.; Tuan, R.S.; Cheung, K.M.; Leung, V.Y. Concise review: The surface markers and identity of human mesenchymal stem cells. Stem Cells 2014, 32, 1408–1419. [Google Scholar] [CrossRef] [PubMed]
- Ullah, I.; Subbarao, R.B.; Rho, G.J. Human mesenchymal stem cells—current trends and future prospective. Biosci. Rep. 2015, 35, e00191. [Google Scholar] [CrossRef]
- Brown, C.; McKee, C.; Bakshi, S.; Walker, K.; Hakman, E.; Halassy, S.; Svinarich, D.; Dodds, R.; Govind, C.K.; Chaudhry, G.R. Mesenchymal stem cells: Cell therapy and regeneration potential. J. Tissue Eng. Regen. Med. 2019, 13, 1738–1755. [Google Scholar] [CrossRef]
- Han, Y.; Li, X.; Zhang, Y.; Han, Y.; Chang, F.; Ding, J. Mesenchymal Stem Cells for Regenerative Medicine. Cells 2019, 8, 886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esfandyari, S.; Chugh, R.M.; Park, H.S.; Hobeika, E.; Ulin, M.; Al-Hendy, A. Mesenchymal Stem Cells as a Bio Organ for Treatment of Female Infertility. Cells 2020, 9, 2253. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.X.; Chen, S.R.; Su, P.P.; Huang, F.H.; Shi, Y.C.; Shi, Q.Y.; Lin, S. Using Mesenchymal Stem Cells to Treat Female Infertility: An Update on Female Reproductive Diseases. Stem Cells Int. 2019, 2019, 9071720. [Google Scholar] [CrossRef]
- Gao, L.; Huang, Z.; Lin, H.; Tian, Y.; Li, P.; Lin, S. Bone Marrow Mesenchymal Stem Cells (BMSCs) Restore Functional Endometrium in the Rat Model for Severe Asherman Syndrome. Reprod. Sci. 2019, 26, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.H.; Kim, B.; Choi, I.; Kim, H.; Choi, H.S.; Suh, K.; Bae, Y.C.; Jung, J.S. Characterization and expression analysis of mesenchymal stem cells from human bone marrow and adipose tissue. Cell Physiol. Biochem. 2004, 14, 311–324. [Google Scholar] [CrossRef]
- Terraciano, P.; Garcez, T.; Ayres, L.; Durli, I.; Baggio, M.; Kuhl, C.P.; Laurino, C.; Passos, E.; Paz, A.H.; Cirne-Lima, E. Cell therapy for chemically induced ovarian failure in mice. Stem Cells Int. 2014, 2014, 720753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sen Halicioglu, B.; Saadat, K.; Tuglu, M.I. Adipose-Derived Mesenchymal Stem Cell Transplantation in Chemotherapy-Induced Premature Ovarian Insufficiency: The Role of Connexin and Pannexin. Reprod. Sci. 2022, 29, 1316–1331. [Google Scholar] [CrossRef]
- Mohamed, S.A.; Shalaby, S.; Brakta, S.; Elam, L.; Elsharoud, A.; Al-Hendy, A. Umbilical Cord Blood Mesenchymal Stem Cells as an Infertility Treatment for Chemotherapy Induced Premature Ovarian Insufficiency. Biomedicines 2019, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Baughn, C.; Campion, S.; Elbabaa, S. Amniotic fluid-derived stem cell potential for therapeutic and surgical use: A review of the literature. Prenat. Diagn. 2022, 42, 157–163. [Google Scholar] [CrossRef]
- Borlongan, C.V. Amniotic fluid as a source of engraftable stem cells. Brain Circ. 2017, 3, 175–179. [Google Scholar] [CrossRef]
- Miki, T. Amnion-derived stem cells: In quest of clinical applications. Stem Cell Res. Ther. 2011, 2, 25. [Google Scholar] [CrossRef] [Green Version]
- Kabagambe, S.; Keller, B.; Becker, J.; Goodman, L.; Pivetti, C.; Lankford, L.; Chung, K.; Lee, C.; Chen, Y.J.; Kumar, P.; et al. Placental mesenchymal stromal cells seeded on clinical grade extracellular matrix improve ambulation in ovine myelomeningocele. J. Pediatr. Surg. 2017, 53, 178–182. [Google Scholar] [CrossRef]
- Liu, J.; Gao, J.; Liang, Z.; Gao, C.; Niu, Q.; Wu, F.; Zhang, L. Mesenchymal stem cells and their microenvironment. Stem Cell Res. Ther. 2022, 13, 429. [Google Scholar] [CrossRef]
- Zenic, L.; Polancec, D.; Hudetz, D.; Jelec, Z.; Rod, E.; Vidovic, D.; Staresinic, M.; Sabalic, S.; Vrdoljak, T.; Petrovic, T.; et al. Polychromatic Flow Cytometric Analysis of Stromal Vascular Fraction from Lipoaspirate and Microfragmented Counterparts Reveals Sex-Related Immunophenotype Differences. Genes 2021, 12, 1999. [Google Scholar] [CrossRef] [PubMed]
- Zakrzewski, W.; Dobrzynski, M.; Szymonowicz, M.; Rybak, Z. Stem cells: Past, present, and future. Stem Cell Res. Ther. 2019, 10, 68. [Google Scholar] [CrossRef]
- Dabrowska, S.; Andrzejewska, A.; Janowski, M.; Lukomska, B. Immunomodulatory and Regenerative Effects of Mesenchymal Stem Cells and Extracellular Vesicles: Therapeutic Outlook for Inflammatory and Degenerative Diseases. Front. Immunol. 2020, 11, 591065. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Garcia, L.; Castro-Manrreza, M.E. TNF-alpha and IFN-gamma Participate in Improving the Immunoregulatory Capacity of Mesenchymal Stem/Stromal Cells: Importance of Cell-Cell Contact and Extracellular Vesicles. Int. J. Mol. Sci. 2021, 22, 9531. [Google Scholar] [CrossRef]
- Fan, X.L.; Zhang, Y.; Li, X.; Fu, Q.L. Mechanisms underlying the protective effects of mesenchymal stem cell-based therapy. Cell Mol. Life Sci. 2020, 77, 2771–2794. [Google Scholar] [CrossRef] [Green Version]
- Sharma, A.; Chakraborty, A.; Jaganathan, B.G. Review of the potential of mesenchymal stem cells for the treatment of infectious diseases. World J. Stem Cells. 2021, 13, 568–593. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.Y.; Yan, Z.B.; Meng, Y.M.; Hong, X.Y.; Shao, G.; Ma, J.J.; Cheng, X.R.; Liu, J.; Kang, J.; Fu, C.Y. Antimicrobial peptides: Mechanism of action, activity and clinical potential. Mil. Med. Res. 2021, 8, 48. [Google Scholar]
- Pahar, B.; Madonna, S.; Das, A.; Albanesi, C.; Girolomoni, G. Immunomodulatory Role of the Antimicrobial LL-37 Peptide in Autoimmune Diseases and Viral Infections. Vaccines 2020, 8, 517. [Google Scholar] [CrossRef] [PubMed]
- Smojver, I.; Katalinić, I.; Bjelica, R.; Gabrić, D.; Matišić, V.; Molnar, V.; Primorac, D. Mesenchymal Stem Cells Based Treatment in Dental Medicine: A Narrative Review. Int. J. Mol. Sci. 2022, 23, 1662. [Google Scholar] [CrossRef]
- Molnar, V.; Pavelić, E.; Vrdoljak, K.; Čemerin, M.; Klarić, E.; Matišić, V.; Bjelica, R.; Brlek, P.; Kovačić, I.; Tremolada, C.; et al. Mesenchymal Stem Cell Mechanisms of Action and Clinical Effects in Osteoarthritis: A Narrative Review. Genes 2022, 13, 949. [Google Scholar] [CrossRef] [PubMed]
- Molnar, V.; Pavelić, E.; Jeleč, Ž.; Brlek, P.; Matišić, V.; Borić, I.; Hudetz, D.; Rod, E.; Vidović, D.; Starčević, N.; et al. Results of Treating Mild to Moderate Knee Osteoarthritis with Autologous Conditioned Adipose Tissue. J. Pers. Med. 2023, 13, 47. [Google Scholar] [CrossRef]
- Polancec, D.; Zenic, L.; Hudetz, D.; Boric, I.; Jelec, Z.; Rod, E.; Vrdoljak, T.; Skelin, A.; Plecko, M.; Turkalj, M.; et al. Immunophenotyping of a Stromal Vascular Fraction from Microfragmented Lipoaspirate Used in Osteoarthritis Cartilage Treatment and Its Lipoaspirate Counterpart. Genes 2019, 10, E474. [Google Scholar] [CrossRef] [Green Version]
- Primorac, D.; Hudetz, D.; Borić, I.; Jeleč, Ž.; Rod, E.; Vrdoljak, T.; Lauc, G.; Skelin APolančec, D.; Zenić, L.; Trbojević-Akmačić, I.; et al. Cell therapy in treatment of cartilage tissue defects: Experiences from St. Catherine Specialty Hospital. Paediatr. Croat. 2018, 62, 167–168. [Google Scholar]
- Primorac, D.; Stojanović Stipić, S.; Strbad, M.; Girandon, L.; Barlič, A.; Frankić, M.; Ivić, I.; Marasović Krstulović, D.; Jukić, I.; Halassy, B.; et al. Compassionate mesenchymal stem cell treatment in a severe COVID-19 patient: A case report. Croat. Med. J. 2021, 62, 288–296. [Google Scholar] [CrossRef]
- Crawford, N.M.; Steiner, A.Z. Age-related infertility. Obstet. Gynecol. Clin. N. Am. 2015, 42, 15–25. [Google Scholar] [CrossRef]
- Practice Committee of the American Society for Reproductive Medicine. Definitions of infertility and recurrent pregnancy loss: A committee opinion. Fertil. Steril. 2013, 99, 63. [Google Scholar] [CrossRef]
- Silvestris, E.; de Pergola, G.; Rosania, R.; Loverro, G. Obesity as disruptor of the female fertility. Reprod. Biol. Endocrinol. 2018, 16, 22. [Google Scholar] [CrossRef]
- Bedenk, J.; Vrtacnik-Bokal, E.; Virant-Klun, I. The role of anti-Mullerian hormone (AMH) in ovarian disease and infertility. J. Assist. Reprod. Genet. 2020, 37, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Rungsiwiwut, R.; Virutamasen, P.; Pruksananonda, K. Mesenchymal stem cells for restoring endometrial function: An infertility perspective. Reprod. Med. Biol. 2021, 20, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Lv, Q.; Wang, L.; Luo, X.; Chen, X. Adult stem cells in endometrial regeneration: Molecular insights and clinical applications. Mol. Reprod. Dev. 2021, 88, 379–394. [Google Scholar] [CrossRef] [PubMed]
- de Miguel-Gomez, L.; Lopez-Martinez, S.; Frances-Herrero, E.; Rodriguez-Eguren, A.; Pellicer, A.; Cervello, I. Stem Cells and the Endometrium: From the Discovery of Adult Stem Cells to Pre-Clinical Models. Cells 2021, 10, 595. [Google Scholar] [CrossRef] [PubMed]
- Ugurlu, B.; Karaoz, E. Comparison of similar cells: Mesenchymal stromal cells and fibroblasts. Acta Histochem. 2020, 122, 151634. [Google Scholar] [CrossRef] [PubMed]
- Skliute, G.; Bausyte, R.; Borutinskaite, V.; Valiuliene, G.; Kaupinis, A.; Valius, M.; Ramasauskaite, D.; Navakauskiene, R. Menstrual Blood-Derived Endometrial Stem Cells’ Impact for the Treatment Perspective of Female Infertility. Int. J. Mol. Sci. 2021, 22, 6774. [Google Scholar] [CrossRef]
- Benor, A.; Gay, S.; DeCherney, A. An update on stem cell therapy for Asherman syndrome. J. Assist. Reprod. Genet. 2020, 37, 1511–1529. [Google Scholar] [CrossRef]
- Hu, J.; Zeng, B.; Jiang, X.; Hu, L.; Meng, Y.; Zhu, Y.; Mao, M. The expression of marker for endometrial stem cell and fibrosis was increased in intrauterine adhesious. Int. J. Clin. Exp. Pathol. 2015, 8, 1525–1534. [Google Scholar]
- Tan, J.; Li, P.; Wang, Q.; Li, Y.; Li, X.; Zhao, D.; Xu, X.; Kong, L. Autologous menstrual blood-derived stromal cells transplantation for severe Asherman’s syndrome. Hum. Reprod. 2016, 31, 2723–2729. [Google Scholar] [CrossRef] [Green Version]
- Smikle, C.; Yarrarapu, S.N.S.; Khetarpal, S. Asherman Sindrome StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: www.ncbi.nlm.nih.gov/books/NBK448088 (accessed on 30 March 2023).
- Zhang, Y.; Shi, L.; Lin, X.; Zhou, F.; Xin, L.; Xu, W.; Yu, H.; Li, J.; Pan, M.; Pan, Y.; et al. Unresponsive thin endometrium caused by Asherman syndrome treated with umbilical cord mesenchymal stem cells on collagen scaffolds: A pilot study. Stem Cell Res. Ther. 2021, 12, 420. [Google Scholar] [CrossRef]
- Zhao, Y.; Luo, Q.; Zhang, X.; Qin, Y.; Hao, J.; Kong, D.; Wang, H.; Li, G.; Gu, X.; Wang, H. Clinical Efficacy and Safety of Stem Cell-Based Therapy in Treating Asherman Syndrome: A System Review and Meta-Analysis. Stem Cells Int. 2020, 2020, 8820538. [Google Scholar] [CrossRef] [PubMed]
- Ma, H.; Liu, M.; Li, Y.; Wang, W.; Yang, K.; Lu, L.; He, M.; Deng, T.; Li, M.; Wu, D. Intrauterine transplantation of autologous menstrual blood stem cells increases endometrial thickness and pregnancy potential in patients with refractory intrauterine adhesion. J. Obstet. Gynaecol. Res. 2020, 46, 2347–2355. [Google Scholar] [CrossRef]
- Wang, R.; Mol, B.W. The Rotterdam criteria for polycystic ovary syndrome: Evidence-based criteria? Hum. Reprod. 2017, 32, 261–264. [Google Scholar] [CrossRef]
- Diamanti-Kandarakis, E.; Dunaif, A. Insulin resistance and the polycystic ovary syndrome revisited: An update on mechanisms and implications. Endocr. Rev. 2012, 33, 981–1030. [Google Scholar] [CrossRef]
- Murri, M.; Luque-Ramirez, M.; Insenser, M.; Ojeda-Ojeda, M.; Escobar-Morreale, H.F. Circulating markers of oxidative stress and polycystic ovary syndrome (PCOS): A systematic review and meta-analysis. Hum. Reprod. Update 2013, 19, 268–288. [Google Scholar] [CrossRef] [PubMed]
- Chugh, R.M.; Park, H.S.; Esfandyari, S.; Elsharoud, A.; Ulin, M.; Al-Hendy, A. Mesenchymal Stem Cell-Conditioned Media Regulate Steroidogenesis and Inhibit Androgen Secretion in a PCOS Cell Model via BMP-2. Int. J. Mol. Sci. 2021, 22, 9184. [Google Scholar] [CrossRef]
- Dumesic, D.A.; Abbott, D.H.; Sanchita, S.; Chazenbalk, G.D. Endocrine-Metabolic Dysfunction in Polycystic Ovary Syndrome: An Evolutionary Perspective. Curr. Opin. Endocr. Metab. Res. 2020, 12, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Chugh, R.M.; Park, H.S.; El Andaloussi, A.; Elsharoud, A.; Esfandyari, S.; Ulin, M.; Bakir, L.; Aboalsoud, A.; Ali, M.; Ashour, D.; et al. Mesenchymal stem cell therapy ameliorates metabolic dysfunction and restores fertility in a PCOS mouse model through interleukin-10. Stem Cell Res. Ther. 2021, 12, 388. [Google Scholar] [CrossRef]
- Kalhori, Z.; Azadbakht, M.; Soleimani Mehranjani, M.; Shariatzadeh, M.A. Improvement of the folliculogenesis by transplantation of bone marrow mesenchymal stromal cells in mice with induced polycystic ovary syndrome. Cytotherapy 2018, 20, 1445–1458. [Google Scholar] [CrossRef]
- Prayitno, G.D.; Lestari, K.; Sartika, C.R.; Djuwantono, T.; Widjaya, A.; Muharam, R.; Hidayat, Y.M.; Wulandari, D.; Haifa, R.; Naura, N.F.; et al. Potential of Mesenchymal Stem Cells and Their Secretomes in Decreasing Inflammation Markers in Polycystic Ovary Syndrome Treatment: A Systematic Review. Medicines 2022, 10, 3. [Google Scholar] [CrossRef]
- Xie, Q.; Xiong, X.; Xiao, N.; He, K.; Chen, M.; Peng, J.; Su, X.; Mei, H.; Dai, Y.; Wei, D.; et al. Mesenchymal Stem Cells Alleviate DHEA-Induced Polycystic Ovary Syndrome (PCOS) by Inhibiting Inflammation in Mice. Stem Cells Int. 2019, 2019, 9782373. [Google Scholar] [CrossRef] [Green Version]
- Welt, C.K. Primary ovarian insufficiency: A more accurate term for premature ovarian failure. Clin. Endocrinol. 2008, 68, 499–509. [Google Scholar] [CrossRef]
- European Society for Human R; Embryology Guideline Group on POI; Webber, L.; Davies, M.; Anderson, R.; Bartlett, J.; Braat, D.; Cartwright, B.; Cifkova, R.; de Muinck Keizer-Scharma, S.; et al. ESHRE Guideline: Management of women with premature ovarian insufficiency. Hum. Reprod. 2016, 31, 926–937. [Google Scholar] [CrossRef]
- Maclaran, K.; Panay, N. Current concepts in premature ovarian insufficiency. Womens Health 2015, 11, 169–182. [Google Scholar] [CrossRef]
- Li, Z.; Zhang, M.; Tian, Y.; Li, Q.; Huang, X. Mesenchymal Stem Cells in Premature Ovarian Insufficiency: Mechanisms and Prospects. Front. Cell Dev. Biol. 2021, 9, 718192. [Google Scholar] [CrossRef]
- Ling, L.; Feng, X.; Wei, T.; Wang, Y.; Wang, Y.; Wang, Z.; Tang, D.; Luo, Y.; Xiong, Z. Human amnion-derived mesenchymal stem cell (hAD-MSC) transplantation improves ovarian function in rats with premature ovarian insufficiency (POI) at least partly through a paracrine mechanism. Stem Cell Res. Ther. 2019, 10, 46. [Google Scholar] [CrossRef] [Green Version]
- Yin, N.; Zhao, W.; Luo, Q.; Yuan, W.; Luan, X.; Zhang, H. Restoring Ovarian Function With Human Placenta-Derived Mesenchymal Stem Cells in Autoimmune-Induced Premature Ovarian Failure Mice Mediated by Treg Cells and Associated Cytokines. Reprod. Sci. 2018, 25, 1073–1082. [Google Scholar] [CrossRef]
- Mohamed, S.A.; Shalaby, S.M.; Abdelaziz, M.; Brakta, S.; Hill, W.D.; Ismail, N.; Al-Hendy, A. Human Mesenchymal Stem Cells Partially Reverse Infertility in Chemotherapy-Induced Ovarian Failure. Reprod. Sci. 2018, 25, 51–63. [Google Scholar] [CrossRef] [Green Version]
- Sun, M.; Wang, S.; Li, Y.; Yu, L.; Gu, F.; Wang, C.; Yao, Y. Adipose-derived stem cells improved mouse ovary function after chemotherapy-induced ovary failure. Stem Cell Res. Ther. 2013, 4, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabr, H.; Elkheir, W.A.; El-Gazzar, A. Autologus stem cell transplantation in patients with idiopathic premature ovarian failure. J. Tissue Sci. Eng. 2016, 7, 27. [Google Scholar]
- Wang, Z.; Wang, Y.; Yang, T.; Li, J.; Yang, X. Study of the reparative effects of menstrual-derived stem cells on premature ovarian failure in mice. Stem Cell Res. Ther. 2017, 8, 11. [Google Scholar] [CrossRef] [Green Version]
- Kagan, R.; Kellogg-Spadt, S.; Parish, S.J. Practical Treatment Considerations in the Management of Genitourinary Syndrome of Menopause. Drugs Aging 2019, 36, 897–908. [Google Scholar] [CrossRef] [Green Version]
- Shifren, J.L. Genitourinary Syndrome of Menopause. Clin. Obstet. Gynecol. 2018, 61, 508–516. [Google Scholar] [CrossRef] [Green Version]
- Angelou, K.; Grigoriadis, T.; Diakosavvas, M.; Zacharakis, D.; Athanasiou, S. The Genitourinary Syndrome of Menopause: An Overview of the Recent Data. Cureus 2020, 12, e7586. [Google Scholar] [CrossRef] [Green Version]
- Kasap, B.; Kasap, S.; Vatansever, S.; Kendirci, R.; Yilmaz, O.; Calisir, M.; Edgunlu, T.; Akin, M.N. Effects of adipose and bone marrow-derived mesenchymal stem cells on vaginal atrophy in a rat menopause model. Gene 2019, 711, 143937. [Google Scholar] [CrossRef]
- Casarotti, G.; Tremolada, C. A new treatment of genito-urinary post-menopausal atrophy with autologous micro-fragmented fat tissue: A thirty-six months follow up case series. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 7420–7426. [Google Scholar]
- Tremolada, C.; Allegri, M.; Slevin, M. Mesenchymal Stromal Cells and Micro Fragmented Adipose Tissue: New Horizons of Effectiveness of Lipogems. J. Stem Cell Res. Dev. 2019, 5, 17. [Google Scholar] [CrossRef]
- Xu, T.; Yu, X.; Yang, Q.; Liu, X.; Fang, J.; Dai, X. Autologous Micro-Fragmented Adipose Tissue as Stem Cell-Based Natural Scaffold for Cartilage Defect Repair. Cell Transplant. 2019, 28, 1709–1720. [Google Scholar] [CrossRef]
- Chamli, A.; Souissi, A. Lichen Sclerosus; StatPearls Publishing: Treasure Island, FL, USA, 2 April 2021. Available online: www.ncbi.nlm.nih.gov/books/NBK538246 (accessed on 2 April 2023).
- Kirtschig, G. Lichen Sclerosus-Presentation, Diagnosis and Management. Dtsch. Arztebl. Int. 2016, 113, 337–343. [Google Scholar] [CrossRef] [Green Version]
- Krapf, J.M.; Mitchell, L.; Holton, M.A.; Goldstein, A.T. Vulvar Lichen Sclerosus: Current Perspectives. Int. J. Womens Health 2020, 12, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Perez-Lopez, F.R.; Vieira-Baptista, P. Lichen sclerosus in women: A review. Climacteric 2017, 20, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Murphy, R. Lichen sclerosus. Dermatol. Clin. 2010, 28, 707–715. [Google Scholar] [CrossRef]
- Eshtiaghi, P.; Sadownik, L.A. Fact or Fiction? Adipose-Derived Stem Cells and Platelet-Rich Plasma for the Treatment of Vulvar Lichen Sclerosus. J. Low. Genit. Tract. Dis. 2019, 23, 65–70. [Google Scholar] [CrossRef]
- Tedesco, M.; Bellei, B.; Garelli, V.; Caputo, S.; Latini, A.; Giuliani, M.; Cota, C.; Chichierchia, G.; Romani, C.; Foddai, M.L.; et al. Adipose tissue stromal vascular fraction and adipose tissue stromal vascular fraction plus platelet-rich plasma grafting: New regenerative perspectives in genital lichen sclerosus. Dermatol. Ther. 2020, 33, e14277. [Google Scholar] [CrossRef]
- Debeche-Adams, T.H.; Bohl, J.L. Rectovaginal fistulas. Clin. Colon. Rectal Surg. 2010, 23, 99–103. [Google Scholar] [CrossRef]
- Laureti, S.; Gionchetti, P.; Cappelli, A.; Vittori, L.; Contedini, F.; Rizzello, F.; Golfieri, R.; Campieri, M.; Poggioli, G. Refractory Complex Crohn’s Perianal Fistulas: A Role for Autologous Microfragmented Adipose Tissue Injection. Inflamm. Bowel Dis. 2020, 26, 321–330. [Google Scholar] [CrossRef]
- Cao, Y.; Su, Q.; Zhang, B.; Shen, F.; Li, S. Efficacy of stem cells therapy for Crohn’s fistula: A meta-analysis and systematic review. Stem Cell Res. Ther. 2021, 12, 32. [Google Scholar] [CrossRef]
- Garcia-Arranz, M.; Herreros, M.D.; Gonzalez-Gomez, C.; de la Quintana, P.; Guadalajara, H.; Georgiev-Hristov, T.; Trebol, J.; Garcia-Olmo, D. Treatment of Crohn’s-Related Rectovaginal Fistula With Allogeneic Expanded-Adipose Derived Stem Cells: A Phase I-IIa Clinical Trial. Stem Cells Transl. Med. 2016, 5, 1441–1446. [Google Scholar] [CrossRef]
- de Weerd, L.; Weum, S.; Norderval, S. Novel treatment for recalcitrant rectovaginal fistulas: Fat injection. Int. Urogynecol. J. 2015, 26, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Dimova, A.; Erceg Ivkošić, I.; Brlek, P.; Dimov, S.; Pavlović, T.; Bokun, T.; Primorac, D. Case report: Novel approach in rectovaginal fistula treatment- the combination of modified Martius flap and microfragmented adipose tissue (Submitted).
- Meng, L.; Zhang, Y.; Hua, Y.; Ma, Y.; Wang, H.; Li, X.; Jiang, Y.; Zhu, G. Identification of oogonial stem cells in chicken ovary. Cell Prolif. 2023, 56, e13371. [Google Scholar] [CrossRef]
- MacDonald, J.A.; Sheehan, H.C.; Piasecki, A.; Faustino, L.R.; Hauschildt, C.; Stolzenbach, V.; Woods, D.C.; Tilly, J.L. Characterization of Oogonial Stem Cells in Adult Mouse Ovaries with Age and Comparison to In Silico Data on Human Ovarian Aging. Stem Cells Dev. 2023, 32, 99–114. [Google Scholar] [CrossRef]
- Wang, C.; Sun, Q.; Li, S.; Liu, G.; Ren, J.; Li, Y.; Ding, X.; Zhu, J.; Dai, Y. Isolation of female germline stem cells from neonatal piglet ovarian tissue and differentiation into oocyte-like cells. Theriogenology 2023, 197, 186–197. [Google Scholar] [CrossRef] [PubMed]
- Wagner, M.; Yoshihara, M.; Douagi, I.; Damdimopoulos, A.; Panula, S.; Petropoulos, S.; Lu, H.; Pettersson, K.; Palm, K.; Katayama, S.; et al. Single-cell analysis of human ovarian cortex identifies distinct cell populations but no oogonial stem cells. Nat. Commun. 2020, 11, 1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sequeira, R.C.; Sittadjody, S.; Criswell, T.; Atala, A.; Jackson, J.D.; Yoo, J.J. Enhanced method to select human oogonial stem cells for fertility research. Cell Tissue Res. 2021, 386, 145–156. [Google Scholar] [CrossRef]
- Mirzaeian, L.; Eivazkhani, F.; Saber, M.; Moini, A.; Esfandiari, F.; Valojerdi, M.R.; Fathi, R. In-vivo oogenesis of oogonial and mesenchymal stem cells seeded in transplanted ovarian extracellular matrix. J. Ovarian Res. 2023, 16, 56. [Google Scholar] [CrossRef]
- Chen, T.; You, Y.; Jiang, H.; Wang, Z.Z. Epithelial-mesenchymal transition (EMT): A biological process in the development, stem cell differentiation, and tumorigenesis. J. Cell Physiol. 2017, 232, 3261–3272. [Google Scholar] [CrossRef] [PubMed]
- So, K.A.; Min, K.J.; Hong, J.H.; Lee, J.K. Interleukin-6 expression by interactions between gynecologic cancer cells and human mesenchymal stem cells promotes epithelial-mesenchymal transition. Int. J. Oncol. 2015, 47, 1451–1459. [Google Scholar] [CrossRef] [Green Version]
- Lin, X.; Qiu, J.; Hua, K. Long non-coding RNAs as emerging regulators of epithelial to mesenchymal transition in gynecologic cancers. Biosci. Trends 2018, 12, 342–353. [Google Scholar] [CrossRef] [Green Version]
- Du, J.; Sun, B.; Zhao, X.; Gu, Q.; Dong, X.; Mo, J.; Sun, T.; Wang, J.; Sun, R.; Liu, Y. Hypoxia promotes vasculogenic mimicry formation by inducing epithelial-mesenchymal transition in ovarian carcinoma. Gynecol. Oncol. 2014, 133, 575–583. [Google Scholar] [CrossRef]
- Bilyk, O.; Coatham, M.; Jewer, M.; Postovit, L.M. Epithelial-to-Mesenchymal Transition in the Female Reproductive Tract: From Normal Functioning to Disease Pathology. Front. Oncol. 2017, 7, 145. [Google Scholar] [CrossRef] [Green Version]
- Ailia, M.J.; Thakur, N.; Chong, Y.; Yim, K. Tumor Budding in Gynecologic Cancer as a Marker for Poor Survival: A Systematic Review and Meta-Analysis of the Perspectives of Epithelial-Mesenchymal Transition. Cancers 2022, 14, 1431. [Google Scholar] [CrossRef] [PubMed]
- Brlek, P.; Bukovac, A.; Kafka, A.; Pecina-Slaus, N. TWIST1 upregulation affects E-cadherin expression in brain metastases. Clin. Transl. Oncol. 2021, 23, 1085–1095. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.M.; Zhang, H.; Han, X. Role of epithelial to mesenchymal transition proteins in gynecological cancers: Pathological and therapeutic perspectives. Tumour Biol. 2014, 35, 9523–9530. [Google Scholar] [CrossRef] [PubMed]
- Keyvani, V.; Riahi, E.; Yousefi, M.; Esmaeili, S.A.; Shafabakhsh, R.; Moradi Hasan-Abad, A.; Mahjoubin-Tehran, M.; Hamblin, M.R.; Mollazadeh, S.; Mirzaei, H. Gynecologic Cancer, Cancer Stem Cells, and Possible Targeted Therapies. Front. Pharmacol. 2022, 13, 823572. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Yi, H.; Song, Y. The safety of MSC therapy over the past 15 years: A meta-analysis. Stem Cell Res. Ther. 2021, 12, 545. [Google Scholar] [CrossRef] [PubMed]
- Bukovac, A.; Kafka, A.; Raguz, M.; Brlek, P.; Dragicevic, K.; Muller, D.; Pecina-Slaus, N. Are We Benign? What Can Wnt Signaling Pathway and Epithelial to Mesenchymal Transition Tell Us about Intracranial Meningioma Progression. Cancers 2021, 13, 1633. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Erceg Ivkošić, I.; Fureš, R.; Ćosić, V.; Mikelin, N.; Bulić, L.; Dobranić, D.; Brlek, P.; Primorac, D. Unlocking the Potential of Mesenchymal Stem Cells in Gynecology: Where Are We Now? J. Pers. Med. 2023, 13, 1253. https://doi.org/10.3390/jpm13081253
Erceg Ivkošić I, Fureš R, Ćosić V, Mikelin N, Bulić L, Dobranić D, Brlek P, Primorac D. Unlocking the Potential of Mesenchymal Stem Cells in Gynecology: Where Are We Now? Journal of Personalized Medicine. 2023; 13(8):1253. https://doi.org/10.3390/jpm13081253
Chicago/Turabian StyleErceg Ivkošić, Ivana, Rajko Fureš, Vesna Ćosić, Nika Mikelin, Luka Bulić, Domagoj Dobranić, Petar Brlek, and Dragan Primorac. 2023. "Unlocking the Potential of Mesenchymal Stem Cells in Gynecology: Where Are We Now?" Journal of Personalized Medicine 13, no. 8: 1253. https://doi.org/10.3390/jpm13081253